Clinical Engineering Benchmarking Comparison Between Zhejiang Province and American Hospitals
2017-01-06 09:13BinsengWangKunZhengJingyiFeng
中国医疗设备 2016年7期
Binseng Wang, Kun Zheng, Jing-yi Feng
1.Sundance Solutions, White Plains, NY 10601, USA & Milwaukee School of Engineering, Milwaukee, WI 53203-2926, USA; 2.Clinical Engineering Department, School of Medicine, Children’s Hospital of Zhejiang University, Hangzhou 310003, Zhejiang Province, China; 3.Department of Clinical Engineering, School of Medicine, First Affiliated Hospital of Zhejiang University, Hangzhou 310003, Zhejiang Province, China
Clinical Engineering Benchmarking Comparison Between Zhejiang Province and American Hospitals
Binseng Wang1, Kun Zheng2, Jing-yi Feng3
1.Sundance Solutions, White Plains, NY 10601, USA & Milwaukee School of Engineering, Milwaukee, WI 53203-2926, USA; 2.Clinical Engineering Department, School of Medicine, Children’s Hospital of Zhejiang University, Hangzhou 310003, Zhejiang Province, China; 3.Department of Clinical Engineering, School of Medicine, First Affiliated Hospital of Zhejiang University, Hangzhou 310003, Zhejiang Province, China
Clinical engineering (CE) has evolved rapidly over the last 25 years in China. Among the 34 provincial-level administrative units within China, the Zhejiang Province is one of the most advanced in terms of healthcare technology maintenance and management. In order to determine Zhejiang’s current stage of development and opportunities for further improvement, a comparison of the performance of its CE departments was made against hospitals in the USA. Data were collected from 21 Zhejiang hospitals and compared to those from 270 acute-care hospitals in USA collected by Truven Health Analytics. The benchmarking comparison was made in three categories: operational, fnancial, and productivity. Within the operational category, the following metrics were compared: equipment inventory size/operating beds, annual repairs/inventory size, and annual scheduled maintenance/inventory size. Within the Financial category, the following metrics were compared: total CE expense/operating beds and total CE expense/total hospital expense. Within the Productivity category, the following metrics were compared: total CE full-time equivalent (FTE)/inventory size and total CE FTE/ total hospital expense. These comparisons showed that: (1) While the equipment inventory in Zhejiang tends to be much smaller than USA for hospitals of comparable amount of operating beds, the numbers of repairs and scheduled maintenance per inventory size are similar; (2) The total CE expense/total hospital expense ratio is around 1% in both Zhejiang and USA; however, the total CE expense/operating beds and total CE expense/ cost of equipment inventory are signifcantly lower in Zhejiang than USA; (3) The FTE amount in Zhejiang is significantly higher than in USA relative to both inventory size and total hospital operating expense, but signifcantly lower relative to the number of operating beds. The fact that repairs and scheduled maintenance are similar in Zhejiang and USA shows that CE leaders are managing equipment in comparable manner. Most of the differences found in the comparisons were traced to a few factors. First, the average length of stay in China is substantially higher than USA, which explains why hospitals in Zhejiang tend to have more operating beds but fewer pieces of equipment. Second, labor cost is signifcantly lower in China than USA, thus allowing Zhejiang hospitals to employ more workers than their American counterparts. Third, there is significantly difference in the cost of living between China and USA; Finally, being public entities Chinese hospitals are managed and operated in a different manner than American hospitals, which are mostly private, albeit nonproft organizations. Nonetheless, it is interesting to note that hospitals in both areas spend roughly 1% of their total expenditure for CE. The results suggest that CE in Zhejiang is comparable to USA in terms of managerial excellence but there could be some room for improvement in fnancial management and productivity.
clinical engineering; performance benchmarking; Zhejiang province hospitals; American hospitals
1 INTRODUCTION
Clinical engineering (CE) is the engineering specialty devoted to the application of engineering principles and expertise to the management and maintenance of medical devices used in clinical settings. While some CE professionals work in academia, consulting, government, or device production, the majority work inside hospitals due to the large concentration of devices there.
Benchmarking is a process used in many industries to measure the performance of a particular organization and compare it to similar organizations. Using benchmarking results, an organization can improve its performance by determining specifi copportunities for improvement and learning how other organizations are achieving higher levels of performance.
CE benchmarking efforts started in the late 1980’s and 1990’s[1-5]but remained dormant for many years due to a lack of consensus on performance metrics and wide acceptance[6-8]. Renewed interests appeared around 2005 and several studies have been published since then[9-14]. Currently, at least three organizations in the USA are offering commercial services in CE benchmarking[15-17].
CE evolved rapidly in China in the last 25 years due to government attention and, especially, commitment and hard work of Chinese CE leaders. Among the 34 provincial-level administrative units within China, the Zhejiang province is certainly one of the most advanced and cohesive in terms of CE. In order to determine Zhejiang’s current stage of development and opportunities for further improvement, a comparison of the performance of its CE departments was made against acute-care hospitals in USA.
This paper provides the results of CE performance benchmarking in three categories: operational, financial, and productivity, and, to the best of our knowledge, it is the first large scale benchmarking comparison between Chinese and American CE Departments.
2 MATERIALS AND METHODS
Data from Zhejiang province were collected from 21 hospitals, including both Western and Traditional Chinese medicine types, on a voluntary basis. For confidentiality reasons, the names of the hospitals are not provided in this article but the results of the comparison were given back to the respective CE leaders for their own use, while their peers’identities were kept confdential.
Data from 270 acute-care American hospitals were obtained from Truven Health Analytics[15]for the full calendar year of 2013. All the data were self-reported with no attempt to verify their accuracy. The identity of these hospitals were kept confdential by Truven except for their teaching characteristics.
Analyses were performed using Microsoft Excel®spreadsheet and its built-in tools. It should be emphasized that the plots shown inResultsuse logarithmic scales in order to accommodate the large range of values. Furthermore, the lines drawn on those fgures were not based on statistical calculations but purely on authors’ best guesstimates, as the presence of unreliable data—from both countries—would yield unrealistic results.
3 RESULTS
3.1 National comparisons
Due to the wide differences in culture, economy, and healthcare provision, all benchmarking comparisons must be made taking into consideration the fundamental differences between China and USA. Table 1 summarizes the key economic and health metrics of these two countries.
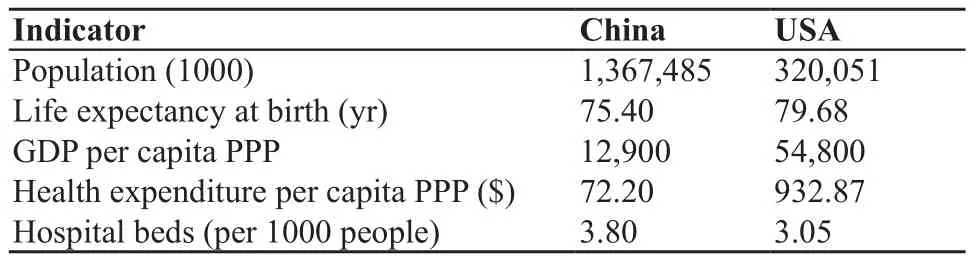
Table 1 Comparison of key economic and health statistics between China and USA
Figure 1A shows the total patient daysvstotal patient discharges. It is clear that the average length of stay (ALOS) in China is signifcantly higher than USA. Figure 1B compares the amount of medical equipment (defned as reusable medical devices with unit value above US $1000)vsthe number of operating—or staffed—beds (i.e., beds actually usable considering personnel and other resources available). Figure 1C and D compare the total hospital operating expensevsthe number of operating beds and the total number of patient discharges, respectively.
3.2 Operational benchmarking
Figure 2 compares the amount of repairs and scheduled maintenance events as a function of the number of pieces of medical equipment in panels A and B, respectively.
3.3 Financial benchmarking
Figure 3 compares the total CE expensesvsthe number of operating beds and the total hospital operating expenses in panelsA and B, respectively. The total CE expenses includes wages and benefts, maintenance supplies, replacement parts, service contracts, training, travel and entertainment, and other miscellaneous expenses. The only costs not included are those related to infrastructure,i.e., building (office and shop space), utilities (electricity, water, telephone,etc.), and housekeeping. The total hospital operating expenses includes the same expense categories for all departments, as well as all those related to infrastructure.
Among the American hospitals, several were classified as “questionable” in terms of their total CE expenses because their reported values were substantially lower than the rest and investigation showed that they probably did not include all CE expenses, notably the service contracts paid directly by the clinical departments (e.g., CT and MRI service contracts paid by the imaging departments)[14].The classifcation criteria adopted was whenever the CE labor expense exceeds 85% of the total CE expense.
3.4 Productivity benchmarking
Figure 4 compares the total number of CE full-time equivalent (FTE) workersvsthe number of pieces of medical equipment and the total hospital operating expenses in panels A and B, respectively.
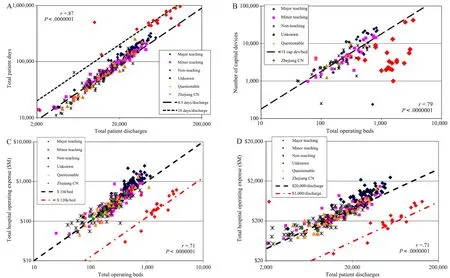
Figure 1 National comparisons. A: Total patient daysvstotal patient discharges; B: Amount of medical equipmentvsthe number of operating—or staffed—beds; C: Total hospital operating expensevsthe number of operating beds; D: Total hospital operating expensevsthe total number of patient discharges.
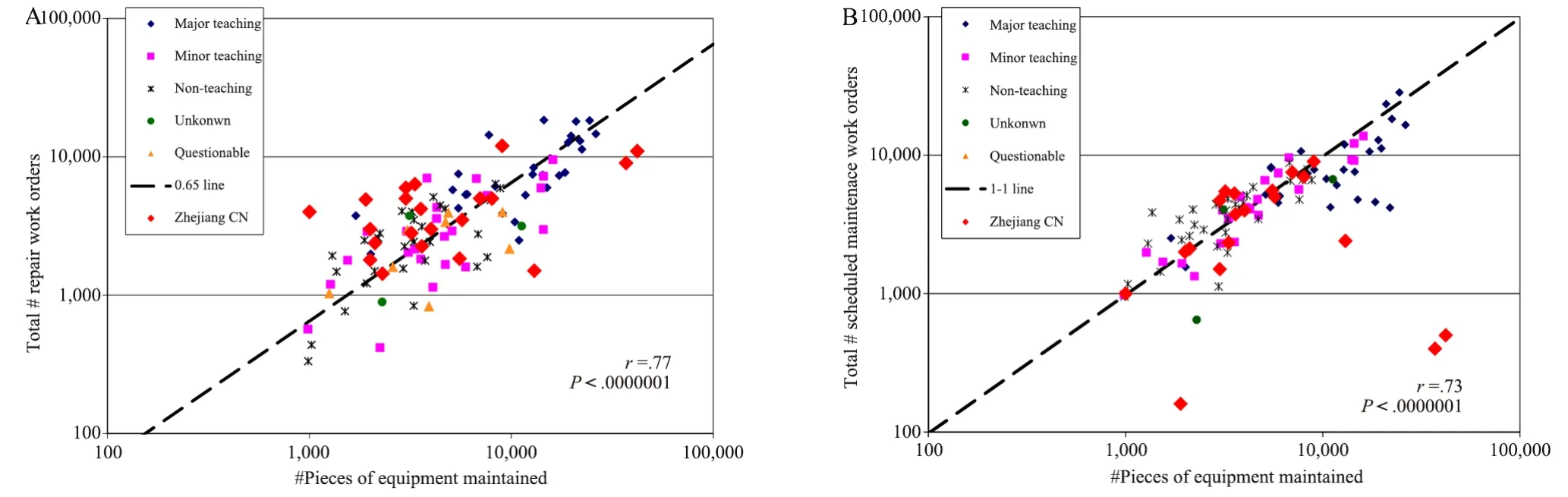
Figure 2 Operational benchmarking. A: Total number of repairsvsthe number of pieces of medical equipment; B: Total number of scheduled maintenance eventsvsthe number of pieces of medical equipment.
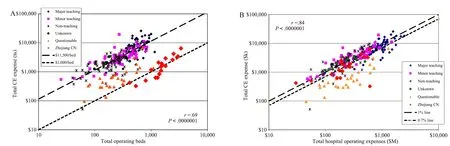
Figure 3 Financial benchmarking. A: Total clinical engineering (CE) expensevsthe number of operating beds. See text for explanation of the American hospitals classifed as “questionable” due to their lower than expected reported total CE expense; B: Total CE expensevsthe total hospital operating expenses. See text for explanation of the American hospitals classifed as “questionable” due to their lower than expected reported total CE expense.
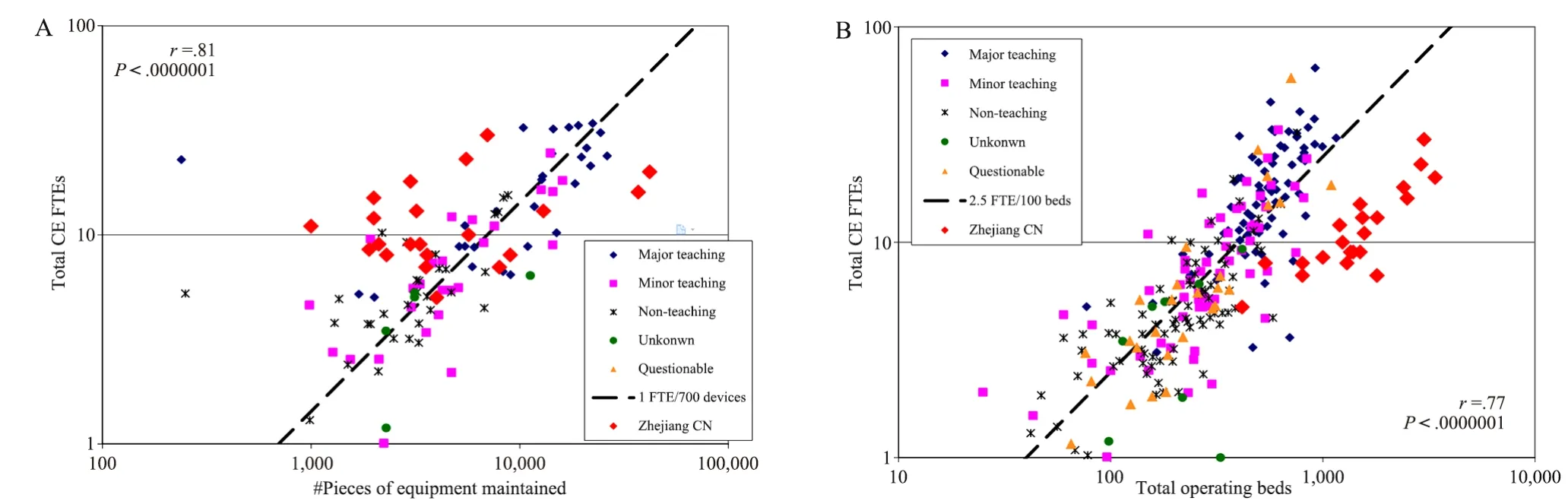
Figure 4 Productivity benchmarking. A: Total clinical engineering (CE) full-time equivalent (FTE)vsquantity of medical equipment; B: Total CE FTEvsthe total hospital operating beds.
4 DISCUSSION
From Figure 1A, it is clear that the average length of stay (ALOS) in China is more than double of that in the USA. This fact explains why most of the Chinese hospitals have many more beds than American counter parts (Figure 1B). However, only some Chinese hospitals have comparable amount of medical equipment, while most of them have fewer per bed.
Figure 1C and D show the total hospital operating expenses with respect to both number of operating beds and patient discharges is much lower in China than USA, by a factor of about 8.3 and 6.7, respectively. This large difference cannot be explained only by currency exchange rate, as the purchasing power parity (PPP) factor is only 0.6 per the World Bank[19]. It is likely that this difference is due to a combination of several factors, including gross domestic product (GDP), labor cost, and health care reimbursement and payment methods.
Focusing on CE activities, Figure 2 shows the number of repairs and scheduled maintenance activities per piece of equipment are comparable in Zhejiang and USA. In terms of fnancial comparison, Zhejiang hospitals’ total CE expenditure is substantially less than their American counterparts per operating bed by a factor of approximately 11.5 as shown on Figure 3A. However, with reference to the respective hospital’s total operating expense, both Zhejiang and American CE department expenses are around 1%, with perhaps approximately 30% lower expense in the former, again probably due to the combination of factors mentioned above.
The relationship of total CE FTEs with respect to quantity of medical equipment and total operating beds is quite different between Zhejiang and American hospitals. Since most of the former have fewer pieces of equipment, one would expect fewer FTEs needed; however, the much lower labor cost in China apparently has motivated Zhejiang hospitals to hire more CE staff. The right shift of Zhejiang data points in Figure 4B is a consequence of the much higher amount of beds due to higher ALOS as mentioned above.
5 CONCLUSION
While there are clear differences in the fnancial comparisons due to a variety of factors, the operational comparisons show Zhejiang CE Departments are operating at comparable levels toAmerican ones. The productivity, as measured by the amount of CE FTEs, suggests that there could be some opportunities for improvement.
These results confrm that CE in China, particularly in the Zhejiang province, has reached a quite high level of excellence due to the impressive dedication and hard work of their CE leaders. Other emerging countries would do well to learn from China how to advance CE in their own countries.
6 ACKNOWLEDGMENTS
The authors wish to acknowledge the valuable contribution of Zhejiang CE leaders who contributed data to this study.
[1] Furst E.Productivity and cost effectiveness of clinical engineering.J Clin Eng,1986,11:105-113.
[2] David Y,Rohe D.Clinical engineering program productivity and measurements.J Clin Eng,1986,11:435-443.
[3] Frize M.Results of an international survey of clinical engineering departments.Part 1- Role,functional involvement and recognition.Med Biol Eng Comput,1990,28:153-159.
[4] Frize M.Results of an international survey of clinical engineering departments.Part 2–Budgets,staffng,resources and fnncial strategies.Med Biol Eng Comput,1990,28:160-165.
[5] Cohen T,Bakuzonics C,Friedman S,et al.Benchmarking indicators for medical equipment repair and maintenance.Biomed Instr Technol,1995,29:308-321.
[6] Johnston GI.Are productivity and cost-effectiveness comparisons between in-house clinical engineering departments possible or useful?J Clin Eng,1987,12:153-158.
[7] Mahachek AR.Benchmarking is for benchwarmers.Biomed Instr Technol,1996,30:372-373.
[8] Stiefel R.Clinical engineering cannot do benchmarking.Biomed Instr Technol,1997,31:286-288.
[9] Wang B,Eliason RW,Vanderzee SC.Global Failure Rate:A promising medical equipment management outcome benchmark.J Clin Eng,2006,31:145-151.
[10] Wang B,Eliason RW,Richards SM,et al.Clinical Engineering Benchmarking, Presented at the 29th Canadian Medical and Biological Engineering Conference,Vancouver,BC,Canada, 2006.
[11] Maddock KE.Glass is half full.Biomed Instr Technol,2006, 40:328.
[12] Wang B,Eliason RW,Richards SM,et al.Clinical Engineering Benchmarking-An Analysis of American Acute Care Hospitals.J Clin Eng,2008,33:24-37.
[13] Wang B,Eliason RW,Richards S,et al.Financial Impact of Medical Technology.IEEE Eng Med Biol,2008,27(4):80-85.
[14] Wang B,Rui T,Fedele J,et al.Clinical Engineering Productivity and Staffing Revisited: How should it be measured and how can it be used?J Clin Eng,2012,37:135-145.
[15] Truven Health Analytics,Action OI.Available from:http:// truvenhealth.com/your-healthcare-focus/hospital-managementdecisions/actionoi,accessed 7/29/2015.
[16] AAMI Benchmarking Solutions.Available from:http://www.aami. org/productspublications/content.aspx?ItemNumber=911,accessed 7/29/2015.
[17] ECRI Biomedical Benchmark.Available from:https://www.ecri.org/ components/BiomedicalbenchMark/Pages/default.aspx,accessed 7/29/2015.
[18] Central Intelligence Agency,The World Factbook Available from:https://www.cia.gov/library/publications/the-worldfactbook/rankorder/2225rank.html,accessed 7/29/2015.
[19] The World Bank,Price level ratio of PPP conversion factor (GDP) to market exchange rate.Available form:http:// data.worldbank.org/indicator/PA.NUS.PPPC.RF,accessed 7/29/2015.
专栏——能谱CT的临床应用
编者按:传统CT虽能产生清晰的解剖图像,但当两种以上不同物质呈现相同密度时便无法区分。科学家们进行了40余年CT能谱成像的相关研究,能谱CT已作为一项新的成像技术展现在我们面前,它以瞬时kVp(80/140)切换和探测器为核心技术,进行数据空间的吸收投影数据到物质密度投影数据的转换,从而在准确的硬化效果校正的基础上得到准确的能谱成像。CT能谱成像已经在全身各系统病变的检查中获得了广泛的应用,并在临床和基础研究方面取得了可喜的成果。在本期的系列文章中,我们主要对CT能谱成像的临床应用进行了综述和分析,介绍了CT能谱成像在人体各部位的临床应用。

栏目主编:石明国(第四军医大学西京医院)
石明国,毕业于西安交通大学,硕士学位。现任第四军医大学西京医院医学影像学教研室主任、教授。兼山东泰山医学院教授、硕士生导师。荣立三等功2次,2012年1月获国防服役金质奖章。多次被评为陕西省医学会先进个人。中华医学会影像技术分会第六届委员会主任委员、中国医学装备协会常务理事、中国医学装备协会CT工程技术专业委员会主任委员、中国人民解放军医学影像技术专业委员会主任委员、陕西省医学会医学影像技术学会名誉主任委员,中华医学科技奖评审委员会委员。先后受聘为中华放射学杂志副总编辑、实用放射学、中华现代影像学、医疗卫生装备、生物医学工程与临床、现代医用影像学等10多部杂志编委、常务编委、副主编。承担国家九五攻关项目、国家自然科学基金等课题研究,获陕西省科学技术二等奖两项,全军科技进步奖5项,国家发明专利3项。主编教材及专著10部,参编多部。其中1995年主编全国首部《实用CT影像技术学》,获优秀科技图书一等奖,被选为全国大型设备CT上岗培训教材。主编十一五国家级规划教材《医学影像设备学》,高等教育出版社出版;主编《医学影像设备质量控制管理学》、《放射师临床工作指南》、《全国大型医用设备使用人员业务考评教材》、国家卫生和计划生育委员会及全国高等医药教材建设研究会“十三五”规划教材《医学影像设备学》等多部教材和专著,人民卫生出版社出版;在各类专业杂志发表论文130余篇。
R197.39 [Document code] A
10.3969/j.issn.1674-1633.2016.07.001
1674-1633(2016)07-0001-05
Binseng Wang, ScD, CCE, FAIMBE, FACCE, Sundance Solutions, 79 Primrose Street, White Plains, NY 10601, USA.
E-mail: binseng@alum.mit.edu
猜你喜欢
放射学实践(2022年11期)2022-11-22
吉林中医药(2022年10期)2022-10-21
吉林中医药(2022年9期)2022-09-23
吉林中医药(2022年8期)2022-08-25
中国临床医学影像杂志(2022年2期)2022-05-25
国际医学放射学杂志(2021年6期)2021-12-08
放射学实践(2021年8期)2021-08-23
放射学实践(2021年6期)2021-06-21
中国临床医学影像杂志(2019年5期)2019-08-27
中国CT和MRI杂志(2019年4期)2019-04-17