肌钙蛋白I和肌红蛋白定量检测在心血管疾病中的应用研究
2009-05-08 03:33唐浩熙李介华张小勇陆灶其梁大立李冬秀
中国实用医药 2009年5期
唐浩熙 李介华 张小勇 陆灶其 梁大立 李冬秀
【摘要】 目的 探讨肌钙蛋白I (cTnI)、肌红蛋白(Mb)定量检测在心血管疾病中的临床价值。 方法 A组:健康对照组100例,男女各50例,平均52岁。于早晨空腹取静脉血3 ml送检。B组:冠心病患者153例,男94例,女59例,于早晨空腹取静脉血3 ml送检;C组:急性心肌梗死(AMI)无合并症组158例,其中男121例,女37例,年龄24~86岁,平均66岁,于胸痛发作后3 h抽静脉血3 ml送检。D组:AMI合并心力衰竭组146例,男 118 例,女28 例。年龄40~84岁,平均65岁,于胸痛发作后3 h临床表现为有心力衰竭症状时抽静脉血3 ml送检。A、B 、C、D组全部采用全自动微粒子化学发光分析仪定量检测cTnI、Mb 。结果 A组cTnI浓度为(0.27±0.18) μg/L ,Mb浓度为(42±21 )μg/L;B组cTnI浓度为(0.45±0.17) μg/L ,Mb浓度为(46±20 )μg/L,A组与B组差异无统计学意义( P=0.52,P>0.5);C组cTnI浓度为(16.71±14.19)μg/L ,Mb浓度为(522±392)μg/L;D组cTnI浓度为(25.01±19.12)μg/L ,Mb浓度为(936±712)μg/L;B组与C、D组比较差异具有统计学意义(P=0.000,P<0.01);C组与D组比较差异具有非常显著性的意义(P=0.002,P<0.01)。结论 cTnI、Mb对冠心病患者继发急性心肌梗死有很高的诊断价值,对有胸痛症状的冠心病患者检测cTnI、Mb可早期诊断AMI,及时溶栓和治疗。从C组和D组的结果来看,D组cTnI 、Mb比C组显著增高,因此,当cTnI浓度达到(25.01±19.12)μg/L,Mb浓度达到(936±712)μg/L时,可合并心力衰竭。
【关键词】 肌钙蛋白I;肌红蛋白;急性心肌梗死;冠心病;定量;价值
Troponin I and myoglobin in the quantitative detection of cardiovascular disease in the applied research TANG Hao-xi,LI Jie-hua,ZHANG Xiao-yong,et al.The Fifth Affiliated Hospital of Medical College Jinan University,Qingyuan City Peoples Hospital,Qingyuan,Guangdong Province 511500,China
【Abstract】 Objective Discussion troponin I (cTnI),myoglobin (Mb) in the quantitative detection of cardiovascular disease in clinical value.Methods Group A:control group of 100 healthy me n and women of all 50 people,average age 52 years old.Venous access in the morning on an empty stomach 3 ml inspection.Group B:153 patients with coronary heart disease,94 men,59 women,on an empty stomach in the morning,take blood 3 ml inspection;C:acute myocardial infarction (AMI) without complications group of 158 people,121 cases of men,37 women patients,aged 24-86 years old,the average 66-year-old,at 3 hours after onset of chest pain pump blood 3 ml inspection.D Group:AMI heart failure combined group of 146 people,118 men and 28 women.Age 40-84 years old,the average 65-year-old,at 3 hours after chest pain onset of clinical performance for heart failure symptoms when blood pumping 3 ml inspection.A,B,C,D groups the use of fully automated microparticle chemiluminescence analyzer quantitative detection of cTnI,Mb.Results A group of cTnI concentration of (0.27 ± 0.18) μg/L,Mb concentration of(42 ± 21) μg/L;B group cTnI concentration of (0.45 ± 0.17 )μg/L,Mb concentration of(46 ± 20) μg/L,A and group B group differences There was no significant meaning (P= 0.52,P> 0.5);C group cTnI concentration of (16.71 ± 14.19)μg/L,Mb concentration of(522 ± 392)μg/L;D group cTnI concentration of(25.01 ± 19.12)μg/L,Mb concentration To (936 ± 712)μg/L;B and Group C,D group differences in a very significant meaning (P= 0.000,P<0.01);C Group D and group differences in a very significant meaning (P= 0.002,P<0.01).ConclusionS cTnI,Mb of coronary heart disease in patients with acute myocardial infarction secondary diagnosis of a very high value on the symptoms of chest pain in patients with coronary heart disease detection of cTnI,Mb to the early diagnosis of AMI,and thrombolytic therapy in a timely manner.From Group C and Group D results,D group cTnI,Mb than the C group were significantly increased,so that when the concentration of cTnI reached (25.01 ± 19.12)μg/L,Mb concentration reached (936 ± 712)μg/L,could be merged with heart failure.
【Key words】 Troponin I;Myoglobin;Acute myocardial infarction;Coronary heart disease;Quantitative;Value
探讨心血管疾病患者与肌钙蛋白I、肌红蛋白浓度的关系,并了解心肌蛋白在冠心病、AMI无合并症、AMI合并心力衰竭患者中的水平变化,本文对153例冠心病、158例AMI无合并症与146例AMI合并心力衰竭患者进行cTnI、Mb定量检测,以探讨其临床价值,现将结果报告如下。
1 材料和方法
1.1 病例选择 ①A组:健康对照组100例,全部为本院保健科健康体检人员,男50例,女50例,年龄21~66岁,平均46岁,经全面检查均无心、肝、肺、肾等疾病,符合健康标准;②B组:冠心病患者153例,男94例,女59例,诊断标准按欧洲心脏学会制定的标准为依据;③ C组:AMI无合并症组158例均为我院住院患者,其中男121例,女37例,年龄24~86岁,平均66岁,均有胸痛等临床表现,结合心电图及心肌蛋白(cTnI Mb)改变而证实;④D组:AMI合并心力衰竭患者146例均为本院住院患者,男118例,女28例。均有呼吸困难,心率>100次/min,两肺可闻湿性啰音与临床表现,结合心电图及心肌蛋白(cTnI Mb)改变而证实,心力衰竭的诊断标准按欧洲心脏学会制定的标准为依据。
1.2 方法
1.2.1 标本采集 A、B两组于09:00空腹抽静脉血3 ml送检;C组:于胸痛发作后3 h抽静脉血3 ml送检。D组:于胸痛发作后3 h临床表现为有心力衰竭症状时抽静脉血3 ml送检。
1.2.2 标本检测方法及试剂 cTnI Mb采用美国BECKMAN COULTER公司提供的ACCESS2全自动微粒子化学发光免疫分析系统检测,操作由专业人员严格按仪器操作规程操作,试剂由日本株式会社提供。阳性标准:cTnI >0.5 μg/L,Mb>70 μg/L。
1.3 统计学方法 计量资料以均数±标准差(x±s)表示,实验设计采用成组设计,两组间比较用t检验,以P<0.05有统计学意义。全部数据采用SPSS 10.0软件进行统计学处理。
2 结果
2.1 对照组与B、C、D组cTnI Mb含量关系见下表1。
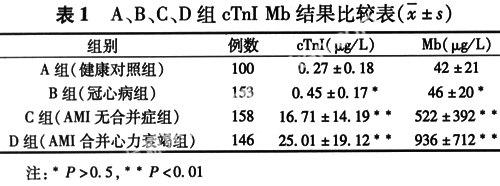
2.2 A组与B组差异无统计学意义(P=0.52,P>0.5);B组与C、D组比较差异具有非常显著性的意义(P=0.000,P<0.01);C组与D组比较差异具有非常显著性的意义(P=0.002,P<0.01)。
3 讨论
3.1 冠心病主要是供给心脏营养物质的血管-冠状动脉发生严重粥样硬化或痉挛,使冠状动脉狭窄或阻塞,以及血栓形成造成管腔闭塞,导致心肌缺血缺氧或梗死的一种心脏病,亦称缺血性心脏病[1]。心肌梗死一般是由于冠状动脉粥样硬化引起管腔狭窄,血管内膜粗糙不平,局部血流通过减少或缓慢,血小板聚集、吸附和血栓形成,致使冠脉闭塞,相应的心肌发生急性缺血性坏死所致。AMI的心肌病理改变是缺血缺氧,细胞内容物外渗,严重者为不可逆性心肌坏死。目前,国外临床资料[2-6]均认为,相对心肌酶标志物,cTnI能更早提供AMI诊断依据。心绞痛后(3.2±1.2) h内可在血中出现并被检测到,再灌注患者cTnI峰值出现于心绞痛后12 h[7]。cTnI 是肌钙蛋白复合体中亚单位之一,参与钙离子诱导的肌肉收缩,心肌和骨骼肌中的肌钙蛋白由不同具有独特氨基序列的基因决定的,所以,cTnI具有组织特异性。cTnI仅存于心肌细胞中[8],为心肌特异型的肌钙蛋白,其敏感性和特异性比CK-MB高,是高度特异、高度灵敏的反映心肌细胞损伤坏死的标志物[9,10]。正常人血液中含量一般低于0.5 μg/L,当心肌细胞缺血缺氧,心肌细胞发生可逆性损伤时,游离的cTnI从被损的细胞膜释放入血液,造成短暂而迅速升高,如发生不可逆性损伤时,结合部分的cTnI从肌纤维上降解下来,不断释放,导致血中cTnI持续升高[11-12]。
3.2 当冠心病患者的冠状动脉硬化并发生冠状动脉痉挛时,可引起心肌缺血,心肌细胞坏死。cTnI Mb增高[13]。如较长时间的冠脉持续痉挛可使冠脉管腔由部分阻塞变为完全阻塞,随之发生梗死;或因冠脉痉挛挤压原有的粥样斑块使其破裂出血,并继发血栓形成而致急性心肌梗死,这时cTnI Mb可显著增高[14-15]。因此,cTnI Mb对冠心病患者是否发生冠状动脉痉挛或因冠脉痉挛挤压原有的粥样斑块使其破裂出血,并继发血栓形成而致急性心肌梗死有很高的诊断价值,对有胸痛症状的冠心病患者检测cTnI Mb可早期诊断AMI,及时溶栓和治疗。
3.3 心力衰竭患者由于改变了冠状动脉血流储备,心肌氧供应失常,导致心肌损伤,cTnI外漏并通过受损细胞膜弥散进入细胞间质,随之进入血管,引起cTnI升高[16],AMI合并心力衰竭主要是冠状动脉阻塞引起心肌缺血缺氧,引起心肌细胞损伤甚至死亡,导致心力衰竭,受损或死亡的心肌细胞大量释放cTnI入血,导致cTnI浓度显著升高[17-18]。从C组和D组的结果来看,D组cTnI Mb比C组显著增高,因此,当cTnI浓度达到(25.01±19.12)μg/L ,Mb浓度达到(936±712)μg/L时,可合并心力衰竭。
参 考 文 献
[1] Mohan S,Wilkes L,Jackson D.Lifestyle of Asian Indians with coronary heart disease:the Australian context.Collegian,2008,15(3):115-121.
[2] Herlitz J,Svensson L.The value of biochemical markers for risk stratification prior to hospital admission in acute chest pain.Acute Card Care,2008,9:1-8.
[3] Buller CE,Fu Y,Mahaffey KW,et al.ST-segment recovery and outcome after primary percutaneous coronary intervention for ST-elevation myocardial infarction:insights from the Assessment of Pexelizumab in Acute Myocardial Infarction (APEX-AMI) trial.Circulation,2008,118(13):1335-1346.
[4] Liao J,Chan CP,Cheung YC,et al.Human heart-type fatty acid-binding protein for on-site diagnosis of early acute myocardial infarction.Int J Cardiol,2008:19.
[5] Leuschner F,Li J,Goser S,et al.Absence of auto-antibodies against cardiac troponin I predicts improvement of left ventricular function after acute myocardial infarction.Eur Heart J,2008,29(16):1949-1955.
[6] Maia PC,Abelha FJ.Predictors of major postoperative cardiac complications in a surgical ICU.Rev Port Cardiol,2008,27(3):321-328.
[7] Ravkilde J,Nissen H ,Horder M ,et al .Independent prognostic Value of serum creatine kinase is oenzyme MB mass ,cardiac Troponin T and myosin light chain levels in suspected acute myocardial infarction .J Am Coll Cardiac ,1995,25:574-581.
[8] Bodor GS ,Porterfield E ,Voss ,et al .Cardiac troponin I is not expressed in fetal and healthy or diseased adult human skeletal musle tissue .Clin Chem,1995,41(12):1710-1725.
[9] Qiao XZ,Yang YM,Xu ZR,et al.Relationship between resistin level in serum and acute coronary syndrome or stable angina pectoris.J Zhejiang Univ Sci B,2007 ,8(12):875-880.
[10] Zhang G,Zhou B,Zheng Y,et al.Time course proteomic profile of rat acute myocardial infarction by SELDI-TOF MS analysis.Int J Cardiol,2008:2.
[11] Mekontso Dessap,A Lellouche,N Audard V,et al .Effect of renal failure on peak troponin Ic level in patients with acute myocardial infarction.Cardiology,2008,109(4):217-221.
[12] Saiki A,Iwase M,Takeichi Y,et al .Diversity of the elevation of serum cardiac troponin I levels in patients during their first visit to the emergency room.Circ J,2007,71(9):1458-1462.
[13] Kavsak PA,MacRae AR,Newman AM,et al .Effects of contemporary troponin assay sensitivity on the utility of the early markers myoglobin and CKMB isoforms in evaluating patients with possible acute myocardial infarction.Clin Chim Acta,2007,380(1-2):213-216.
[14] Al-AhmadRS,Mahafzah AM,Al-Mousa E N.Immunological changes in acute myocardial infarction.Saudi Med J,2004,25(7):923-928.
[15] Chapelle JP,Dubois B,Bovy C.Comparison of plasma cardiac troponins T and I in chronically hemodialyzed patients in relation to cardiac status and age.Clin Chem Lab Med,2002,40(3):240-245.
[16] GaudinoM,Anselmi A,Abbate A,et al.Myocardial apoptosis predicts postoperative course after aortic valve replacement in patients with severe left ventricular hypertrophy.J Heart Valve Dis,2007,16:344-348.
[17] Stanley BA,Gundry RL,Cotter RJ,et al.Heart disease,clinical proteomics and mass spectrometry.Dis Markers,2004,20:167-178.
[18] Maynard C,Lowy E,Rumsfeld J,et al .The prevalence and outcomes of in-hospital acute myocardial infarction in the Department of Veterans Affairs Health System.Arch Intern Med,2006,166(10):1410-1416.
猜你喜欢
中学生数理化·高一版(2022年4期)2022-05-09
健康博览(2020年2期)2020-02-27
中学生数理化·高一版(2016年8期)2016-12-07
中国实用医药(2016年24期)2016-10-17
中国民族民间医药·下半月(2014年4期)2014-09-26
祝您健康(1985年3期)1985-12-30
祝您健康(1985年1期)1985-12-29