
Cryptosporidiosis among children with diarrhoea in three Asian countries:A review
2015-11-01 02:44BahaLatifNurulFarizaRossle
Baha Latif,Nurul Fariza Rossle
Faculty of Medicine,Universiti Teknologi MARA,47000 Sungai Buloh,Selangor,Malaysia
Cryptosporidiosis among children with diarrhoea in three Asian countries:A review
Baha Latif*,Nurul Fariza Rossle
Faculty of Medicine,Universiti Teknologi MARA,47000 Sungai Buloh,Selangor,Malaysia
ARTICLE INFO
Article history:
2nd revised form 4 Mar 2015
Accepted 20 May 2015
Available online 18 Aug 2015
Cryptosporidium spp.
Children
Diagnosis
Prevalence
This review focuses on studies concerning cryptosporidiosis in three Asian countries. Cryptosporidium spp.infection was investigated in children<12 years old afflicted with diarrhoea and admitted to the paediatric hospitals in Iraq,Jordan and Malaysia.Most of the patients complained of abdominal pain,watery diarrhoea and mild-to-severe dehydration.Stool samples were collected from children and five methods were used to detect oocysts of Cryptosporidium spp.including:direct wet mount,Sheather's sugar flotation,formalin-ether sedimentation,modified Ziehl-Neelsen and direct fluorescent antibody(DFA).The infection rate was 8.56,37.3 and 4.6 in Iraq,Jordan and Malaysia,respectively.A combination of formalin ether sedimentation and acid fast stain was used to detect Cryptosporidium oocysts in Iraq.The DFA test showed the highest sensitivity for samples of children in Jordan.In Malaysia,direct wet mount,formalin-ether sedimentation,modified Ziehl-Neelsen and DFA gave the same results(4.62%)while Sheather's sugar flotation was 3.85%.Source of drinking water appeared to be an important risk factor in transmission of infection.In Jordan,the high rate of infection was recorded in rainy season(January-May).
Review articlehttp://dx.doi.org/10.1016/j.apjtb.2015.05.021
1.Introduction
Cryptosporidium is a coccidian protozoan parasite found in the brush-border of the enterocytes of the small intestine in many vertebrates,includinghumans[1].Cryptosporidiosisis recognized as a cause of diarrhoeal illness in man and animal[1].The first case of human cryptosporidiosis was reported in 1976,andthereareincreasingnumbersofdocumented infection with Cryptosporidium spp.since then.Now,it is considered a common enteric pathogen in humans and animals worldwide[2].Cryptosporidiosis can induce self-limiting diarrhoea in immunocompetent people or severe and prolonged diarrhoea in immunocompromised patients,such as those with AIDS,transplant recipients,those are receiving chemotherapy for cancer,and patients with immunosuppressive infectious disease[3].In developing countries,Cryptosporidium mostly infects children below five years of age and peaks in children below two years of age[4,5].However,in industrialisedcountries,cryptosporidiosis also occurs in adults due to foodborne or waterborne outbreaks[6,7].
Diagnosis of the infection requires the detection of the oocysts in stool.Owing to the small size(4-6μm)of the oocysts,the routine wet mount preparation and concentration methods have limited value for detection of oocysts in stool samples,which can easily be confused with other materials[8].
In Iraq,cryptosporidiosis was reported in children with severe diarrhoea and dehydration.Latif(unpublished data),Mahdi et al.[9]and Mahdi and Ali[10]showed that the infection rate in childrenunderfiveyearswas8.56%,8.8%and9.7% respectively.Cryptosporidium spp.oocyst was identified using modified Ziehl-Neelsen staining method.
In Jordan,Nimri and Batchoun found that 2.5%of asymptomatic children in the 6-14 years old age group were infected with Cryptosporidium spp.and an infection rate of 1.5%in symptomatic children with diarrhoea and other clinical symptoms[11].Another study on elementary school children found theinfectionratetobe7%[12].Thehighestreported prevalence of cryptosporidiosis in Jordan is 37.3%and was found in paediatric patients[13].
In Malaysia,the documented prevalence of Cryptosporidium infection ranged within 0.9%-23% [14-21].However,very few of these studies have focused solely on paediatric cases,with HIV-positive intravenous drug user accountingfor the highest prevalence(23%).Using both microscopy and PCR techniques,Menon et al.showed that 0.9%of children hospitalized with acute diarrhoea in Kelantan was positive for Cryptosporidiumparvum[14].Ludinetal.reporteda prevalence of cryptosporidiosis of 4.3%in Penang[15].The reported figures in Malaysia are relatively low compared to Jordan(37.3%)[13],Nicaragua(35.7%)[22],and Ethiopia(12.1%)[23].
Now,there is no doubt that cryptosporidiosis poses a threat to health in both human and animals worldwide[24].The aim of thisreviewistohighlightontheprevalenceof cryptosporidiosis among children with diarrhoea in three different Asian countries(Iraq,Jordan,and Malaysia).In addition,the review was focused on some epidemiological factors concerned with the infection.
2.Source of infection
Drinking water plays an important role in the transmission of infection.In Iraq,it is common practice to store commercial waters in barrels and containers for a few days before consumption[10].This might lead to exposure to viable oocysts in the environment,thus contaminating the water.Many people in Jordan depended on untreated rainwater collected directly from the roof,then stored in metal or cement tanks.Treated water from water treatment plants sometimes got contaminated with burst sewage pipes due to bombings of streets and buildings in Iraq.Moreover,oocysts of Cryptosporidium spp. can survive in chlorine used for water treatment[25].The low prevalence of infection in Malaysia could be attributed to the use of treated water,and the absence of household pets. Treated water supplies were available to approximately 99% of urban and 91%of rural populations[26].Earlier studies in these areas have revealed no oocysts in treated water[27,28],although they were found in filter backwash water samples fromtreatmentplants.Studies fromother countrieshad reported high prevalence of Cryptosporidium spp.oocysts in water from wells and springs[13,22].Other possible methods of transmission in Iraq are contacted with person suffering fromdiarrhoea,associationwithdogsandcats,or consumption of untreated milk[9].People living in urban areas with proper amenities and no domestic pets,it is logical to concludethatthesourceofinfectionisprobably anthroponotic.However,nothing concrete can be proven without further testing using genotyping method or molecular identification of species.
Seasonal or temporal trends associated with increased incidence vary from country to other.In Central America,South Africa,and India,the peak of incidence was reported in rainy season[29].This review showed that the results were similar to thatconductedinKuwaitregardingtheseasonalityof cryptosporidiosis in Kuwaiti children.The results of that study showed that the maximum numbers of cases were recorded during the rainy seasons[30].
3.Diagnosis
Stool samples were collected from children<12 years old who were suffering from abdominal pain,watery diarrhoea and dehydration admitted to hospitals in Iraq(500/province),Jordan(300),and Malaysia(130).Up to five different methods were used for diagnosis of infection,including direct wet mount,Sheather's sugar flotation,formalin-ether sedimentation,modified Ziehl-Neelsen staining and direct fluorescent antibody(DFA).
In direct wet mount preparation,Cryptosporidium oocysts appeared spherical in shape with a thick cell wall and diameter ranged from 4 to 6μm.In modified acid-fast,oocysts stained pinkish red with blue or green background,depending on the counter stain used.In fluorescent assay,oocysts fluoresce an apple green colour over a dark background.
4.Prevalence
The infection rate of cryptosporidiosis in children in Iraq was 8.6%-9.7%[9,10].The high rate was in Baghdad(14.60%)and the lowest was in Babylon(2.20%)(Latif,unpublished data)(Table 1).These studies used direct wet mount and modified Ziehl-Neelsen staining method.Mahdi and Ali reported that combination of formalin-ether sedimentation and modified acidfast stain methods has been regarded with high sensitivity and specificity,since it both concentrates the oocysts and differentiates them from other faecal matters[10].
In Jordan,out of 300 stool samples,112(37.3%)were positive for Cryptosporidium sp.Direct fluorescence test gave the highest rate of positive samples(37.3%)and statistically the most sensitive compared with the other diagnostic methods(Figure 1).
In Malaysia,out of 130 stool samples,6(4.62%)samples were positive for Cryptosporidium sp.All the children with positive results were below 4 years of age.Regarding the five tests used,direct wet mount,formalin-ether sedimentation concentration,modified Ziehl-Neelsen staining,and direct monoclonal fluorescent antibody tests gave the same result(4.62%)while Sheather's sugar flotation detect only positive in 5 children(3.85%).The comparative result between the five methods isillustrated in Figure 2.There was no difference in the distribution of cases between males and females.All infected individuals lived in urban areas.These areas were supplied with tap water from water treatment plants and have structured plumbing.Four(66.67%)of the positive cases are Malays,while the rest are Chinese and Indians.None of the families owned animals(Table 2).
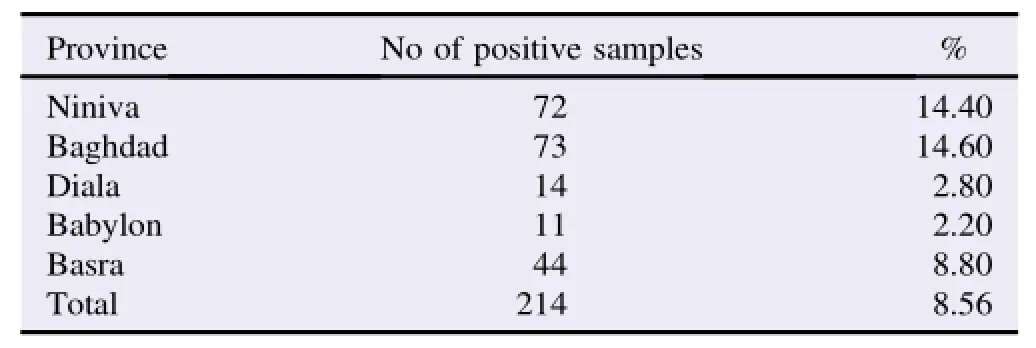
Table 1 Prevalence of Cryptosporidium spp.oocysts in stool samples from children in Iraq.
Jordan showed a high rate of infection(37.3%)followed by Iraq(8.6%)and Malaysia(4.62%).Although this figure is higher than those previously reported in Jordan[11,12],it was attributed to the specificity of tests used for detection of oocysts in stool samples.
In Malaysia,the prevalence of cryptosporidiosis in this study(4.62%)is similar to that of previous reports where the infection rate ranges between 0.9%and 11% [14-17,20].A majority of infected cases were children<four years of age.This is in agreement with other Malaysian studies[14,16].In Ireland[31],China[32]and Bangladesh[33],the highest frequency of cryptosporidiosis were reported in children below three years of age.
The infection rate of cryptosporidiosis varied according to the number of samples,diagnostic tests,availability of facilities and reporting systems.Infection rate of 13.5%-19.5%have been reported in Egypt[34],and 10%in Kuwaiti children[30].Very high rates have been reported in Bedouin children(48%)[35],in Texas-Mexico border(70.2%)[36]and from the Republic of Korea(57%)[37].
In Jordan,the direct wet mount showed the lowest number of positive samples(17.3%)in comparison with other methods[38].Positivesamplesincreasedto22.6%byflotation concentration method.This method necessitated reading the results within 15 min of preparation because the oocysts tend to shrink and disappear if left for a long time.Moreover,thepresence of Sheather's sugar solution inhibits the staining procedure[39].

Table 2 Demographic data of Cryptosporidium-positive children in Malaysia[21].
The acid-fast staining technique showed a higher rate of infection(30.6%).Oocysts appeared red to pink colour.DFA gave the highest rate of positive samples(37.3%).This method showed high sensitivity and was able to detect oocysts even when present in low number and large number of samples could be scanned.
Meanwhile,the outcome for the different techniques did not differ much in Malaysian study.The five methods showed the same results except for Sheather's sugar flotation method,which detect one less positive than others.This may be due to the distortion of oocysts over time because of osmotic effects,making it harder to identify.The best way that we would recommend to screen for Cryptosporidium spp.in hospitals is by using modified Ziehl-Neelsen staining since it is cheap,rapid and easy to interpret.DFA could be used to confirm the acid-fast positive samples or to diagnose cases of persistent diarrhoea with unknown cause.
Although some studies reported discrepancies in detection of oocysts between direct microscopy,concentration technique,acid-fast staining and DFA[13,40-42],it is also not uncommon for the results to be similar[43].Menon et al.found that the prevalence of cryptosporidiosis by modified Ziehl-Neelsen was similar to that by PCR assay,which was considered more sensitive than conventional microscopy[14].
5.Conclusion
The infection rate was 8.56,37.3,and 4.62 in Iraq,Jordan and Malaysia,respectively.A combination of formalin ether sedimentation and acid fast stain was used to detect Cryptosporidium oocysts in Iraq.DFA test showed the highest sensitivity for samples of children in Jordan.In Malaysia,direct wet mount,formalin-ether sedimentation,modified Ziehl-Neelsen and DFA gave the same results(4.62%)while Sheather's sugar flotation was 3.85%.Source of drinking water plays an important role in the transmission of infection.
Conflict of interest statement
We declare that we have no conflict of interest.
Acknowledgments
This study was part of the project funded by MARA University of Technology Excellence Fund[600-RMI/ST/DANA 5/ 3/Dst(334/2011)].
[1]Fayer R.Taxonomy and species delimitation in Cryptosporidium. Exp Parasitol 2010;124(1):90-7.
[2]Meisel JL,Perera DR,Meligro C,Rubin CE.Overwhelming watery diarrhea associated with a Cryptosporidium in an immunosuppressed patient.Gastroenterology 1976;70(6):1156-60.
[3]Fayer R,Morgan U,Upton SJ.Epidemiology of Cryptosporidium: transmission,detection and identification.Int J Parasitol 2000;30(12-13):1305-22.
[4]Bern C,Ortega Y,Checkley W,Roberts JM,Lescano AG,Cabrera L,et al.Epidemiologic differences between cyclosporiasis and cryptosporidiosis in Peruvian children.Emerg Infect Dis 2002;8:581-5.
[5]Snelling WJ,Xiao L,Ortega-Pierres G,Lowery CJ,Moore JE,Rao JR,et al.Cryptosporidiosis in developing countries.J Infect Dev Ctries 2007;1(3):242-56.
[6]Fayer R.Cryptosporidium:a water-borne zoonotic parasite.Vet Parasitol 2004;126:37-56.
[7]Xiao L,Ryan UM.Cryptosporidiosis:an update in molecular epidemiology.Curr Opin Infect Dis 2004;17:483-90.
[8]Vohra P,Sharma M,Chaudary U.A comprehensive review of diagnostic techniques for detection of Cryptosporidium parvum in stool samples.J Pharm 2012;2(5):15-26.
[9]Mahdi NK,Al-Sadoon IA,Mohamed AT.First report of cryptosporidiosis among Iraqi children.East Mediterr Health J 1996;2(1):115-20.
[10]Mahdi NK,Ali NH.Cryptosporidiosis and other intestinal parasitic infections in patients with chronic diarrhea.Saudi Med J 2004;25(9):1204-7.
[11]Nimri LF,Batchoun R.Prevalence of Cryptosporidium species in elementary school children.J Clin Microbiol 1994;32(4):1040-2.
[12]Nimri LF,Hijazi SS.Cryptosporidium.A cause of gastroenteritis in preschool children in Jordan.J Clin Gastroenterol 1994;19(4): 288-91.
[13]Mahgoub ES,Almahbashi A,Latif B.Cryptosporidiosis in children in a north Jordanian paediatric hospital.East Mediterr Health J 2004;10:494-501.
[14]Menon BS,Abdullah S,Mahamud F,Morgan UM,Malik AS,Choo KE,et al.Low prevalence of Cryptosporidium parvum in hospitalized children in Kota Bharu,Malaysia.Southeast Asian J Trop Med Public Health 2001;32(2):319-22.
[15]Ludin CM,Afifi SA,Hasenan N,Maimunah A,Anuar AK. Cryptosporidiosis among children with acute gastroenteritis in the paediatric ward in the General Hospital,Penang.Southeast Asian J Trop Med Public Health 1991;22(2):200-2.
[16]Lai KPF.Intestinal protozoan infections in Malaysia.Southeast Asian J Trop Med Public Health 1992;23:578-86.
[17]Ng KP,Shekhar KC.The prevalence of cryptosporidiosis in children and adults at University Hospital,Kuala Lumpur.Med J Malays 1993;48(3):293-6.
[18]Kamel AG,Kasim MS,Lai KPF.Parasitic infections among Orang Asli community in Pangsun,Hulu Langat.Institute for Medical Research Annual Report.Kuala Lumpur:Institute for Medical Research;1994,p.46-7.
[19]Kamel AG,Maning N,Arulmainathan S,Murad S,Nasuruddin A,Lai KP.Cryptosporidiosis among HIV positive intravenous drug users in Malaysia.Southeast Asian J Trop Med Public Health 1994;25(4):650-3.
[20]Lim YA,Rohela M,Sim BL,Jamaiah I,Nurbayah M.Prevalence of cryptosporidiosis in HIV-infected patients in Kajang Hospital,Selangor.Southeast Asian J Trop Med Public Health 2005;36:30-3.
[21]Rossle NF,Latif B,Malik AS,Fadzli FM,Abu NA.Cryptosporidiosis among children with diarrhea admitted to Hospital Selayang and Hospital Sungai Buloh in Selangor,Malaysia.J Trop Med Parasitol 2012;35(2):55-62.
[22]Muñoz-Antoli C,Pav´on A,Marcilla A,Toledo R,Esteban JG. Prevalence and molecular characterization of Cryptosporidium in school children from department of Rio San Juan(Nicaragua). Trop Biomed 2011;28(1):40-7.
[23]Ayalew D,Boelee E,Endeshaw T,Petros B.Cryptosporidium and Giardia infection and drinking water sources among children in Lege Dini,Ethiopia.Trop Med Int Health 2008;13(4):472-5.
[24]Rossle NF,Latif B.Cryptosporidiosis as threatening health problem:a review.Asian Pac J Trop Biomed 2013;3(11):916-24.
[25]Ran Z,Li S,Huang J,Yuan Y,Cui C,Williams CD.Inactivation of Cryptosporidium by ozone and cell ultrastructures.J Environ Sci(China)2010;22(12):1954-9.
[26]WHO-UNICEF.Malaysia:estimates on the use of water sources and sanitation facilities.Geneva:World Health Organization;2015.[Online]Available from:http://www.wssinfo.org/fileadmin/user_ upload/resources/Malaysia.xls[Accessed on 25th December,2014]
[27]Ahmad RA,Lee E,Tan ITL,Mohamad-Kamel AG.Occurrence of Giardia cysts and Cryptosporidium oocysts in raw and treated water from two water treatment plants in Selangor,Malaysia. Water Res 1997;31(12):3132-6.
[28]Lim YA,Aahmad RA.Occurrence of Giardia cysts and Cryptosporidium oocysts in the Temuan Orang Asli(aborigine)River System.Southeast Asian J Trop Med Public Health 2004;35(4): 801-10.
[29]Casemore DP,Wright SE,Coop RL.Cryptosporidiosis-human and animal epidemiology.In:Fayer R,editor.Cryptosporidium and cryptosporidiosis.New York:CRC Press;1997.
[30]Iqbal J,Hira PR,Al-Ali F,Philip R.Cryptosporidiosis in Kuwaiti children:seasonality and endemicity.Clin Microbiol Infect 2001;7(5):261-6.
[31]Corbett-Feeney G.Cryptosporidium among children with acute diarrhoea in the west of Ireland.J Infect 1987;14:79-84.
[32]Chen YG,Yao FB,Li HS,Shi WS,Dai MX,Lu M.Cryptosporidium infection and diarrhea in rural and urban areas of Jiangsu,People's Republic of China.J Clin Microbiol 1992;30(2):492-4.
[33]Bhattacharya MK,Teka T,Faruque AS,Fuchs GJ.Cryptosporidium infection in children in urban Bangladesh.J Trop Pediatr 1997;43:282-6.
[34]Abdel-Maboud AI,Rossignol JF,El-Kady MS,Mostafa MS,Kabil SM.Cryptosporidiosis in Benha,study of some modalities in diagnosis and treatment.J Egypt Soc Parasitol 2000;30(3):717-25.
[35]Robin G,Fraser D,Orr N,Sela T,Slepon R,Ambar R,et al. Cryptosporidium infection in Bedouin infants assessed by prospective evaluation of anticryptosporidial antibodies and stool examination.Am J Epidemiol 2001;153(2):194-201.
[36]Leach CT,Koo FC,Kuhls TL,Hilsenbeck SG,Jenson HB.Prevalence of Cryptosporidium parvum infection in children along the Texas-Mexico border and associated risk factors.Am J Trop Med Hyg 2000;62(5):656-61.
[37]Chai JY,Kim NY,Guk SM,Park YK,Seo M,Han ET,et al.High prevalence and seasonality of cryptosporidiosis in a small rural village occupied predominantly by aged people in the Republic of Korea.Am J Trop Med Hyg 2001;65:518-22.
[38]Chalmers RM,Campbell BM,Crouch N,Charlett A,Davies AP. Comparison of diagnostic sensitivity and specificity of seven Cryptosporidium assays used in the UK.J Med Microbiol 2011;60(Pt 11):1598-604.
[39]Weber R,Bryan RT,Bishop HS,Wahlquist SP,Sullivan JJ,Juranek DD.Threshold of detection of Cryptosporidium oocysts in human stool specimens:evidence for low sensitivity of current diagnostic methods.J Clin Microbiol 1991;29(7):1323-7.
[40]Zaglool DA,Mohamed A,Khodari YA,Farooq MU.Crypto-Giardia antigen rapid test versus conventional modified Ziehl-Neelsen acid fast staining method for diagnosis of cryptosporidiosis.Asian Pac J Trop Med 2013;6(3):212-5.
[41]Ranjbar-BahadoriSH,SangsefidiH,ShemshadiB,Kashefinejad M.Cryptosporidiosis and its potential risk factors in children and calves in Babol,north of Iran.Trop Biomed 2011;28(1):125-31.
[42]Tuli L,Singh DK,Gulati AK,Sundar S,Mohapatra TM. A multiattribute utility evaluation of different methods for the detection of enteric protozoa causing diarrhea in AIDS patients. BMC Microbiol 2010;10:11.
[43]Kehl KS,Cicirello H,Havens PL.Comparison of four different methods for detection of Cryptosporidium species.J Clin Microbiol 1995;33(2):416-8.
30 Dec 2014
Baha Latif,Faculty of Medicine,Universiti Teknologi MARA,47000 Sungai Buloh,Selangor,Malaysia.
E-mail:bahalatif@yahoo.com
Peer review under responsibility of Hainan Medical University.
Foundation Project:Partly funded by MARA University of Technology Excellence Fund[600-RMI/ST/DANA 5/3/Dst(334/2011)].
in revised form 19 Jan,
 Asian Pacific Journal of Tropical Biomedicine2015年11期
Asian Pacific Journal of Tropical Biomedicine2015年11期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- Conjunctival cytological examination,bacteriological culture,and antimicrobial resistance profiles of healthy Mediterranean buffaloes(Bubalus bubalis)from Southern Italy
- Cytotoxicity evaluation of extracts and fractions of five marine sponges from the Persian Gulf and HPLC fingerprint analysis of cytotoxic extracts
- Molecular study on methicillin-resistant Staphylococcus aureus strains isolated from dogs and associated personnel in Jordan
- ERG11 mutations associated with azole resistance in Candida albicans isolates from vulvovaginal candidosis patients
- Evaluation of zoonotic potency of Escherichia coli O157:H7 through arbitrarily primed PCR methods
- Anti-inflammatory and antipyretic properties of Kang 601 heji,a traditional Chinese oral liquid dosage form