
特应性皮炎患者血清维生素D检测及其临床意义
2016-11-06 03:05栾红丁洁刘义华陈双峰张颖新
中华皮肤科杂志 2016年9期
栾红 丁洁 刘义华 陈双峰 张颖新
252000 山东省聊城市人民医院皮肤科(栾红),中心实验室(丁洁、刘义华、陈双峰、张颖新)
特应性皮炎患者血清维生素D检测及其临床意义
栾红 丁洁 刘义华 陈双峰 张颖新
252000 山东省聊城市人民医院皮肤科(栾红),中心实验室(丁洁、刘义华、陈双峰、张颖新)
目的检测特应性皮炎(AD)患者血清中维生素D(VitD)、总免疫球蛋白E(tIgE)、白细胞介素4(IL⁃4)、IL⁃6水平,评价VitD与AD患者病情严重程度的关系及其在AD发病中炎症与免疫调节中的作用。方法采集37例AD组和30例对照组外周血,检测血清VitD、tIgE、IL⁃4、IL⁃6水平,通过SCORAD评分评估AD患者病情严重程度。采用t检验或U检验分析组间差异,采用χ2检验比较VitD缺乏、不足与充足患者比例,采用Pearson或Spearman相关进行各组间的相关性分析。结果AD组血清VitD水平[(24.77±9.29)μg/L]低于对照组[(28.98±6.87)μg/L,t=2.015,P=0.048],tIgE水平[137.68(37.59~414.53)IU/ml]高于对照组[45.16(14.56 ~112.12)IU/ml,Z=-3.399,P=0.001],IL⁃4水平[(8.86±4.83)ng/L]高于对照组[(4.78±3.07)ng/L,t=4.147,P< 0.001],IL⁃6水平[6.53(3.99~15.30)ng/L]高于对照组[4.58(2.85~8.17)ng/L,Z=-2.173,P=0.030]。AD组SCORAD评分与血清VitD水平负相关(r=-0.505,P=0.001),与tIgE、IL⁃4水平正相关(r值分别为0.531、0.519,P值均为0.001),与IL⁃6无相关性(r=-0.139,P=0.411)。AD组与对照组相比,VitD缺乏、不足与充足患者比例差异有统计学意义,χ2=8.762,P=0.013。VitD缺乏患者血清tIgE[2846.87(319.02~7300.00)IU/ml]与IL⁃4水平[(16.37±2.05)ng/L]分别高于VitD不足[110.07(26.20~501.48)IU/ml,P=0.045;(8.28±4.48)ng/L,P=0.011]和VitD充足患者[123.93(91.61~273.68)IU/ml,P=0.024;(8.00±4.63)ng/L,P=0.041]。VitD缺乏患者IL⁃6水平[15.10(8.49~ 30.72)ng/L]高于充足[6.22(4.47~ 9.47)ng/L,P=0.011]。结论AD患者存在VitD缺乏或不足,VitD缺乏与高水平tIgE、IL⁃4、IL⁃6有关,且AD的严重程度与tIgE、IL⁃6升高及VitD降低关系密切。
皮炎,特应性;维生素D;免疫球蛋白E;白细胞介素4;白细胞介素6;疾病严重程度指数
目前特应性皮炎(AD)的病因尚不明确,包括遗传易感性、环境因素以及免疫因素的相互作用等,免疫平衡失调尤其是Th1和Th2比例失衡在AD的发病过程中起重要作用[1]。近年来研究表明,维生素D(VitD)作为一种类固醇激素,不仅在骨、磷代谢中发挥重要作用,而且对机体具有重要的抗感染和免疫调节作用[2⁃3],且与AD、银屑病、白癜风等多种皮肤病相关[4]。我们通过检测AD患者血清中VitD、总免疫球蛋白E(tIgE)、白细胞介素4(IL⁃4)、IL⁃6的水平,评估各指标与AD病情严重程度指数SCORAD评分间的关系,了解VitD在AD中的免疫调节作用,探讨其辅助治疗的可能性。
对象与方法
一、对象
我院2012—2014年门诊AD患者。入选标准:①诊断均符合Williams 1994年制订的标准[5];②病程至少在1年以上,而且反复发作。排除标准:①合并其他慢性疾病如高血压、糖尿病、甲状旁腺功能亢进症或减退症;②合并急慢性感染和肿瘤性疾病等;③3个月曾接受VitD类似物如阿法骨化醇、骨化三醇、维D钙咀嚼片等治疗。共入选37例患者,其中男17例,女20例,年龄[中位年龄20.00(四分位67.50~8.00)]岁,SCORAD评分23.94±10.76。同时选30例健康体检者作为对照组,其中男14例,女16例,年龄[中位年龄24.00(四分位54.00~11.00)]岁,均无过敏性疾病史及其他特殊疾病史,体检无异常发现,近2个月内无明显感染史。AD组和对照组年龄、性别差异无统计学意义(均P>0.05)。本研究通过山东省聊城市人民医院医学伦理委员会批准,患者均签署知情同意书。
二、试剂与方法
1.标本采集:采集空腹静脉血3 ml,1 600×g离心5 min,分离血清至-70℃贮存。
2.血清VitD、tIgE、IL⁃6检测:将血清恢复至室温加至样品管,血清VitD用Liaison化学发光分析仪检测,试剂为美国DiaSorin公司生产的25⁃羟基总VitD3定量测定试剂盒,根据文献[6]以及试剂盒推荐参考值范围将VitD水平划分:缺乏为<10 μg/L、不足为10~29 μg/L、充足为30~100 μg/L。血清tIgE采用Beckman Coulter UniCel DxI 800免疫化学分析仪检测,试剂为美国BeckmanCoulter公司产品;血清IL⁃6采用Roche Cobas e 601电化学发光仪检测,试剂由德国Roche Diagnostics GmbH提供。以上检测均采用化学发光技术的夹心酶免疫测试法,根据多点校准曲线计算各自浓度。
3.IL⁃4检测:利用美国RD Systems公司的ELISA试剂盒检测。按试剂盒说明书进行,最后在酶标仪内450 nm处读数,绘制标准曲线,计算血清IL⁃4浓度。
4.AD患者病情评价:根据欧洲AD评分标准SCORAD计分系统[7]进行评价,内容包括客观体征(皮损范围、皮损严重程度)和主观症状(瘙痒、睡眠影响程度),根据总分来确定疾病的严重程度,总分为0~103分。
5.统计学处理:采用SPSS 16.0进行数据分析。正态分布资料以±s描述,两组间比较采用两独立样本t检验,组间相关性应用Pearson相关分析;非正态资料以M(P25,P75)表示,两组比较采用Mann⁃WhitneyU检验,组间相关性应用Spearman相关分析。两组VitD缺乏、不足、充足者分布比较采用χ2检验。以P<0.05为差异有统计学意义。
结 果
一、AD组与对照组VitD、tIgE、细胞因子IL⁃6、IL⁃4水平比较
AD组血清VitD水平低于对照组,差异有统计学意义(P=0.048),但tIgE、IL⁃4、IL⁃6水平均高于对照组(P<0.01或0.05)。见表1。
二、AD组SCORAD评分与血清VitD、tIgE及IL⁃6、IL⁃4水平相关性分析
AD组SCORAD评分与血清VitD水平呈负相关(r=-0.505,P=0.001),与tIgE水平呈正相关(r=0.519,P=0.001),与IL⁃4水平呈正相关(r=0.531,P=0.001),与IL⁃6水平无相关性(r=-0.139,P=0.411),见图1。
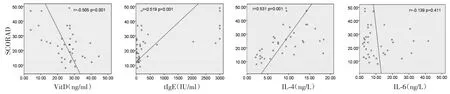
图1 特应性皮炎患者SCORAD评分与血清维生素D(VitD)、总IgE(tIgE)及白细胞介素4(IL⁃4)、IL⁃6水平的相关性
三、两组不同VitD水平分布
AD组37例中VitD缺乏3例(8.1%),不足26例(70.3%),充足8例(21.6%);对照组30例中VitD缺乏1例(3.3%),VitD不足12例(40%),VitD充足17例(56.7%),两组不同VitD水平比较,差异有统计学意义(χ2=8.762,P=0.013)。
四、VitD缺乏、不足与充足间tIgE、IL⁃4、IL⁃6水平比较
AD组中,VitD缺乏tIgE水平显著高于VitD不足(Z=-2.153,P=0.024)和VitD充足(Z=-2.008,P=0.045),VitD不足与充足相比,差异无统计学意义(Z=-0.203,P=0.839)。VitD缺乏IL⁃4水平显著高于VitD不足(Z=-2.544,P=0.011)和VitD充足(Z=-2.041,P=0.041),VitD不足与VitD充足相比差异无统计学意义(Z=-0.284,P=0.776)。VitD缺乏IL⁃6水平显著高于VitD充足(Z=-2.046,P=0.041),但VitD不足与缺乏(Z=-1.218,P=0.223)或充足(Z=-0.102,P=0.919)相比,差异均无统计学意义。
对照组中,VitD不足tIgE水平、IL⁃4水平、IL⁃6水平与充足相比差异均无统计学意义(Z=-0.699,P=0.485;Z=-0.940,P=0.347;Z=-0.546,P=0.585)。见表1。
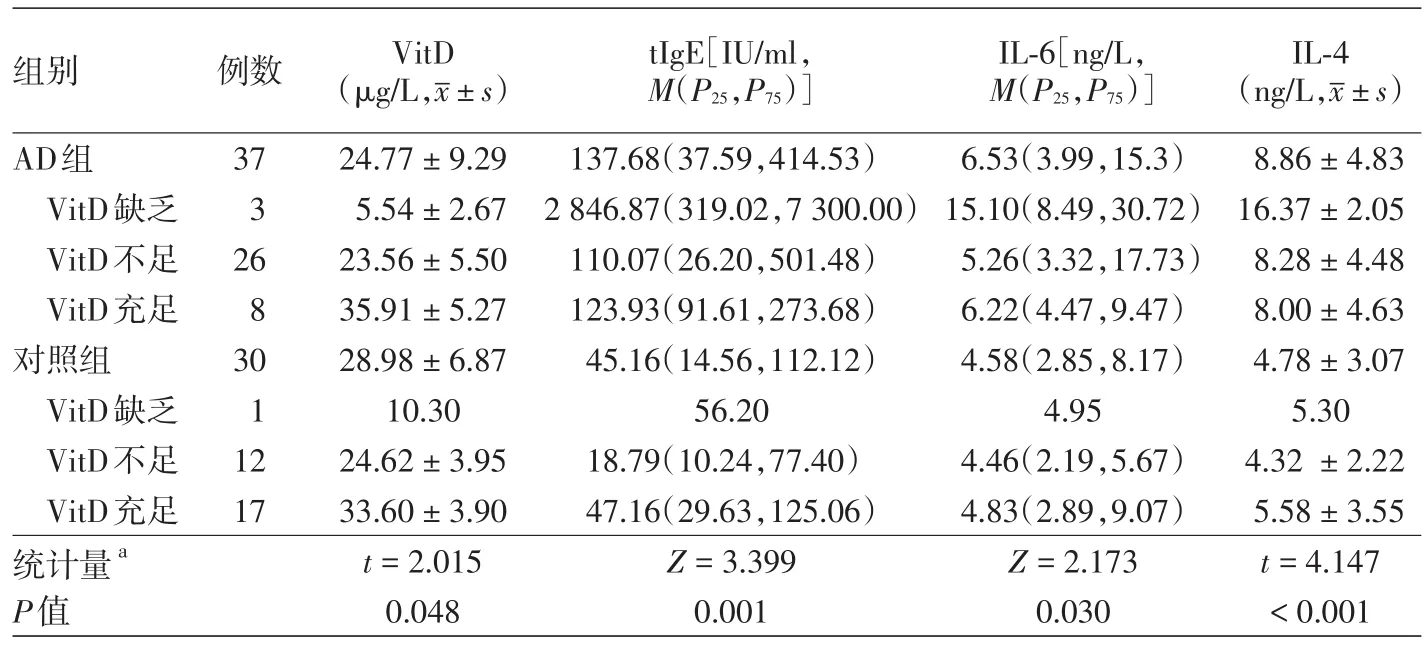
表1 特应性皮炎(AD)组与对照组血清维生素D(VitD)、总IgE(tIgE)、白细胞介素(IL)6、IL⁃4水平
讨 论
VitD是一种脂溶性维生素,活性VitD作用于细胞膜上的VitD受体(VDR)。VDR表达于人体几乎所有组织,也表达于多种免疫细胞[8]。体外实验发现,VitD可以影响T淋巴细胞、B淋巴细胞、抗原提呈细胞、巨噬细胞等的活化和进一步分化[9]。本研究中AD组血清VitD水平普遍存在缺乏和不足,水平显著低于对照组,且患者体内VitD水平与SCORAD评分呈负相关,结果与文献[10⁃11]一致,提示通过补充VitD提高患者血清VitD水平可能改善AD患者病情。另外Samochocki等[12]和Amestejani等[13]也证实,对AD患者给予口服维生素D3,可使患者皮损好转,SCORAD评分显著降低。
VitD缺乏与Th2偏移、B细胞增殖增加有关,AD病情发展中存在Th1/Th2细胞平衡紊乱,IL⁃4、IL⁃6是典型的Th2型细胞因子,其水平过高会促进肥大细胞、B细胞增殖分化,体液免疫增强。我们发现,AD患者血清 IL⁃4、IL⁃6水平明显升高,且IL⁃4与SCORAD评分呈正相关。VitD缺乏的AD患者血清IL⁃4水平显著高于VitD不足和充足的患者,IL⁃6显著高于VitD充足的患者,说明VitD缺乏可能与高水平的IL⁃4、IL⁃6有关,高水平的IL⁃4水平能使静止的B细胞活化,促进tIgE合成[14],机体对过敏原及刺激因子的反应性增强,导致病情加重。
tIgE介导的炎症反应在AD发病机制中起关键作用。有资料表明,AD患者血清tIgE升高,升高程度与皮损严重程度有关,而且病程越长血清tIgE值越高[15]。本研究中,AD患者tIgE水平明显升高,且与SCORAD评分呈正相关。Heine等[16]证实,VitD可以抑制B淋巴细胞tIgE合成。本实验也发现,VitD缺乏的AD患者tIgE水平显著高于VitD不足和充足的患者,推断VitD缺乏可能与tIgE过度产生有关,与Wang等[17]的结论符合。
综上所述,VitD缺乏可能与AD患者IL⁃6、IL⁃4等升高有关。补充VitD或可作为AD辅助治疗,但目前补充VitD是否可以改善AD愈后缺乏随机对照证据。AD多发生于婴幼儿,由于病历资料及其对照相关资料较难获得,未单独对儿童组进行观察分析是本研究的局限之处。VitD缺乏在AD发病与进展中的作用机制尚待进一步研究。
[1]Haussler MR,Whitfield GK,Kaneko I,et al.Molecular mechanisms of vitamin D action[J].Calcif Tissue Int,2013,92(2):77⁃98.DOI:10.1007/s00223⁃012⁃9619⁃0.
[2]Ginde AA,Mansbach JM,Camargo CA.Vitamin D,respiratory infections,and asthma[J].Curr Allergy Asthma Rep,2009,9(1):81⁃87.
[3]Hewison M.Antibacterial effects of vitamin D[J].Nat Rev Endocrinol,2011,7(6):337⁃345.DOI:10.1038/nrendo.2010.226.
[4]Holick MF.Vitamin D deficiency[J].N Engl J Med,2007,357(3):266⁃281.DOI:10.1056/NEJMra070553.
[5]Williams HC,Burney PG,Strachan D,et al.The U.K.Working Party′s Diagnostic Criteria for Atopic Dermatitis.Ⅱ.Observer variation of clinical diagnosis and signs of atopic dermatitis[J].Br J Dermatol,1994,131(3):397⁃405.
[6]Bischoff⁃Ferrari HA.Optimal serum 25⁃hydroxyvitamin D levels for multiple health outcomes[J].Adv Exp Med Biol,2008,624:55⁃71.DOI:10.1007/978⁃0⁃387⁃77574⁃6_5.
[7]Severity scoring of atopic dermatitis:the SCORAD index.Con⁃sensus report of the european task force on atopic dermatitis[J].Dermatology,1993,186(1):23⁃31.
[8]Adams JS,Hewison M.Update in vitamin D[J].J Clin Endocrinol Metab,2010,95(2):471⁃478.DOI:10.1210/jc.2009⁃1773.
[9]Griffin MD,Xing N,Kumar R.Vitamin D and its analogs as regulators of immune activation and antigen presentation[J].Annu Rev Nutr,2003,23:117⁃145.DOI:10.1146/annurev.nutr.23.011702.073114.
[10]Peroni DG,Piacentini GL,Cametti E,et al.Correlation between serum 25⁃hydroxyvitamin D levels and severity of atopic dermatitis in children[J].Br J Dermatol,2011,164(5):1078⁃1082.DOI:10.1111/j.1365⁃2133.2010.10147.x.
[11]Akan A,Azkur D,Ginis T,et al.Vitamin D level in children is correlated with severity of atopic dermatitis but only in patients with allergic sensitizations[J].Pediatr Dermatol,2013,30(3):359⁃363.DOI:10.1111/pde.12058.
[12]Samochocki Z,Bogaczewicz J,Jeziorkowska R,et al.Vitamin D effects in atopic dermatitis[J].J Am Acad Dermatol,2013,69(2):238⁃244.DOI:10.1016/j.jaad.2013.03.014.
[13]Amestejani M,Salehi BS,Vasigh M,et al.Vitamin D supple⁃mentation in the treatment of atopic dermatitis:a clinical trial study[J].J Drugs Dermatol,2012,11(3):327⁃330.
[14]Deo SS,Mistry KJ,Kakade AM,et al.Role played by Th2 type cytokines in IgE mediated allergy and asthma[J].Lung India,2010,27(2):66⁃71.DOI:10.4103/0970⁃2113.63609.
[15]Bieber T.The pro⁃and anti⁃inflammatory properties of human antigen⁃presenting cells expressing the high affinity receptor for IgE(Fc epsilon RI)[J].Immunobiology,2007,212(6):499 ⁃503.DOI:10.1016/j.imbio.2007.03.001.
[16]Heine G,Anton K,Henz BM,et al.1 alpha,25⁃dihydroxyvitamin D3 inhibits anti⁃CD40 plus IL⁃4⁃mediated IgE productionin vitro[J].Eur J Immunol,2002,32(12):3395⁃3404.DOI:10.1002/1521⁃4141(200212)32:12<3395::AID⁃IMMU3395>3.0.CO;2⁃#.
[17]Wang SS,Hon KL,Kong AP,et al.Vitamin D deficiency is associated with diagnosis and severity of childhood atopic dermatitis[J].Pediatr Allergy Immunol,2014,25(1):30 ⁃35.DOI:10.1111/pai.12167.
Detection of vitamin D in sera of patients with atopic dermatitis and its clinical significance
Luan Hong,Ding Jie,Liu Yihua,Chen Shuangfeng,Zhang Yingxin
Department of Dermatology,Liaocheng People′s Hospital,Liaocheng 252000,Shandong,China(Luan H);Central Laboratory,Liaocheng People′s Hospital,Liaocheng 252000,Shandong,China(Ding J,Liu YH,Chen SF,Zhang YX)
ObjectiveTo measure the serum levels of vitamin D,total immunoglobulin E(tIgE),interleukin⁃4(IL⁃4)and IL⁃6 in patients with atopic dermatitis(AD),to evaluate the association between vitamin D and severity of AD,and to investigate the role of vitamin D in inflammatory and immunoregulatory processes during the occurrence of AD.MethodsPeripheral blood samples were collected from 37 patients with AD(AD group)and 30 healthy controls(control group).The serum levels of vitamin D,tIgE,and IL⁃6 were measured by chemiluminescent sandwich enzyme immunoassay,and those of IL⁃4 by enzyme⁃linked immunosorbent assay.The severity of AD was assessed by the SCORing atopic dermatitis(SCORAD)score.Thettest or Mann⁃Whitney U test was performed to assess the differences in vitamin D,tIgE,IL⁃4 and IL⁃6 levels between the AD group and control group,chi⁃square test to compare the proportion of patients with vitamin D deficiency,insufficiency and sufficiency,and Pearson′s correlation analysis or Spearman′s correlation analysis to evaluate the correlations between the SCORAD score and serum levels of vitamin D,tIgE,IL⁃4 and IL⁃6.ResultsCompared with the control group,the AD group showed significantly decreased serum levels of vitamin D(24.77±9.29vs.28.98±6.87 μg/L,t=2.015,P=0.048),but significantly increased serum levels of tIgE(137.68[37.59-414.53]vs.45.16[14.56-112.12]IU/ml,Z=-3.399,P=0.001),IL⁃4(8.86±4.83vs.4.78±3.07 ng/L,t=4.147,P< 0.001)and IL⁃6(6.53[3.99-15.30]vs.4.58[2.85-8.17]ng/L,Z=-2.173,P=0.030).Among patients with AD,the SCORAD score was negatively correlated with serum levels of vitamin D(r=-0.505,P=0.001),positively correlated with those of tIgE(r=0.531,P=0.001)and IL⁃4(r=0.519,P=0.001),but uncorrelated with those of IL⁃6(r=-0.139,P=0.411).There were significant differences in the proportion of patients with vitamin D deficiency,insufficiency and sufficiency between the AD group and control group(χ2=8.762,P=0.013).AD patients with vitamin D deficiency showed significantly increased serum levels of tIgE(2846.87[319.02-7300.00]IU/ml)and IL⁃4([16.37±2.05]ng/L)compared with those with vitamin D insufficiency(110.07[26.20-501.48]IU/ml,P=0.045;[8.28±4.48]ng/L,P=0.011)and those with vitamin D sufficiency(123.93[91.61-273.68]IU/ml,P=0.024;[8.00±4.63]ng/L,P=0.041).In addition,serum levels of IL⁃6 were also higher in patients with vitamin D deficiency than in those with vitamin D sufficiency(15.10[8.49-30.72]vs.6.22[4.47-9.47]ng/L,P=0.011].Conclusions Vitamin D deficiency or insufficiency exists in patients with AD.Vitamin D deficiency is correlated with high serum levels of tIgE,IL⁃4 and IL⁃6,and the severity of AD is closely correlated with increased serum levels of tIgE and IL⁃6 as well as decreased serum levels of vitamin D.
Dermatitis,atopic;Vitamin D;Immunoglobulin E;Interleukin⁃4;Interleukin⁃6;Severity of illness index
Zhang Yingxin,Email:912244312@qq.com
2015⁃11⁃02)
(本文编辑:尚淑贤)
张颖新,Email:912244312@qq.com
10.3760/cma.j.issn.0412⁃4030.2016.09.002
猜你喜欢
中老年保健(2021年5期)2021-08-24
皮肤病与性病(2021年3期)2021-07-30
医学食疗与健康(2021年25期)2021-05-12
智慧健康(2021年33期)2021-03-16
中华养生保健(2020年10期)2021-01-18
保健医苑(2020年1期)2020-07-27
童话世界(2020年8期)2020-06-15
新世纪智能(英语备考)(2019年11期)2020-01-18
中华老年口腔医学杂志(2016年6期)2017-01-15
转化医学电子杂志(2015年4期)2015-12-27
