
三尖瓣环大小和经食管超声心动图在功能性三尖瓣成形术中的应用
2017-09-13 06:55左明良尹立雪李春梅王斯佳
实用医院临床杂志 2017年5期
左明良,尹立雪,李春梅,邓 燕,王斯佳,徐 云,于 涛
(四川省医学科学院·四川省人民医院 a.心血管超声及心功能科;b.心脏外科,四川 成都 610072)
三尖瓣环大小和经食管超声心动图在功能性三尖瓣成形术中的应用
左明良a,尹立雪a,李春梅a,邓 燕a,王斯佳a,徐 云a,于 涛b
(四川省医学科学院·四川省人民医院 a.心血管超声及心功能科;b.心脏外科,四川 成都 610072)
目的评估和比较经胸超声心动图和经食道超声心动图测量三尖瓣环。方法从2015年12月至2017年4月我院心脏外科中心接受因功能性三尖瓣返流行三尖瓣成形的146名患者。完成左心手术后三尖瓣缝线成形或成形环成形,并分为缝线组72例,成形环成型组74例。分别采用经胸超声心动图心尖切面及经食道超声心动图食管中段右室流入道流出道切面测量三尖瓣环,并与术中实际测值比较。结果79例女性患者,平均年龄(46.2±14.7)岁,平均左室射血分数60.1%,肺动脉收缩压(44.9±14.9)mmHg。同时进行二尖瓣置换或成形78例,主动脉瓣置换51例,其中双瓣置换62例,房间隔缺损修复17例。三尖瓣缝线和成形环成形两组间比较,两组主动脉阻断时间、体外循环时间、肺动脉收缩压、左室收缩功能无显著区别,然而,成形环成形组年龄小于缝线组,二尖瓣置换或修复及房间隔修复患者多于缝线组,三尖瓣返流程度较缝线组重。经食管超声心动图右室流入道流出道切面测量三尖瓣瓣环径与术中实测值比较,差异无统计学意义;经胸超声心动图测值显著低于术中实测值。结论经食管超声心动图能提供加准确的三尖瓣环测值,而经胸超声心动图低估三尖瓣环直径。
经食道超声心动图;三尖瓣环;功能性三尖瓣成形
功能性三尖瓣返流,即不合并器质性瓣膜和心肌病变情况下的三尖瓣返流,是目前最常见的三尖瓣功能失调。三尖瓣返流的持续存在和加重可以导致充血性心力衰竭,从而增加发病率和死亡率。即便中度三尖瓣返流,无论左心室功能和肺动脉压力如何,亦会对患者生存产生负面影响[1]。因此,对于二尖瓣和主动脉瓣手术时,若合并轻到中度三尖瓣返流或者右房扩大,必须对三尖瓣进行外科探查。而精确判断瓣环径线不仅能识别三尖瓣返流机制,而对于手术修复成功与否尤为重要[2]。而瓣环扩张是三尖瓣返流最常见的原因,瓣环直径增加20%就可引起瓣叶对合不良,继而导致返流。相较于二尖瓣,三尖瓣超声心动图提供信息不够准确和详细。而既往ASE指南尽管提供了正常右心详细测量以及正常值,但却未包括三尖瓣环的标准测量方法[3]。目前认为四腔心切面中瓣环直径达到40 mm即表明扩张,并对应术中前隔交界至前后交界[4,5]。然而,心尖四腔心切面仅显示隔瓣与前瓣中份的距离,而功能性三尖瓣返流中,扩张最严重部分是后瓣环对应右室游离壁,可使该处长度增加80%,而前瓣受影响程度较低,其次为隔瓣,四腔心切面并不能敏感显示瓣环扩大。因此,有必要经胸及经食管超声心动图重新评估瓣环大小并与术中直接测量对比,以指导手术方式的选择,并有助于对三尖瓣返流机制的认识。
1 资料与方法
1.1一般资料选取2015年12月至2017年4月在我院心脏手术同时进行功能性三尖瓣返流共146例患者,根据患者三尖瓣返流情况、瓣环大小及合并症选择成形方法,分别进行缝线成形和瓣环成形术,并选择相应大小的成形环。其中,分为三尖瓣改良Kay及De Vega缝线成形72例,成形环成形74例,79例为女性患者,年龄(46.2±14.7)岁,体表面积(1.52±0.20)m2,体外循环时间(110.3±27.5)分钟,根据成形方法分为两组,缝线组和成形环成形组。因风湿性心脏病、二尖瓣脱垂、感染性心内膜炎行二尖瓣置换或成形78例,因风湿性心脏病、主动脉瓣发育异常、感染性心内膜炎行主动脉瓣置换51例,其中双瓣置换62例,因房间隔缺损行房间隔缺损修复17例。
1.2手术方法全部病例均在全麻体外循环下进行,处理左心原发瓣膜病变或房间隔缺损修复后进行三尖瓣成形[6]。心房切开后,观察三尖瓣形态,直尺测量瓣环径,测量前隔交界至前后交界之间距离(图1)。
1.3超声检测三尖瓣环径超声仪器Philips IE Elite和CX50,探头5 S-1、X7-2 t,频率分别为5.1 MHz和7.2 MHz。由两位有经验超声医师进行超声心动图手术前常规测量,根据美国超声心动图协会对三尖瓣返流程度进行评估,分轻、中、重度。将多普勒取样线通过三尖瓣返流口血流聚集区,连续多普勒测量3个连续心动周期的返流速度,取最大峰值速度,根据伯努利方程和右房压计算,得到收缩期肺动脉压(sPAP)。每名患者均术前经胸超声心动图及术中经食管超声心动图评估瓣环径及术后效果。术前经胸超声心动图心尖四腔心切面测量舒张期三尖瓣环径;术中经食管超声心动图瓣环径通过食管中段测量,食管中段右室流入道流出道切面,显示主动脉右无冠瓣后探头稍向深面显示三尖瓣前隔瓣交界并微调获得该切面三尖瓣环舒张期最大径(图2)。

图1 术中测量三尖瓣环,前隔交界至前后交界距离

图2 经食管超声心动图影像 a:舒张期三尖瓣环测值;b:收缩期三尖瓣环。
1.3统计学方法应用SPSS 16.0软件进行统计分析。计量资料以均数±标准差表示,组间比较采用配对t检验;计数资料以百分比表示,组间比较采用卡方检验。P< 0.05为差异有统计学意义。
2 结果
2.1两组术中情况比较三尖瓣成形环成形组二尖瓣置换及房间隔修复患者显著多于三尖瓣缝线成形组,而主动脉瓣置换患者显著少于缝线成形组。缝线成形组年龄大于成形环成形组,而体外循环时间、主动脉阻断时间两组相似见表1。
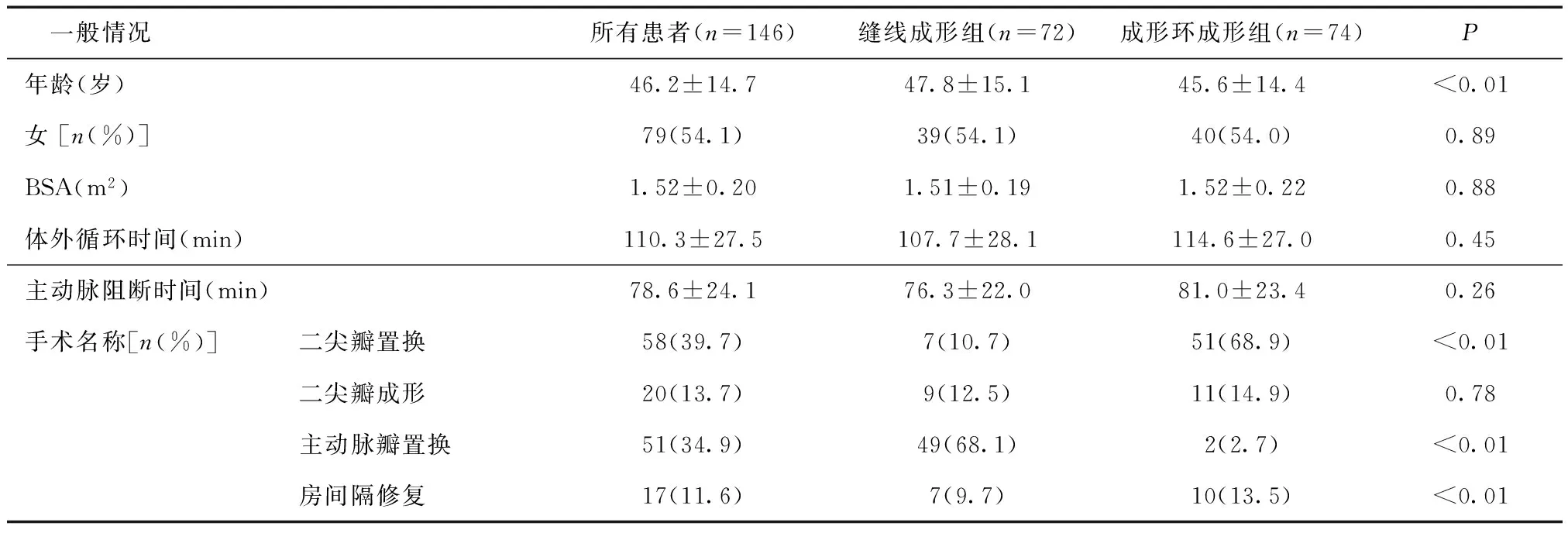
表1 人口特征及手术治疗名称
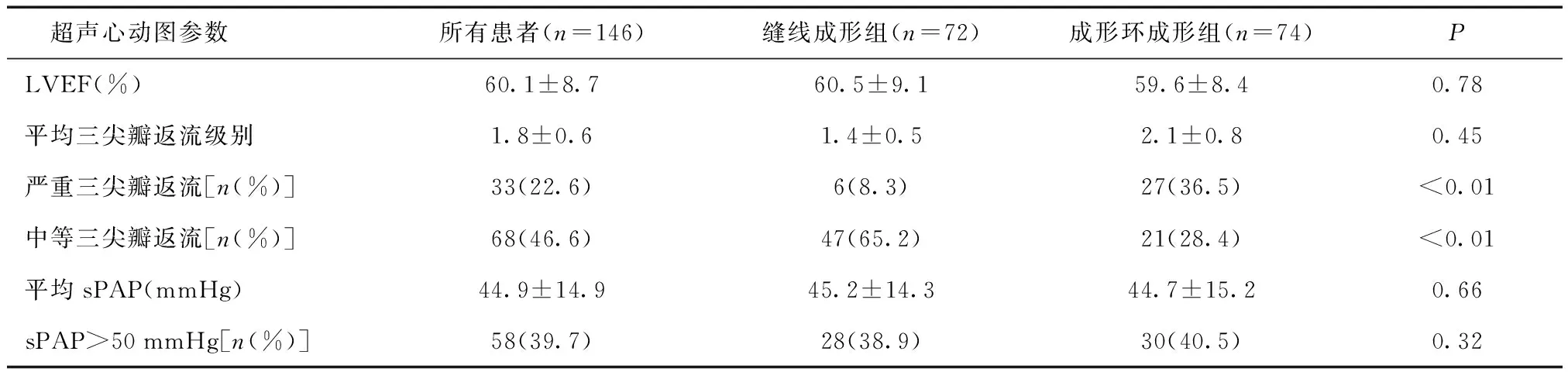
表2 超声心动图特征
2.2两组超声心动图参数及不同方法检测两组瓣环径结果比较成形环成形组三尖瓣返流严重程度重于缝线成形组见表3。无论经胸超声心动图或经食管超声心动图的三尖瓣环测量值,成形环成形组均明显大于缝线成形组,经胸超声心动图瓣环测值明显小于术中实测值,差异有统计学意义(P< 0.01);经食管超声心动图测值与术中实测值比较,差异无统计学意义(P= 0.06)。

表3 不同方法检测两组瓣环径结果比较(mm)
2.3两组预后比较两组三尖瓣返流未见明显返流;术后3月复查,未见明显三尖瓣返流。
3 讨论
既往对功能性三尖瓣返流在左心瓣膜病手术治疗过程中往往被忽略,它常被认为在二尖瓣病变矫治后会得到恢复;然而,近年来临床实践证明,功能性三尖瓣关闭不全在左心系统疾病纠治后并没有得到改善,甚至部分患者三尖瓣关闭不全进一步加重,出现右心功能不全症状。所以对于功能性三尖瓣返流同时行一期治疗是十分必要的[7]。而功能性三尖瓣返流主要是由于三尖瓣环扩大、右室扩大和功能障碍所致。既往认为,超声心动图是最理想评估三尖瓣返流工具,不仅能区分原发或继发性返流,而且能判断瓣环扩张程度。当经胸胸骨旁四腔心切面舒张期瓣环径≥40 mm 或0.21 mm/m2[4,5],即作为三尖瓣成形手术的指针。文献报道,三尖瓣瓣环的正常值范围,在心尖四腔心为31.5 mm(男性)和30.1 mm(女性)[8]。然而,本研究发现,二维经胸超声心动图测量系统性低估真实的三尖瓣环径,与Badano等结果一致[9]。考虑原因,是由于右心室几何结构的特殊性,四腔心切面仅显示部分隔瓣和前瓣[10],五腔心切面尽管可显示主动脉段的前隔交界,右侧却仅能显示部分前瓣,而瓣环扩张主要是在前后瓣,并且随着瓣环的进一步扩张,后瓣环扩张尤为严重,使之增加80%,导致前后瓣叶远离对合点,引起关闭裂隙的产生。因此,经胸超声心动图并不能真实测量三尖瓣瓣环,尤其瓣环扩张严重时。而精确判断瓣环径线不仅能识别三尖瓣返流机制,亦是三尖瓣成形的重要指针。三尖瓣轻度返流及以下,瓣环径<40 mm,无手术指针;三尖瓣轻中度返流以上,瓣环>40 mm,推荐三尖瓣成形[2]。本研究中,成形环成形组瓣环径远大于缝线成形组,进一步显示三尖瓣环的精确测量,有助于手术方式的选择。
本研究发现,经食管超声心动图食管中段右心室流入道流出道切面显示右无冠瓣及右室流出道,能获得瓣环最大直径,与术中直接测量无显著差异。究其原因,考虑与三尖瓣环分段有关,三尖瓣环自前隔交界处,分为4个节段,主动脉段是指靠近主动脉根部附近的瓣环部分,前段指右室流出道相对应的瓣环部分,其上附着前叶及前后交界瓣叶部分,后段附着后叶及后隔交界瓣叶组织,隔段对应室间隔,并附着隔瓣及邻近的前隔交界瓣叶组织。因此,食管中段右室流入道流出道切面显示主动脉段,即为前隔交界,而右室流出道侧,即为前瓣及前后交界瓣叶部分,获得二者之间的距离,即为三尖瓣环最大距离。
鉴于三尖瓣环对手术指导的重要价值,有必要根据经食道超声心动图评估三尖瓣环大小,制定新的手术指针。
[1] Nath J, Foster E, Heidenreich PA.Impact of tricuspid regurgitation on long-term survival[J].J Am Coll Cardiol, 2004, 43:405-409.
[2] Dreyfus GD, Martin RP, Chan KM, et al.Functional tricuspid regurgitation:a need to revise our understanding[J].J Am Coll Cardiol, 2015,65(21):2331-2336.
[3] Rudski LG, Lai WWW, Afilalo J, et al.Guidelines for the echocardiographic assessment of the right heart in adults:a report from the american society of echocardiography endorsed by the european association of echocardiography, a registered branch of the european society of cardiology[J].Canadian Society of Echocardiography,2010,23(7):685-713.
[4] Lancellotti P, Moura L, Pierard LA, et al.European Association of Echocardiography recommendations for the assessment of valvular regurgitation.Part 2:mitral and tricuspid regurgitation (native valve disease) [J].Eur J Echocardiogr, 2010,11:307-332.
[5] Dreyfus GD, Corbi PJ, Chan KM, Bahrami T.Secondary tricuspid regurgitation or dilatation:which should be the criteria for surgical repair [J].Ann Thorac Surg, 2005,79:127-132.
[6] Hata H, Fujita T, Shimahara Y, et al.Mid-term outcomes of aggressive tricuspid annuloplasty with the MC3 ring[J].J Heart Valve Dis, 2014, 23:601-608.
[7] Rogers JH, Bolling SF.Circulation,the tricuspid valve:current perspective and evolving management of tricuspid regurgitation[J].Bolling Circulation, 2009,119(20):2718-2725.
[8] Dwivedi G, Mahadevan G, Jimenez D, et al.Reference values for mitral and tricuspid annular dimensions using two-dimensional echocardiography[J].Echo Res Pract,2014,1(2):43-50.
[9] Badano LP, Agricola E, Perez de Isla L, et al.Evaluation of the tricuspid valve morphology and function by transthoracic real-time three-dimensional echocardiography[J].Eur J Echocardiogr, 2009,10:477-484.
[10]Ancona F, Stella S, Taramasso M.Multimodality imaging of the tricuspid valve with implication for percutaneous repair approaches[J].Heart,2017, 103(14):1073-1081.
Applicationoftricuspidannularsizeandtransesophagealechocardiographyinfunctionaltricuspidannuloplasty
ZUOMing-lianga,YINLi-xuea,LIChun-meia,DENGYana,WANGSi-jiaa,XUYuna,YUTaob
(a.DepartmentofCardiovascularUltrasoundandNon-invasiveCardiology;b.DepartmentofCardiacSurgery,SichuanAcademyofMedicalScience&SichuanProvincialPeople’sHospital,Chengdu, 610072,China)
YINLi-Xue
ObjectiveTo assess and compare the measurement of tricuspid annular (TA) dimensions using transthoracic echocardiography and transesophageal echocardiography.MethodsFrom December 2015 to April 2017, 146 patients underwent tricuspid annuloplasty (TAP) in our cardiac surgery center due to functional tricuspid regurgitation.Their tricuspids were stitched to suture annuloplasty or ring annuloplasty after left heart operation.According to the manners of operation, 146 cases were divided into suture annuloplasty group (n= 72) and ring annuloplasty group (n= 74).TA was evaluated in apical acoustic windows views using transthoracic echocardiography (TTE) and in mid-esophageal right ventricular (RV) inflow-outflow view by transesophageal echocardiography (TEE).The TA assessed by TTE and TEE was compared with actual measurement during the operation.ResultsOf the patients, there were 79 females and 67 males with the average age of (46.2 ± 14.7) years old.The mean left ventricular ejection fraction (LVEF) was 60.1%.The systolic pulmonary artery pressure was (44.9 ± 14.9)mmHg.There were 78 cases with mitral valve replacement or repair, 51 with aortic valve replacement, 62 with double valve replacement, and 17 with atrial septal defect (ASD) repair.There were no difference in the aorta block time, circulation bypass time, systolic pulmonary artery pressure and LVEF between the suture annuloplasty and the ring annuloplasty group.However, patients in the suture annuloplasty group were significantly older, and the cardiac operation of mitral replacement or repair and atrial septal defect repair were more frequent in the suture annuloplasty group.There were the more prevalence of severe TR and greater dilatation of TA in the patients of ring annuloplasty group when compared to suture annuloplasty group.No significant difference in the TA diameter between TEE and actual measurements during operation was found.However, diameter of TA measured by TTE was found to be significantly smaller than that by the direct measurement during operation.ConclusionTEE could provide more accurate measurements of tricuspid annulus.The TA diameter measured by TTE systematically underestimates the actual TA diameter.
Transesophageal echocardiography;Tricuspid annular;Functional tricuspid annuloplasty
尹立雪
R445.1;542.5+3
A
1672-6170(2017)05-0202-04
2017-03-22;
2017-07-30)
猜你喜欢
中国典型病例大全(2022年7期)2022-04-22
法人(2021年12期)2021-05-09
中国循环杂志(2021年1期)2021-02-04
中国循证心血管医学杂志(2017年11期)2017-01-12
中国心血管病研究(2017年8期)2017-01-10
腹腔镜外科杂志(2016年10期)2016-06-01
中国循环杂志(2015年10期)2015-12-24
中国循环杂志(2015年10期)2015-12-24
中国当代医药(2015年32期)2015-03-01
郑州大学学报(医学版)(2015年2期)2015-02-27
