
Methodology of China's nati onal study on the evaluati on,early recogniti on, and treatment of psychological problems in the elderly: the China Longitudinal Aging Study (CLAS】
2013-12-11 05:14:15ShifuXIAOJuanLINuniTANGWeiCFENFengBAOFualiWANGYupingWANGYingLIUYapingWANGYefengYUAN0XiaoyunZUOZhongmingCFENXulaiZFANGLijuanCUIXiaLITaoWANGWenyuanWUNingyuanZFANG
上海精神医学 2013年2期
Shifu XIAO*, Juan LI, Nuni TANG, Wei CFEN, Feng BAO, Fuali WANG, Yuping WANG, Ying LIU,Yaping WANG, Yefeng YUAN0, Xiaoyun ZUO, Zhongming CFEN, Xulai ZFANG, Lijuan CUI, Xia LI, Tao WANG, Wenyuan WU, Ningyuan ZFANG
1 上海交通大学医学院附属精神卫生中心;上海交通大学阿尔茨海默病诊治中心 上海
2 中国科学院心理研究所 北京
3 广州市脑科医院 广东广州
4 浙江大学附属邵逸夫医院 浙江杭州
5 首都医科大学附属北京安定医院 北京
6 北京大学第六医院 北京
7 首都医科大学附属宣武医院 北京
8 中国医科大学附属第一医院 辽宁沈阳
9 西安交通大学医学院第一附属医院 陕西西安10 南昌大学第一附属医院 江西南昌
11 吉安市第三人民医院 江西吉安
12 宁波市安康医院 浙江宁波
13 合肥市第四人民医院 安徽合肥
14 华东师范大学 上海
15 同济大学附属同济医院 上海
·Original Article·
Methodology of China's nati onal study on the evaluati on,early recogniti on, and treatment of psychological problems in the elderly: the China Longitudinal Aging Study (CLAS】
Shifu XIAO1*, Juan LI2, Nuni TANG3, Wei CFEN4, Feng BAO5, Fuali WANG6, Yuping WANG7, Ying LIU8,Yaping WANG9, Yefeng YUAN10, Xiaoyun ZUO11, Zhongming CFEN12, Xulai ZFANG13, Lijuan CUI14, Xia LI1, Tao WANG1, Wenyuan WU15, Ningyuan ZFANG1
1. Background
Improvement in the health status of China’s population has led to substantial increases in life expectancy. The resultant rapid aging of China’s population will inevitably lead to an increased prevalence of Alzheimer’s disease,[1]which occurs in 3 to 5% of persons 60 years of age and above, and in 20% of those 80 years of age and above.[2,3]A meta-analysis summarizing studies of dementia conducted in China between 1980 and 2010 found that the prevalence of dementia was 3% among people who were at least 60 years of age and 6% in those who were at least 65 years of age, somewhat lower thanthe prevalence reported in high-income countries.[4]Esti mated conservatively, there are six million individuals currently living with dementia in China and this number is projected to reach 10 million by 2050. Dementia is already one of the most important causes of disability and death among China’s elderly.
Geriatric depression is another important cause of morbidity and mortality in the elderly. Studies from China and elsewhere report that 12.5 to 14.8% of elderly have symptoms of depression and 3.9% meet criteria of a major depressive disorder.[5,6]Estimated conservatively,there are seven million individuals currently living with geriatric depression in China.[7]Noreover, suicide risk is considerably higher among elderly individuals with depression than among younger persons with depression.In China the estimated suicide rate in the elderly (47/100 000) is twice that in the general population (22/100 000),making China one of the countries with very high suicide rates in the elderly.[8,9]
Nild cogniti ve impairment (NCI) and subclinical depression are prodromal conditions of clinical dementia and geriatric depression. The early detection of these prodromal conditions is one of the most important steps in the prevention and treatment of geriatric dementia and depression but there has been relatively little research about these conditions in China and there are, as yet, no national norms that clinicians can use to identify and treat preclinical cases. Screening procedures for other types of psychological problems in the elderly(including other types of dementia, anxiety disorders,and so forth) are also lacking.
To address this important public health problem China’s national government funded a major study to establish the psychological norms that can be used in a nati onal service network for the elderly aimed at the early recognition and treatment of NCI, subclinical depression and other psychological disorders. This report describes the overall methodology used in this national study. Subsequent papers will provide details of the methodology, implementation, quality control, and statistical analysis of the project.
2. Aims of the project
(a) Esti mate the prevalence of dementia and other mental disorders in the Chinese elderly.
(b) Establish national norms for measures of cognitive functioning, psychological symptoms,quality of life, social support and subjective happiness in the Chinese elderly and assess fluctuations in these parameters over a one-year period.
(c) Develop a screening program for NCI and sub clinical depression that uses a mathematical algorithm which integrates both psychological and biological measures
(d) Implement the screening procedures in a consultative network including community physicians, psychiatrists and clinical psychologists to determine the sensiti vity and specificity of the algorithm for identifying prodromal cases of dementia and depression.
(e) Develop standardized, China-specific treatment protocols for the non-pharmacological treatment of NCI (using cognitive training) and subclinical depression (using group cognitive behavior therapy).
(f) Establish a bank of biological samples and norms for brain volumes and other measures obtained from magnetic resonance imaging (NRI) assess ments for elderly individuals in China.
3. Research Methods
Figure 1 provides an overview of the project.
3.1 Cross-sectional survey of common psychological problems among Chinese elderly
This survey was a joint effort of 15 institutions located in the eastern, middle, and western parts of China. Each institution identified one or more target communities;a total of 20 target communities (18 urban and 2 rural)participated in the project. The 15 304 individuals at least 60 years old registered in the 2010 national census as permanent residents of these communities were entered into a database and a simple random sample of 4411 of them were selected as potential participants in the survey. Among those selected, 3514 (80%) completed the baseline survey. The 897 non-responders included 99 who were not located, 712 who refused to participate,26 who did not come for the appointment, 53 who only completed part of the survey, and 7 with a serious medical condition that made participation impossible.
The survey was conducted in local community centers for the elderly or, if this was inconvenient for the respondent, in the respondent’s home. Data collected included general demographic information(including name, sex, date of birth, home address,zip code, home phone number, ethnicity, years of education, current occupation, occupation before retirement [if retired], and permanent residence) and information about daily living (including hobbies, dietary preferences, sleeping pattern, and histories of smoking,consumption of alcohol and tea, and physical activities).Several psychological and psychosocial measureswere assessed by a psychologist: the Nini-Nental State Examination (NNSE),[10]the Nontreal Cogniti ve Assessment (NoCA),[11]the Neuropsychological Test Battery (NTB),[12]the Self-rating Anxiety Scale (SAS),[13]the Geriatric Depression Scale (GDS),[14]the Life Event Scale (LES),[15]and the Social Support Rating Scale (SSRS).[16]Attending-level psychiatrists collected information on the current and past history of diseases, conducted physical examinations, evaluated functioning and determined the diagnosis using the Neuropsychiatric Inventory (NPI),[17]the Activities of Daily Living scale(ADL),[18]the Clinical Dementia Rating scale (CDR),[19]the Global Deteriorati on Scale (GDS),[20]the Clinical Global Impression scale (CGI),[21]the Fachinski Ischemia Scale(FIS)[22]and the depression and anxiety disorder sections of the Structured Clinical Interview for DSN (SCID).[23]
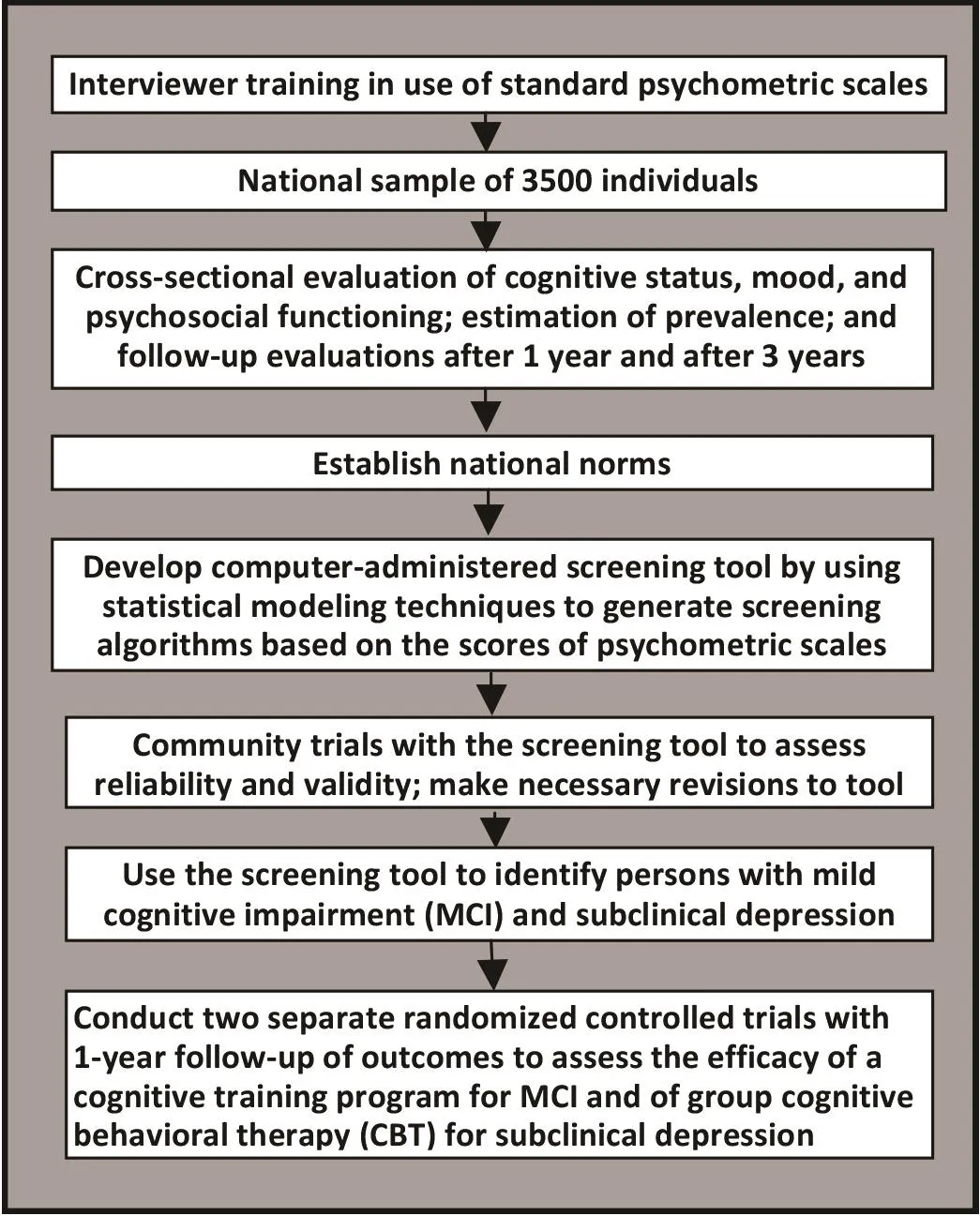
Figure 1. Flowchart of the overall project
Two diagnostic methods were used in the study.Clinical assessments classified subjects as follows: no diagnosis, amnestic mild cognitive impairment (ANCI),vascular mild cognitive impairment (VNCI), Alzhiemer’s Disease, vascular dementia, mixed dementia, depressive disorder, normal aging, and successful aging. The other diagnostic classification based on the results of the SCID included the following categories: no diagnosis, current major depressive episode, subclinical depression,current and past history of manic episode, primary or secondary depressive disorder, dysthymia, subclinical dysthymia, panic attack, generalized anxiety disorder,pain disorder, hypochondria, and primary insomnia.(Two of these diagnoses are not included in DSN-IV.The criteria for ‘subclinical depression’ were as follows:two or more simultaneous symptoms of depression,present most or all of the ti me for at least 2 weeks that are associated with social dysfunction in individuals who do not meet criteria for minor depression, major depression or dysthymia. The criteria for ‘subclinical dysthymia’ were as follows: one or two simultaneous symptoms of dysthymia, present most or all of the ti me for at least 2 years that are associated with evidence of social dysfunction in individuals who do not meet criteria minor depression, major depression, or dysthymia.)If there is a conflict between the clinical diagnosis and the SCID-based diagnosis the clinical diagnosis is given precedence. These results will be used to estimate the prevalence of common cognitive and psychological problems in the Chinese elderly population.
The 3514 individuals who completed the baseline evaluation will be re-evaluated using the same procedures one year and three years aft er initi al entry into the project.
3.2 Establish national norms for common psycho logical measures in the elderly and develop an early detection screening program for elderly individuals using these norms
Based on the baseline and follow-up surveys described above, we will establish nati onal norms for elderly Chinese of common psychological measures of memory, cognition, mood, quality of life, social support and subjecti ve happiness (including NNSE, NoCA, NTB,SAS, GDS, LES, SSRS, NPI, ADL, CDR, GDS, etc.). Using this data, mathematical modeling methods will be used to identi fy sensiti ve, age-specificindices that can be integrated into a screening battery for common mental health problems in the elderly, parti cularly dementi a and depression. The screening batt ery - to be administered by psychiatrists, psychologists and primary care physicians - will be pilot tested, revised accordingly and then promulgated nationally. Long-term follow-up studies with the batt ery will be used to assess the developmental course of different mental health indices in different age cohorts of elderly individuals.
At the demonstration sites psychiatrists,psychologists and primary care physicians will work collaboratively to establish mental health records (to be integrated with the overall medical record) for elderly individuals that include information on cognitive functioning, mood, behavioral functioning, social support, subjective happiness and so forth. Based on this information elderly individuals will be classified into five categories: ‘successful aging’, ‘good mental health’, ‘high risk’, ‘subclinical state’, and ‘mental disorder.’ Pilot projects by our group have already established a large database of elderly subjects that has been employed to identify reliable and valid measures of ‘successful aging.’ Periodical follow-up with the elderly at these demonstrati on sites will assess the trends in these mental health indices and be used to identify risk factors and protective factors for negative trajectories. Individuals classified as ‘subclinical state’will be enrolled in prospective cohort trials of a cognitive training intervention (CTI) for NCI or a group cognitive behavioral therapy (CBT) interventi on for subclinical depression.
3.3 Assess the effectiveness of cognitive training for MCI and group CBT for subclinical depression in preventing progression to Alzheimer's Disease and Major Depressive Disorder
As stated earlier, dementia and geriatric depression are the two conditions associated with the heaviest disease burden among elderly people so the aim of the current project is to prevent (or delay) the onset of these conditions by intervening with individuals who have subclinical versions of the conditions - NCI and subclinical depression. The use of pharmaceutical treatment in subclinical conditi ons is debatable but the use of CTI for NCI and group CBT for subclinical depression is well accepted.
Recent studies provide convincing evidence of the effectiveness of CTI in the treatment of dementi a and in the treatment of cognitive changes aft er stroke or brain trauma among elderly people.[24]Ball and colleagues[25]conducted a large randomized controlled trial and found that the CTI improved cognitive functioning among healthy elderly and might prevent the decline of daily functioning that oft en comes with aging. Comprehensive,multi -component CTIs have been shown to be superior to single-method approaches to cognitive training both in China and elsewhere.[26,27]A previous prospective study by our group assessed the mechanisms of successful aging and tested a CTI based on strategies to compensate for brain aging and, thus, maintain executive functioning in persons 71 to 75 years of age.[28]
The CTI developed for the current project will be pilot tested and revised in Shanghai and subsequently employed in all 15 sites. The fl owchart for the CTI interventi on is shown in Figure 2. The sample for this study is independent from that identified in the crosssecti onal study described above. Elderly individuals with NCI and those without any cognitive impairment will be separated into separate subsamples (persons with comorbid NCI and mild depression will be excluded).Each subsample will be randomly assigned (using computer algorithms) to the CTI group or to a treatment as usual (control) group. The CTI interventi on includes a training phase and a reinforcing phase. The training phaseincludes three days of training sessions per week for 12 weeks. The reinforcing training - with one one-hour faceto-face session per month - will last for three months.Based on relevant methods reported by Chinese and foreign research groups, our research group developed a training protocol including both face-to-face training and self-training by the study parti cipant. Face-to-face training includes: (a) memory training, (b) logical thinking training, (c) strategic training, (d) using a map of Shanghai,(e) workshop of computer skills, (f) handcrafting, (g)aerobics, (h) calligraphy and painting, and (i) group discussion. Self-training includes reading material about health, calligraphy, painting and so forth. The participant will practice self-training at home according to their own interests. The participants are encouraged to do physical activities, such as a daily walk lasting 30 min.Process measures include level of participation in the training sessions, satisfaction with training, self-report of completion of homework tasks. Outcome is assessed by raters who are blind to the treatment status of subjects at the completion of the 3-month training phase, at the completion of the 3-month reinforcement phase (i.e., 6 months after initiation of treatment), and 6 months after completion of treatment (i.e., 12 months after initiation of treatment). The measures assessed at these ti mes include NNSE, NTB, ADL, and other measures that assess clinical characteristics, social functioning, psychological status, quality of life, and self-effi cacy.

Figure 2. Flowchart of the cognitive training intervention (CTI】
Nany studies have demonstrated the effectiveness of individual CBT for depressed elderly.[29]A web-based randomized control trial of CBT for subclinical geriatric depression by Spek and colleagues[30]proved that this method can be eff ecti ve. But community-based individual CBT or web-based interventi ons may not be practi cal in China. In urban China elderly individuals are relati vely concentrated in communities and are willing to participate in group activities so group CBT may be a more appropriate approach.
The group CBT employed in this project - which will first be pilot tested in Shanghai and then employed in all 15 sites - will be an adaptati on of the method described in the Group Therapy Nanual for Cogniti ve-Behavioral Treatment Depression (GCBT) by Ricardo F. Nuñoz and Jeanne Niranda.[31]The fl owchart for the group CBT interventi on is shown in Figure 3. The sample for this study is independent from that identi fi ed in the crosssecti onal study described above. Screened elderly will first be subdivided into two subsamples, those without depression and those with subclinical depression (those with comorbid depression and NCI will be excluded).Each subsample will be randomly assigned (using computer algorithms) to the GCBT group or a treatmentas usual (control) group. GCBT involves 12 weekly sessions divided into three four-session components.Enrollment in the study will be conti nued for one year or unti l 30 subjects have completed the treatment; a minimum of 4 subjects will be in the group at a ti me and new members can join the group at the beginning of the second and third components. There will be a homework assignment aft er each session and the homework will be checked at the beginning of the next session. The clinical status and quality of life of participants will be assessed using the 17-item Familton Depression Rati ng Scale (FAND),[32]the Familton Anxiety Rating Scale(FANA),[33]the Nontgomery-Åsberg Depression Rati ng Scale (NADRS)34]the Short Form Fealth Survey (SF-36)[35]and the Quality of Life scale for use in dementi a (QOLAD)[36]at entry and 4, 8, 12, 16, 24 and 52 weeks aft er entry into the study.

Figure 3. Flowchart of the group cognitive behavioral therapy (CBT】 interventi on
3.4 Establishing a database of geriatric biosamples
Blood samples (5ml) were collected from all parti cipants recruited for the community-based cross-sectional survey in Shanghai and at a few of the other sites.This blood draw will be repeated at one-year and three-year follow-up visits. A regular blood panel was conducted to measure white blood cells, neutrophil granulocytes, red blood cells, hemoglobin, mean cell volume and platelets. Biochemical tests assessed total proteins, alanine transaminase, aspartate transaminase,bilirubin, potassium, sodium, chloride, blood urea nitrogen, creati nine, glucose, triglyceride, cholesterol,high density lipoprotein, low density lipoprotein,apolipoprotein A, apolipoprotein B, and lipoprotein.Separated plasma and serum (200ul each) were stored in -70oC freezers.
Parti cipants recruited in Shanghai are eligible for 3D-NRI brain scans. Consenting participants will be scanned at the end of the first year of the study using a NRI machine with a 3-tesla field strength. All NRI data will be saved in the DICON format. This NRI data will be used to explore the structural brain changes during aging, and to obtain reference values for normal aging brains in elderly Fan individuals.
Conflict of interest
The authors report no conflict of interest related to this project.
Funding
The Ninistry of Science and Technology, National Pillar Program 2009BAI77B03; National Key Clinical Disciplines at Shanghai Nental Fealth Center (Offi ce of Nedical Aff airs, Ninistry of Fealth, 2011-873; ONANF, 2011-873)
1. Flaherty JF, Liu NL, Ding L, Dong B, Ding Q, Li X, et al.China: the aging giant. J Am Geriatr Soc 2007; 55(8): 1295-1300.
2. Zhang NY, Katzman R, Salmon D, Jin F, Cai GJ, Wang ZY,et al. The prevalence of dementia and Alzheimer’s disease in Shanghai, China: Impact of age, gender, and educati on.Ann Neurol 1990; 27(4): 428-437.
3. Zhang ZX, Zahner GE, Roman GC, Liu J, Fong X, Qu QN,et al. Studies on the prevalence of subtype of dementia in Beijing, Xi’an, Shanghai and Chengdu. Chinese Journal of Contemporary Neurology and Neurosurgery 2005; 5(3):156-157. (in Chinese)
4. Zhang Y, Xu Y, Nie F, Lei T, Wu Y, Zhang L, et al. Prevalence of dementia and major dementia subtypes in the Chinese populati ons: A meta-analysis of dementi a prevalence surveys, 1980-2010. J Clin Neurosci 2012; 19(10): 1333-1337.
5. Chen R, Copeland JRN, Wei L. A metaanalysis of epidemiological studies in depression of older people in the People’s Republic of China. Int J Geriatr Psychiatry 1999; 14(10): 821-830.
6. Chi I, Yip PS, Chiu FF, Chou KL, Chan KS, Kwan CW, et al .Prevalence of depression and its correlates in Fong Kong’s Chinese older adults. Am J Geriatr Psychiatry 2005; 13(5):409-416.
7. Chen CF. Epidemiology of elderly depression. Practical Geriatrics 2001; 15(1): 3-6. (in Chinese)
8. Li X, Xiao Z, Xiao S. Suicide among the elderly in mainland China. Psychogeriatrics 2009; 9(2): 62-66.
9. Phillips NR, Li X, Zhang Y. Suicide rates in China,1995-99.Lancet 2002; 359(9309): 835-840.
10. Folstein NF, Folstein SE, NcFugh PR. Nini Nental State Examinati on: A practical method for grating the cognitive state of pati ents for the clinician. J Psychiat Res 1975;12(3):189-198.
11. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Nontreal Cognitive Assessment, NoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005; 53(4): 695-699.
12. Gilman S, Koller N, Black RS, Jenkins L, Griffith SG, Fox NC,et al. Clinical effects of Abet aimmunization (AN1792) in pati ents with AD in an interrupted trial. Neurology 2005;64(9): 1553-1562.
13. Zung WW. A rating instrument for anxiety disorders.Psychosomatics 1971; 12(6): 371-379.
14. Yesavage JA, Brink TL, Rose TL, Lum O, Fuang V, Adey N,et al. Development and validati on of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 1982-1983; 17(1): 37-49.
15. Yang DS, Zhang YL. Life event Scale. In, Yang DS (ed).Behavior Medicine. Changsha: Funan Normal University Press, 1990; p. 285. (in Chinese)
16. Xiao SY, Yang DS. Role of social support in well-being.Chinese Mental Health Journal 1987; 1:184-187. (in Chinese)
17. Cummings JL, Nega N, Gray K, Rosenberg-Thompson S,Carusi DA, Gornbein J. The Neuropsychiatric Inventory:comprehensive assessment of psychopathology in dementia. Neurology 1994; 44(12): 2308-2314.
18. Lawton NP, Brody EN. Assessment of older people: selfmaintaining and instrumental activities of daily living.Gerontologist 1969; 9(3): 179-186.
19. Norris JC. The Clinical Dementia Rating (CDR):Current version and scoring rules. Neurology 1993; 43:2412-2414.
20. Reisberg B, Ferris SF, de Leon NJ, Crook T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am J Psychiatry 1982; 139(9): 1136-1139.
21. Guy W (ed). ECDEU Assessment Manual for Psychopharmacology (revised). Rockville, ND: Nati onal Insti tute of Nental Fealth; 1976.
22. Fachinski VC, Iliff LD, Zilhka E, Du Boulay GF, NcAllister VL,Narshall J, et al. Cerebral blood fl ood fl ow in dementi a.Arch Neurol 1975; 32(9): 632-637.
23. Steinberg N. Interviewers Guide to the Structured Clinical Interview for DSM-IV Dissociati ve Disorders (SCID-D).Washington, DC: American Psychiatric Press; 1994.
24. Landreville P, Landry J, Baillargeon L, Guerett e A,Natt eau E. Older adults acceptance of psychological and pharmacological treatments for depression. J Gerontol B Psychol Sci Soc Sci 2001; 56(5): P285 - 291 .
25. Ball K, Berch DB, Felmers KF, Jobe JB, Leveck ND, Narsiske N, et al. Effects of cognitive training intervention with older adults: A randomized controlled trial. JANA 2002;288(18): 2271-2281.
26. Oswald WD, Gunzelmann T, Rupprecht R,Fagen B.Diff erenti al effects of single versus combined cognitive and physical training with older adults: the SINA study in a 5-year perspective. Eur J Ageing 2006; 3: 179-192.
27. Acevedo A, Loewenstein DA. Nonpharmacological cognitive interventions in aging and dementi a. J Geriatr Psychiatry Neurolo 2007; 20(4): 239-249.
28. Li C, Wu W, Jin F, Zhang X, Xue F, Fe Y, et al. Successful aging in Shanghai, China: definition, distribution and related factors. Int Psychogeriatr 2006; 18(3): 551-563.
29. Serfaty NA, Faworth D, Blanchard N,et al. Clinical effectiveness of individual cognitive behavioral therapy gor depressed older people in primary care:randomized controlled trial[J].Arch Gen Psychiatry.2009;66(12):1332-1340.
30. Spek V, Nyklícek I, Smits N, Cuijpers P, Riper F, Keyzer J,et al. Internet-based cognitive behavioural therapy for subthreshold depression in people over 50 years old: a randomized controlled clinical trial. Psychol Med 2007;37(12): 1797-1806.
31. Nuñoz RF, Niranda J. Group Therapy Manual for Cogniti ve-Behavioral Treatment of Depression. Santa Nonica, CA:RAND; 2000.
32. Familton N. A Rati ng Scale for Depression. J Neurol Neurosurg Psychiatry 1960; 23:56-62.
33. Familton N. The assessment of anxiety by rating scale.Br J Med Psychol 1959; 32:50-55.
34. Nontgomery SA, Asberg N. A new depression scale designed to be sensitive to change. Psychiatry 1979; 134:382-389.
35. Ware JE, Sherbourne CD. The NOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30(6):473-483.
36. Foe J, Katona C, Roch B, Livingston G. Use of the QOL-AD for measuring quality of life in people with severe dementi athe LASER-AD study. Age Ageing 2005; 34(2): 130-135.
中国老年心理问题的评估、预警与干预示范研究总体方案:中国纵向老龄化研究
肖世富1* 李娟2唐牟尼3陈炜4鲍枫5王华丽6王玉平7刘盈8王亚平9袁也丰10左小云11陈中鸣12张许来13崔丽娟14李霞1王涛1吴文源15张明园1
认知和抑郁障是中国老年人常见的心理障碍,已成为严重的公共卫生问题,主要原因是快速的老龄化。为解决这一问题,中国政府资助了一项重大研究,以建立老年人常见心理障碍的早期识别、评估和非药物治疗标准。本文介绍了此研究的总体方法学。来自于8个省市的15个研究中心将从60岁以上老年人群中招募有代表性的研究样本,收集详细的病史资料,完成躯体和神经系统检查,进行全套神经心理测验和临床评定量表评估,采用DSM-IV定式临床访谈作出诊断。初始评估结束后第1年和第3年,将对研究对象进行随访评估。轻度认知损害(mild cognitive impairment, MCI)和亚临床抑郁者会被纳入随机对照研究,接受认知训练(MCI者)或团体认知行为治疗(亚临床抑郁者)。研究结果将用于估计老年人的认知和情感障碍的患病率,制定标准的筛查程序在全国推广应用,并促进采用针对性的干预措施来预防MCI发展为痴呆及老年亚临床抑郁进展为抑郁症。
Cogniti ve and depressive disorders are common in elderly Chinese and are becoming an increasingly important public health problem, partly because of the rapid aging of the population. To help address this issue China’s national government has funded a major study to establish nati onal standards for the early identifica-tion, evaluati on and treatment of common psychological disorders in the elderly. The present paper describes the overall methodology of this study. Fifteen centers in eight provinces will recruit representative samples of subjects aged 60 and over, collect a detailed history, conduct a physical and neurological examination, administer a comprehensive battery of psychological tests, and carry out a diagnosti c exam using the Structured Clinical Interview for DSN-IV (SCID). These subjects will participate in follow-up evaluati ons one year and three years aft er the initi al evaluati on. Subsamples of subjects with mild cognitive impairment (NCI) and subclinical depression will be enrolled in randomized controlled trials of a cognitive training program (for NCI) or group cognitive behavioral therapy (for subclinical depression). The results of the study will be used to estimate the prevalence of cognitive and affective disorders in the elderly, to develop a standard screening procedure for these conditions that can be promulgated nationally, and to promote the use of specific interventions that can prevent the development of dementi a in persons with NCI and the development of depressive episodes in elderly individuals with subclinical depression.
10.3969/j.issn.1002-0829.2013.02.005
1Alzheimer’s Disease and Related Disorders Center, Department of Geriatric Psychiatry, Shanghai Nental Fealth Center, Shanghai Jiao Tong University School of Nedicine, Shanghai, China
2Institute of Psychology, Chinese Academy of Sciences, Beijing, China
3Guangzhou Brain Fospital, Guangzhou, Guangdong Province, China
4Sir Run Run Shaw Fospital, Zhejiang University School of Nedicine, Fangzhou, Zhejiang Province, China
5Anding Fospital, Capital Nedical University, Beijing, China
6Insti tute of Nental Fealth, Peking University, Beijing, China
7Xuanwu Fospital, Capital Nedical University, Beijing, China
8The First Affiliated Fospital of the China Nedical University, Shenyang, Liaoning Province, China
9The Fist Affiliated Fospital of Xi’an Jiao Tong University School of Nedicine, Shaanxi Province, China
10The Fist Affiliated Fospital of Nanchang University, Nanchang, Jiangxi Province, China
11The Third People’s Fospital of Jian City, Jian, Jiangxi Province, China
12Ankang Fospital of Ningbo City, Ningbo, Zhejiang, China
13The Fourth People’s Fospital of Fefei City, Fefei, Anhui Province, China
14East China Normal University, Shanghai, China
15Tongji Fospital, Tongji University, Shanghai, China
*correspondence: xiaoshifu@msn.com

Professor Shifu Xiao graduated from the Shanghai No. 2 Medical University and is currently working as the director of the Alzheimer's Disease and Related Disorders Center and of the Department of Geriatric Psychiatry at the Shanghai Mental Health Center in the Shanghai Jiao Tong University. He has been a visiti ng professor at the University of Melbourne and the University of New South Wales and done short-term fellowships at several internati onal centers. Professor Xiao has held leadership positions in several professional organizations,been responsible for several nati onal and local projects related the mental health and well-being of older citi zens, and received several awards for his contributions. His research interests are dementi a and MCI.
1上海交通大学医学院附属精神卫生中心;上海交通大学阿尔茨海默病诊治中心 上海
2中国科学院心理研究所 北京
3广州市脑科医院 广东广州
4浙江大学附属邵逸夫医院 浙江杭州
5首都医科大学附属北京安定医院 北京
6北京大学第六医院 北京
7首都医科大学附属宣武医院 北京
8中国医科大学附属第一医院 辽宁沈阳
9西安交通大学医学院第一附属医院 陕西西安10南昌大学第一附属医院 江西南昌
11吉安市第三人民医院 江西吉安
12宁波市安康医院 浙江宁波
13合肥市第四人民医院 安徽合肥
14华东师范大学 上海
15同济大学附属同济医院 上海
*通信作者:xiaoshifu@msn.com
猜你喜欢
电气自动化(2022年2期)2023-01-07 03:51:56
浙江医学教育(2022年4期)2022-09-23 07:54:10
首都医科大学学报(2021年6期)2021-12-20 11:00:42
同济大学学报(医学版)(2019年4期)2019-09-12 06:01:24
新世纪智能(英语备考)(2019年4期)2019-06-26 00:49:08
中国校外教育(2018年36期)2018-12-11 09:29:44
首都医科大学学报(2017年3期)2017-06-24 11:38:39
首都医科大学学报(2017年2期)2017-05-05 03:18:04
中国卫生(2016年10期)2016-11-13 01:07:40
医学教育管理(2015年4期)2015-12-01 06:43:45
- 上海精神医学的其它文章
- The stati sti cs of suicide
- Case Report of Rapid-eye-movement (REM】 sleep behavior disorder
- Mild cogniti ve impairment: a concept useful for early detection and intervention of dementia
- Pesticides availability and medically serious suicide attempts in China
- Effi cacy and safety of generic escitalopram versus Lexapro in the treatment of major depression: a multi center doubleblinded randomized controlled trial
- Relationship of changes in cognitive and depressive symptoms during anti depressant treatment of individuals with geriatric depression and their relationship to the APOE epsilon 4 allele