
A simple practical balloon anchoring technique within the guide catheter for chronic total occlusion(CTO) of the coronary artery
2015-02-14 02:40:11LeileiChen,YiCheng,YangYang等
A simple practical balloon anchoring technique within the guide catheter for chronic total occlusion(CTO) of the coronary artery
Dear Editor:
Chronic total occlusions(CTOs)of the coronary artery are commonly encountered complex lesions[1]. Percutaneous coronary intervention(PCI)for CTO is technically challenging due to low procedural success rates[2].Microcatheter is one of the important devices for treatment of CTO[3].It has been widely used attributed to the excellent crossability whenever angulation and tortuousity of the coronary artery is encountered[4].In the process,the microcatheter has to be withdrawn from the guide wire after the wire is proved to locate in the true lumen.For microcatheter removal, the guidewire should be fixed to avoid shifting by either adding prolonged wire to the guidewire or using prolonged wire(such as RG3)at the beginning of the operation,and then pressing the proximal part of the guidewire to fix it.However,in actual operation,the distal part of the guidewire may shift.Besides,the time for removing the microcatheter is much longer with prolonged guidewire.
To overcome the previous problem,we designed a new technique for withdrawing the microcatheter:the balloon anchoring technique within the guide catheter. Detailed steps are as follows:(1)Insert the guidewire into the occluded segment in support of the microcatheter and insert the microcatheter into the occluded segment alongside the wire.Remove the wire when it has arrived at distal vascular lesions through the occluded segment the wire.After the wire is proved to locate in the ture lumen of blood vessel by the contrast agent injected from the microcatheter,the wire is advanced into the occluded segment.(2)Withdraw the microcatheter several centimeters in the guide catheter(probably at the end of ascending aorta).(3)Insert a predilation balloon with diameter ranged from 2.0-2.5mm(the balloon can be used in percutaneous transluminal coronary angioplasty(PTCA)afterwards)into the distal end of the catheter via the guide catheter on the outside of the microcatheter(Fig.1A). (4)Release the balloon with pressure ranged from 8 to 10atm and press the guidewire on the wall of the guide catheter,then withdraw the microcatheter with slow and uniform speed under X-ray fluoroscopy(Fig.1B).(5)Withdraw the predilation balloon gradually when the microcatheter is completely removed.

Fig.1 Detailed steps of the new technique for withdrawing the microcatheter.A:The microcatheter is withdrawn to the end of the ascending aorta.The predilation balloon is advanced into the distal microcatheter alongside the guide catheter.B:Release the predilation balloon at 8-10atm.The guidewire is anchored at the wall of the guide catheter to fix the guidewire and then the microcatheter is withdrawn.
Here we present a case which was performed with the new tchnique.A 84-year-old male patient was admitted to our hospital because of chest tightness for 8years. Conventional coronary angiography demonstrated approximately 60-70% stenosis in proximal-segment of left anterior descending artery(LAD),around 50% steno-sis in proximal-segment of diagonal branch and around 90% steno-sis in proximal-segment of OM 2.Left circumflex artery(LCx):30% stenosis in proximal-segment and 60% stenosis in distal-segment.Coronary angiography showed a CTO of the proximal right coronary artery (RCA).No stenosis was found in LM.After seeking theconcurrence of a relative,PCI for CTO of RCA was performed.SAL guiding catheter arrived at the RCA orifice with additional unfractionated heparin 8000u.FIELDXT gained access to the distal-segment through the occluded part under the guidance of the microcatheter, withdrew the microcatheter,Stent implantation was successfully performed using a 2.5*32mm and 2.75*38mm TAXUS stent from the distal to the proximal part following PTCA,followed by post-balloon dilatation.A Runthrough NS guide wire was advanced at the diatal part through the lesion.A 2.25*18mm ENDEAVOR stent was successfully implanted at the lesion after a 2.0*15mm SPRINTER balloon predialation.The operation was successful and the patient returned to the ward safely.
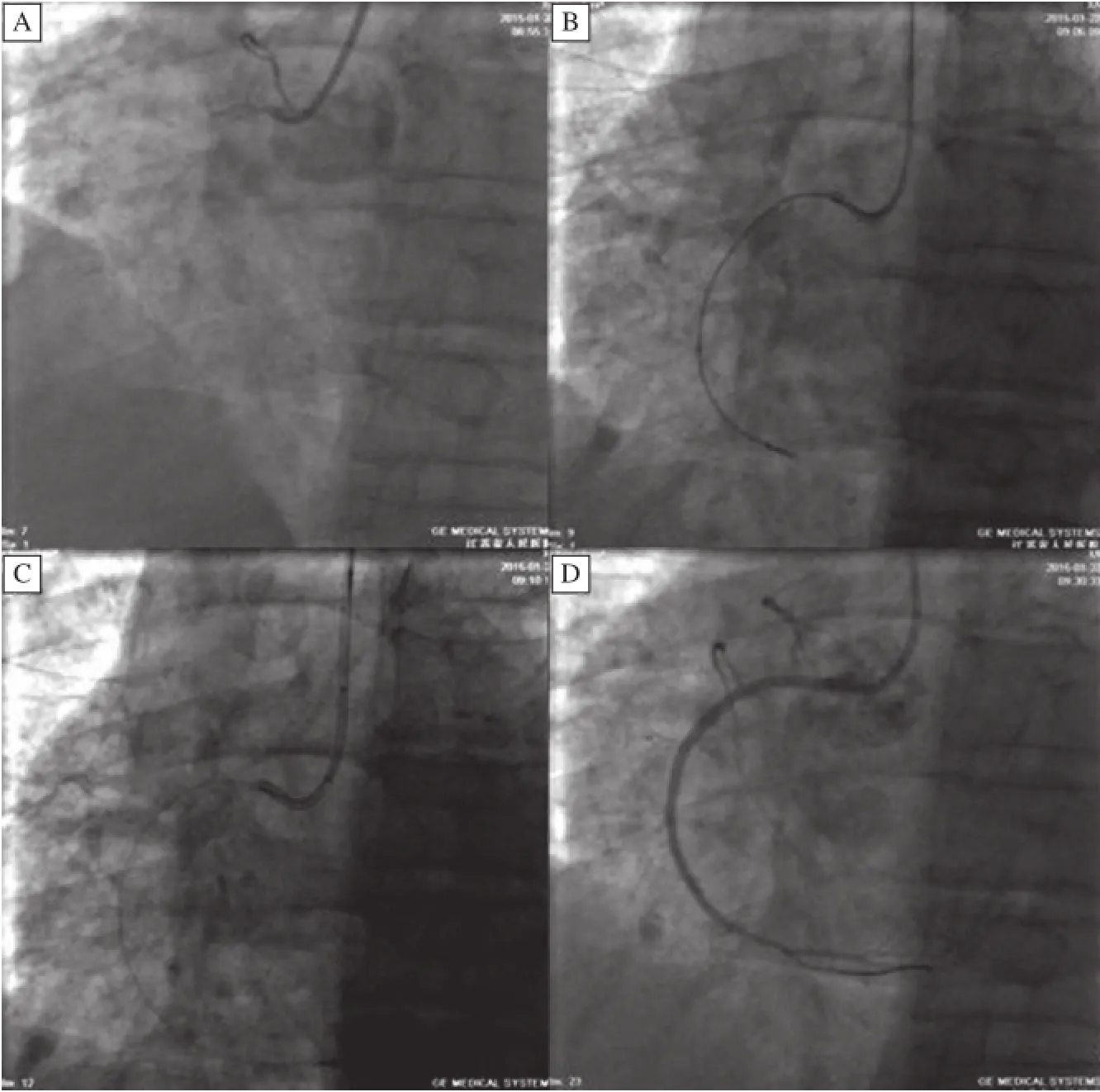
Fig.2 Ope ration process of the patient performed with the new technique.A:CAG showed completely obstruction in the proximal RCA. B:The microcatheter advanced into the distal part of the RCA through the CTO lesion.C:The microcatheter was withdrew within the guide catheter(at the end of the the ascending aorta).The balloon was dilated with 8-10atm when the predilation balloon was inserted 2-3cm distal the microcatheter to fix the guidewire at the inside wall of the guide catheter.The microcatheter was withdrawn slowly with no shifting of the guidewire.D:CAG after the operation showed nostenosis in the distal vessels of RCA and TIM I 3 flow.
Withdraw microcatheter with the balloon anchoring technique within the guide catheter has the following advantages over the traditional technique with prolonged wire:(1)The traditional technique is to fix the proximal wire.In the process of withdrawal microcatheter,the guidewire is much likely to shift.If the guidewire move to the distal part,there are risks as damaging the vessels, dissection and vascular perforation.If the guidewire move to the proximal part,the guidewire is in danger of exiting the CTO lesion.It is difficult for the guidewire to traverse the CTO again.The increase of the operation time,contrast agent dosage and X-ray exposure time adds to the occurrence of complications and operation failure.In the technique we introduce here,the guidewire is anchored at the inside wall of guide catheter with 8-10atm produced by the balloon.The pressure is enough to fix the wire. Besides,anchor point is near the distal wire,which decreases the possibility of the distal wire shifting. Moreover,the speed of withdrawing the microcatheter is faster with the introduced technique than that with traditional technique.(2)Compared with the technique that using prolonged wire(such as RG3)at the beginning of the operation,the time that the technique costs is decreased because of the short wire,decreasing X-ray exposure time and contrast agent dosage.(3)The operator does not need to press the proximal guidewire.The operator can withdraw the microcatheter with one hand,and fix the guide catheter with the other hand,reducing the possibility of guide catheter shifting and the difficulty of operation, mean while increasing the operation safety.
In summary,the balloon anchoring technique within the guide catheter could withdraw the microcatheter faster and more convenient,reduce the operation time, contrast agent dosage,X-ray exposure time,the difficulty of operation and the occurrence of complications, the guidewire shifting.The technique is simple,safe and effective for CTO-PCI operators,and it is why we decide to promote the technique.
This work was supported by grants from the Project Funded by the Science and Technological Innovation Group of Jiangsu Higher Education Institution‘Qing-Lan Project’(JX2161015030)and a Project Funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions(PAPD).
Yours sincerely,
Leilei Chen1,△,Yi Cheng1,2,△,Yang Yang1,
Zhen Zhang1,Dingguo Zhang1,Liansheng Wang1,✉
1Department of Cardiology,the First Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China.
2Department of Cardiology,the First People' Hospital of Suqian,Suqian,Jiangsu 223800,China.
△Lei-lei Chen and Yi Cheng contributed equally to this work.
✉Correspondent author:Liansheng Wang,MD,PhD, Department of Cardiology,the First Affiliated Hospital of Nanjing Medical University,300 Guangzhou Road, Nanjing,210029,Jiangsu Province,China.E-mail: drlswang@njmu.edu.cn,Fax/Tel.:0086-25-83724440
[1] Fefer P,Knudtson ML,Cheema AN,et al.Current perspectives on coronary chronic total occlusions:the Canadian Multicenter Chronic Total Occlusions Registry[J].J Am Coll Cardiol,2012,59:991-997
[2] Grantham JA,Marso SP,Spertus J,et al.Chronic totaI occlusion angioplasty in the United States[J].J Am Coll Cardiol Intv,2009,2:479-486
[3] Tsuchikane E,Katoh O,Shimogami M,et al.First clinical experience of a novel penetration catheter for patients with severe coronary artery stenosis[J].Catheter Cardiovasc Interv,2005,65(3):368-373
[4] Otsuka Y,Nakamura K,Saito T.Usefulness of the Corsair microcatheter for treatment of complex chronic total occlusion[J].J Invasive Cardiol,2012,24(2):E35-E38
Received 05 May 2015,Revised 28 May 2015,Accepted 09 June 2015, Epub 30 July 2015.
R714.252,Document code:B
The authors reported no conflict of interests.
©2015 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.29.20150068
 THE JOURNAL OF BIOMEDICAL RESEARCH2015年5期
THE JOURNAL OF BIOMEDICAL RESEARCH2015年5期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Serum IL-1βand IL-18 correlate with ESR and CRP in m ultid rug-resistant tuberculosis patients
- Prostate-specific antigen doubling time and response to cabazitaxel in a hormone-resistant metastatic prostate cancer patient
- Assessment of phytochemicals and antioxidant activities of raw and germinating Ceiba pentandra(kapok)seeds
- Diacerein protects against iodoacetate-induced osteoarthritis in the femorotibial joints of rats
- Differential mRNA expression profiling of oral squamous cell carcinoma by high-throughput RNA sequencing
- Acute effect of aspartame-induced oxidative stress in Wistar albino rat brain