
Analgesic effect of paracetamol combined with lowdose morphine versus morphine alone on patients with biliary colic: a double blind, randomized controlled trial
2016-06-07 07:58MohammadRezaFarniaRasoulBabaeiFarzanehShiraniMehdiMomeniMajidHajimaghsoudiElnazVahidiMortezaSaeediEmergencyMedicineDepartmentImamRezaHospitalKermanshahUniversityofMedicalSciencesKermanshahIranEmergencyMedicineDepartmentShariat
Mohammad Reza Farnia, Rasoul Babaei, Farzaneh Shirani, Mehdi Momeni, Majid Hajimaghsoudi, Elnaz Vahidi, Morteza SaeediEmergency Medicine Department, Imam Reza Hospital, Kermanshah University of Medical Sciences, Kermanshah, IranEmergency Medicine Department, Shariati Hospital, Tehran University of Medical Sciences, Tehran, IranEmergency Medicine Research Center, Emergency Medicine Department, Shariati Hospital, Tehran University of Medical Sciences, Tehran, IranEmergency Medicine Department, Shahid Dr Rahnemoon Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Analgesic effect of paracetamol combined with lowdose morphine versus morphine alone on patients with biliary colic: a double blind, randomized controlled trial
Mohammad Reza Farnia1, Rasoul Babaei2, Farzaneh Shirani3, Mehdi Momeni3, Majid Hajimaghsoudi4, Elnaz Vahidi3, Morteza Saeedi31Emergency Medicine Department, Imam Reza Hospital, Kermanshah University of Medical Sciences, Kermanshah, Iran2Emergency Medicine Department, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran
3Emergency Medicine Research Center, Emergency Medicine Department, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran
4Emergency Medicine Department, Shahid Dr Rahnemoon Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
KEY WORDS:Biliary colic; Morphine; Paracetamol; Visual analogue scale
World J Emerg Med 2016;7(1):25–29
INTRODUCTION
Many patients' visits to emergency departments are associated with complaints of pain.Because of nausea and vomiting accompanying pain in most patients with biliary colic, physicians usually cannot prescribe oral analgesic for pain control.[1]
In the United States, about 20 million people (10%–20% of adults) each year suffer from gallstones.These patients are frequently admitted to the emergency department because of acute pain.[2]The options for intravenous analgesia include non-steroidal antiinflammatory drugs (NSAIDs) including ketorolac or opioids such as morphine and meperidine.Previous studies[3–7]have shown that morphine could increase Oddi sphincter pressure, thus meperidine might be a better choice.However, a recent review concluded that all narcotics could have the same effect while there was no evidence confirming that opioids could aggravate biliary colic.[8]
Although pain in patients with biliary colic usually subsides within hours, pain management at the time of admission is of great importance.Nowadays, in most emergency departments (EDs) biliary pain in patients is controlled with routine opioid components.[8–9]
Various medications have been tried in patients with biliary pain such as narcotics, anticholinergic and anti-inflammatory agents.The first optional analgesics are NSAIDs such as ketorolac and opioids (morphine, meperidine and hydromorphin).The best choice would have most analgesic effect, least complication and cost, easiest way to administer, in accordance with the patient's clinical conditions and comorbidities.[3–9]
Kumar et al[10]in 2004 and Dula et al[11]in 2001 compared the analgesic effect of intravenous paracetamol versus morphine in patients with renal colic and they found that there was no significant difference in pain reduction between the two groups and they concluded that intravenous paracetamol could be an efficacious treatment for ED patients with renal colic.
Unlike opioids, N-acetyl-p-amino-phenol (paracetamol, acetaminophen) is an effective and safe drug with known analgesic effect and fewer side effects.[12]The intravenous form was introduced in European and American market in 2002 and 2010 respectively.Due to the lack of data on the effect of this drug in biliary pain management, the present study was conducted to address the effect of Paracetamol in order to reduce the frequent need of opioids.
This drug with the commercial name, Apotel, has been provided in 1 000 mg intravenous form in Iran.It has the onset of action near 5 minutes, peak effect within 1 hour and half-life of 4–6 hours.Acetaminophen has central analgesic effects through inhibition of central cyclooxygenase 1 and 2 and serotonergic system.Paracetamol has been frequently regarded as one of the most effective analgesia in different managements of emergency pain in recent years.[13]
Based on most studies mentioned above, intravenous morphine and paracetamol were used at doses of 0.05–1 mg/kg and 10–15 mg/kg, respectively.[10–12]
Since there has been no similar study in patients with biliary pain, this study compares the effect of intravenous paracetamol+low-dose morphine combination versus morphine alone in controlling pain in patients with biliary pain.
METHODS
Participants
We conducted a randomized double-blind parallel group study (with blocked randomization) in 98 patients with biliary pain recruited from the emergency department of Shariati and Imam Khomeini hospitals, two tertiary referral centers, from August 2012 to August 2013.Finally, 87 patients with abdominal pain and paraclinic data suggesting biliary origin were enrolled in the study.Inclusion criteria were age between 18 to 65 years, new onset upper half abdominal pain (VAS≥3) in favor of biliary origin, and gallstones in the bile ducts shown by sonography and laboratory data.
Exclusion criteria were as follows: previous or known hypersensitivity reactions to opioids or paracetamol; unstable vital signs (systolic blood pressure less than 90 mmHg); evidence of peritoneal irritation; pregnancy; history of renal, liver or heart failure; patients undergoing kidney, lung, liver or heart transplantation; altered mental status (GCS<15); patients who cannot cooperate in the study; visual analogue scale (VAS) less than 3; patients taking analgesics during the last 6 hours; substance or drug abuse and not giving consent to participate in the study (Figure 1).The diagnosis was confi rmed by the treating emergency physician and then the chief investigator was contacted.The patients were randomly divided into two groups: group A, 44 patients (paracetamol and low-dose morphine); group B, 43 patients (high-dose morphine).Randomization was performed by a random double digit codes list extracted from the website http://www.randominization.com by the chief investigator.Patients' allocation was concealed and both drugs were the same in color and shape.Only the chief investigator and thetriage nurse were aware of the assignment.Both the patients and emergency physician who diagnosed biliary colic were blinded to the injected medication.
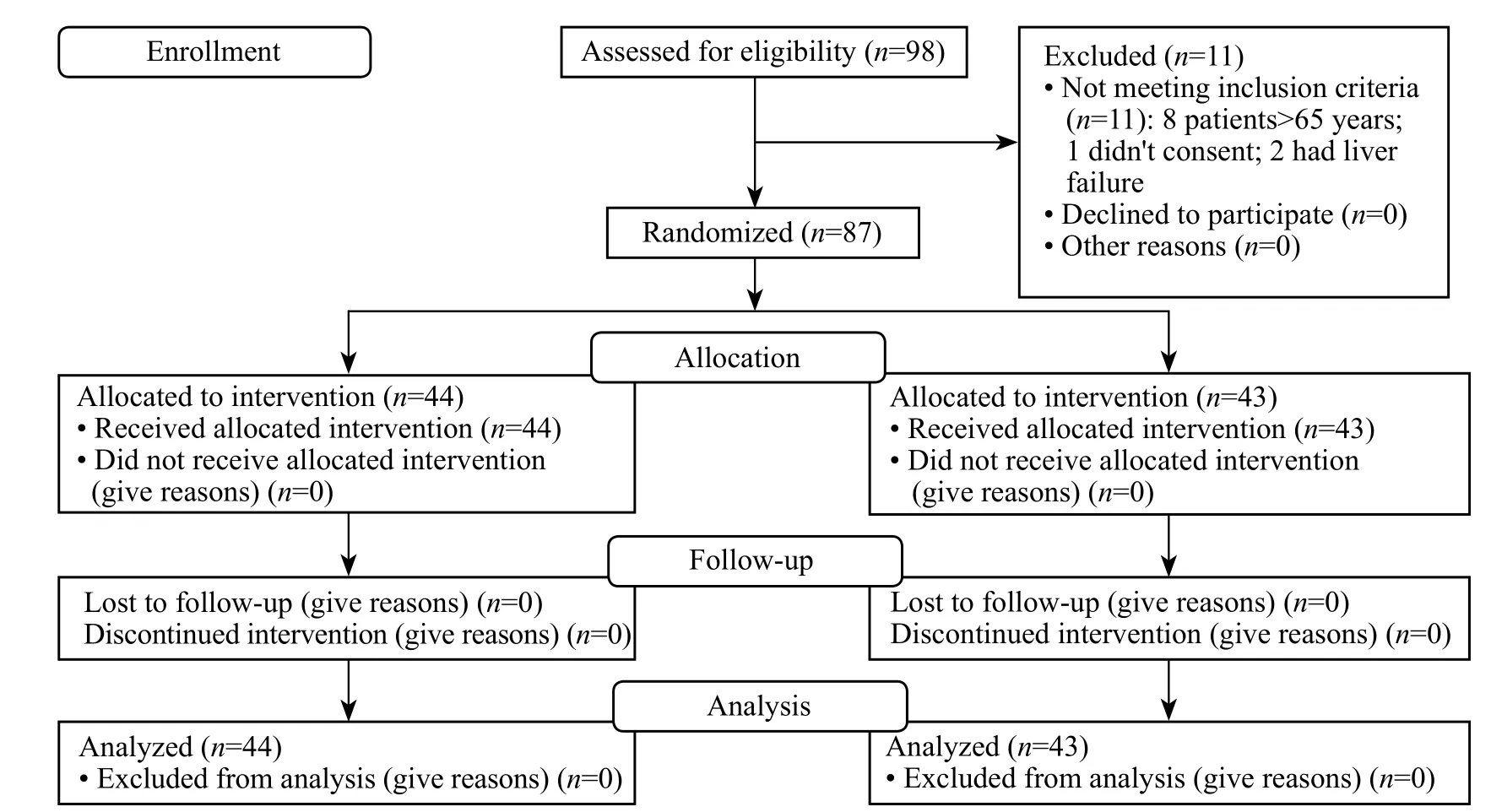
Figure 1.CONSORT fl ow diagram.
Drug administration
The patients were interviewed.The method of drug administration, visual analogue pain score (VAS; where 10 represented the worst imaginable pain and 0 was pain-free) and possible complications were explained to them and informed written consent was obtained.Ethics approval was obtained from the ethics committee of Tehran University of Medical Sciences.Demographic data including age, sex and VAS scores at 0, 15 and 30 minutes after drug administration were recorded by the emergency physician responsible for patients' treatment who was blinded to the assignment.Group A received 0.05 mg/kg morphine and 1 000 mg paracetamol in 100 mL of normal saline solution within 5 minutes (paracetamol prescribed as brand name "APOTEL" by COBEL DAROU Company).Group B received 0.1 mg/kg morphine and 100 mL normal saline solution as placebo within 5 minutes.The drugs and doses were prepared by the triage nurse according to patients' weight and treatment code and administered by the emergency physician.If pain score was lower than 13 mm or the patients themselves asked for more analgesics after 30 minutes, 1–2 macro/kg intravenous fentanyl would be injected.During the infusion, the patients were monitored for adverse effects and, if there were adverse effects, the infusion was stopped.Statistical analysis and sample size calculation
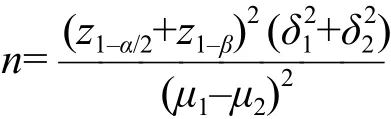
There was a 15 mm difference in the mean VAS pain score, which was considered clinically a signifi cant change, with a power of 80%, α=0.05, β=0.2 and SD of 2.5.A sample size of 45 patients in each group was calculated by means of the following formula:
All data were analyzed using SPSS V.21 software.The Kolmogronov–Smirnov (KS) test was conducted to compare the normal distribution of quantitative data such as VAS score.Subsequently, Student's t test was performed to compare the quantitative data, showing a normal distribution with a 95%CI.All the descriptive data were expressed as mean±SD.A P value <0.05 was considered statistically signifi cant.
RESULTS
In 98 patients with abdominal pain of biliary origin, 11 were excluded: 8 patients were more than 65 years old, 1 didn't consent, and 2 had liver failure.Thus 87 patients were enrolled and they all had biliary pain confirmed by physical examination, laboratory data and ultrasound in the ED.These patients were randomly divided into two groups: group A (paracetamol+morphine) and group B (morphine), 44 and 43 patients in each group respectively.
In the 87 patients, 29 (33.3%) were male and 58(66.7%) female.There were 44 patients in group A (paracetamol+morphine) and 43 in group B (morphine group).There was no signifi cant difference in gender between the two groups (P=0.36) nor in age (P=0.91).The demographics of the two groups are shown in Table 1.Side effects in the two groups are shown in Table 2.
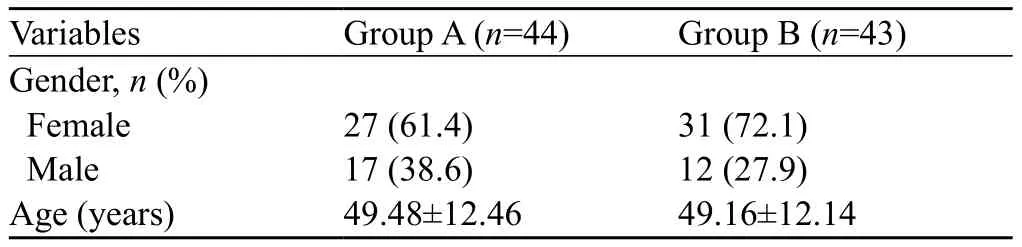
Table 1.Demographics of the two groups
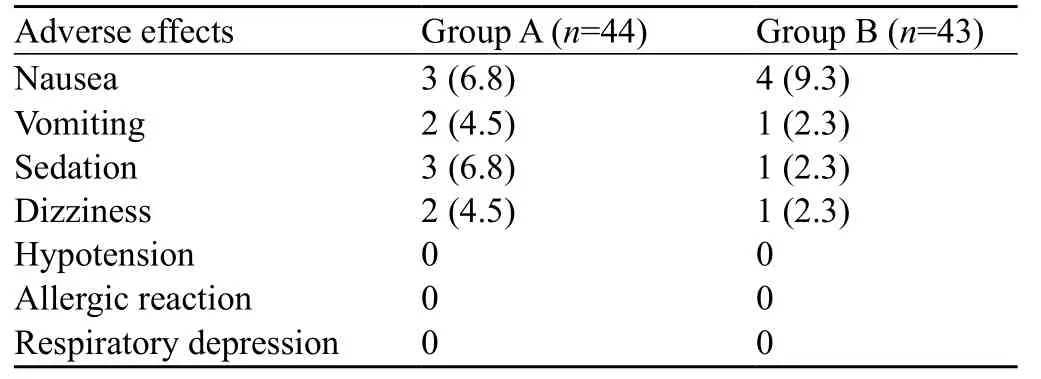
Table 2.Side effects of the two groups, n (%)
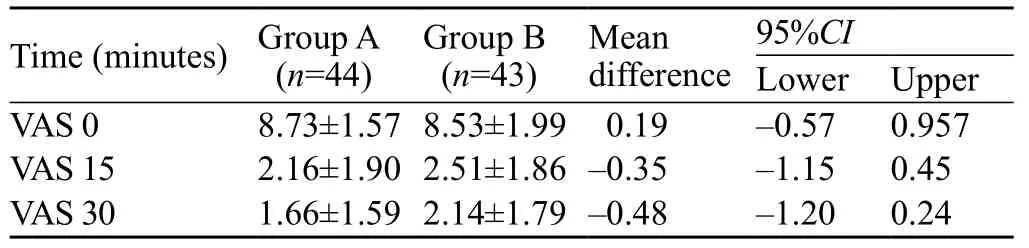
Table 3.Mean value of pain scores in the two gro
The mean pain scores in the two groups are shown in Table 3.Baseline mean±SD VAS scores were 8.73±1.57 in group A and 8.53±1.99 in group B.At 15 minutes after drug administration, the mean±SD VAS scores was 2.16±1.90 in group A vs.2.51±1.86 in group B.The mean difference was –0.35, with 95%CI –1.15 to 0.45 (P=0.38).At 30 minutes the mean±SD VAS scores were 1.66±1.59 in group A vs.2.14±1.79 in group B.The mean difference was –0.48, 95%CI –1.20 to 0.24 (P=0.19).The mean pain scores in the two groups at 0, 15 and 30 minutes demonstrated no signifi cant difference (Table 3).
ANOVA revealed that mean VAS pain score reduced after administration of paracetamol+low-dose morphine and morphine alone in both groups (P=0.001).But there was no significant difference in mean VAS scores between the two groups (Figure 2).
There were no patients in group B but two (2.3%) patients in group A, who needed fentanyl as rescue analgesia.
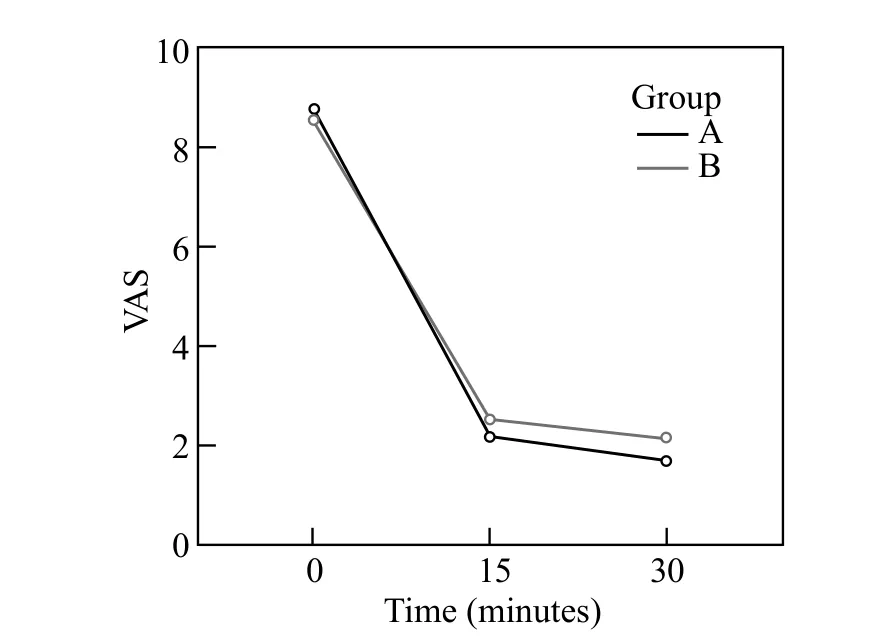
Figure 2.Changes of mean VAS scores in both groups.
DISCUSSION
Abdominal pain originating from the biliary system is one of the most common presentations of patients treated in emergency departments.Over the decades studies[12–13]have suggested intravenous paracetamol as an alternative for alleviating acute pain in patients.
A study[10]compared intravenous paracetamol versus morphine in the treatment of renal colic and found that there was no signifi cant difference in reduction of pain intensity.
Another study[11]also compared the two drugs in the treatment of renal colic and concluded that intravenous paracetamol might be as effective as morphine in pain control with less side effects.
A randomized controlled study of intravenous paracetamol versus morphine for acute traumatic limb pain found that there was neither signifi cant difference in pain scores reduction nor the rescue analgesia administered.[14]
Innes et al[15]evaluated the analgesic effects of paracetamol versus dexketoprofen vs.morphine on acute low back pain and found that three drugs administered were not superior to each other.
Opioids can cause spasm in the sphincter of Oddi.Since there are many patients in EDs who refuse to take any narcotics, other alternatives like paracetamol can be helpful.Intravenous paracetamol (intravenous acetaminophen) as an analgesic and antipyretic agent, is prescribed as the fi rst-line agent for reducing acute pain in adults and children.Paracetamol has reduced opioid rescue medication, and the intravenous form is well tolerated in clinical trials.[12–18]
In our study, paracetamol+low-dose morphine was as effective as high-dose morphine in alleviating biliary colic pain.
Limitations of the study
The sample size of our study was not adequate todetect adverse effects appropriately.
Intravenous paracetamol plus low-dose morphine may be as effective as high-dose morphine alone in alleviating pain of patients with biliary colic.Thus paracetamol administration may reduce the use of large and repeated doses of opioids.
Funding: None.
Ethical approval: Ethics approval was obtained from the ethics committee of Tehran University of Medical Sciences.
Confl icts of interest: The authors declare that there is no confl ict of interest.
Contributors: Farnia M and Babaei R contributed to the design of the study.Babaei R is responsible for data gathering and Shirani F for data analysis.All authors approved the fi nal manuscript.
REFERENCES
1 Olsen JC, McGrath NA, Schwarz DG, Cutcliffe BJ, Stern JL.A double-blind randomized clinical trial evaluating the analgesic efficacy of ketorolac versus butorphanol for patients with suspected biliary colic in the emergency department.Acad Emerg Med 2008; 15: 718–722.Epub 2008 Jul 11.
2 Lawrence P.Essentials of General Surgery.Philadelphia, PA: Lippincott, Williams &Wilkins, 2000.
3 Wu SD, Zhang ZH, Jin JZ, Kong J, Wang W, Zhang Q, et al.Effects of narcotic analgesic drugs on human Oddi's sphincter motility.World J Gastro 2004; 10: 2901–2904.
4 Barlas D, Margouleff D, Vignogna-Barlas L, Lesser ML.Opioids prolong nuclear hepatobiliary imaging when given prior to scanning.J Emerg Med 2002; 23: 231–236.
5 Mc Cammon R, Stoelting R, Madura J.Effects of butorphanol, nalbuphine and fentanyl on intrabiliary tract dynamics.Anest Analg 1984; 63:139–142.
6 Radnay PA, Duncalf D, Novakovic M, Lesser ML.Common bile duct pressure changes after fentanyl, morphine, meperidine, butorphanol, and naloxone.Anesth Analg 1980; 29: 26–29.
7 Wu SD, Zhang ZH, Li DY, Jin JZ, Kong J, Tian Z, et al.Nitroester drug's effects and their antagonistic effects against morphine on human sphincter of oddi motility.World J Gastroenterol 2005; 11: 2319–2323.
8 Linklater DR, Pemberton L, Taylor S, Zeger W.Painful dilemmas: an evidence-based look at challenging clinical scenarios.Emerg Med Clin N Am 2005; 23: 367–392.
9 Al-Waili N, Saloom KY.The analgesic effect of intravenous tenoxicam in symptomatic treatment of biliary colic: a comparison with hyoscine N-butylbromide.Eur J Med Res 1998; 3: 475–479.
10 Kumar A, Deed JS, Bhasin B, Kumar A, Thomas S.Comparison of the effect of diclofenac with hyoscine-N-butylbromide in the symptomatic treatment of acute biliary colic.ANZ J Surg 2004; 74: 573–576.
11 Dula DJ, Anderson R, Wood GC.A prospective study comparing i.m.ketorolac with i.m.meperidine in the treatment of acute biliary colic.J Emerg Med 2001; 20: 121–124.
12 Bektas F, Eken C, Karadeniz O, Goksu E, Cubuk M, Cete Y.Intravenous paracetamol or morphine for the treatment of renal colic: a randomized, placebo-controlled trial.Ann Emerg Med 2009; 54: 568–574.Epub 2009 Jul 31.
13 Serinken M, Eken C, Turkcuer I, Elicabuk H, Uyanik E, Schultz CH.Intravenous paracetamol versus morphine for renal colic in the emergency department: a randomised double-blind controlled trial.Emerg Med J 2012; 29: 902–905.doi: 10.1136/ emermed–2011–200165.Epub 2011 Dec 20.
14 Duqqan ST, Scott LJ.Intravenous Paracetamol.Drugs 2009; 69: 101–113.
15 Innes G, Murphy M, Nijssen-Jordan C, Ducharme J, Drummond A.Procedural sedation and analgesia in the emergency department.Canadian Consensus Guidelines.J Emerg Med 1999; 17: 145–156.
16 Craig M, Jeavons R, Probert J, Benger J.Randomised comparison of intravenous paracetamol and intravenous morphine for acute traumatic limb pain in the emergency department.Emerg Med J 2012; 29: 37–39.doi: 10.1136/ emj.2010.104687.Epub 2011 Mar 1.
17 Eken C, Serinken M, Elicabuk H, Uyanik E, Erdal M.Intravenous paracetamol versus dexketoprofen versus morphine in acute mechanical low back pain in the emergency department.Emerg Med J 2014; 31: 177–181.
18 Lachiewicz P.The role of intravenous acetaminophen in multimodal pain protocols for perioperative orthopedic patients.Orthopedics 2013; 36: 15–19.
Received September 16, 2015
Accepted after revision January 8, 2016
BACKGROUND: Numerous drugs have been proposed to alleviate pain in patients with biliary colic, especially opioids, but still there is a tendency to use less narcotics because of their side effects and the unwillingness of some patients.The present study aimed to compare the analgesic effect of paracetamol combined with low-dose morphine versus morphine alone in patients with biliary colic.
METHODS: A randomized double-blind controlled trial was performed in 98 patients with biliary colic, recruited from two emergency departments from August 2012 to August 2013.Eleven patients were excluded and the remaining were randomized into two groups: group A received 0.05 mg/kg morphine+1 000 mg paracetamol in 100 mL normal saline and group B received 0.1 mg/kg morphine+normal saline (100 mL) as placebo.Pain scores were recorded using visual analogue scale (VAS) at baseline and 15 and 30 minutes after drug administration.Adverse effects and the need for rescue medication (0.75 μg/kg intravenous fentanyl) were also reported within 60 minutes of drug administration.
RESULTS: Before the infusion, the mean±SD VAS scores were 8.73±1.57 in group A and 8.53±1.99 in group B.At 15 minutes after drug administration, the mean±SD VAS scores were 2.16±1.90 in group A vs.2.51±1.86 in group B; mean difference was –0.35, and 95%CI –1.15 to 0.45 (P=0.38).At 30 minutes the mean±SD VAS scores were 1.66±1.59 in group A vs.2.14±1.79 in group B; mean difference was –0.48, and 95%CI –1.20 to 0.24 (P=0.19).The mean pain scores in the two groups at 15 and 30 minutes demonstrated no signifi cant difference.
CONCLUSION: Paracetamol combined with low-dose morphine may be effective for pain management in patients with biliary colic.
Corresponding Author:Morteza Saeedi, Email: m_saeedi@tums.ac.ir
DOI:10.5847/ wjem.j.1920–8642.2016.01.004
 World journal of emergency medicine2016年1期
World journal of emergency medicine2016年1期
- World journal of emergency medicine的其它文章
- Airway foreign bodies: A critical review for a common pediatric emergency
- End-tidal capnometry during emergency department procedural sedation and analgesia: a randomized, controlled study
- Intranasal ketamine for the treatment of patients with acute pain in the emergency department
- Comparison of intravenous pantoprazole and ranitidine in patients with dyspepsia presented to the emergency department: a randomized, double blind, controlled trial
- A correlation analysis of Broselow™ Pediatric Emergency Tape-determined pediatric weight with actual pediatric weight in India
- Emergency department patients with small bowel obstruction: What is the anticipated clinical course?