
慢性心力衰竭患者血尿酸水平和房颤的关系
2015-04-21 07:43:07张献斌许新录
中华老年多器官疾病杂志 2015年4期
肖 婷,张献斌,罗 磊,杨 娜,梁 晗,许新录
慢性心力衰竭患者血尿酸水平和房颤的关系
肖 婷*,张献斌,罗 磊,杨 娜,梁 晗,许新录
(商洛市中心医院心血管内科,商洛 726000)
分析慢性心力衰竭(CHF)患者血尿酸(SUA)水平与房颤(AF)的关系。回顾性地分析2010年1月至2014年2月期间在商洛市中心医院心血管内科住院的218例CHF患者的人口学资料、既往相关病史、血液生化指标、超声心动图及颈部血管超声结果。根据是否AF将218例患者分为AF组和窦性心律组。218例患者中,有49例合并AF,169例为窦性心律,AF发生率为22.5%。与窦性心律组相比,SUA水平在AF组明显升高。AF组的年龄比窦性心律组更高[(64.32±9.87)(56.78±10.14)岁,<0.05。];射血分数前者比窦性心律组低,差异有统计学意义(<0.05);而包括左心房内径、左心室舒张末内径、左心室收缩末内径等在内的超声心动图参数,AF组比窦性心律组高;颈动脉内膜中层厚度AF组也明显高于窦性心律组(<0.05)。多因素logistic回归分析显示,SUA水平为发生AF的独立危险因素。AF组患者有更高的SUA水平和更差的心功能。
心力衰竭;尿酸;心房颤动
心房颤动(atrial fibrillation,AF),是临床上最常见的一种心律失常。近年来,国外的诸多研究均表明,血尿酸(serum uric acid,SUA)水平升高增加了AF发生的危险;但国内此方面的研究报道却寥寥无几。本文通过对住院慢性心力衰竭(chronic heart failure,CHF)患者的相关资料进行分析,从而探寻SUA与AF之间的关系。
1 对象与方法
1.1 研究对象
选择2010年1月至2014年2月期间在商洛市中心医院心血管内科住院的CHF患者218例,现阶段无感染、肿瘤等导致血清超敏C反应蛋白(high sensitivity-C reactive protein,hs-CRP)、红细胞沉降率(erythrocyte sedimentation rate,ESR)升高的疾病、既往无痛风或高尿酸血症病史,未服用别嘌醇(allopurinol)、丙磺舒(probenecid)、苯溴马隆(benzbromarone)、氢氯噻嗪(hydrochlorothiazide)等影响尿酸代谢的药物,无肾功能不全病史。
1.2 方法
1.2.1 临床资料的采集 入院后收集患者的一般资料如年龄、性别、吸烟、体质量指数(body mass index,BMI)、高血压史、糖尿病史。
1.2.2 实验室指标的测定 所有患者入院后根据肾脏病膳食改良研究(Modification of Diet in Renal Disease study,MDRD)公式[1]计算肾小球滤过率(glomerular filtration rate,GFR)、测定SUA、甘油三酯(triglycerides,TG)、总胆固醇(total cholesterol,TC)、低密度脂蛋白胆固醇(low-density lipoprotein- cholesterol,LDL-C)、高密度脂蛋白胆固醇(high-density lipoprotein- cholesterol,HDL-C)、hs-CRP、标准十二导联心电图、卧位超声心动图、颈部血管超声等。
1.3 统计学处理
2 结 果
2.1 AF组与窦性心律组患者的一般情况
218例患者中AF组49例,窦性心律组169例,AF患病率22.5%,AF组比窦性心律组年龄大(<0.05)。其中AF组男性患者32例,占该组总例数65.31%,窦性心律组男性患者86例,占该组总例数50.89%,两组性别比较差异有统计学意义(=0.009)。两组患者在高血压、糖尿病史、血脂、估测GFR(eGFR)、BMI方面差异无统计学意义(>0.05;表1)。
2.2 AF组与窦性心律组患者炎性指标及心功能比较
与窦性心律组相比,AF组SUA、hs-CRP、ESR均明显升高,差异有统计学意义(<0.05;表2)。
与窦性心律组相比,AF组的颈动脉内膜中层厚度(intima-media thickness,IMT)明显增厚,且射血分数明显降低;左心房内径、左心室舒张末内径、左心室收缩末内径等超声心动图指标,AF组均高于窦性心律组(<0.05 ;表2)。
2.3 AF发生的多因素logistic回归分析
按是否AF对218例患者先行单因素相关分析,筛选出有统计学意义的变量为SUA、hs-CRP、左心房内径。然后对上述变量行多因素logistic回归分析,发现SUA[OR=1.425,95%可信区间(confidence interval,CI):1.164~1.658,<0.01]、左心房内径(OR=1.193,95%CI:1.009~1.405,<0.05)为影响CHF患者AF发生的独立危险因素。其中SUA水平越高,左心房内径越大,AF发生的风险则越高。
3 讨 论
AF是器质性心脏病最常合并的心律失常,且可导致脑卒中和其他血栓栓塞并发症,并诱发和加重心衰,有很高的致死率与致残率[2]。与非AF患者相比,AF患者有大约4~5倍的卒中风险、2倍左右的痴呆风险、3倍左右的心衰风险,全因死亡可升高40%~90%[3]。
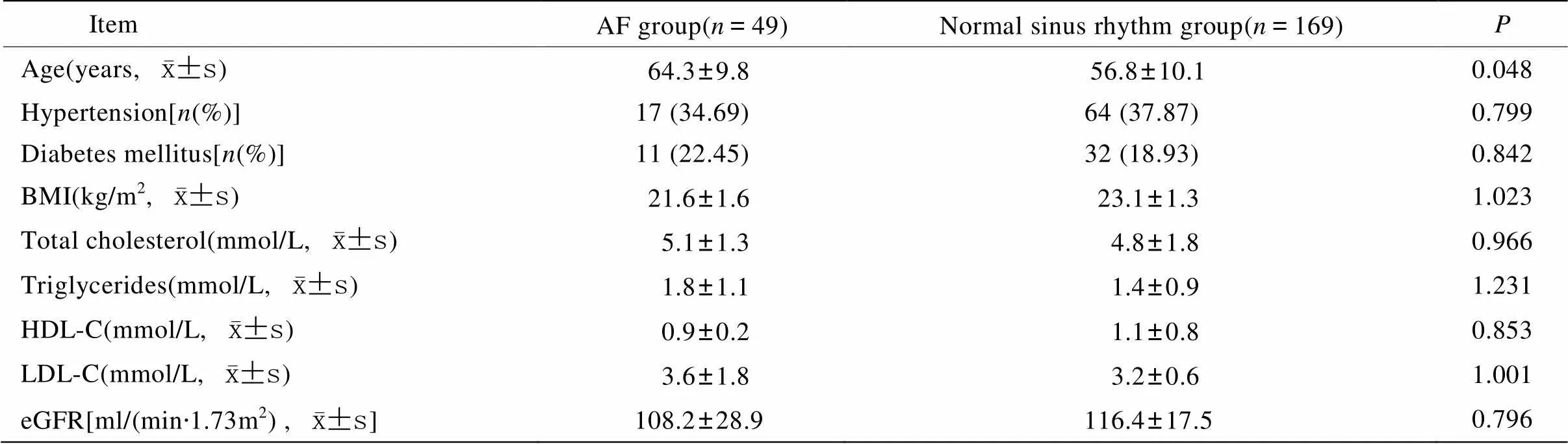
表1 AF组与窦性心律组患者临床一般资料比较
AF: atrial fibrillation; BMI: body mass index; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; eGFR: estimated glomerular filtration rate

表2 AF组与窦性心律组患者炎性指标及心功能比较
AF: atrial fibrillation; SUA: serum uric acid; hs-CRP: high sensitivity-C reactive protein; IMT: intima-media thickness; LVEF: left ventricular ejection fraction; LVESD: left ventricular end-systolic diameter; LAD: left atrial diameter; LVEDD: left ventricular end-diastolic diameter; ESR: erythrocyte sedimentation rate. Compared with normal sinus rhythm group,*<0.05
据统计,AF在成人中总人群发病率为1%,且随着年龄的增加发病率增加,<60岁的人群发病率约1%,而>80岁者发病率则高达6%[4]。我们的研究也证实,AF组患者年龄较窦性心律组高,两组间差异具有统计学意义(<0.05)。这可能与老年患者器质性心脏病患病率高、心脏病史时间长、心脏扩大尤其是左心房扩大,最终引起患者心肌重塑而发生AF。
研究表明炎症、氧化应激参与AF发生发展、导致心房电重构及结构重构[5]。尿酸是体内嘌呤代谢的终产物,高尿酸血症的发生也与氧化应激和炎症密切相关[6,7]。本文的研究表明,AF组患者SUA水平明显高于对照组,且该组与炎症相关的指标如ESR、hs-CRP均高于窦性心律组。SUA的产生过程需要两步反应:次黄嘌呤转化为黄嘌呤和黄嘌呤转化为尿酸,这两步反应都需要黄嘌呤氧化酶(xanthine oxidase,XO)的催化。SUA水平升高反映XO活性增加。XO激活过多可导致活性氧簇(reactive oxygen species,ROS)产生过多,ROS通过一系列的作用,最终导致心房结构性重构,从而引起AF的发生[8]。Letsas等[9]首先评价了SUA水平与AF的关系,结果显示与对照组相比,阵发性AF和永久性AF患者SUA水平均显著增高;多变量分析也显示SUA是永久性AF的独立预测因素。Liu等[10]评价了SUA水平与高血压患者发生AF的相关关系,伴有AF的高血压患者SUA水平显著升高,多变量回归分析提示SUA水平是高血压患者发生AF的独立危险因素。本文的研究也证实SUA与AF的发生明显相关,是其发生的独立危险因素。
本文的研究还表明,AF组患者的IMT明显高于窦性心律组,两组比较差异有统计学意义。众所周知,动脉粥样硬化斑块的形成是一系列复杂的过程,与炎症反应、氧化应激、遗传等多种因素有关[11],而尿酸的形成具有类似的机制,这也为AF组患者SUA水平高于对照组提供了理论依据。本文的研究还表明,在反映心脏收缩功能的指标射血分数上,AF组低于窦性心律组;在其他如左心房内径、左心室舒张末内径、左心室收缩末内径等反映CHF患者心功能的客观指标上,AF组明显高于窦性心律组(<0.05),而上述指标越高,则表明心功能越差。这就间接为SUA成为多种缺血性心脏病、心衰患者的重要血浆标志物提供了理论依据,从侧面可反映病情的严重程度,与疾病的发病率和死亡率密切相关[12−16]。
总之,通过本研究表明尿酸在伴有CHF的AF患者血清中升高,尤其在男性患者中升高显著,通过SUA水平检测,对评价病情有一定的参考价值。但发生AF的SUA水平、SUA对CHF合并AF的患者AF转复后复发的预测方面尚需更多具有说服力的大样本前瞻性研究。
[1] Ma YC, Zuo L, Chen JH,. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease[J]. J Am Soc Nephrol, 2006, 17(10): 2937−2944.
[2] Numa S, Hirai T, Nakagawa K,. Hyperuricemia and transesophageal echocardiographic thromboembolic risk in patients with atrial fibrillation at clinically low-intermediate risk[J]. Circ J, 2014, 78(7): 1600−1605.
[3] Tamariz L, Hernandez F, Bush A,. Association between serum uric acid and atrial fibrillation: a systematic review and meta-analysis[J]. Heart Rhythm, 2014, 11(7): 1102−1108.
[4] Tekin G, Tekin YK, Erbay AR,. Serum uric acid levels are associated with atrial fibrillation in patients with ischemic heart failure[J]. Angiology, 2013, 64(4): 300−303.
[5] Korantzopoulos P, Kolettis TM, Galaris D,. The role of oxidative stress in the pathogenesis and perpetuation of atrial fibrillation[J]. Int J Cardiol, 2007, 115(2): 135−143.
[6] Doehner W, Landmesser U. Xanthine oxidase and uric acid in cardiovascular disease: clinical impact and therapeutic options[J]. Semin Nephrol, 2011, 31(5): 433−440.
[7] Landmesser U, Spiekermann S, Preuss C,. AngiotensinⅡ induces endothelial xanthine oxidase activation: role for endothelial dysfunction in patients with coronary disease[J]. Arterioscler Thromb Vasc Biol, 2007, 27(4): 943−948.
[8] Glantzounis GK, Tsimoyiannis EC, Kappas AM,. Uric acid and oxidative stress[J]. Curr Pharm Des, 2005, 11(32): 4145−4151.
[9] Letsas KP, Korantzopoulos P, Filippatos GS,. Uric acid elevation in atrial fibrillation[J]. Hellenic J Cardiol, 2010, 51(3): 209−213.
[10] Liu T, Zhang X, Korantzopoulos P,. Uric acid levels and atrial fibrillation in hypertensive patients[J]. Intern Med, 2011, 50(8): 799−803.
[11] Sun Y, Yu X, Zhi Y,. A cross-sectional analysis of the relationship between uric acid and coronary atherosclerosis in patients with suspected coronary artery disease in China[J]. BMC Cardiovasc Disord, 2014, 14: 101.
[12] Dawson J, Walters M. Uric acid and xanthine oxidase: future therapeutic targets in the prevention of cardiovascular disease[J]? Br J Clin Pharmacol, 2006, 62(6): 633−644.
[13] George J, Struthers AD. The role of urate and xanthine oxidase inhibitors in cardiovascular disease[J]. Cardiovasc Ther, 2008, 26(1): 59−64.
[14] Ndrepepa G, Braun S, Haase HU,. Prognostic value of uric acid in patients with acute coronary syndromes[J]. Am J Cardiol, 2012, 109(9): 1260−1265.
[15] Nyrnes A, Toft I, Njølstad I,. Uric acid is associated with future atrial fibrillation: an 11-year follow-up of 6308 men and women—the Tromso Study[J]. Europace, 2014, 16(3): 320−326.
[16] Kaya EB, Yorgun H, Canpolat U,. Serum uric acid levels predict the severity and morphology of coronary atherosclerosis detected by multidetector computed tomography[J]. Atherosclerosis, 2010, 213(1): 178−183.
(编辑: 李菁竹)
Relationship of serum uric acid with atrial fibrillation in patients with chronic heart failure
XIAO Ting*, ZHANG Xian-Bin, LUO Lei, YANG Na, LIANG Han, XU Xin-Lu
(Department of Cardiology, Central Hospital of Shangluo City, Shangluo 726000, China)
To analyze the association of serum uric acid (SUA) with atrial fibrillation (AF) in the patients with chronic heart failure (CHF).A total of 218 CHF patients admitted in our department from January 2010 to February 2014 were enrolled in this study. Their demographic data, medical history, blood biochemical parameters, ultrasonic echocardiogram and cervical vascular ultrasound results were collected and retrospectively analyzed. The patients were divided into 2 groups, that is, normal sinus rhythm group and AF group.Of 218 CHF patients, 49 patients (22.5%) had AF, and 169 patients were in normal sinus rhythm. SUA was significantly higher in the patients with AF than those with normal sinus rhythm (<0.05). AF patients were older than those with normal sinus rhythm [(64.32±9.87)(56.78±10.14) years,<0.05], had lower ejection fraction (EF,<0.05), higher values in echocardiographic parameters, such as left atrium diameter, left ventricular end-diastolic diameter, and left ventricular end systolic diameter, and obviously larger intimal medial thickness (<0.05). Multivariate logistic regression analysis showed that SUA was the independent risk factor for AF.AF patients have significantly higher SUA levels, and poorer heart function.
heart failure; uric acid; atrial fibrillation
R541.61
A
10.11915/j.issn.1671-5403.2015.04.068
2015−01−13;
2015−03−16
肖 婷, E-mail: xiaotingr@sina.com
猜你喜欢
红蜻蜓·中年级(2024年5期)2024-06-14 09:11:51
建筑与预算(2024年1期)2024-03-01 09:23:04
中国临床医学影像杂志(2022年5期)2022-07-26 07:11:48
趣味(作文与阅读)(2021年12期)2021-04-19 12:16:54
保健与生活(2020年24期)2020-12-23 06:59:18
哈尔滨轴承(2020年1期)2020-11-03 09:16:18
戏剧之家(2018年35期)2018-02-22 12:32:40
分析化学(2017年12期)2017-12-25 11:42:47
作文评点报·高中版(2017年9期)2017-03-27 13:20:15
中国当代医药(2015年22期)2015-03-01 02:05:16
