声触诊组织定量在胰腺局灶性病变鉴别诊断中的初步应用
2017-05-09 18:05姜玉新李建初何蒙娜
中国医学科学院学报 2017年2期
韩 洁,吕 珂,姜玉新,戴 晴,李建初,何蒙娜,高 嫔
中国医学科学院 北京协和医学院 北京协和医院超声医学科,北京 100730
·论 著·
声触诊组织定量在胰腺局灶性病变鉴别诊断中的初步应用
韩 洁,吕 珂,姜玉新,戴 晴,李建初,何蒙娜,高 嫔
中国医学科学院 北京协和医学院 北京协和医院超声医学科,北京 100730
目的 探讨声触诊组织定量(VTQ)鉴别胰腺局灶性病变应用价值。方法 对51例胰腺占位患者行VTQ检查,分别获取病灶剪切波速(LSWV)、相邻胰腺实质剪切波速(PSWV)及剪切波速差值(DSWV)(DSWV=LSWV-PSWV),对照病理结果或临床诊断,评估LSWV、PSWV和DSWV在胰腺局灶性病变的鉴别诊断价值。结果 恶性组的LSWV和PSWV分别为(2.39±1.25) m/s(0.60~4.39 m/s)和(1.59±0.63) m/s (0.76~3.22 m/s);潜在恶性组的LSWV和PSWV分别为(1.92±1.07) m/s(0.79~4.00 m/s)和(1.43±0.41) m/s(0.80~2.23 m/s);良性组的LSWV和PSWV分别为(2.40±1.10) m/s (0.89~3.42 m/s)和(1.48±0.44) m/s (1.03~2.11 m/s);良、恶性组内LSWV和PSWV差异有统计学意义(P=0.029,P=0.005),潜在恶性组的LSWV和PSWV差异无统计学意义(P=0.087)。LSWV、PSWV和DSWV在3组间差异无统计学意义(P=0.401,P=0.638,P=0.625)。LSWV与病灶大小不相关(r=0.253,P>0.05);LSWV与感兴趣区深度呈负相关(r=-0.413,P<0.05)。结论 利用VTQ鉴别诊断胰腺局灶性病变的价值有待进一步的研究。
声触诊组织定量;剪切波速;胰腺占位;诊断
ActaAcadMedSin,2017,39(2):266-271
胰腺癌是最常见的胰腺原发性恶性肿瘤,其恶性度高,预后极差,5年总体生存率不超过5%。而且随着生活水平的提高、肥胖人群的增加及人口老龄化等原因,胰腺癌的发病率呈逐年上升趋势[1- 2],对人类的健康造成了极大的危害。常规超声是胰腺病变首选的影像学筛查手段,能够有效地发现胰腺占位性病变,但定性诊断困难,尤其胰腺癌和炎性病变的鉴别诊断。然而,病灶的定性诊断决定着临床治疗方案的制定,与疾病的预后息息相关。所以,胰腺病变良恶性的鉴别诊断研究具有重要的临床意义。超声弹性成像技术是通过分析病灶硬度的差异判断病灶性质,目前该术已广泛应用于甲状腺、乳腺及前列腺等浅表器官肿瘤的诊断,能够有效提高病变良恶性鉴别诊断特异性[3- 6]。声辐射力脉冲成像(acoustic radiation force impulse,ARFI)作为一种剪切波弹性成像技术,包括声触诊组织成像和声触诊组织定量(virtual touch tissue quantification,VTQ)。其中VTQ能对某一明确深度(≤8 cm)的解剖结构的组织硬度进行定量评价,使得通过经腹超声对腹膜后胰腺病变的硬度评估成为可能。目前,其在胰腺的应用研究主要集中在正常胰腺测值的建立及炎症纤维化方面[7- 12]。本研究主要探讨VTQ在胰腺局灶占位性病变的鉴别诊断价值。
对象和方法
对象 选取2014年1月至2015年1月因胰腺占位在北京协和医院行常规超声及VTQ检查的51例患者。男26例、女25例,平均年龄(50.5±14.1)岁(11~80岁),病灶最大径(4.7±2.0) cm(1.7~10.7 cm)。纳入标准:(1)常规超声能清晰显示病灶;(2)胰腺实性或以实性为主囊实性病灶,且病灶直径>1 cm;(3)患者签署知情同意书。排除标准:(1)病灶距体表位置>8 cm;(2)不能配合屏气的患者;(3)放化疗或支架置入术后患者;(4)胰管明显扩张伴胰腺实质萎缩者。
方法 采用Siemens Acuson S2000彩色多普勒超声诊断仪(Siemens,Mountain View,CA,USA),4C1凸阵探头,频率1.0~4.0 MHz,配备ARFI成像技术(Virtual TouchTMTissue Quantification package)。先行常规超声检查,选择病灶显示最佳切面,切换至VTQ模式,尽量保持取样线与角度<15°,以保持测量的标准化。分别将感兴趣区(region of interest,ROI)(10 mm×6 mm)置于病灶内及相邻的胰腺实质,“Update”一键测量时嘱受检者屏住呼吸,各连续成功测量5次。去除最大值、最小值后,取其平均值作为病灶的剪切波速值(lesional shear wave velocity,LSWV)和相邻胰腺实质的剪切波速值(parenchymal shear wave velocity,PSWV)。当速度显示为“X.XX”时,需重新计数5次测量。ROI的选取原则:病灶内ROI不能包含血管、胰胆管结构、坏死及出血囊性变区、钙化灶;相邻胰腺实质的ROI置于距病灶2~3 cm处,亦不能包括血管及胰胆管结构。剪切波速差值(difference shear wave velocity,DSWV)=LSWV-PSWV。所有检查均由同一名对超声弹性成像有经验的医师独立完成,以避免不同操作者对结果可能产生的影响。检查图像均以数字化格式存储于仪器硬盘中。
诊断标准 (1)对行外科手术治疗的患者,以手术切除标本的病理学诊断为诊断标准;(2)对未行手术治疗的患者,以穿刺细胞/组织学诊断为诊断标准;(3)对未行穿刺或穿刺细胞/组织学诊断阴性者,依据患者的症状、体征、病史、影像学(CT、磁共振成像、正电子发射计算机断层显像-CT等)特征、肿瘤标记物等作出临床诊断或至少6个月的临床随访排除恶性病变作为诊断标准。
统计学处理 采用SPSS version 20.0统计学软件,计量资料以均数±标准差表示。多组间的比较采用单因素方差分析(one way ANOV);符合正态分布的计量资料两个样本均数比较采用t检验;非正态分布的计量资料采用非参数检验;两变量之间的关系采用Pearson相关系数。P<0.05为差异有统计学意义。
结 果
病理或临床诊断结果 51例患者中,25例行手术切除病灶,14例行粗/细针穿刺活检术,12例为综合判断的临床诊断。最终诊断恶性病变27例(胰腺癌19例、神经内分泌癌1例、腺泡细胞癌1例、临床诊断恶性病变6例),潜在恶性病变17例(神经内分泌肿瘤6例、实性假乳头状瘤10例、临床诊断实性假乳头状瘤1例),良性病变7例(神经鞘瘤1例、腹腔结核1例、临床诊断自身免疫性胰腺炎2例、临床诊断肿块型胰腺炎1例、临床诊断良性病变2例)(图1、2)。
CEA:癌胚抗原
CEA: carcinoembryonic antigen
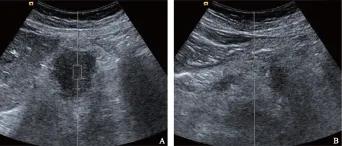
A.病灶的剪切波速均值为2.82 m/s,对应深度为5.0 cm;B.相邻胰腺实质的剪切波速均值为1.54 m/s,对应深度为3.9 cm
A. the mean shear wave velocity of pancreatic lesion was 2.82 m/s and the depth was 5.0 cm; B. the mean shear wave velocity of the surrounding pancreatic parenchyma was 1.54 m/s and the depth was 3.9 cm
图 1 58岁女性,左上腹不适1个月,于当地医院行腹部超声发现胰尾占位就诊,CA19- 9、CEA、CA242、CA72- 4均正常,行剖腹探查及腹壁结节活检术,术后病理提示低分化腺癌
Fig 1 A 58-year-old woman with left epigastric discomfort for 1 month. A mass in pancreatic tail was found by transabdominal ultrasound examination in local hospital. CA19- 9, CEA, CA242, and CA72- 4 levels were normal. Exploratory laparotomy and abdominal wall nodule biopsy were performed, and the postoperative pathology confirmed poorly differentiated adenocarcinoma

A.病灶的剪切波速均值为1.25 m/s,对应深度为6.7 cm;B.相邻胰腺实质剪切波速均值为1.60 m/s,对应深度为5.3 cm
A. the mean shear wave velocity of pancreatic lesion was 1.25 m/s and the depth was 6.7 cm; B. the mean shear wave velocity of the surrounding pancreatic parenchyma was 1.60 m/s and the depth was 5.3 cm
图 2 61岁女性,体检发现胰体占位就诊,CA19- 9、CEA、甲胎蛋白均正常,术后病理符合胰腺神经内分泌肿瘤
Fig 2 A 61-year-old woman with a mass in pancreatic body, which was found during health check-up. CA19- 9, CEA, and alpha fetal protein levels were normal. Postoperative pathology confirmed pancreatic neuroendocrine tumor
观察者内一致性 51例病灶的LSWV测量中,单次测量的组内相关系数(interclass correlation coefficient,ICC)为0.631(95%CI=0.516~0.741),5次测量均值的ICC为0.895(95%CI=0.842~0.935);对51例相邻胰腺实质的PSWV测量中,单次测量的ICC为0.571(95%CI=0.449~0.692),5次测量均值的ICC为0.869(95%CI=0.803~0.918)。
LSWV的影响因素 LSWV与病灶大小不相关(r=0.253,P>0.05);而LSWV与ROI深度呈负相关(r=-0.413,P<0.05)。
胰腺局灶性病变的剪切波速值 良性组和恶性组的LSWV与PSWV的差异有统计学意义(P=0.029,P=0.005);潜在恶性组的LSWV与PSWV的差异无统计学意义(P=0.087)。3组间的LSWV、PSWV及DSWV差异无统计学意义(P=0.401,P=0.638,P=0.625);胰腺癌与胰腺炎性病变(2例自身免疫性胰腺炎和1例肿块型胰腺炎)的LSWV、PSWV及DSWV差异无统计学意义(P=0.886,P=0.667,P=0.811);实性假乳头状瘤与神经内分泌肿瘤的LSWV、PSWV及DSWV差异无统计学意义(P=0.372,P=0.778,P=0.326)(表1)。
讨 论
ARFI测量的剪切波速反映了组织内在的固有性征,可以作为绝对的组织硬度的量化指标,无需考虑相邻胰腺实质的软硬度,从而可以利用剪切波速(shear wave velocity,SWV)在不同的患者间进行直接比较[13]。
ICC是评价定量资料中观察一致性的指标,介于0~1。ICC值越大,表明测量结果的可重复性越好,可信度越高。本研究SWV 5次测量均值的ICC高于单次测量的ICC,表明多次测量可提供更加可靠的SWV值。Goertz等[14]通过对36例正常受试者和18例健康对照组的研究,得出尽管胰腺位置靠近腹主动脉,但其观察者内的ARFI测值稳定性好。国内的一项210名健康志愿者的胰腺正常弹性值的测定研究也证实了胰腺SWV的稳定性与可靠性[8]。SWV的可靠性为VTQ临床应用提供了先决条件。
一项利用弹性成像模型进行的SWV影响因素研究显示,使用凸阵探头时,以取样线角度≤15°时,角度对SWV测值的影响较小[15]。本研究在测量时设置取样线角度<15°,以保证测量值的可靠。Hirche等[16]研究提出,绝大多数良、恶性胰腺占位的病灶均较相邻胰腺实质硬,所以弹性成像在胰腺病变良恶性鉴别方面价值有限。但本研究出现了病灶较相邻实质软的病例,通过后期图像复习发现,这些病灶的ROI位置一般较相邻实质ROI深。通过相关性分析显示SWV与ROI深度呈中等程度的负相关,这与文献[17]观点一致,并推测这可能与脉冲波在传播过程中衰减及剪切波的振幅减小相关。但文献[17]还指出在实质均一的胰腺中,以胰头、体、尾的SWV代表胰腺实质的硬度,其测值差异小于5%。另外,Goertz等[14]也得出SWV与测量深度不相关。
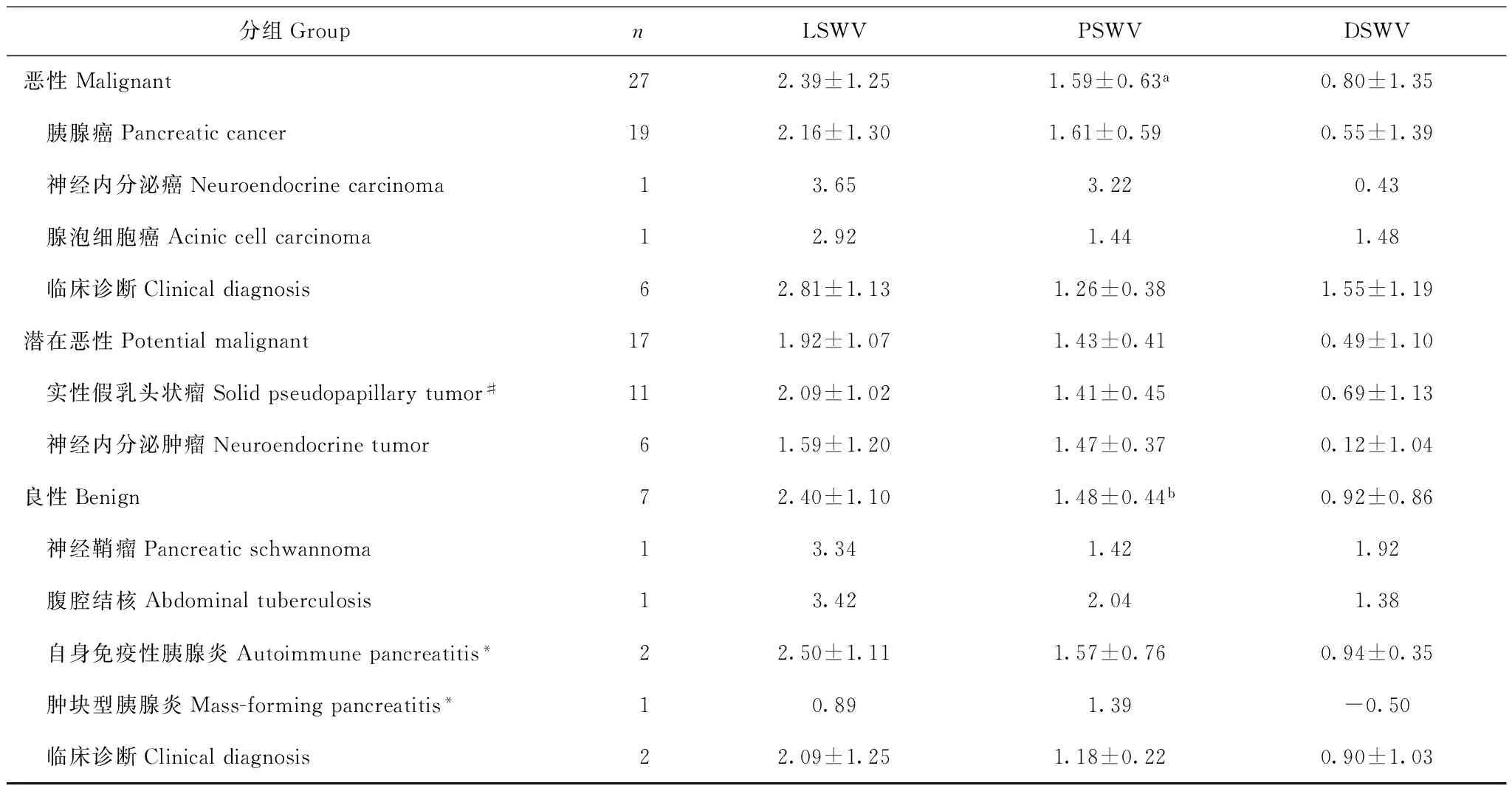
表 1 胰腺局灶性病变的LSWV、PSWV及DSWV均值(m/s)
LSWV:病灶剪切波速;PSWV:相邻胰腺实质剪切波速;DSWV:剪切波速差值;#:包含1例临床诊断实性假乳头状瘤;*:临床诊断结果;与LSWV比较,aP=0.005,bP=0.029
LSWV:lesional shear wave velocity;PSWV:parenchymal shear wave velocity;DSWV:difference shear wave velocity;#:including one clinical diagnostic solid pseudopapillary tumor;*:clinical diagnosis;aP=0.005,bP=0.029 compared with LSWV
目前,关于ARFI在胰腺的应用研究较少,主要是胰腺正常测值的建立和炎症纤维化的相关性研究。根据文献报道,正常胰腺实质的SWV为1.28~1.40 m/s[10- 12,14]。本研究相邻胰腺实质的SWV均值为1.52 m/s,其中恶性组为1.59 m/s,有高于潜在恶性组和良性组的1.43 m/s和1.48 m/s的趋势,但差异无统计学意义。有文献报道也支持胰腺癌患者的胰腺实质较正常胰腺实质硬[17- 19],并提出这可能与慢性胰腺炎症致癌途径学说相关[20]。
胰腺癌的肿瘤间质含有丰富的Ⅰ和Ⅳ型胶原以及纤连蛋白,相对其他胰腺病变质地硬韧,这为弹性成像的应用提供了生物学基础。Park等[21]对19例恶性病灶与8例炎性病灶的SWV的对比研究得出,良、恶性病变的SWV差异无统计学意义;而恶性病灶与周围胰腺实质的SWV差值明显高于良性病灶(P=0.011),并提出这可能因为良性组除病灶内发生纤维化,其相邻的胰腺实质同时发生纤维化改变,从而减小了两者间的硬度差值。但本研究结果显示胰腺癌与胰腺炎性病变的LSWV、PSWV及DSWV的差异均无统计学意义(P>0.05)。本研究3例炎性病变包括2例自身免疫性胰腺炎和1例肿块型胰腺炎,样本量较少;另外,因肿块型胰腺炎的病灶位置较深,测量的LSWV低于PSWV,也会对结果产生直接影响。与胰腺癌及胰腺炎性病变的纤维化不同,低度恶性的实性假乳头状瘤和神经内分泌肿瘤以细胞实性巢为主,而表现为质软的肿物,研究结果也显示恶性组的LSWV有高于潜在恶性组的趋势,但差异无统计学意义。但研究中纳入的1例神经内分泌癌的LSWV明显高于神经内分泌肿瘤组,而LSWV是否与神经内分泌肿瘤的分级存在相关性,则有待大样本的研究。
本研究的局限性在于:(1)本研究共纳入51例胰腺实性病灶,12例为临床诊断结果,样本量偏小;(2)未对病灶进行多点取样,SWV存在取样误差;(3)因为胰腺为腹膜后位器官,位置深在,多数情况下需对探头加压以达到最佳的图像显示效果,则很难对外力进行控制。
综上,声触诊组织定量利用SWV定量鉴别诊断胰腺局灶性病变的价值有待进一步研究。
[1]Tempero MA,Malafa MP,Behrman SW,et al. Pancreatic adenocarcinoma,version 2.2014:featured updates to the NCCN guidelines [J]. J Natl Compr Canc Netw,2014,12(8):1083- 1093.
[2]He Y,Zheng R,Li D,et al. Pancreatic cancer incidence and mortality patterns in China,2011 [J]. Chin J Cancer Res,2015,27(1):29- 37.
[3]Balleyguier C,Ciolovan L,Ammari S,et al. Breast elastography:the technical process and its applications [J]. Diagn Interv Imaging,2013,94(5):503- 513.
[4]Correas JM,Tissier AM,Khairoune A,et al. Prostate cancer:diagnostic performance of real-time shear-wave elastography [J]. Radiology,2014,275(1):280- 289.
[5]Dighe M,Luo S,Cuevas C,et al. Efficacy of thyroid ultrasound elastography in differential diagnosis of small thyroid nodules [J]. Eur J Radiol,2013,82(6):274- 280.
[6]Dudea SM,Botar-Jid C. Ultrasound elastography in thyroid disease [J]. Med Ultrason,2015,17(1):74- 96.
[7]Yashima Y,Sasahira N,Isayama H,et al. Acoustic radiation force impulse elastography for noninvasive assessment of chronic pancreatitis [J]. J Gastroenterol,2012,47(4):427- 432.
[8]谢娟,吴蓉,姚明华. 声触诊组织定量技术测量胰腺弹性的初步研究 [J]. 同济大学学报(医学版),2012,33(6):90- 94.
[9]Gallotti A,D’Onofrio M,Pozzi Mucelli R. Acoustic radiation force impulse (ARFI) technique in ultrasound with virtual touch tissue quantification of the upper abdomen [J]. Radiol Med,2010,115(6):889- 897.
[10]Mateen MA,Muheet KA,Mohan RJ. et al. Evaluation of ultrasound based acoustic radiation force impulse (ARFI) and eSie touch sonoelastography for diagnosis of inflammatory pancreatic diseases [J]. JOP,2012,13(1):36- 44.
[11]Nightingale K,Soo MS,Nightingale R. et al. Acoustic radiation force impulse imaging:invivodemonstration of clinical feasibility [J]. Ultrasound Med Biol,2002,28(2):227- 235.
[12]Fahey BJ,Nightingale KR,Nelson RC. et al. Acoustic radiation force impulse imaging of the abdomen:demonstration of feasibility and utility [J]. Ultrasound Med Biol,2005,31(9):1185- 1198.
[13]Lupsor M,Badea R,Stefanescu H. et al. Performance of a new elastographic method (ARFI technology) compared to unidimensional transient elastography in the noninvasive assessment of chronic hepatitis C. Preliminary results [J]. J Gastrointestin Liver Dis,2009,18(3):303- 310.
[14]Goertz RS,Amann K,Heide R. et al. An abdominal and thyroid status with acoustic radiation force impulse elastometry-a feasibility study:acoustic radiation force impulse elastometry of human organs [J]. Eur J Radiol,2011,80(3):226- 230.
[15]杨龙,袁建军,王绮,等. 超声弹性成像测量剪切波速度的影响因素[J]. 中国医学影像学杂志,2014,22(9):697- 700.
[16]Hirche TO,Ignee A,Barreiros AP. et al. Indications and limitations of endoscopic ultrasound elastography for evaluation of focal pancreatic lesions [J]. Endoscopy,2008,40(11):910- 917.
[17]Kawada N,Tanaka S,Uehara H. et al. Potential use of point shear wave elastography for the pancreas:a single center prospective study [J]. Eur J Radiol,2014,83(4):620- 624.
[18]Harada N,Ishizawa T,Inoue Y. et al. Acoustic radiation force impulse imaging of the pancreas for estimation of pathologic fibrosis and risk of postoperative pancreatic fistula [J]. J Am Coll Surg,2014,219(5):887- 894.
[19]Lee TK,Kang CM,Park MS, et al. Prediction of postoperative pancreatic fistulas after pancreatectomy:assessment with acoustic radiation force impulse elastography [J]. J Ultrasound Med,2014,33(5):781- 786.
[20]DiMagno EP,Reber HA,Tempero MA. AGA technical review on the epidemiology,diagnosis,and treatment of pancreatic ductal adenocarcinoma. American Gastroenterological Association [J]. Gastroenterology,1999,117(6):1464- 1484.
[21]Park MK,Jo J,Kwon H. et al. Usefulness of acoustic radiation force impulse elastography in the differential diagnosis of benign and malignant solid pancreatic lesions [J]. Ultrasonography,2014,33(1):26- 33.
Initial Experience in the Application of Virtual Touch Tissue Quantification in the Differential Diagnosis of Focal Pancreatic Lesions
HAN Jie,LÜ Ke,JIANG Yuxin,DAI Qing,LI Jianchu,HE Mengna,GAO Pin
Department of Ultrasound,PUMC Hospital,CAMS and PUMC,Beijing 100730,China
Corresponding author:JIANG Yuxin Tel:010- 69155491,E-mail:yuxinjiangxh@163.com
Objective To explore the potential value of the virtual touch tissue quantification (VTQ) in the differential diagnosis of focal pancreatic lesions. Methods Totally 51 patients with focal pancreatic lesions underwent the quantitative analysis by VTQ. Based on the pathologic or clinical diagnosis,the VTQ values including lesional shear wave velocity (LSWV),parenchymal shear wave velocity (PSWV),and difference shear wave velocity (DSWV)(DSWV=LSWV-PSWV) were compared between the lesions and background parenchyma. Results The mean LSWV and PSWV were (2.39±1.25) m/s(0.60- 4.39 m/s) and (1.59±0.63) m/s (0.76- 3.22 m/s) in malignant group,(1.92±1.07) m/s(0.79- 4.00 m/s) and (1.43±0.41) m/s(0.80- 2.23 m/s) in potentially malignant group,and (2.40±1.10) m/s (0.89- 3.42 m/s) and (1.48±0.44) m/s (1.03- 2.11 m/s) in benign group. There were statistically significant difference between LSWV and PSWV in bengin and malignant group (P=0.029,P=0.005),while no statistical significance in potential malignant group (P=0.087). However,LSWV,PSWV,and DSWV showed no significant difference among these three groups (P=0.401,P=0.638,P=0.625,respectively). LSWV was not significantly associated with the tumor size (r=0.253,P>0.05) but had negative correlation with the depth of region of interest (r=-0.413,P<0.05). Conclusion VTQ may be valuable in the differential diagnosis of focal pancreatic lesions,although further research is still required.
virtual touch tissue quantification;shear wave velocity;pancreatic lesion;diagnosis
公益性行业基金(201402001) Supported by the Foundation of Non-profit Public Service (201402001)
姜玉新 电话:010- 69155491,电子邮件:yuxinjiangxh@163.com
R576;R445.1
A
1000- 503X(2017)02- 0266- 06
10.3881/j.issn.1000- 503X.2017.02.017
2016- 01- 20)
猜你喜欢
山西建筑(2022年21期)2022-10-28
大地测量与地球动力学(2022年10期)2022-10-10
家庭影院技术(2021年10期)2021-11-20
国际医学放射学杂志(2021年4期)2021-08-05
铁道建筑技术(2021年4期)2021-07-21
影像研究与医学应用(2021年2期)2021-03-09
煤矿安全(2021年1期)2021-02-05
中国现代医药杂志(2020年12期)2020-02-06
活力(2019年19期)2020-01-06
当代陕西(2019年14期)2019-08-26