
抗血小板聚集药物对上消化道出血患者的临床病症及影响因素分析
2016-07-10 10:27郑东阳颜丽卿张卓群潘金水
中国生化药物杂志 2016年9期
郑东阳,颜丽卿,张卓群,潘金水
(1.厦门大学附属第一医院 消化内科,福建 厦门 361022;2.厦门大学附属第一医院 消化内镜室,福建 厦门 361022;3.厦门大学附属中山医院 消化内科,福建 厦门 361022)
抗血小板聚集药物对上消化道出血患者的临床病症及影响因素分析
郑东阳1Δ,颜丽卿2,张卓群2,潘金水3
(1.厦门大学附属第一医院 消化内科,福建 厦门 361022;2.厦门大学附属第一医院 消化内镜室,福建 厦门 361022;3.厦门大学附属中山医院 消化内科,福建 厦门 361022)
目的 抗血小板聚集药物对上消化道出血患者临床病症及影响因素分析。方法 采用回顾性分析的研究方法,收集2012年6月~2015年6月入厦门大学附属第一医院治疗消化道出血的110例患者资料,分为2组,对照组79例未服用抗血小板聚集药物治疗,实验组31例服用单一抗血小板聚集药物治疗,观察2组患者的消化道出血程度、出血方式,以及在内镜下表现的特征,参照每位患者的年龄、INR值,服用的药物类型,进一步分析该类药物对上消化道出血患者的临床病症和影响因素。结果 实验组消化道出血严重率明显高于对照组(P<0.05),患者年龄越大,消化道出血率越高,在内镜下主要表现为胃炎或溃疡,INR>3的患者消化道出血严重率明显高于INR<3的患者。结论 抗血小板聚集药物会明显增加消化道严重出血的机率,患者年龄及药物种类均能影响消化道出血的发生率;长期使用该类药物对十二指肠的影响最为严重,可导致该部位肠粘膜受损;随患者年龄增大,患者消化道的不良反应增大。
抗血小板聚集药物;消化道出血;INR值;内镜检查
目前,随着心脑血管疾病发病率增高,医学界对该病的预防医疗逐渐加深,人们发现抗血小板聚集药物在血栓栓塞性疾病的预防和治疗中显著疗效。治疗中,普遍使用阿司匹林和氯吡格雷,或2药联合使用。脑血管疾病如冠心病等患者可以服用小剂量的阿司匹林[1-2],对于急性冠状动脉综合征(acute coronary syndrome,ACS)和进行支架植入或搭桥手术的患者,强调联合抗血小板治疗的重要性[3]。既往史患者,如短暂性脑缺血、心房颤动、肺部栓塞等,服用该类药物后,消化道出血率有增多的趋势。抗血小板药物在保护心脑血管的同时,也会给肠胃消化道带来伤害,最严重的不良反应是消化道出血,临床工作发现非静脉曲张性消化道出血的病例越来越多[4-7]。因此,对服用抗血小板聚集药物对上消化道出血患者的影响成为热点研究。随着人口老龄化的发展,患心脑血管疾病的人不断增加,越来越多的人服用抗血小板聚集药物[8],其风险性普遍存在,只有进一步了解该类药物在心脑血管疾病中的疗效和所存在的风险,才能更准确评估利用其功能并且降低不良反应,减轻患者病痛。本次回顾性研究从患者基本资料出发,结合患者的临床表现和内镜检查[9]的表现特征,从2个方面分析研究,现报道如下。
1 资料与方法
1.1 一般资料 随机选取从2012年6月~2015年6月厦门大学附属第一医院收治的上消化道出血患者110例,分为2组。对照组79例,实验组31例,患者年龄40~80岁,性别分布无统计学意义。本研究方案获患者或近亲属知情并签署知情同意书,经我院伦理委员会批准同意。
纳入标准[12]:参照《急性非静脉曲张性上消化道出血诊治指南(草案)》[10];呕血、便色为黑或者带血等症状。
排除标准[13]:由静脉曲张所引起的上消化道出血患者;服用除阿司匹林外其他NSAIDs药物导致消化道出血患者;合并肝硬化、食管破裂患者;患有胃癌、食管癌、结肠癌等消化道癌症;患有其他各种慢性肝病史或急性感染性疾病。
1.2 方法
1.2.1 治疗方法:本次研究采取回顾性研究方法,实验组31例采用单一抗血小板聚集药物治疗,其中21例患者服用华法林(<5 mg/天),10例患者服用阿司匹林(75-325 mg/天);对照组79例未服用药物。观察患者消化道出血程度、出血方式,以及在内镜下表现特征,参照每位患者的年龄、INR值、服用药物类型,分析患者消化道出血程度与患者基本生理状况和既往史等之间的关系。
1.2.2 观察指标:观察患者年龄、INR值、吸烟史、饮酒史、既往史;利用全自动生化仪(蓝韵300T)对患者进行急查生化常规,用血常规全自动分析仪对患者血液进行分析,记录每位患者的临床表现及检查结果。

2 结果
2.1 2组患者一般资料比较 对照组,男性48例,女性31例,年龄40~80岁,平均56.54±16.49岁。实验组,男性18例,女性13例,年龄40~80岁,平均68.42±9.61岁。2组性别比较差异无统计学意义,年龄比较差异显著(P<0.05)。见表1。

表1 2组性别、年龄比较[n(%)]
#P<0.05,与对照组比较,compared with control group
2.2 2组患者既往史比较 数据显示,2组患者吸烟史、饮酒史、溃疡史及脑梗死史比较差异无统计学意义;冠心病、高血压、糖尿病史比较差异显著(P<0.05)。见表2。
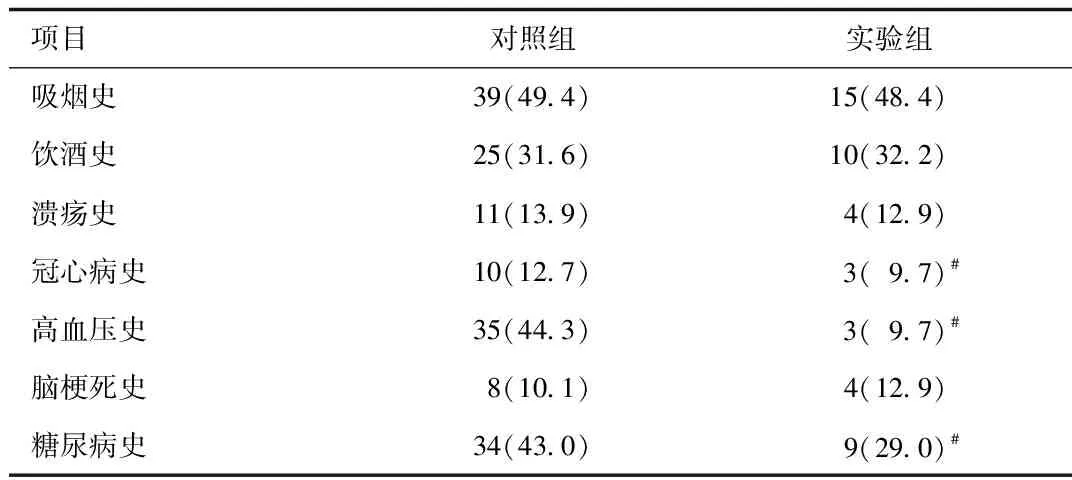
表2 2组既往史比较[n(%)]
#P<0.05,与对照组比较,compared with control group
2.3 2组患者出血形式及内镜下结果比较 有3例患者因年龄问题未能够做内镜检查。2组患者在内镜下表现主要为胃炎和溃疡,溃疡多为十二指肠球部溃疡。实验组患者发生溃疡率略高于对照组(P<0.05),且对照组主要是胃体和胃底部的溃疡,实验组主要是胃窦溃疡。见表3。

表3 2组辅助检查结果对比[n(%)]
3 讨论
目前,心脑血管疾病治疗中,多数运用抗血小板治疗[14-16],抗血小板聚集药物在血栓栓塞性疾病的预防和治疗中疗效显著,一般治疗中,普遍使用阿司匹林和氯吡格雷,或者联合使用。随着该治疗方案的普遍运用,抗血小板聚集药物对人体消化道的损害日渐突出,特别是越来越多的病例消化道严重出血,社会人口继续老龄化,进而对抗血小板药物的需求增加。本次研究考虑到药物的作用机理,阿司匹林会抑制TXA2介导的血小板聚集[17-21],破坏PGE2和PGI2介导的胃粘膜保护作用[22-23],氯吡格雷选择性地抑制二磷酸腺苷(ADP)与之血小板受体的结合和继发性ADP介导的糖蛋白复合物的活化,因此抑制血小板的聚集。血小板聚集在促进伤口愈合、止血中发挥很大作用,故血小板被抑制后,进一步会导致相关部位出血,且不易止血[24-25]。
本次研究中,在非静脉曲张上消化道出血比例中,患者年龄偏大,随着年龄的增加,消化道出血的人数逐渐增加。无论是否服用抗血小板药物,年龄与患者消化道出血率呈正相关,一方面在于随着年龄的增长,胃粘膜会发生退行性病变。同时,由于血管硬化等原因,血供应不足导致营养不良,会影响溃疡的粘膜再生;另一方面,人体肝肾功能随着年龄增长会退化,服用的抗血小板聚集药物不能及时完全被代谢排出体外,所以会损伤消化道,严重时导致出血。
综上所述,服用抗血小板聚集药物对消化道影响较大,患者应注意日常生活习惯、年龄、INR值、是否有既往史等。长期使用该类药物对十二指肠的影响最严重,可导致十二指肠粘膜受损,患者的年龄越大,幽门螺旋杆菌(Hp)感染、联合用药对消化道的不良反应明显增大。不论单一或是联合用药,其风险性普遍存在,只有进一步了解该类药物在心脑血管疾病中的疗效和相应的风险性,才能更准确评估利用其功能并且降低不良反应,减轻使用者的痛苦。
[1] Zamecnik PC, Kim B,Gao MJ,et al.Analogues of diadenosine 5',5'''-P1,P4-tetraphosphate(Ap4A) as potential anti-platelet-aggregation agents[J].Proceedings of the National Academy of Sciences,2014,89(6):2370-2373.
[2]Buchanan GR, Martin V, Levine PH,et al.The effects of “anti-platelet” drugs on bleeding time and platelet aggregation in normal human subjects[J].Am J Clin Pathol,2014,68(3):355-359.
[3]Gryglewski RJ, Korbut R, Ocetkiewicz A,et al.In vivo method for quantitation of anti-platelet potency of drugs[J].Naunyn Schmiedebergs Arch Pharmacol, 2014,302(1):25-30.
[4]Sogo N,Magid KS,Shaw C A,et al.Inhibition of human platelet aggregation by nitric oxide donor drugs: relative contribution of cGMP-independent mechanisms[J].Biochem Biophys Res Commun,2015,279(2):412-419.
[5]Jick H.Risk of upper gastrointestinal bleeding and perforation associated with individual non-steroidal anti-inflammatory drugs[J].The Lancet,2015,343(8900):769-772.
[6]Bernard B, Grangé JD, Khac EN,et al.Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding:A meta‐analysis[J].Hepatology,2015,29(6):1655-1661.
[7]Triester SL, Leighton JA, Leontiadis GI,et al.A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with obscure gastrointestinal bleeding[J].Am J Gastroenterol,2014,100(11):2407-2418.
[8]Barkun A, Bardou M,Marshall JK.Consensus recommendations for managing patients with nonvariceal upper gastrointestinal bleeding[J].Annals of internal medicine,2014,139(10):843-857.
[9]Ell C, Remke S, May A,et al.The first prospective controlled trial comparing wireless capsule endoscopy with push enteroscopy in chronic gastrointestinal bleeding[J].Endoscopy,2015,34(9):685-689.
[10]中华内科杂志编委会.急性非静脉曲张性上消化道出血诊治指南(2009,杭州).中华内科杂志,2009,48(10):891-894.
[11]Carlsson U,Grattidge P.Sedation for upper gastrointestinal endoscopy: a comparative study of propofol and midazolam[J].Endoscopy,2015,27(3):240-243.
[12]Wahab PJ, Mulder CJJ,Den Hartog G,et al.Argon plasma coagulation in flexible gastrointestinal endoscopy: pilot experiences[J].Endoscopy,2014,29(3):176-181.
[13]Rosendaal FR, Cannegieter SC, Van der Meer FJ,et al.A method to determine the optimal intensity of oral anticoagulant therapy[J].Thrombosis and haemostasis,2015,69(3):236-239.
[14]Crowther MA, Donovan D,Harrison L,et al.Low-dose oral vitamin K reliably reverses over-anticoagulation due to warfarin[J].Thrombosis and haemostasis,2014,79(6):1116-1118.
[15]Zhang X, Zhang X, Zhang Q,et al.Thromboelastographic evaluation of the different dosage anti-platelet aggregation drugs on stentassisted embolization of intracranial aneurysms[J].Chinese J of Cerebro Dis,2015.3(12):741-744.
[16]Lee JK, Wu CK, Juang JM,et al.Non-Carriers of Reduced-Function CYP2C19 Alleles are Most Susceptible to Impairment of the Anti-Platelet Effect of Clopidogrel by Proton-Pump Inhibitors:A Pilot Study.[J].ActaCardiologicaSinica,2016,32(2):215-222.
[17]Han B, Mao X, Han SX, et al.Anti-platelet aggregation bioassay based quality control for XST capsules[J].Zhongguo Zhongyao zazhi,2015,40(23):4597-4602.
[18]乐兆升,刘娴芳,孙颖立,等.53 种中草药抗血小板聚集作用的初步观察[J].中国中药杂志,1985,10(1):44.
[19]刘玲,杨防,李敏.血栓弹力图评价患者颅内外动脉狭窄支架置入术后抗血小板聚集药物的疗效[J].中国脑血管病杂志,2015,9(2):67-71.
[20]钟捷,张晨莉,马天乐,等.双气囊小肠镜与胶囊内镜诊断小肠出血病因比较[J].中华消化杂志, 2004,24(12):741-744.
[21]秦金玉,郭天骄,王瑾,等.胶囊内镜对不明原因消化道出血的诊断价值[J].四川医学, 2015, 29(3):282-285.
[22]刘跃辉.内镜止血在急性非静脉曲张性上消化道出血治疗中的临床价值[J].延边医学, 2014,10.
[23]边婕.急救护理程序在肝硬化合并上消化道出血患者中的应用[J].世界中医药,2015(A01):520-521.
[24]华艳.循证护理与预见性护理在上消化道出血急救中的应用[J].心理医生,2015,21(11):174.
[25]鹿洪霞.上消化道出血的临床护理体会[J].中国卫生标准管理,2015,21(5):180-181.
(编校:苗加会)
Analysis of clinical symptoms and influencing factors of anti-platelet aggregation drugs in patients with upper gastrointestinal bleeding
ZHENG Dong-yang1Δ, YAN Li-qing2, ZHANG Zhuo-qun2, PAN Jin-shui3
(1.Department of Digestive Internal Medicine, The First Affiliated Hospital of Xiamen University, Xiamen 361022, China; 2.Digestive Endoscopy Room,The First Affiliated Hospital of Xiamen University, Xiamen 361022, China; 3.Department of Digestive Internal Medicine, Zhongshan Hospital Affiliated to Xiamen University, Xiamen 361022, China)
ObjectiveTo analysis of clinical symptoms and influencing factors of anti-platelet aggregation drugs in patients with upper gastrointestinal bleeding.MethodsUsing the research methods of retrospective analysis,collected 110 cases of gastrointestinal bleeding patients from June 2012 to June 2015 into the first affiliated hospital of xiamen university,and divided into two groups,the control group,79 patients were treated without antiplatelet aggregation drugs,the experimental group,31 patients were treated with single antiplatelet aggregation drug.observed the degree of gastrointestinal bleeding,the mode of bleeding, and the characteristics of endoscopic findings between two groups,according to the age,INR, and the type of drug taken,the clinical symptoms and influencing factors of the patients were analyzed further.ResultsThe rate of gastrointestinal bleeding was significantly higher in the experimental group than in the control group(P<0.05).The older the patient,the higher rate of gastrointestinal bleeding,the main manifestations were gastritis or ulcers in endoscopy,patients with INR>3 had a significantly higher rate of gastrointestinal bleeding than patients with INR<3.ConclusionAnti-platelet aggregation drugs can significantly increase the chance of serious bleeding in the digestive tract,the patient’s age,INR value and the type of medication can affect the incidence of gastrointestinal bleeding;long-term use of these drugs lead the most serious impact on the duodenum, can lead to the site intestinal mucosa damage,with the increasing age of patients,adverse reactions of the digestive tract increased.
anti-platelet aggregation drugs; gastrointestinal bleeding; INR value; endoscopy
10.3969/j.issn.1005-1678.2016.09.040
福建省卫生系统中青年骨干人才培养项目(2013-ZQN-ZD-33)
郑东阳,男,本科,主任医师,研究方向:消化内科临床及内镜,E-mail:lpluck_66@yeah.net。
R571
A
猜你喜欢
中国典型病例大全(2022年12期)2022-05-13
保健医苑(2022年4期)2022-05-05
中国药学药品知识仓库(2022年5期)2022-04-11
感染、炎症、修复(2021年1期)2021-07-28
中华养生保健(2020年3期)2020-11-16
中华养生保健(2020年2期)2020-11-16
医学新知(2019年4期)2020-01-02
小学生优秀作文(低年级)(2019年5期)2019-04-25
腹腔镜外科杂志(2016年10期)2016-06-01
中国当代医药(2015年7期)2015-03-01
