
So much research,so little application:Barriers to dissemination and practical implementation of Tai Ji Quan
2014-03-21 01:41PeterHarmer
Peter A.Harmer
Department of Exercise Science,Willamette University,Salem,OR 97301,USA
So much research,so little application:Barriers to dissemination and practical implementation of Tai Ji Quan
Peter A.Harmer
Department of Exercise Science,Willamette University,Salem,OR 97301,USA
Despite the large number of articles published in the medical literature advocating the use of Tai Ji Quan for a wide variety of health-related outcomes,there has been little systematic broad-scale implementation of these programs.It may be argued that the lack of funding from organizations capable of implementing and overseeing large-scale programs,such as governmental health agencies or national non-governmental organizations concerned with healthcare for older adults,is to blame.However,the evidence these organizations need to justify underwriting such programs is in short supply because of conflicting priorities and standards related to determining the efficacy and effectiveness of Tai Ji Quan.Establishing efficacy through acceptable designs such as randomized controlled trials involves strict protocols to ensure meaningful internal validity but different approaches are needed to demonstrate meaningful effectiveness(external validity)outside the study setting.By examining the quality,quantity,and relative proportions of the randomized controlled trials,systematic reviews,and dissemination studies reported in the medical literature,this paper highlights the disparity in emphasis between efficacy and effectiveness research that has impeded the development of a cohesive literature on Tai Ji Quan and concludes that until more researchers develop a systematic,long-range commitment to investigating its health-related benefits,the research related to Tai Ji Quan will remain fractured and sporadic,limiting the incentive of large funding agencies to support its wide-spread use.
Dissem ination;Effectiveness;Efficacy;Practical trials;Randomized controlled trial;Tai Ji Quan
1.Introduction
Tai Ji Quan is a form of physical and mental training derived from the Chinese martial art of Wushu1that has become increasingly popular among older adults outside of China over the past 40 years because of its purported beneficial effects on physical and mental well-being.While its signature slow,rhythmic,no-impact movement characteristics have obvious appeal to this demographic,whether practicing Tai Ji Quan can actually enhance health by improving physical function,diminishing the risk of disease or curing illness is still unclear for the majority of conditions to which it has been applied.2Although there is a growing body of research supporting the value of Tai Ji Quan practice in maintaining or improving health-related quality of life,overall the evidence is limited,fractured,and poorly reported.3Because wide-spread implementation of any health intervention requires the support of state or national agencies,whether governmental or nongovernmental,it may be argued that the lack of a cohesive and compelling literature on Tai Ji Quan has impeded its use as a population-level health intervention even as more studies examining the health value of Tai Ji Quan across an increasing range of conditions appear in the literature.The apparent disconnect between the grow ing interest in Tai Ji Quan by medical researchers,clinicians and the general public and the reluctance of funding agencies to promote Tai Ji Quanprograms on a large scale may be found in the fact that primarily two different types of evidence are needed by funding agencies4before they are willing to underw rite a public health initiative—evidence of efficacy and evidence ofeffectiveness, including cost-effectiveness— but the vast majority of researchers have only focused on establishing efficacy,and often not very well,in“one off”studies.
2.Efficacy vs.effectiveness
Although efficacy and effectiveness are often used interchangeably,it is useful to parse their difference to understand the problems facing Tai Ji Quan as a population-level health promotion program.Efficacy is considered the capacity of an intervention to produce a beneficial change under ideal circumstances,such as in a research setting,but effectiveness is determined by how well the intervention works in the real world.5From a research design standpoint,establishing efficacy is primarily concerned with internal validity while the key issue for effectiveness is external validity;therefore each has different research design considerations and standards by which to establish its value.While there are several research designs that can be used to determine efficacy,well-designed randomized controlled trials(RCTs)are considered the gold standard in this regard because of their methodological framework with in which strict controls allow the intervention to show its causal relationship to an outcome,if such a relationship exists,and remove alternative explanations for any change(s)identified.Unfortunately,there is no universal gold standard to determine effectiveness although the RE-AIM model6has found increasing favor among researchers for its theoretical grounding and the appropriateness of the evaluation dimensions of the model as they relate to the feasibility of introducing an intervention into a community setting.The five parts of RE-AIM cover individual-level aspects(Reach and Efficacy),organization-level considerations(Adoption and Implementation),and shared(individual and organization) responsibilities(Maintenance).Finally,potential health promotion organizations need evidence that funding a program will be fiscally responsible,that is,even if a program is shown to be efficacious and effective,it has to have significant returnon-investment capacity in terms of health gained to money spent to be worthwhile implementing.Cost-effectiveness analysis typically involves measures such as dollars per quality adjusted life year(QALY)gained or disability adjusted life year(DALY)prevented to quantify the financial burden against health gain.7,8
Given this background,the preponderance of efficacy studies in Tai Ji Quan research is understandable.If efficacy cannot be demonstrated it makes little sense to try to implement a program outside the research setting(i.e.,determine effectiveness)and less sense to consider any potential costbenefits issues as there are no discernable benefits.Alternatively,the ideal process should begin with well-designed RCTs that drive the development of programs that can be implemented in community settings and that maximize health improvement per dollar spent compared to existing interventions.9,10Unfortunately,this logical sequence has been stalled at the first step by the questionable quality of many RCTs and the paucity of coordinated research programs on Tai Ji Quan that go beyond one-time,isolated efficacy studies.The problem is highlighted by the relative numbers of different types of reports in the medical and healthcare literature.Table 1 summarizes the results of a search on PubMed/Medline,the largest medical literature resource in the world,conducted in September2013 using all variations of the term Tai Ji Quan.A total of 710 articles were returned,of which only nine were published prior to 1990(including 2 RCTs).Given that Tai Ji Quan was only introduced into the American mainstream in the 1970s,the lack of scientific interest before 1990 in what may have been considered,at best,a type of complementary and alternative medicine or,at worst,a fringe activity or quackery is not surprising.However,Tai Ji Quan continued to spread to the point that according to a National Health Interview Survey report published in 2007,almost 2.5 million Americans indicated they had practiced Ti Ji Quan in the previous year.11Paralleling participant grow th was interest from the scientific and medical communities,spurred by the pioneering work of Wolf,12—14as seen in the number of Tai Ji Quan-related publications since 1990,including 173 RCTs and 162 reviews.
However,it is instructive to note the significant increase in the number of review papers,especially over the past5 years, compared to the grow th of RCTs.Systematic and critical reviews,often involving meta-analyses,are designed to summarize the current state of know ledge in a field and to impose some order on disparate findings.It is clear from the conclusions of the most recent reviews that the field of Tai Ji Quan research is very active but in disarray.
For example,the 27 reviews involving Tai Ji Quan(either as the primary intervention for a particular condition or as one of several interventions investigated to determine their effect on a particular condition)published between January 2012 and October 2013 covered 15 different conditions,including fall prevention,15—18rheumatology,18—23Parkinson’s disease,24—26fibromyalgia,27,28psychological conditions,29—32cardiovascular conditions,33—36peripheral neuropathy,37and chronic pain.38Despite the range of conditions being investigated,the consensus of the reviews’authors is that the research literature,including that involving RCT,leaves much to be desired. Too few studies involving specific conditions,small sample sizes,poor protocols,inadequate controls,inconsistent intervention characteristics(e.g.,dosage,format),and w idely varying project lengths and outcome variables(even for thesame condition)were determined to undermine the value of the findings from these studies and/or make it difficult to discern a clear relationship between Tai Ji Quan and conditions of interest.
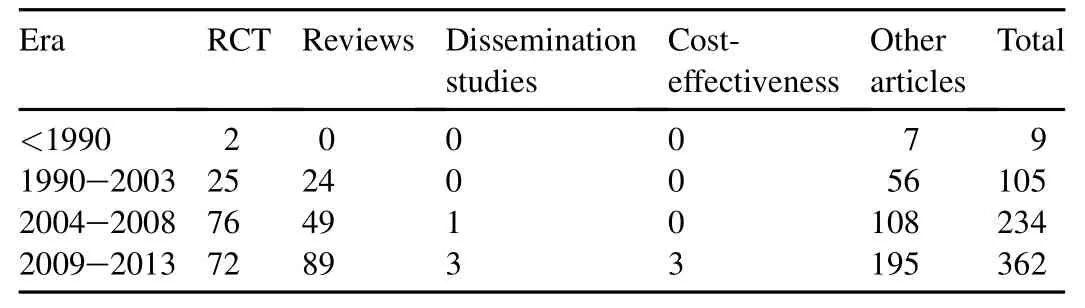
Table 1 Number and types of articles on Tai Ji Quan indexed in Medline/PubMed.
Not surprisingly,the most consistent recommendation from these reviews was for more,better designed and conducted RCTs to avoid the problems that detract from the credibility of the results.There was no recommendation to increase research on the effectiveness of Tai Ji Quan.Given that evidence of efficacy is the foundation on which any subsequent work must be based,this position is quite logical.If the intervention cannot demonstrate an effect under the“ideal”conditions involved in RCT,there is little to argue for implementing it in an environment such as a community setting that is less conducive to its effects becoming evident.
3.The importance of a coordinated approach to research
However,this appeal for better efficacy evidence by increasing the number of RCTs may be misplaced.If the majority of RCTs,even if well conducted,are not part of a coordinated research program then the literature will remain a collection of disparate results that makes clearly identifying the utility of Tai Ji Quan as a prevention program or health promoting activity problematic because of random and significant variations in intervention characteristics,protocols, sample populations and outcome variables.For example,of the 175 Tai Ji Quan RCTs indexed by Medline/PubMed,112 involved one-time only research groups;11 principal investigators(PIs)conducted two Tai Ji Quan RCTs,seven groups had three RCTs and two PIs had four each.While a lack of cohesion in the study details of the one-time only groups is to be expected,it is instructive to note that of the multiple RCT researchers only Li and colleagues39—45had specifically developed and systematically implemented a Tai Ji Quan protocol across all of their studies.Appropriately this line of research produced two of the four dissemination studies,with a pilot developmental phase44and a full implementation project,45in accordance with the framework discussed previously(three of the dissemination studies involved fall prevention44—46and one involved end-stage renal disease47).The remaining two dissemination studies,46,47as well as one large RCT investigating fall prevention that was implemented in community settings,48were not built on any specific precedent efficacy research and constituted a form of pragmatic or practical clinical trial.4Nonetheless,two of the implementation projects for fall prevention45,46aptly used the RE-AIM model to measure the effectiveness of their intervention.The results,if applied appropriately,can provide a meaningful foundation for the feasibility of large-scale community implementation and future cost-effectiveness analysis.
with fall prevention being the most common application of Tai Ji Quan health-related research,the fact that the only cost effectiveness studies related to Tai Ji Quan available to date49—51all focus on fall prevention is not unreasonable. However,all three involved statistical modeling that did not use data from specific RCT or implementation studies but rather secondary analyses based on systematic reviews and meta-analytic techniques.Although they are important first steps in building a critical mass of evidence that can be used by policy-makers to determine how to best promote population health,data from actual implementation studies are needed to ensure an accurate understanding of Tai Ji Quan fall prevention cost-benefits for various programs.Additionally,as noted by Frick and colleagues,51notonly does the cost-effectiveness of individual fall prevention programs need to be established but the relative cost-effectiveness of different programs is critical to identifying best practices and ensuring integrated healthcare systems allocate resources in the most fiscally prudent way.For example,of the three Tai Ji Quan programs14,44,48recommended by the U.S.Centers for Disease Control and Prevention (CDC)as fall prevention interventions,52only one44has been funded by the CDC and specifically translated into a community-based program, formally tested for its effectiveness,and implemented in multiple states across the country.9Having a program like this, with proven efficacy,translated into a format that meets the recommendations to be a covered service under multiple sections of the Affordable Care Act10,53(the U.S.government mandate that requires both government and private insurers to provide coverage for prevention services with out co-pays or cost-sharing)opens a significant door to broad dissemination. However,without additional programs against which to measure the real-world impact of this one program the potential to identify the Tai Ji Quan fall prevention framework that will have the greatest influence on the health of the population will be unrealized.
4.Conclusion
There is little doubt that Tai Ji Quan has gained a substantial following with in the healthcare community as researchers and clinicians look for new and more powerful interventions to prevent,treat or cure illness and injuries associated with modern life.The depth of its impact in the consciousness of medical researchers may be seen by the fact that in reviews for two disparate conditions(phantom limb pain54and stress incontinence in women55),the authors specifically comment on the absence of Tai Ji Quan studies related to these conditions.However,it is more clearly evident in the increasing number of studies using Tai Ji Quan to address a growing array of conditions ranging from ager elated decline in physical function to psychological wellbeing and metabolic pathologies.Unfortunately,very little of the work done to date is part of a deliberate and well-planned strategy to systematically address efficacy,effectiveness and cost-effectiveness issues related to Tai Ji Quan as an intervention to prevent health declines or to enhance physical and psychological function.Despite the high quality of some individual research projects,methodological weaknesses in Tai Ji Quan efficacy studies and the overall disjointed and inconsistent research approach to exam ining Tai Ji Quan does not provide sufficient grounds for governmental or nongovernmental organizations to underwrite comprehensiveimplementation of Tai Ji Quan for the good of the public’s health.10,53Concerted,systematic and coordinated long-term research programs by individual researchers or collaborative groups are critical if the full potential of Tai Ji Quan to enhance health-related quality of life is to be realized on a broad scale.
Acknowledgment
The work presented in this paper is supported in partby a research grant from the National Institute on Aging (AG034956).
1.Guo Y,Qiu P,Liu T.Tai Ji Quan:an overview of its history,health benefits,and cultural value.J Sport Health Sci2014;3:3—8.
2.Lee M,Ernst E.Systematic reviews of t’ai chi:an overview.Br J Sports Med2012;46:713—8.
3.Li JY,Zhang YF,Smith GS,Xue CJ,Luo YN,Chen WH,etal.Quality of reporting of randomized clinical trial in tai chi interventions—a systematic review.Evid Based Complement Alternat Med2011;2011:383245. http://dx.doi.org/10.1093/ecam/nep022.
4.Zwarenstein M,Oxman A.Why are so few randomized trials useful,and what can we do about it?J Clin Epidemiol2006;59:1125—6.
5.Dorland’s illustrated medical dictionary.32nd ed.Philadelphia,PA: Elsevier/Saunders;2011.
6.Glasgow R,Vogt T,Boles S.Evaluating the public health impact of health promotion interventions:the RE-AIM framework.Am J Public Health1999;89:1322—7.
7.Cobiac L,Vos T,Barendregt J.Cost-effectiveness of interventions to promote physical activity:a modeling study.PLoS Med2009;6:e1000110. http://dx.doi.org/10.1371/journal.pmed.1000110.
8.Roux L,Pratt M,Tengs TO,Yore MM,Yanagawa TL,Van Den Bos J, et al.Cost effectiveness of community-based physical activity interventions.Am J Prev Med2008;35:578—88.
9.Sleet D,Moffett D,Stevens J.CDC’s research portfolio in older adult fall prevention:a review of progress,1985—2005,and future research directions.J Safety Res2008;39:259—67.
10.TinettiM,Brach J.Translating the fall prevention recommendations into a covered service:can it be done,and who should do it?Ann Intern Med2012;157:213—4.
11.National Center for Complementary and A lternative Medicine.Tai Chi: anintroduction. Available at: http://nccam.nih.gov/health/taichi/ introduction.htm[accessed 15.09.2013].
12.Wolf S,Kutner N,Green R,M cNeely E.The Atlanta FICSIT study:two exercise interventions to reduce frailty in elders.J Am Geriatr Soc1993;41:329—32.
13.Wolf SL,Barnhart HX,Kutner NG,M cNeely E,Coogler C,Xu T. Reducing frailty and falls in olderpersons:an investigation of Tai Chi and computerized balance training.Atlanta FICSIT Group.Frailty and injuries:cooperative studies of intervention techniques.J Am Geriatr Soc1996;44:489—97.
14.Wolf S,BarnhartH,Ellison G,Coogler C.The effectof TaiChi Quan and computerized balance training on postural stability in older subjects. Atlanta FICSIT Group.Frailty and injuries:cooperative studies of intervention techniques.Phys Ther1997;77:371—81.
15.Gillespie LD,Robertson MC,Gillespie WJ,Sherrington C,Gates S, Clemson LM,et al.Interventions for preventing falls in older people living in the community.Cochrane Database Syst Rev2012;9:CD007146. http://dx.doi.org/10.1002/14651858.CD007146.pub3.
16.Kozaki K.Fall risk and fracture.Aging and fall/fracture.Clin Calcium2013;23:653—60[in Japanese].
17.Schleicher M,Wedam L,Wu G.Review of TaiChias an effective exercise on falls prevention in elderly.Res Sports Med2012;20:37—58.
18.Gaught A,Carneiro K.Evidence for determining the exercise prescription in patients with osteoarthritis.Phys Sportsmed2013;41:58—65.
19.Hantikainen V,Betschon E.Tai Chi in rheumatoid arthritis.Pflege Z2012;65:486—7[in German].
20.Uhlig T.Tai Chi and yoga as complementary therapies in rheumatologic conditions.Best Pract Res Clin Rheumatol2012;26:387—98.
21.Wang C.Role of Tai Chi in treatment of rheumatologic diseases.Curr Rheumatol Rep2012;14:598—603.
22.Macfarlane GJ,Paudyal P,Doherty M,Ernst E,Lewith G,MacPherson H, etal.A systematic review of evidence for the effectiveness of practitionerbased complementary and alternative therapies in the management of rheumatic diseases: rheumatoid arthritis.Rheumatology(Oxford)2012;51:1707—13.
23.Macfarlane GJ,Paudyal P,Doherty M,ErnstE,Lewith G,MacPherson H, etal.American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand,hip,and knee.Arthritis Care Res2012;64:465—74.
24.Alvarez V,Rossetti AO,M ichel P,Kuntzer T,Nater B,De´monet JF,etal. 2012:news in neurology.Rev Med Suisse2013;9:62—5[in French].
25.Lee M,Lam P,ErnstE.Effectiveness of TaiChi for Parkinson’s disease:a critical review.Parkinsonism Relat Disord2008;14:589—94.
26.Grazina R,Massano J.Physical exercise and Parkinson’s disease:influence on symptoms,disease course and prevention.Rev Neurosci2013;24:139—52.
27.Langhorst J,Ha¨user W,Bernardy K,Lucius H,Settan M,Winkelmann A, etal.Complementary and alternative therapies for fibromyalgia syndrome. Systematic review,meta-analysis and guideline.Schmerz2012;26:311—7 [in German].
28.Langhorst J,K lose P,Dobos GJ,Bernardy K,Ha¨user W.Efficacy and safety of meditative movement therapies in fibromyalgia syndrome:a systematic review and meta-analysis of randomized controlled trials.Rheumatol Int2013;33:193—207.
29.Blake H,Haw ley H.Effects of Tai Chi exercise on physical and psychological health of older people.Curr Aging Sci2012;5:19—27.
30.Jimenez P,Melendez A,Albers U.Psychological effects of TaiChiChuan.Arch Gerontol Geriatr2012;55:460—7.
31.Wang F,Lee EK,Wu T,Benson H,Fricchione G,Wang W,et al.The effects of Tai Chion depression,anxiety,and psychological well-being:a systematic review and meta-analysis.Int J Behav Med2013 Sept.28. http://dx.doi.org/10.1007/s12529-013-9351-9[Epub ahead of print].
32.Woltz P,Chapa D,Friedmann E,Son H,Akintade B,Thomas SA.Effects of interventions on depression in heart failure:a systematic review.Heart Lung2012;41:469—83.
33.Lin C,Lin C,Lien S.The effectof taichi for blood pressure,blood sugar, blood lipid control for patients with chronic diseases:a systematic review.Hu Li Za Zhi2013;60:69—77[in Chinese].
34.Ng SM,Wang CW,Ho RT,Ziea TC,He J,Wong VC,et al.Tai chi exercise for patients with heart disease:a systematic review of controlled clinical trails.Altern Ther Health Med2012;18:16—22.
35.Pan L,Yan J,Guo Y,Yan J.Effects of Tai Chi on exercise capacity and quality of life in patients with chronic heart failure:a meta-analysis.Eur J Heart Fail2013;15:316—23.
36.Wang J,Feng B,Yang X,Liu W,Teng F,Li S,etal.Tai Chi for essential hypertension.Evid Based Complement Alternat Med2013;2013:215254. http://dx.doi.org/10.1155/2013/215254.
37.Li L,Hondzinski J.Select exercise modalities may reverse movement dysfunction because of peripheral neuropathy.Exerc Sport Sci Rev2012;40:133—7.
38.Peng P.Taichi and chronic pain.Reg Anesth Pain Med2012;37:372—82.
39.Li F,Fisher JK,Harmer P,Shirai M.A simpler 8-form easy Tai Chi for elderly persons.J Aging Phys Act2003;11:217—29.
40.Li F,Harmer P,McAuley E,Duncan TE,Duncan SC,Chaumeton N,etal. An evaluation of the effects of Tai Chi exercise on physical function among older persons:a randomized controlled trial.Ann Behav Med2001;23:139—46.
41.Li F,Fisher KJ,Harmer P,Irbe D,Tearse RG,Weimer C.Tai Chiand self rated quality of sleep and daytime sleepiness in older adults:a randomized controlled trial.J Am Geriatr Soc2004;52:892—900.
42.Li F,Harmer P,Fisher KJ,M cAuley E,Chaumeton N,Eckstrom E,etal. Tai Chiand fall reductions in olderadults:a random ized controlled trial.J Gerontol Med Sci2005;60A:187—94.
43.LiF,Harmer P,Fitzgerald K,Eckstrom E,Stock R,Galver J,etal.TaiChi and postural stability in patients with Parkinson’s disease.N Engl J Med2012;366:511—9.
44.Li F,Harmer P,Mack KA,Sleet D,Fisher KJ,Kohn MA,et al.Tai Chi: moving for better balance—development of a community based falls prevention program.J Phys Act Health2008;5:445—55.
45.Li F,Harmer P,Glasgow R,Mack KA,Sleet D,Fisher KJ,et al.Translation of an effective Tai Chi intervention into a community-based falls prevention program.Am J Public Health2008;98:1195—8.
46.Jahnke R,Larkey L,Rogers C.Dissem ination and benefits of a replicable Tai Chi and Qigong program for older adults.GeriatrNurs2010;31:272—80.
47.Ling KW,Wong FS,Chan WK,Chan SY,Chan EP,Cheng YL,et al. Effect of a home exercise program based on tai chi in patients with endstage renal disease.Perit Dial Int2003;23:S99—103.
48.Voukelatos A,Cumming R,Lord S,Rissel C.A randomized,controlled trial of taichi for the prevention of falls:the Central Sydney Tai Chi Trial.J Am Geriatr Soc2007;55:1185—91.
49.Church J,Goodall S,Norman R,Haas M.The cost-effectiveness of falls prevention for older community-dwelling Australians.Aust N Z J Public Health2012;36:241—8.
50.Church J,Goodall S,Norman R,Haas M.An economic evaluation of community and residential aged care falls prevention strategies in NSW.N S W Public Health Bull2011;22:60—8.
51.Frick K,Kung J,Parrish J,Narrett M.Evaluating the cost-effectiveness of fall prevention programs that reduce fall-related hip fractures in older adults.J Am Geriatr Soc2010;58:136—41.
52.Stevens J.A CDC compendium of effective fall interventions:whatworks for community-dwelling older adults.2nd ed.Atlanta,GA:Centers for Disease Controland Prevention,National Center for Injury Prevention and Control;2010.
53.Koh H,Sebelius K.Promoting prevention through the Affordable Care Act.N Engl J Med2010;363:1296—9.
54.Moura VL,Faurot KR,Gaylord SA,Mann JD,Sill M,Lynch C,et al. M ind-body interventions for treatment of phantom limb pain in persons with amputations.Am J Phys Med Rehabil2012;91:701—14.
55.BøK,Herbert R.There is not yet strong evidence that exercise regimens other than pelvic floor muscle training can reduce stress urinary incontinence in women:a systematic review.J Physiother2013;59:159—68.
Received 15 October 2013;revised 21 October 2013;accepted 22 October 2013
E-mail address:pharmer@willamette.edu.
Peer review under responsibility of Shanghai University of Sport.
2095-2546/$-see front matter CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.A ll rights reserved. http://dx.doi.org/10.1016/j.jshs.2013.10.005
CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved.
 Journal of Sport and Health Science2014年1期
Journal of Sport and Health Science2014年1期
- Journal of Sport and Health Science的其它文章
- Tai Ji Quan:An overview of its history,health benefits,and cultural value
- Effects of latissimus dorsi length on shoulder flexion in canoeists, sw immers,rugby players,and controls
- Implementing an evidence-based Tai Ji Quan program in a multicultural setting:A pilot dissemination project
- Tai Ji Quan,the brain,and cognition in older adults
- Tai Ji Quan as an exercise modality to prevent and manage cardiovascular disease:A review