双相障碍患者的风险决策偏好:来自三水平元分析的证据
2025-01-13 00:00:00陆嘉琦李雨斯何贵兵
心理学报 2025年1期
关键词:元分析






摘 "要""本研究采用三水平元分析定量估计双相患者与健康个体的风险决策偏好差异, 并检验该差异是否受到样本特征和测量特征的调节。基于71篇文献和176个效应量的元分析发现, 双相患者比健康个体更偏好风险寻求(Hedges' g"= 0.301), 且这一偏好在风险态度量表(Hedges' g"= 0.624)、行为实验任务(Hedges' g"= 0.252)和日常风险行为(Hedges' g"= 0.312)中都稳定存在。同时, 该差异还受到年龄(β"= 0.009)和心境阶段的调节, 其中不论心境阶段如何, 双相患者均比健康个体更偏好风险寻求(缓解期: Hedges' g"= 0.245; lt;轻gt;躁狂期: Hedges' g"= 0.604; 重性抑郁期: Hedges' g"= 0.417)。此外, 在行为实验任务中, 该差异受到年龄(β"= 0.012)和地区的调节。特别是欧洲(Hedges' g"= 0.419)和南美洲(Hedges' g"= 0.420)的患者, 以及在爱荷华赌博任务(Hedges' g = 0.396)和剑桥赌博任务(Hedges' g = 0.220)中的患者, 均比健康个体更偏好风险寻求; 而在日常态度和行为中, 该差异仅受到心境阶段的调节, lt;轻gt;躁狂期患者(Hedges' g"= 0.747)比健康个体更偏好风险寻求。本研究首次通过多种风险决策偏好测量类型探讨双相障碍与风险决策的关系, 得出了较稳定的结果, 并提出未来研究应充分考虑心境阶段、任务类型等因素的影响, 深入挖掘双相障碍影响风险决策的心理机制, 为双相障碍的临床管理和心理教育提供参考。
关键词""双相障碍, 风险决策, 元分析, 决策范式, 跨心境特异性
分类号""B849: C91; R395
1 "引言
双相障碍(Bipolar Disorder)是一种以躁狂、轻躁狂、重性抑郁交替反复发作为特征的心境障碍, 影响着全世界约4000万人(WHO, 2022), 也是我国六大重性精神障碍之一。双相障碍的全球终生患病率约为2.4%, 部分地区高达4.4% (Merikangas et al.,"2011), 而在我国约为0.6% (Huang et al., 2019)。双相患者认知、社会和职业功能受损, 有极高的自杀倾向, 容易做出有灾难性后果的行为。据调查, 双相患者自杀率是精神障碍中最高的, 约为一般人群的20~30倍(Plans et al., 2019), 其中15%~20%的自杀企图是致命的(Schaffer et al., 2015)。受其影响最大的是社会主要劳动人口(Plana-Ripoll et al., 2023), 因此该疾病会造成严重的经济和社会成本。然而, 双相障碍心境交替乃至混合发作的复杂特征, 使其易误诊、难治疗。鉴于双相障碍的普遍性、严重性和复杂性, 学界一直重视探索其认知和行为特征, 以助于有效识别、评估和干预。
决策(Decision-making)作为高级认知功能, 又关乎个体日常行为, 其如何受双相障碍的影响备受关注。有研究发现双相患者的决策功能受损, 容易做出非理性、不适宜的决策(如Amlung et al., 2019; Ramírez-Martín et al., 2020), 进而影响其行为。双相患者的风险决策尤为重要, 它可能产生潜在的严重后果, 不仅关乎患者的社会、职业功能, 甚至可能危及其身体健康和生命安全, 如自杀行为等(Miller amp; Black, 2020)。因此, 有必要深入了解患者的风险偏好, 及时识别并干预其风险行为。
风险决策(Risky Decision-making)是指个体在不确定情境中的决策, 其风险决策偏好(简称风险偏好)常分为风险寻求和风险规避。风险寻求(risk-seeking)是指个体在面对多个风险选项时选择高风险选项的倾向(Lejuez et al., 2002; Meertens amp; Lion, 2008)。与之相反的是风险规避(risk-aversion)。双相障碍的诊断标准指出, 患者在躁狂或轻躁狂发作时容易过度参与那些很可能产生痛苦后果的高风险活动(APA, 2013), 这意味着双相患者常伴有风险决策异常。对患者的临床观察(Krantz et al., 2018; Williams et al., 2017)、行为实证研究(Edge et"al., 2013; Richard-Devantoy et al., 2016)和神经影像学研究(Blankenstein et al., 2017; Miklowitz amp; Johnson, 2006)也表明双相障碍会影响患者的风险偏好。
以往研究主要通过比较双相患者与健康个体在风险偏好上的差异来探讨双相障碍对风险决策的影响, 但所得结论并不一致。早期研究者根据躁狂或轻躁狂诊断中“过度地参与那些很可能产生痛苦后果的高风险活动” 的标准, 结合双相障碍常与风险行为相关的精神障碍共病(如, 物质使用障碍和破坏性、冲动控制与品行障碍) (APA, 2013), 推测双相患者比健康个体更偏好风险寻求(如Ernst et"al., 2004; Holmes et al., 2009), 且这一推测也得到了行为实证研究和神经影像学研究的证据支持。一方面, 以往研究通过比较双相患者与健康个体在自陈量表和行为实验任务中的风险偏好, 发现双相患者比健康个体更偏好风险寻求。如, 在自陈量表上, 双相患者在特定领域风险态度量表(Domain-"Specific Risk-Taking Scale, DOSPERT)和反应风格量表(Response Styles Questionnaire, RSQ)的冒险维度上的得分均比健康个体更高, 更偏好风险寻求(Pavlickova et al., 2014; Thomas et al., 2007); 在行为实验任务中, 双相患者比健康个体在爱荷华赌博任务(Iowa Gambling Task, IGT)中更偏好选择不利卡牌, 即风险选项(Edge et al., 2013); 在剑桥赌博任务(Cambridge Gambling Task, CGT)中下的赌注更高, 即更偏好风险寻求(Linke et al., 2013)。另一方面, 神经影像学证据也表明, 双相患者的大脑结构较健康个体有所变化, 且这一变化与风险决策有关, 使其可能更偏好风险寻求。如, 患者的额叶白质束完整性下降, 研究表明这种完整性破坏使其更偏好风险寻求(Scholz et al., 2016); 又如, 患者的顶−枕−小脑网络灰质减少, 使其冲动性增加, 更容易做出风险行为(Lapomarda et al., 2021)。因此, 越来越多研究者认为, 风险寻求增加是双相患者常见的认知和行为特征, 并可能成为双相障碍潜在的核心症状之一(Hıdıroğlu et al., 2013; Ramírez-Martín et"al., 2020)。
然而, 近期有一些研究却发现双相患者的风险偏好并非始终不同于健康个体(如Martino et al., 2011; Reddy et al., 2014), 甚至有些研究表明双相患者比健康个体更偏好风险规避。如, Wong等人(2021)采用气球模拟风险任务(Balloon Analogue Risk Task, BART)发现, 双相患者在未爆炸气球中的平均按压次数和气球爆破率都显著小于健康个体, 即更偏好风险规避。Hart等人(2019)则采用概率折扣任务(Probability Discounting, PD)发现, 双相患者的折扣率显著大于健康个体, 即更偏好保守选项。本研究在深入分析上述相互矛盾的研究结果后, 推测双相患者与健康个体风险偏好差异的方向以及程度可能受到三个方面的影响。
1.1""心境阶段的调节作用
双相患者的风险偏好可能随心境阶段变化而变化。根据美国精神疾病诊断与统计手册第五版(Diagnostic and Statistical Manual of Mental Disorder Fifth Edition, DSM-V; APA, 2013), 双相患者有时会表现出心境膨胀、极度自信, 目标活动增多, 易过度参与高风险活动, 即lt;轻gt;躁狂期, 包括躁狂发作和轻躁狂发作; 而有时则会表现出情绪低落、自我贬低, 思考能力下降或犹豫不决, 几乎对所有活动的兴趣或愉悦感都明显减少, 即重性抑郁期(简称抑郁期), 对应重性抑郁发作。两者常统称为发病期。而发病间隙患者的症状得到缓解, 情绪趋于稳定, 即缓解期。因此, 患者存在3种不同的心境阶段, 且在不同心境阶段下他们的认知、动机和行为表现都有明显差异。
健康个体的风险决策研究表明, 正负情绪对风险偏好的影响各异。尽管相关理论和实证研究(Isen amp; Patrick, 1983; Johnson amp; Tversky, 1983; Prietzel et al., 2020)对此影响尚未达成共识, 但情绪效价的作用不容忽视。鉴于双相障碍的心境阶段与情绪效价紧密相关, 心境阶段在风险决策研究中显得尤为重要。然而, 当前研究常忽视心境阶段的影响, 将不同心境阶段患者混合成组与健康个体比较, 这可能导致因心境阶段分布不同而导致结果产生偏差。如, Bauer等人(2017)选取30个缓解期患者、44个抑郁期患者和11个lt;轻gt;躁狂期患者形成患者组, 发现患者与健康个体在IGT任务中的风险偏好无差异; Malloy-Diniz等人(2009)则选取20个缓解期患者、10个抑郁期患者和9个lt;轻gt;躁狂期患者形成患者组, 同样选用IGT任务, 却发现患者比健康个体更偏好风险寻求。
尽管有研究区分双相患者的心境阶段, 但大多选取缓解期患者, 对发病期患者的探究相对较少。而且, 鲜有同一个研究直接比较不同心境阶段患者的风险偏好差异(仅4篇该类文献纳入后续元分析; Adida et al., 2011; Thomas et al., 2007; 魏格欣 等, 2018; Yechiam et al., 2008), 且研究结果也不一致。例如, Adida等人(2011)比较躁狂期、抑郁期和缓解期患者与健康个体的IGT任务表现, 结果发现, 不同心境阶段患者均比健康个体显著更多选择不利卡牌即更偏好风险寻求, 但是各个心境阶段间的差异并不显著(躁狂期:Cohen’s d"= 0.68; 抑郁期:Cohen’s d"= 0.59; 缓解期:Cohen’s d"= 0.35)。同样是比较3个心境阶段患者和健康个体的差异, Thomas等人(2007)发现不同心境阶段患者比健康个体在RSQ量表冒险维度上的得分都显著更高, 即更偏好风险寻求, 其中躁狂期患者的偏好程度显著大于抑郁期和缓解期患者。而同样采用IGT任务的Yechiam等人(2008)和魏格欣等人(2018)却没有发现发病期、缓解期和健康个体的差异。据此, 不同心境患者的风险偏好可能并不一致, 但由于研究量少、样本小, 其结论可靠性仍需检验。故此, 本研究采用元分析的方式, 选择心境阶段为潜在调节变量, 以探究不同心境阶段患者的风险偏好方向和程度是否有所差异。
1.2""测量特征的调节作用
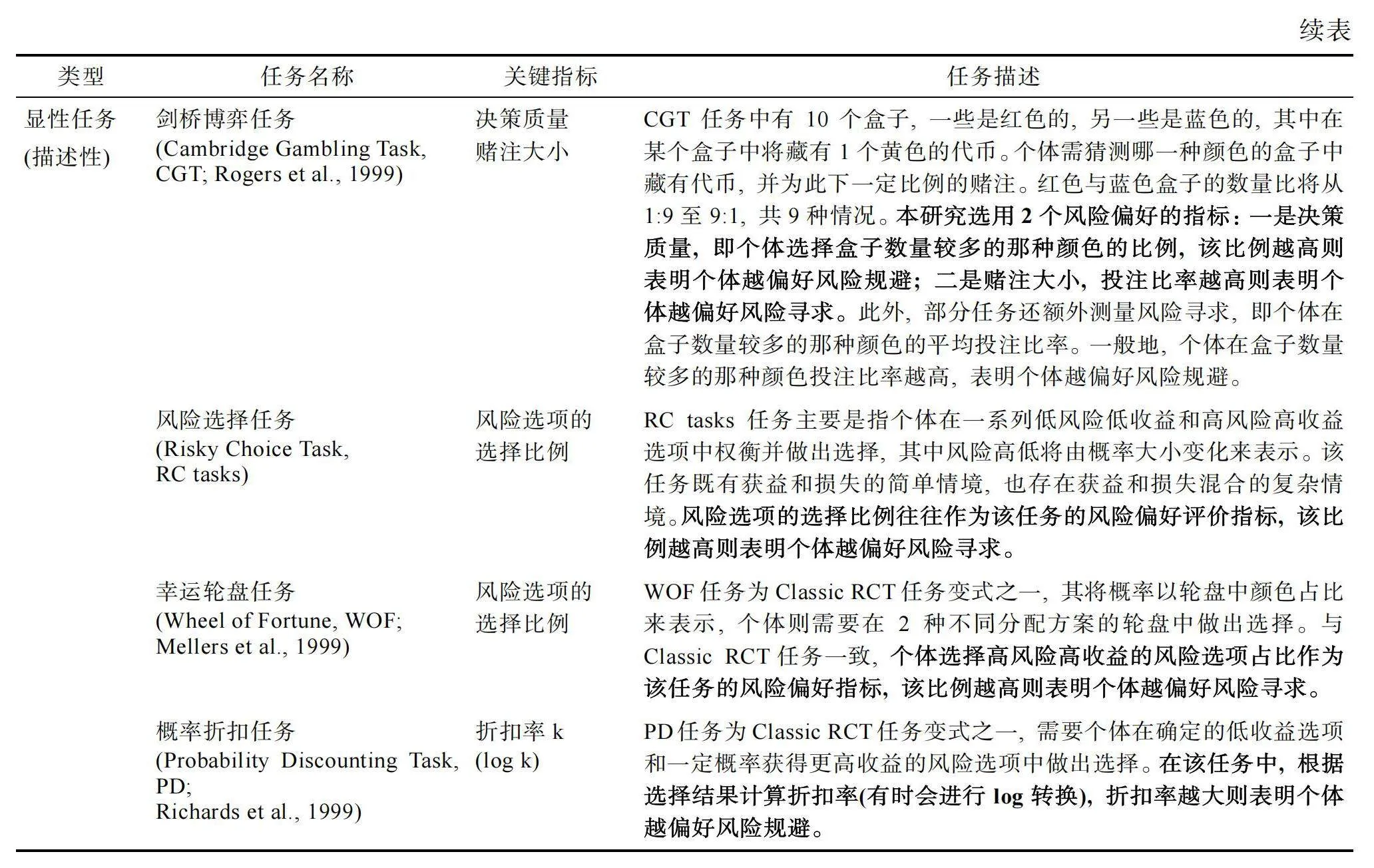
双相患者的风险偏好可能在不同测量特征下存在差异。以往研究主要采用3种测量类型来评估个体的风险偏好(Frey et al., 2017)。首先, 早期被广泛使用的测量类型是借助自陈量表中的态度题目来评估即风险态度量表。这类题目既涵盖抽象层面(如“我经常做冒险的决定”, Zhang et al., 2019), 也涉及特定情境(如“你有多大可能性用一天的收入来赌某一项体育赛事”, Blais amp; Weber, 2006)。然而, 这种测量类型虽简便, 却易受社会赞许性、记忆偏差的影响, 且难以进行动态评估。基于此, 研究者开发出了一系列行为实验任务。常见的有风险选择任务(Risky Choice Task, RC tasks), 即个体在低风险低收益选项和高风险高收益选项间选择的决策对任务; 决策对相关变式, 如幸运轮盘任务(Wheel of Forture, WOF; Mellers et al., 1999)和PD任务(Richards et al., 1999); 动态赌博任务, 如IGT任务、CGT任务等; 以及更具现实模拟性的任务, 如BART任务、钓鱼风险任务(Angling Risk Tasks, ART; Pleskac, 2008)等。这些任务虽规避了量表的局限, 但多聚焦经济结果, 生态性有限, 与真实风险决策有一定差距(Fischhoff amp; Broomell, 2020)。第三种测量类型常见于临床和流行病学研究, 直接观察和记录个体真实发生的日常风险行为(如, “你一天抽多少支烟”)。目前研究多关注健康领域的风险行为。如, 美国疾控中心的青年风险行为检测系统(Youth Risk Behavior Surveillance System, YRBSS)涵盖了非故意伤害行为、烟草使用、酒精和其他物质使用、与意外怀孕和性传播感染有关的性行为、不健康饮食和缺乏锻炼等6种风险行为(Brener et al., 2004)。我国疾控中心也有类似调查, 其保留了YRBSS的后3种行为, 并将前3种行为调整为4种行为, 即导致非故意伤害的行为、导致故意伤害的行为、物质成瘾行为和精神成瘾行为(含网络成瘾、赌博成瘾等) (季成叶, 2007)。此外, 过往对风险行为的元分析也多关注物质使用、性风险行为、危险驾驶、赌博等行为(如Roberts et al., 2021; Tinner et"al., 2018)。据此, 本研究将重点关注上述研究涉及的典型日常风险行为, 包括物质使用、性风险行为、不健康饮食、缺乏锻炼以及非故意伤害行为中的危险驾驶行为等。
然而, 当研究者采用不同的风险偏好测量类型时, 其结果可能存在差异。Frey等人(2017)采用3种测量类型39个测量指标评估1507名个体的风险偏好。结果发现, 风险态度量表与日常风险行为的关联性较强, 而行为实验任务与这两者的关联性较弱。这提示我们, 采用单一测量类型判断双相患者的风险偏好可能会导致研究结论因测量工具的局限而产生偏差。如, Hart等人(2019)发现双相患者在PD任务中的折扣率显著大于健康个体即更偏好风险规避, 但在抽烟行为上却明显高于健康个体。这也凸显了不同测量类型下双相患者风险偏好的复杂性。事实上, 不仅跨测量类型的结果有差异, 即便采用同一种测量类型, 不同风险态度量表、行为实验任务或日常风险行为间的结果也可能不同。如, Edge等人(2013)采用IGT任务发现缓解期患者比健康个体更偏好风险寻求, 而Wong等人(2021)在BART任务中却发现缓解期患者比健康个体更偏好风险规避。即便是同一研究, 选用不同任务或行为也会造成结果差异。如, Ibanez等人(2012)同时采用IGT任务和理性风险决策任务(Rational Decision-"Making Under Risk, RDMUR)比较双相患者与健康个体的风险偏好, 但仅在IGT任务中发现患者比健康个体更偏好风险寻求; Di Nicola等人(2010)发现, 同样测量日常风险行为, 双相患者比健康个体在病态赌博、过度消费、工作成瘾和性成瘾方面的行为频率显著更高, 在网络成瘾方面显著更低, 而在运动成瘾方面无差异。可见, 不同测量类型甚至同种测量类型中不同量表、任务或风险行为都可能造成结果矛盾, 这可能和测量内容有关(如选取不同领域、不同性质的行为)。因此, 我们有理由认为, 采用单个测量类型来比较双相患者与健康个体风险偏好的研究结论可能难以全面反映个体的风险偏好。也因此, 本研究拟将测量特征(如测量类型、任务类型等)作为潜在调节变量, 检验不同测量特征下双相患者与健康个体的风险偏好差异有无变化。
1.3""人口学特征的调节作用
值得关注的是, 样本的人口学特征差异也可能导致双相患者风险偏好的研究结果不一致。Byrnes等人(1999)的元分析揭示, 在14种风险决策测量(共16种)中, 男性均比女性更偏好风险寻求。日常观察亦发现, 相较男性, 女性对风险事件更敏感(Paluckaitė amp; Žardeckaitė-Matulaitienė, 2017), 更厌恶风险(Croson amp; Gneezy, 2009), 更少做出风险行为(Charness amp; Gneezy, 2012; Dir et al., 2014)。双相患者中, 性别与风险偏好的关系同样值得探讨。研究表明, 男女双相患者在临床症状上存在差异(Benazzi, 2003)。如, 女性更易抑郁, 自杀意图高, 容易出现进食、焦虑等问题; 而男性更易躁狂, 伴随酗酒和其他物质滥用问题(Azorin et al., 2013)。然而, 这些症状差异是否意味着风险偏好的不同尚不清晰, 因此不同性别的患者与健康个体的风险偏好差异是否不同仍需探究。本研究旨在探讨女性占比对双相患者与健康个体风险偏好差异的影响, 以检验性别的调节作用。若双相患者存在与健康个体相似的性别差异, 那么女性占比的增加可能会减少两者的风险偏好差异; 反之, 若这一性别差异消失或逆转, 则两者的风险偏好差异可能会随女性占比增加而扩大。
年龄对风险偏好的影响也值得关注。研究表明, 相较青少年, 成年人常表现出更低的风险寻求(Defoe et al., 2015; Josef et al., 2016)。然而, 这一趋势在双相患者中是否存在值得探究。双相患者常伴有认知功能损害(Bora et al., 2009), 且随着年龄增长, 这种损害可能加剧(John et al., 2019; Lewandowski et al., 2014), 因而可能导致老年患者做出更多非理性的风险决策。另一方面, 双相障碍的发病年龄较早(Bolton et al., 2021), 超过六成患者在21岁前发病(Duffy, 2009)。青少年和成年早期患者常面临混合症状、病程长和共病障碍多等问题, 这可能对其正常发育和社会心理功能造成较大影响, 继而增加了他们自杀、物质滥用、学业问题等风险(Birmaher, 2013)。据此推测, 年轻患者也可能更偏好风险寻求。可见, 目前研究对双相患者的年龄如何影响其风险偏好尚存争议, 因而双相患者与健康个体的风险偏好差异如何受年龄影响不得而知。若年龄对双相患者和健康个体的风险偏好的影响趋势相似, 那么两者的风险偏好差异就可能随年龄增大而减小; 反之, 若该影响趋势减弱甚至方向相反, 那么两者的风险偏好差异则可能随年龄增大而扩大。因此, 我们将年龄作为潜在调节变量, 探究其是否影响双相患者与健康个体的风险偏好差异。此外, 根据元分析需要, 本研究还将纳入样本受教育程度和所属地区作为潜在调节变量。
综上所述, 双相患者的风险偏好与健康个体是否存在差异以及差异的方向和程度需要进行系统性梳理。虽然有研究者对2019年前发表的双相障碍和风险决策关系的研究开展过元分析(Edge et al., 2013; Ramírez-Martín et al., 2020; Richard-Devantoy et al., 2016), 但Edge等人(2013)和Richard-"Devantoy等人(2016)的元分析仅纳入了采用IGT任务的研究结果, 不足以全面反映双相患者的风险决策特征。因此, 本研究将纳入多种风险偏好测量类型的研究(即风险态度量表、行为实验任务和日常风险行为等)。再者, 此前元分析纳入的研究样本几乎全部来自西方国家(Ramírez-Martín et al., 2020), 且主要关注缓解期患者(Edge et al., 2013)或有无自杀行为的患者(Richard-Devantoy et al., 2016), 因而结果的泛化性和可靠性都待检验。因此, 本研究将基于更全面的最新文献检索结果(6个数据库中截至2024年4月的文献), 将风险决策测量特征(测量类型、任务类型、任务明确性和领域类型)、患者心境阶段(缓解期、抑郁期和lt;轻gt;躁狂期)、样本人口学特征(性别、年龄等)等纳入元分析, 再次探索双相障碍和风险决策的关系, 并检验测量特征、心境阶段、人口学特征等的调节。
2 "方法
本研究已在PROSPERO平台进行预注册, 预注册编号为CRD42022346204。
2.1 "文献检索
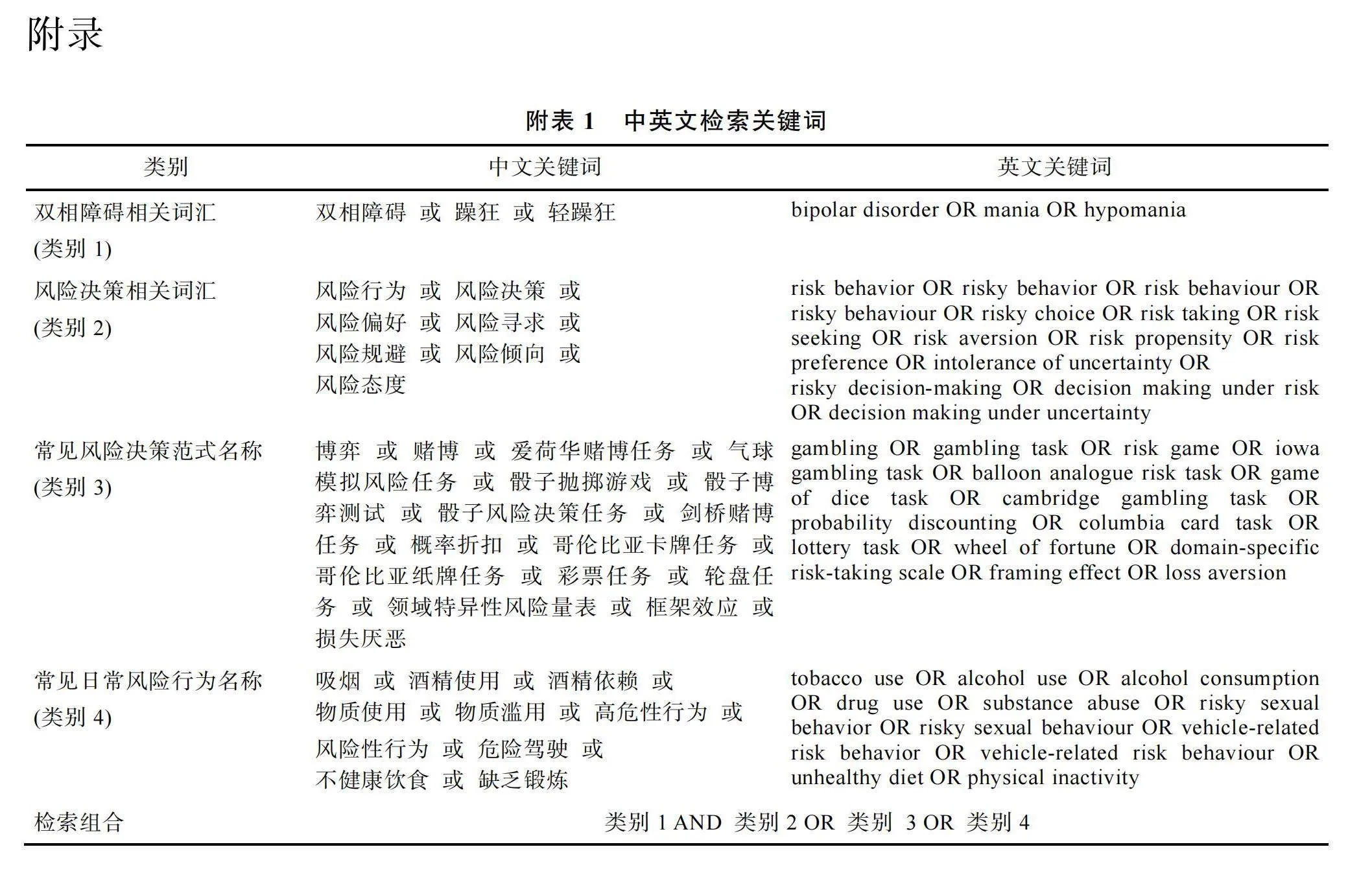
文献检索涵盖中英文献, 检索时间自数据库建立至2024年4月15日。中文文献检索使用中国知网和万方两个数据库, 而英文文献检索使用Web of Science、PubMed、Scopus和PsycINFO四个数据库。同时本研究还采用文献回溯法, 从相关元分析和综述的参考文献中筛选论文以查漏补缺。基于研究主题, 文献检索选择与“双相”和“风险决策”相近或相关的中英文词汇为检索关键词。中英文检索词都由4类词汇组成:(1)双相障碍相关词汇; (2)风险决策相关词汇; (3)常见风险决策范式名称; (4)常见日常风险行为名称(具体检索词见网络版附表1)。
2.2""文献纳入与排除标准
文献纳入标准同时包括:(1)包含以双相障碍为主要诊断的患者组; (2)包含未有任何精神病学诊断的健康对照组; (3)包含风险决策的测量(风险态度量表、行为实验任务或者日常风险行为)。在全文筛选阶段实施的其他标准包括:(4)有明确的诊断标准(如, DSM-V); (5)研究提供足够数据计算效应量(如平均数、标准差和样本量等)。如果发现未报告可转换指标的研究, 我们尝试通过在已发表的双相
障碍与风险决策的元分析(Edge et al., 2013; Ramírez-Martín et al., 2020; Richard-Devantoy et al., 2016)中查找获得相关数据, 若仍无法获得则排除该研究。最终Yechiam等人(2008)的效应量数据从Edge等人(2013)的元分析中获取; (6)数据重复仅保留其中一篇, 如会议摘要以论文形式发表在学术期刊并且报告相关数据, 则以正式发表的学术论文为准, 反之采用会议摘要里的数据。
如图1所示, 文献筛查包括了检索、初筛、标题/摘要筛选和全文筛选4个阶段。两名评价者(本文的第1和第2作者)依据纳入标准进行筛查, 确定最终纳入元分析的文献。本研究按上述标准检索出8153篇文献, 其中7785篇在标题和摘要筛选时被排除。对剩余368篇文献进行全文筛选, 最终纳入71篇文献。同时, 我们从相关综述和元分析的参考文献列表中又发现并纳入了2篇文献。因此, 本研究最终纳入73篇文献。其中, 符合要求的中文文献有4篇, 英文文献有69篇。
2.3""数据提取与质量评价
本研究的两位作者对纳入元分析的文献独立提取所需数据, 在提取过程中主要遵循以下原则:(1)如果一篇文献同时报告多个独立样本, 则需提取各个样本的数据; (2)如果文献在不同被试特征(如有无自杀行为或不同心境阶段)中均报告对应均
值和标准差, 则需提取各个特征样本的数据; (3)如果对风险偏好有多个测量指标, 则需提取每个测量指标对应的数据。若出现两名作者提取的数据不一致时, 则需经过讨论并查阅原始文献确定最终提取方案。本研究需提取的数据变量如下:
(1)基本信息
文献信息(第一作者和发表年份)和效应量数量。
(2)样本特征
a)样本量
b)年龄:提取文献中各个组别的平均年龄(标准差)。
c)性别比:提取文献中各个组别的男女人数或性别比, 最终都转换成女性占比。
d)受教育程度:考虑到纳入文献大多采用受教育年限来反映受教育程度, 所以本研究提取文献中各个组别的受教育年限。若文献未报告该指标, 本研究将其标为缺失值。
e)所属国家及地区:提取文献中样本所属国家, 并根据国家所在地区进行标注(如, 欧洲、北美洲、亚洲等)。
f)心境阶段:提取文献中样本当时所处的心境阶段(缓解期、lt;轻gt;躁狂期和抑郁期)。若文献未报告心境阶段或将不同心境的患者混为一组比较, 本研究将其标为缺失值。
g)诊断标准:提取文献中用于判断样本患病与否的诊断标准。
h)抑郁/躁狂程度:提取文献中样本的抑郁/躁狂程度(均值和标准差)及其量表名称。
(3)测量特征
a)测量类型:提取文献中所涉及的风险偏好测量类型名称(风险态度量表、日常风险行为、行为实验任务)和所有反映风险偏好的指标名称。
b)风险决策:提取文献中样本在所有风险决策指标上的表现(均值和标准差)。
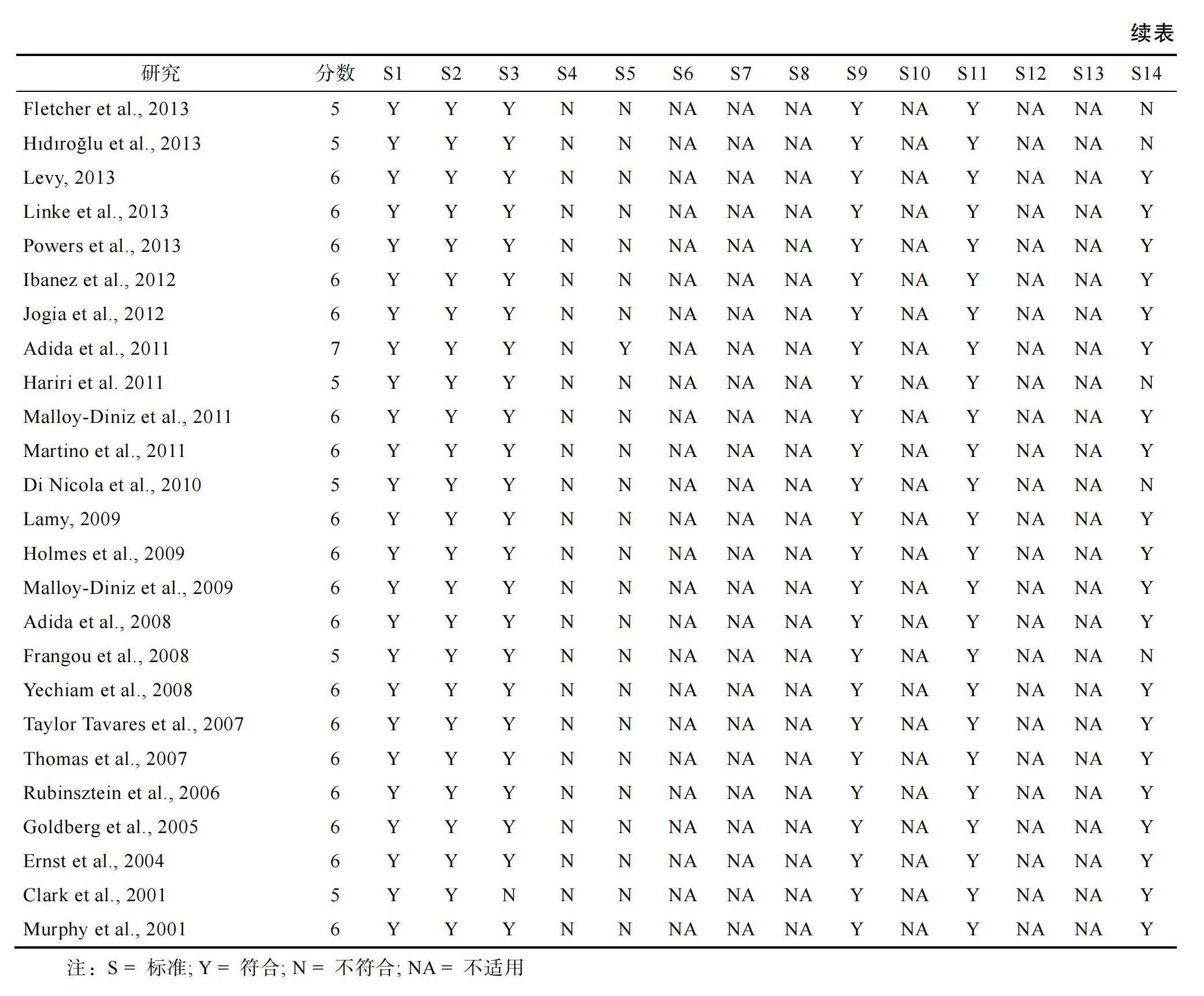
本研究还将对纳入的每篇文献进行质量评分。研究者根据美国国立卫生研究院(National Institutes of Health, NIH)的纵向和横断研究质量评估工具(Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies)的标准进行评估, 其中符合标准计1分, 不符合标准则计0分(National Institutes of Health, 2014)。横断研究的质量评分介于0~8之间, 纵向研究的质量评分则介于0~14之间。研究质量评分结果见网络版附表2, 评分越高说明文献质量越高。
2.4""统计分析
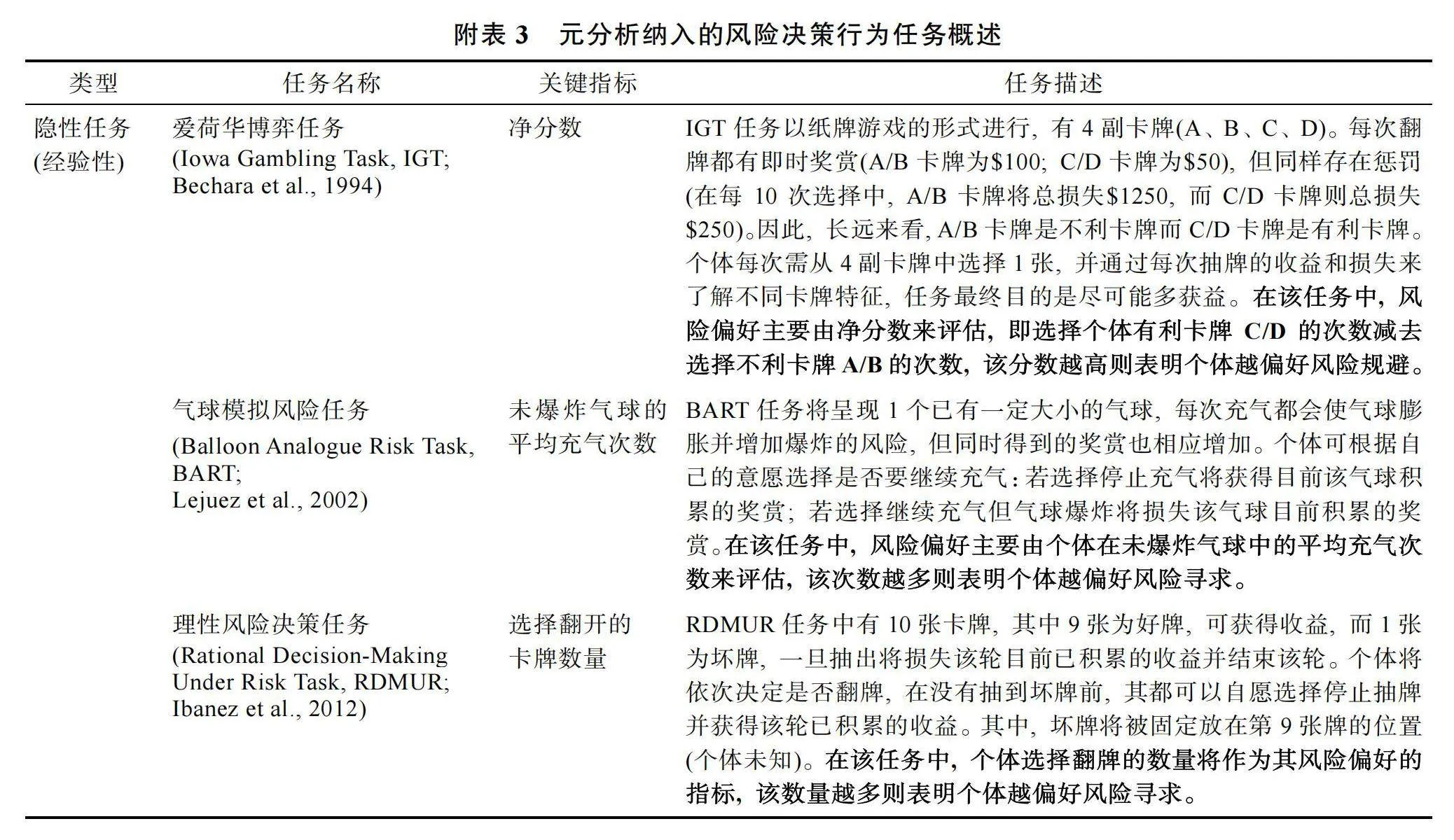
本研究使用R 4.3.2的metafor程序包(Viechtbauer, 2010)统计分析, 计算双相患者与健康个体间的风险偏好差异, 并以Hedges' g作为效应量指标。g值采用双相患者在风险决策测量指标中的表现减去健康个体的表现, 但在某些风险决策测量类型中不同指标的大小对应的风险偏好不同。例如, IGT任务的测量指标为净分数, 个体净分数越大表明其越偏好风险规避, 此时g值为正表明双相患者比健康个体更偏好风险规避; 而BART任务的测量指标为调整后平均充气次数, 个体充气次数越多则表明其越偏好风险寻求, 此时g值为正表明双相患者比健康个体更偏好风险寻求。因此, 不同测量类型中g值为正有2种截然相反的含义, 所以本研究对效应量进行统一编码, 使g值为正表示双相患者比健康个体更偏好风险寻求, g值为负则表示更偏好风险规避。如果文献报告了其他可转换为效应量的数据(如, t值), 将通过R软件的esc程序包将其转换为Hedges' g"(Lüdecke, 2019)。
目前纳入文献报告的双相患者与健康个体风险偏好差异的Hedges' g从−2.82至2.98, 结果差异较大。为了避免极端值对研究结论的影响(Kepes amp; Thomas, 2018), 本研究参考过往的元分析研究(如Fernandes amp; Garcia-Marques, 2020; Kathawalla amp; Syed, 2021), 选择剔除大于和小于所有效应量的均值或中位数3个标准差的单个效应量。研究共剔除4个效应量(Rai et al., 2018; Richard-Devantoy et al., 2016 lt;第2个效应量gt;; Saxena et al., 2023 lt;第2个效应量gt;; 朱承刚, 2020), 最终有71篇文献纳入后续元分析。
在本研究中, 部分被纳入的文献报告了多个可能存在相关的效应量。其中, 出现多个效应量的主要原因包括以下三方面:(1)文献使用多种测量工具评估风险决策; (2)文献报告了多个风险决策评价指标; (3)文献选取多个临床样本(如, 缓解期患者和lt;轻gt;躁狂期患者)。此时如若使用嵌套效应量分析, 则违反传统元分析效应量间相互独立的假设。但若不考虑效应量间的关联性, 则会使结果产生偏差(Assink amp; Wibbelink, 2016)。因此, 我们采用三水平随机效应模型并选择了限制性最大似然方法来估计模型结果。相比传统的元分析方法, 该模型考虑了效应量间的相关性, 既最大化地保留了信息, 又具有更高的统计检验力(Cheung, 2014)。
2.4.1""异质性分析
本研究采用Cochran’ Q检验和I2统计量来检验和评价研究间的异质性。Q检验判断观测到的效应量间的变异性是否大于研究的抽样误差。若Q检验的结果显著, 则数据呈现异质, 反之则同质。而I2统计量衡量的是可归因于异质性而非抽样误差造成的研究间效应量变异在总变异中所占百分比, I2越大, 异质性越明显。25%、50%和75% 分别表示异质性的低、中、高。此外, 三水平随机模型涉及三种不同的方差来源, 包括观察到的效应量的抽样方差(水平1), 同一研究中不同效应量间的方差(水平2)以及不同研究间的方差(水平3)。本研究将进一步估计抽样方差、研究内方差和研究间方差, 并对研究内和研究间方差进行对数似然比检验, 以确定其是否显著。当研究异质性较高且研究内和研究间方差显著时, 则需检验调节效应以确定异质性的来源(Gao et al., 2017)。
2.4.2""发表偏差检验
发表偏差是指已发表文献不能全面代表该主题已完成的研究总体的现象, 它往往与有统计学意义的研究结果更易发表而不显著或效应量较小的研究结果较难发表有关。为了控制发表偏差, 本研究不仅纳入已出版的期刊论文, 还纳入了暂未出版的学位论文和会议论文。同时, 本研究采用漏斗图和Egger-MLMA回归检验发表偏差。当效应量间并非相互独立时, 相较于传统Egger检验, Egger-"MLMA回归更能有效控制I类错误(Rodgers amp; Pustejovsky, 2020)。如若存在显著的发表偏差, 漏斗图将呈现不对称的现象, 同时Egger-MLMA检验结果也会显著。如果存在显著的发表偏差时, 则需要采用剪补法(Trim and fill method)进一步检验和校正(Duval amp; Tweedie, 2000)。
2.4.3""调节效应分析
本研究预期效应量间可能存在较高的异质性, 为具体分析变异的来源, 将对随机效应模型进行调节效应分析。为了避免相互关联的调节变量造成的多重共线性问题, 本研究将进一步纳入所有显著的调节变量进行多调节变量分析(Multiple-moderator Model) (Hox et al., 2010)。
(1)样本特征
大多数研究匹配了双相患者与健康个体的人口学特征, 因此本研究选取双相患者的人口学特征为调节变量, 包括年龄、性别、受教育程度, 地区(1 = 欧洲, 2 = 北美洲, 3 = 南美洲, 4 = 亚洲)和患者所处心境阶段(1 = 缓解期; 2 = lt;轻gt;躁狂期; 3 = 抑郁期)。
(2)测量特征
基于过往研究对风险决策测量类型的分类(Frey et al., 2017), 本研究在纳入的文献中区分了3种测量类型, 以考察双相障碍对风险决策的影响是否因测量类型的不同而不同。具体编码为:1 = 风险态度量表; 2 = 行为实验任务; 3 = 日常风险行为。值得注意的是, 风险态度量表聚焦个体的一般性风险态度或在特定领域的风险态度, 而日常风险行为则聚焦个体真实发生的风险行为。
行为实验任务特征:研究选取任务类型为调节变量。在行为实验任务的文献中, 除了IGT任务、BART任务和CGT任务外, 剩余任务均为风险选择任务(RC tasks)及其变式(具体介绍见网络版附表3)。据此, 将任务类型编码为1 = IGT; 2 = BART; 3"= CGT; 4 = RC tasks。此外, 研究者还根据事件概率和结果是否已知将风险决策任务分为描述性和经验性两类(Hertwig et al., 2004), 前者指个体获知所有选项的信息, 包括奖赏大小和概率高低, 如CGT任务, 而后者指个体未被告知具体概率等信息而需通过任务反馈进行学习, 如IGT任务。本研究参考Dekkers等(2016)采用任务明确性来区分这2种任务, 1 = 显性任务(对应描述性决策任务), 2 = 隐性任务(对应经验性决策任务)。
日常风险态度和行为特征:基于前人对风险决策领域的划分(Blais amp; Weber, 2006; Butler et al., 2012; Wang et al., 2016)以及本研究纳入文献所涉风险行为的领域归属情况, 本研究将风险行为所属领域分为1 = 健康; 2 = 经济; 3 = 总体态度, 并将领域类型作为调节变量。其中, 部分态度和行为反映了个体的总体风险偏好并未聚焦于单一领域(如, “我在生活的很多方面都喜欢寻求风险。”), 因此本研究将该类态度和行为归属于“总体态度”。
3 "结果
3.1""文献特征
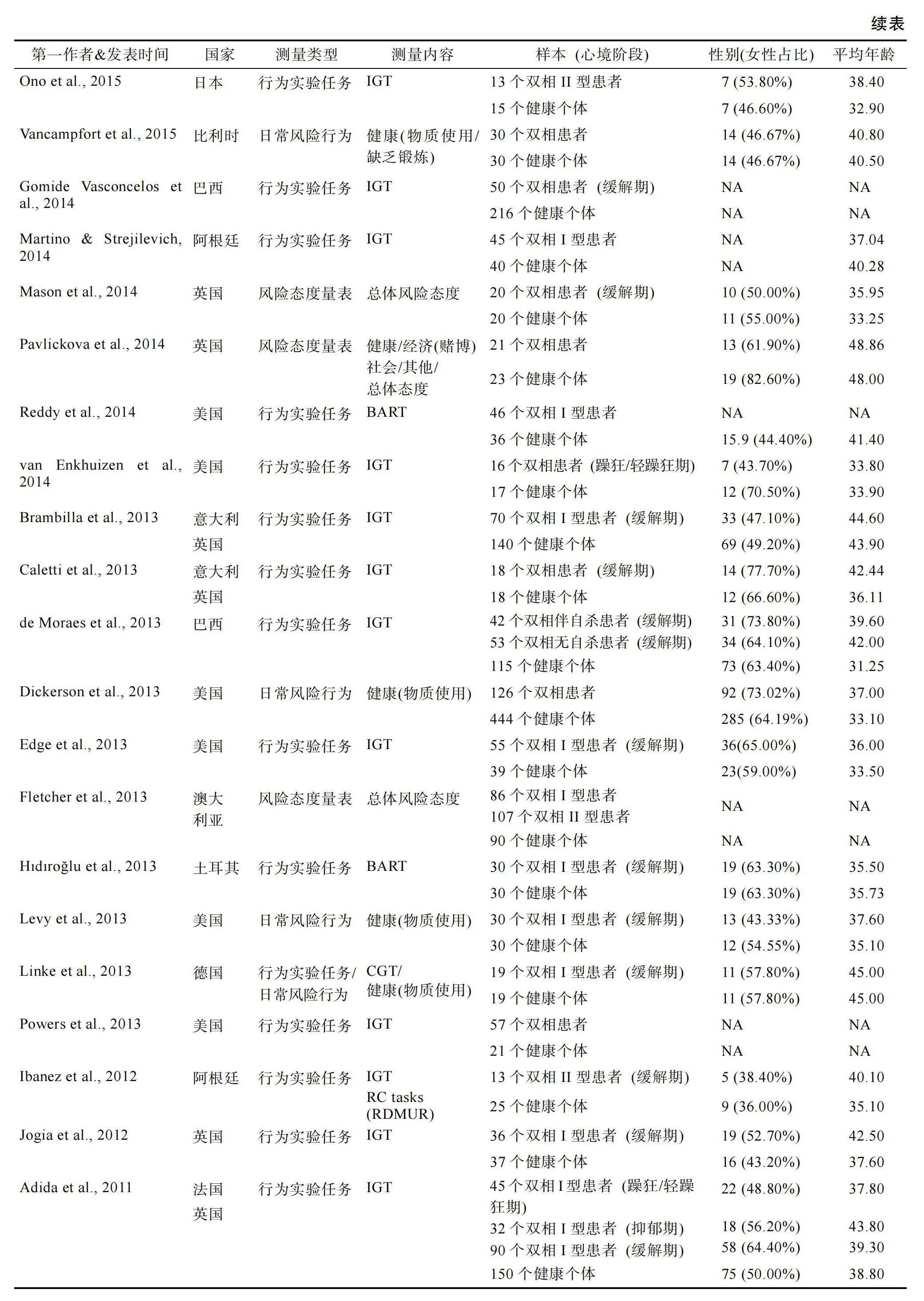
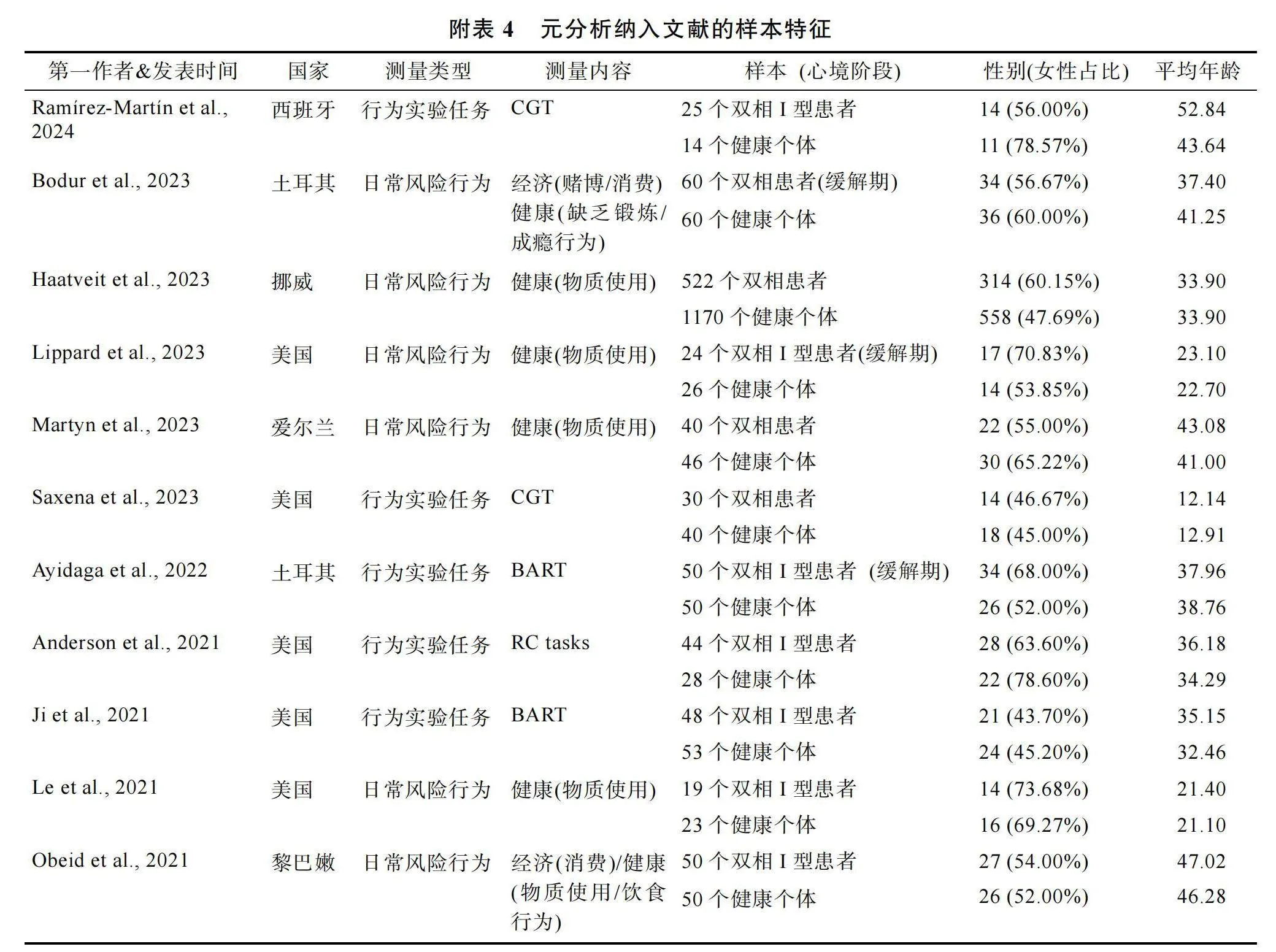
本元分析最终纳入71篇符合标准的文献, 中文文献3篇, 英文文献68篇。这71篇文献包含176个效应量, 其中同一篇文献中效应量数最多有9个, 最少的有1个。在纳入的文献中(见网络版附表4), 有12篇发表于2001~2009年(16.90%), 45篇发表于2010~2019年(63.38%), 剩余14篇发表于2020~"2024年(19.72%)。文献中被试来自欧洲(42.25%, n = 30)、北美洲(33.80%, n"= 24)、南美洲(11.27%, n"= 8)、亚洲(11.27%, n = 8)和大洋洲(1.41%, n"= 1)。所有纳入的文献均为横断研究。36篇文献纳入不同心境阶段的患者并予以区分, 其中30篇纳入缓解期患者, 8篇纳入lt;轻gt;患者, 3篇纳入抑郁期患者。在风险决策测量类型上, 有48篇文献采用行为实验任务, 其中23篇采用IGT任务, 8篇采用BART任务, 12篇采用CGT任务, 其余采用RC tasks任务。有5篇文献采用风险态度量表, 报告被试对各个决策领域或总体的风险态度, 以及有22篇文献报告被试真实的日常风险行为状况, 包括物质使用、缺乏锻炼、风险性行为等方面。
3.2 "总体模型
3.2.1 "主效应检验
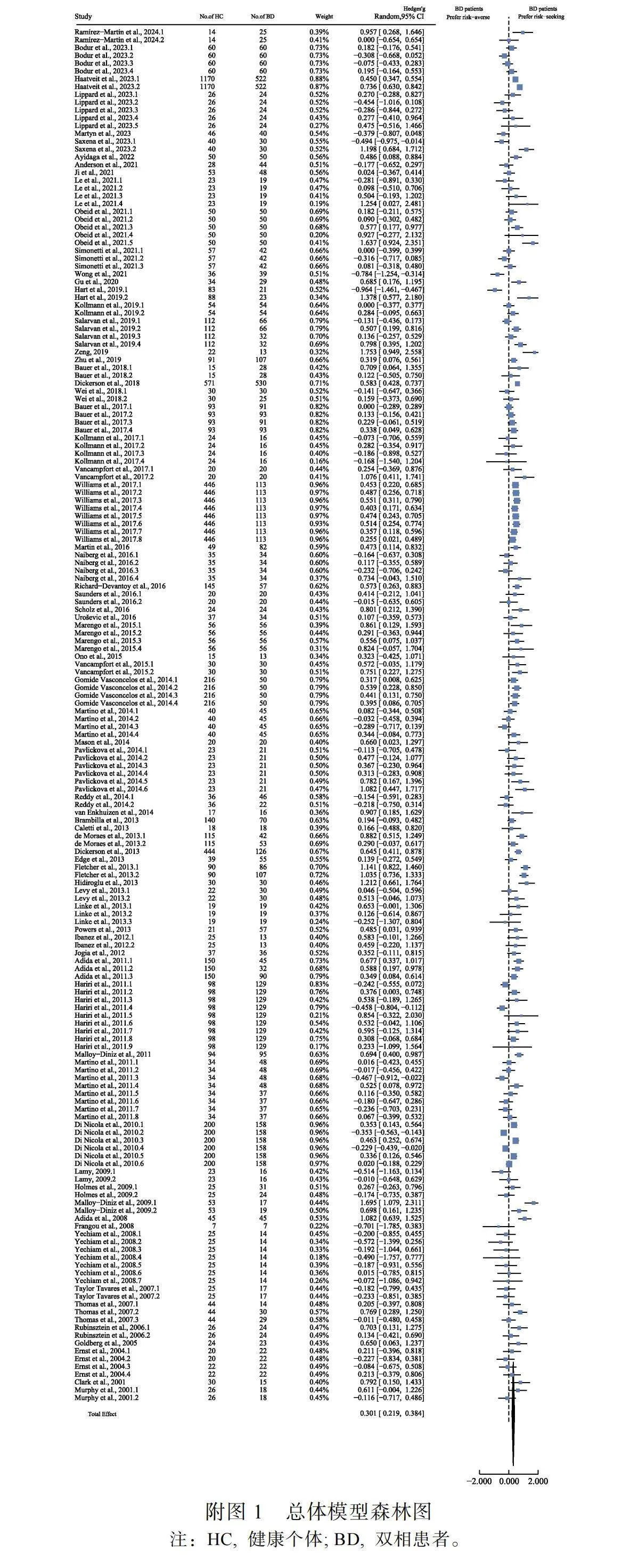
三水平随机模型比较了双相患者与健康个体在所有风险决策测量类型中的风险偏好是否存在显著差异。结果发现(见网络版附图1), 总体效应量显著(k = 176, Hedges' g"= 0.301, 95% CI [0.219, 0.384], t"= 7.21, p"lt; 0.001), 表明双相患者(N"= 4574, Mage"= 36.43岁, 60.85%女性)比健康个体(N"= 5965, Mage"= 35.63岁; 53.47%女性)更偏好风险寻求。
3.2.2""异质性检验
对所有风险决策指标进行异质性检验。结果表明, 总体模型均存在高异质性(QE"(175) = 684.33, p"lt; 0.001, I2"= 77.25%)。进一步分析发现, 研究内方差(LRT = 75.98, p"lt; 0.001)和研究间方差(LRT = 9.20, p"= 0.002) 均显著。在其总方差来源中, 抽样方差、研究内方差和研究间方差分别为22.75%, 44.65%和32.60%。因此, 非常必要进一步分析调节变量以探究双相障碍与风险决策的关系。
3.2.3 "发表偏差检验
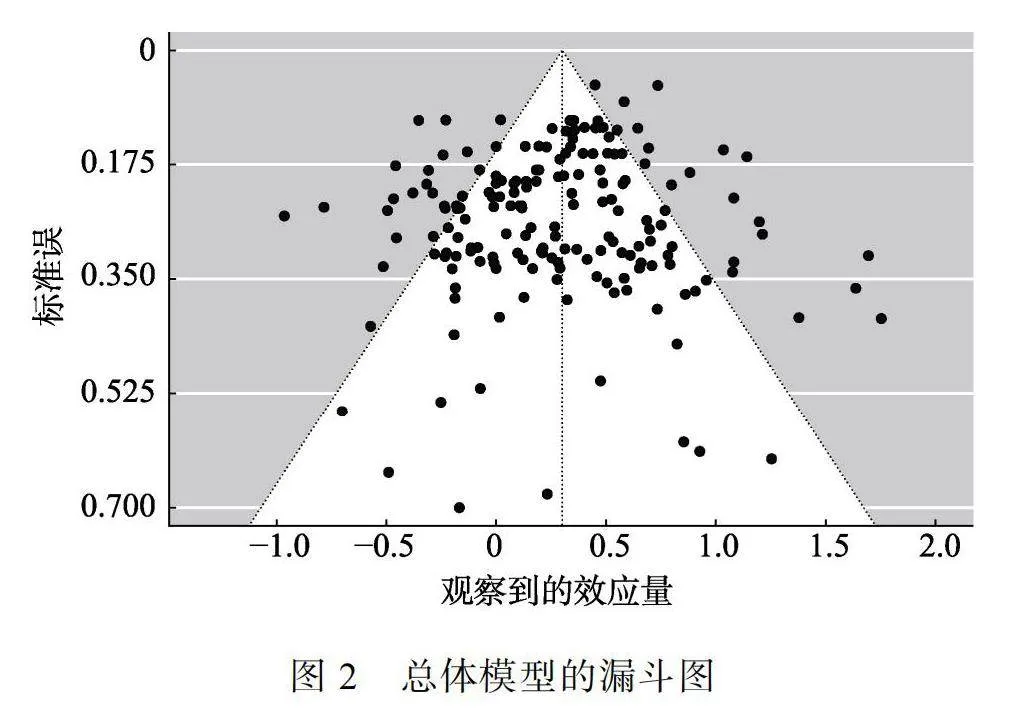
本研究采用漏斗图和Egger-MLMA回归以检验发表偏差。结果发现, 在漏斗图上的每个效应量基本均匀分布在总体效应量两侧(见图2), 且Egger-"MLMA回归结果也不显著(t"= 1.64, p"= 0.102)。由此说明当前模型没有显著的发表偏差, 继而本研究无需采用剪补法进行校正。
3.2.4""调节效应检验
考虑到样本具有高异质性, 本研究从样本特征和测量特征两方面选择潜在的调节变量。样本特征包含年龄、性别比、受教育程度、所属地区和患者所处心境阶段, 而测量特征则包含风险偏好测量类型、领域类型、行为实验任务类型和任务明确性。同时, 研究还将进一步进行亚组分析得到各分类调节变量中各组的主效应和组间差异。
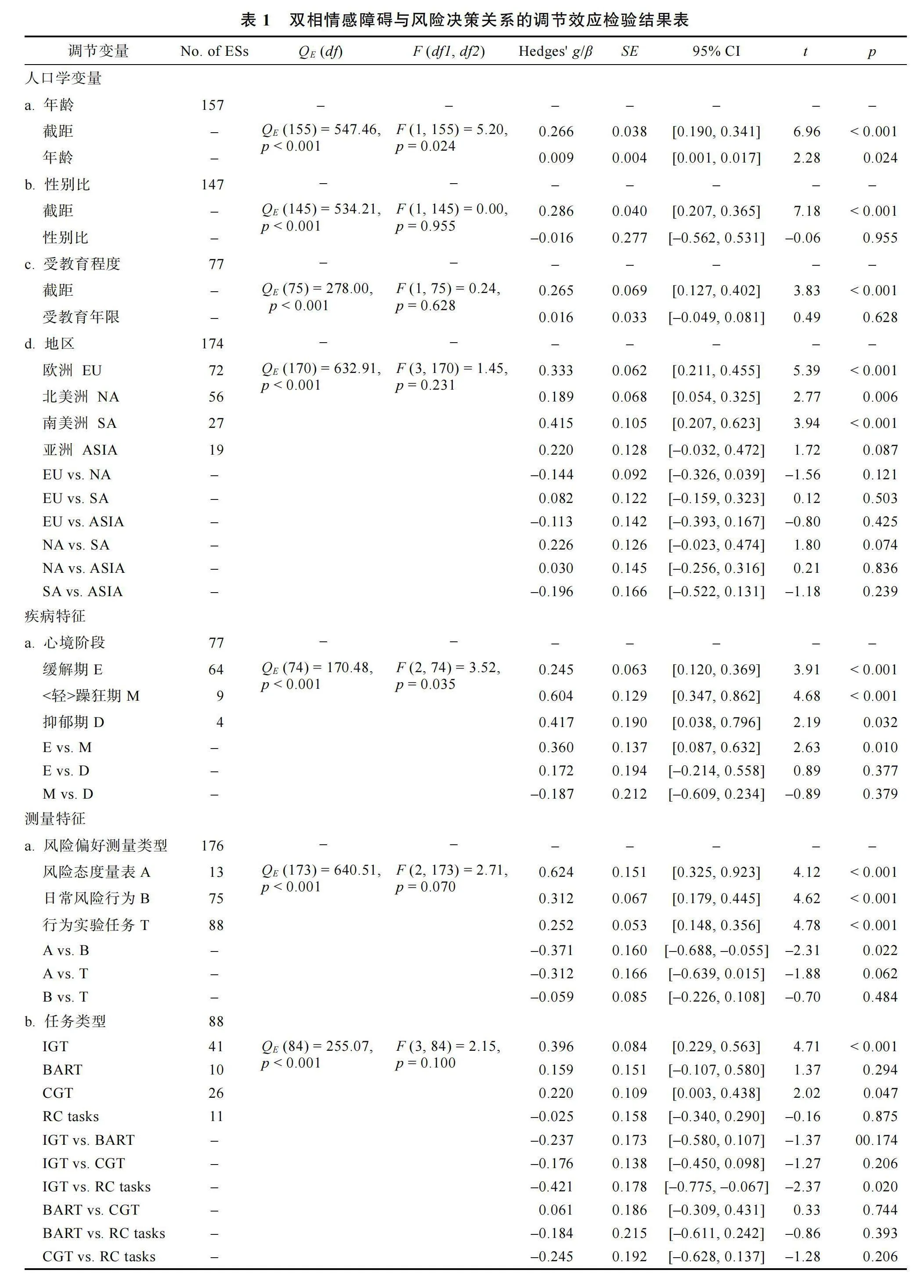
调节效应检验结果见表1。就样本特征而言, 年龄的调节作用显著(β"= 0.009, p"= 0.024), 即随年龄增大, 双相患者比健康个体偏好风险寻求的程度增加。心境阶段的调节作用显著(p"= 0.035), 以缓解期(Hedges' g = 0.245, p lt; 0.001)、lt;轻gt;躁狂期(Hedges' g = 0.604, p lt; 0.001)和抑郁期患者(Hedges' g = 0.417, p lt; 0.001)为样本的效应量均显著, 即不论心境阶段如何, 患者均比健康个体更偏好风险寻求。其中, lt;轻gt;躁狂期的效应量显著大于缓解期(β"= 0.360, p = 0.010)。虽然其他样本特征的调节作用不显著, 但在地区中部分亚组的效应量显著。除了亚洲的效应量不显著外(Hedges' g = 0.220, p = 0.087), 其余地区效应量均显著(欧洲: Hedges' g"= 0.333, p lt; 0.001; 北美洲: Hedges' g = 0.189, p = 0.006; 南美洲: Hedges' g = 0.415, p lt; 0.001)。
就测量特征而言, 本研究未发现风险偏好测量类型显著的调节作用(p"= 0.070)。不论采用风险态度量表(Hedges' g = 0.624, p lt;"0.001)、日常风险行为(Hedges' g = 0.312, p lt; 0.001)还是行为实验任务(Hedges' g = 0.252, p lt; 0.001)的效应量都显著。其中, 行为实验任务与风险态度量表的效应量间存在显著差异(β"= 0.371, p = 0.022), 其余效应量间差异不显著。因此, 采用不同风险偏好测量类型探究双相障碍与风险决策的关系时, 研究结果方向一致, 都表现为双相患者比健康个体更偏好风险寻求, 但具体差异程度有所不同。风险态度量表效应量最大, 而行为实验任务效应量最小。
在行为实验任务中, 虽然研究未发现任务类型显著的调节作用(p"= 0.100), 但采用IGT (Hedges' g"= 0.396, p lt; 0.001)和CGT任务(Hedges' g = 0.220, p = 0.047)的效应量显著, 即患者在这2个任务中均比健康个体更偏好风险寻求, 且IGT任务的效应量显著大于RC 任务(β"= 0.421, p = 0.020)。此外, 本研究还发现在隐性任务时, 患者也比健康个体更偏
好风险寻求(Hedges' g = 0.343, p lt; 0.001)。
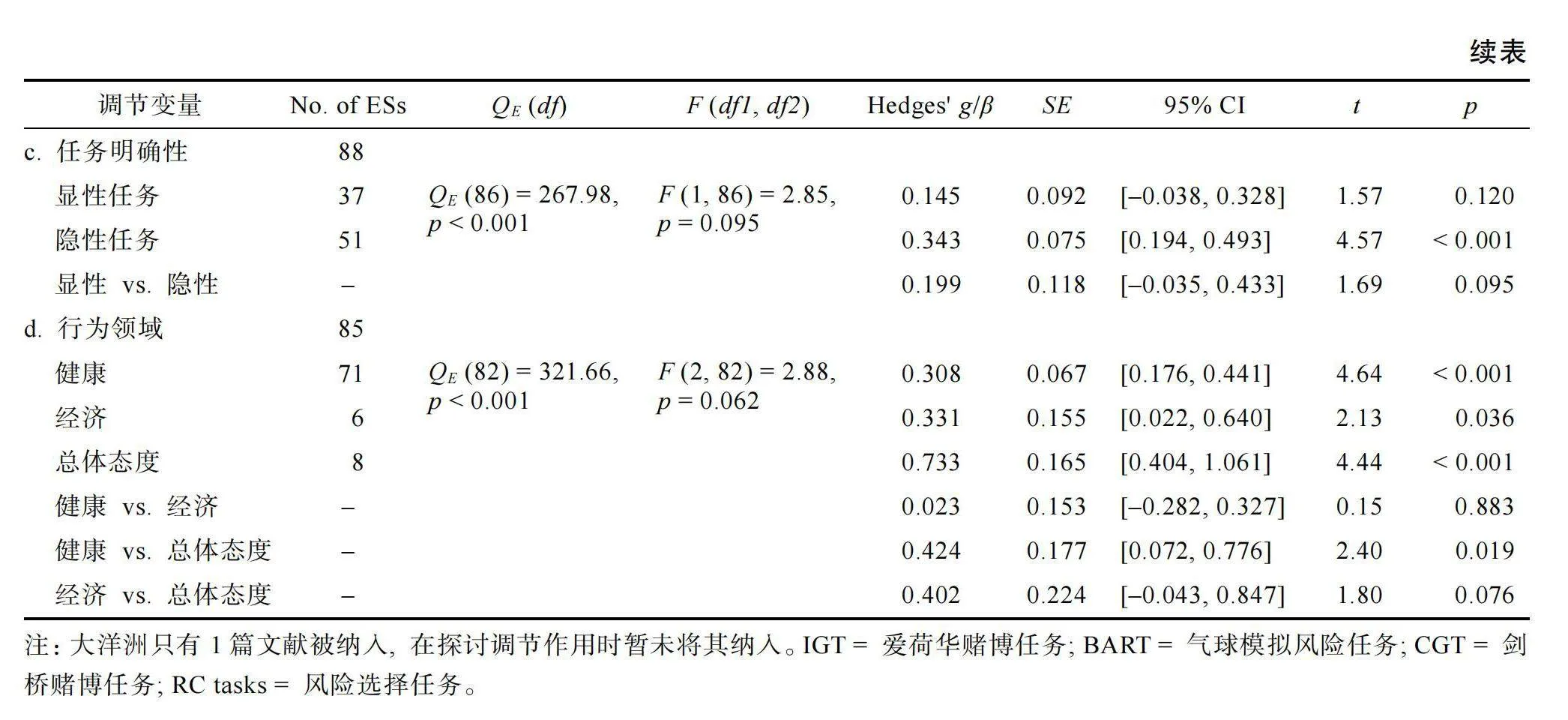
在日常态度和行为中, 本研究包含健康和经济领域的态度和行为以及总体态度。结果发现, 领域类型的调节作用不显著(p"= 0.062), 但在健康领域(Hedges' g = 0.308, p"lt; 0.001)、经济领域(Hedges' g"= 0.331, p = 0.036)和总体态度(Hedges' g = 0.733, p"lt; 0.001)中, 双相患者的风险寻求程度均显著高于健康个体。其中, 总体态度和健康领域间的效应量差异显著(β"= 0.424, p = 0.019)。
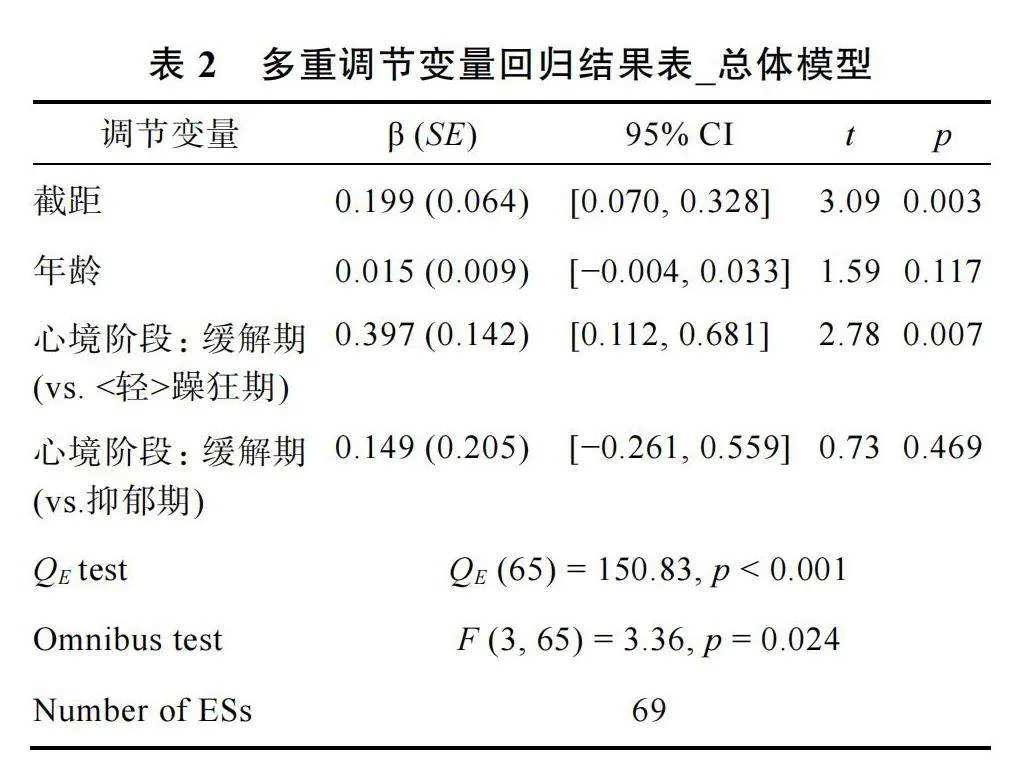
为了排除调节变量间的共线性, 根据Assink和Wibbelink (2016)的方法, 本研究纳入所有显著的调节变量(年龄和心境阶段lt;缓解期为参照gt;)进行回归分析。结果表明, 至少一个调节变量的回归系数与0有显著差异(见表2), 年龄的效应变得不显著(β"= 0.015, p = 0.117), 缓解期患者与lt;轻gt;躁狂期患者的效应量差异依然显著(β"= 0.397, p ="0.0007)。
3.3""子模型
尽管本研究发现患者在所有风险偏好测量类型上均比健康个体更偏好风险寻求, 但每种测量类型的效应量大小不同, 尤其是行为实验任务和风险态度量表的差异显著(β"= 0.371, p = 0.022)。因此, 本研究区分测量类型形成2个子模型再次检验, 包括行为实验任务模型和日常态度和行为模型, 其中后者包括风险态度量表和日常风险行为的研究。本研究将这两种类型进行合并的原因, 一是这2种测量主要以量表或问卷形式进行, 测量形式上较接近, 两者效应量在本研究中也无显著差异, 且以往研究表明这两种测量类型的相关较高(Frey et al., 2017); 二是本研究中纳入风险态度量表的文献仅5篇, 将其单独分为一个子模型, 可能会影响结论的稳健性。
3.3.1""行为实验任务模型
首先, 三水平随机模型比较双相患者与健康个体在行为实验任务中的风险偏好有无显著差异。结果发现, 总体效应量显著(k"= 88, Hedges' g"= 0.266, 95% CI [0.145, 0.387], t"= 4.36, p"lt; 0.001), 表明双相患者(N"= 2161, Mage"= 36.33岁, 58.75%女性)比健康个体(N"= 2312; Mage"= 34.22岁, 53.84%女性)在行为实验任务中也更偏好风险寻求。
其次, 对行为实验任务测得的风险决策这一结果变量进行异质性检验。结果表明该模型同样存在高异质性(QE"(87) = 284.79, p"lt; 0.001, I2"= 74.94%)。后续分析发现, 行为实验任务模型的研究内方差(LRT = 8.82, p"= 0.003)和研究间方差(LRT = 6.45, p"= 0.011)显著。在其总方差来源中, 抽样方差、研究内方差和研究间方差分别为25.06%, 25.56%和49.38%。
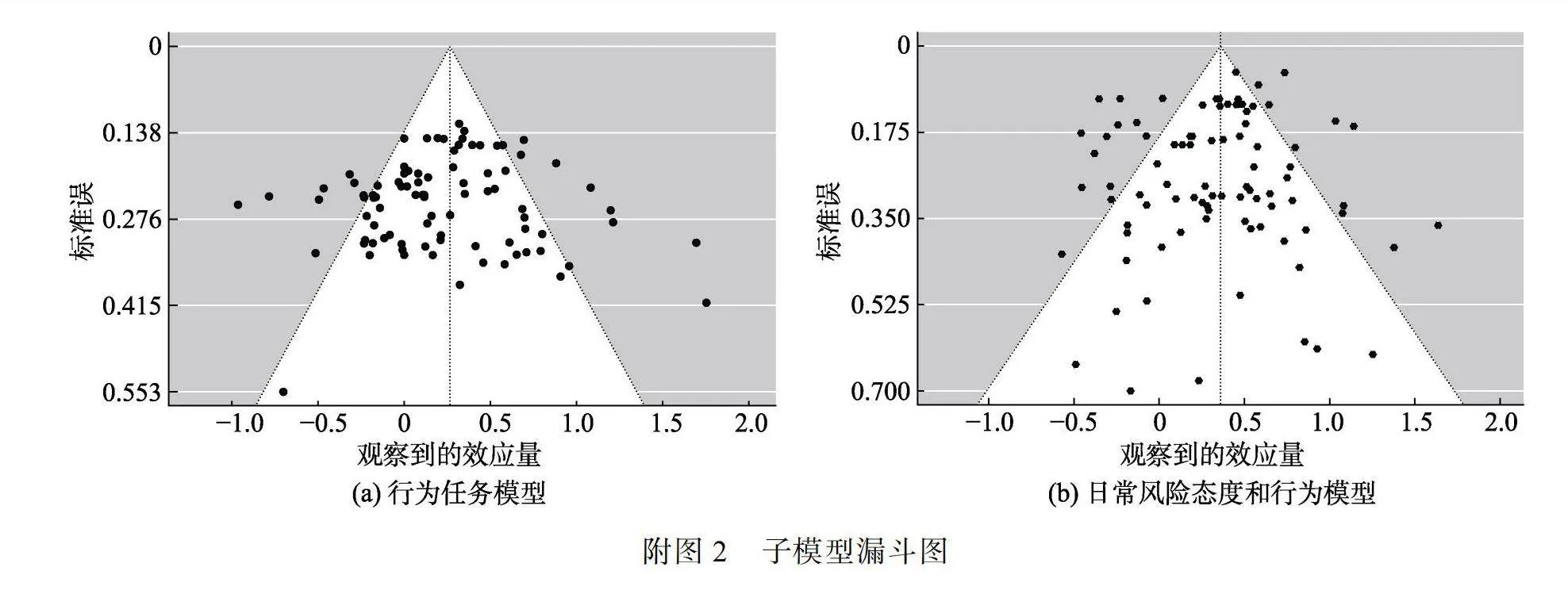
然后, 本研究采用漏斗图和Egger-MLMA回归检验发表偏差。结果发现, 采用行为实验任务的研究每个效应量在漏斗图上基本均匀分布在总体效应量的两侧(见网络版附图2a), 且Egger-MLMA回归结果也并不显著(t"= 0.63, p"= 0.531), 表明该模型不存在显著的发表偏差。
最后, 除了上文检验的任务类型和任务明确性, 本研究在行为实验任务中再次检验样本特征的调节作用(见表3)。结果发现, 年龄的调节作用显著(β"= 0.012, p"= 0.014), 即随着年龄增大, 双相患者比健康个体在行为实验任务中的风险寻求程度有所增加。地区的调节作用显著, 欧洲(Hedges' g = 0.419, p lt; 0.001)和南美洲(Hedges' g = 0.420, p = 0.002)的效应量显著, 且都显著大于北美洲的效应量(欧洲: β"= 0.377, p = 0.007; 南美洲: β"= 0.379, p"= 0.020)。虽然未有其他样本特征的显著作用, 但不同心境阶段的主效应均显著, 即缓解期(Hedges' g = 0.291, p lt; 0.001)、lt;轻gt;躁狂期(Hedges' g"= 0.553, p lt; 0.001)和抑郁期患者(Hedges' g"= 0.479, p = 0.043)均比健康个体更偏好风险寻求。
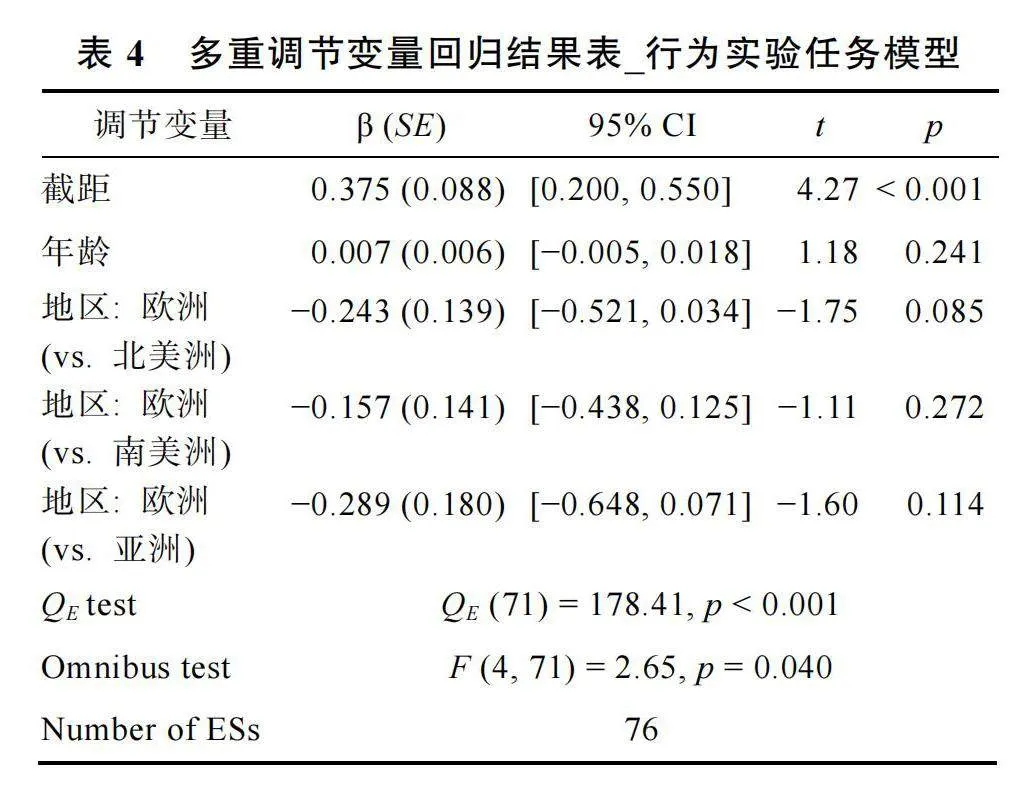
为了排除调节变量间的共线性, 根据Assink和Wibbelink (2016)的方法, 本研究纳入所有显著的调节变量(年龄和地区lt;欧洲为参照gt;)进行回归分析。虽然Omnibus检验结果显著, 但除了截距外并未有其他回归系数显著(见表4), 仅欧洲和北美洲的效应量有差异趋势(β"= −0.243, p = 0.085)。
3.3.2""日常风险态度和行为模型
首先, 三水平随机模型比较双相患者与健康个体在日常态度和行为中的风险偏好有无显著差异。结果发现, 总体效应量同样显著(k"= 88, Hedges' g"= 0.360, 95% CI [0.232, 0.487], t"= 5.60, p"lt; 0.001), 表明双相患者(N"= 2537, Mage"= 36.82岁, 62.41%女性)比健康个体(N"= 3815; Mage"= 36.39岁, 53.44%女性)在日常态度和行为中也同样更偏好风险寻求。
其次, 对日常态度和行为测得的风险决策这一结果变量进行异质性检验。结果表明该模型同样存在高异质性(QE"(87) = 378.16, p"lt; 0.001, I2"= 80.00%)。后续发现, 日常态度和行为模型的研究内方差(LRT = 57.32, p"lt; 0.001)和研究间方差(LRT = 6.77, p"= 0.009)显著。在其总方差来源中, 抽样方差、研究内方差和研究间方差分别为20.00%, 41.71 %和38.29%。
然后, 本研究采用漏斗图和Egger-MLMA回归检验发表偏差。结果发现, 采用日常态度和行为的研究每个效应量在漏斗图上基本均匀分布在总体效应量的两侧(见网络版附图2b), 且Egger-MLMA回归结果也不显著(t"= 1.54, p"= 0.126), 表明该模型不存在显著的发表偏差。
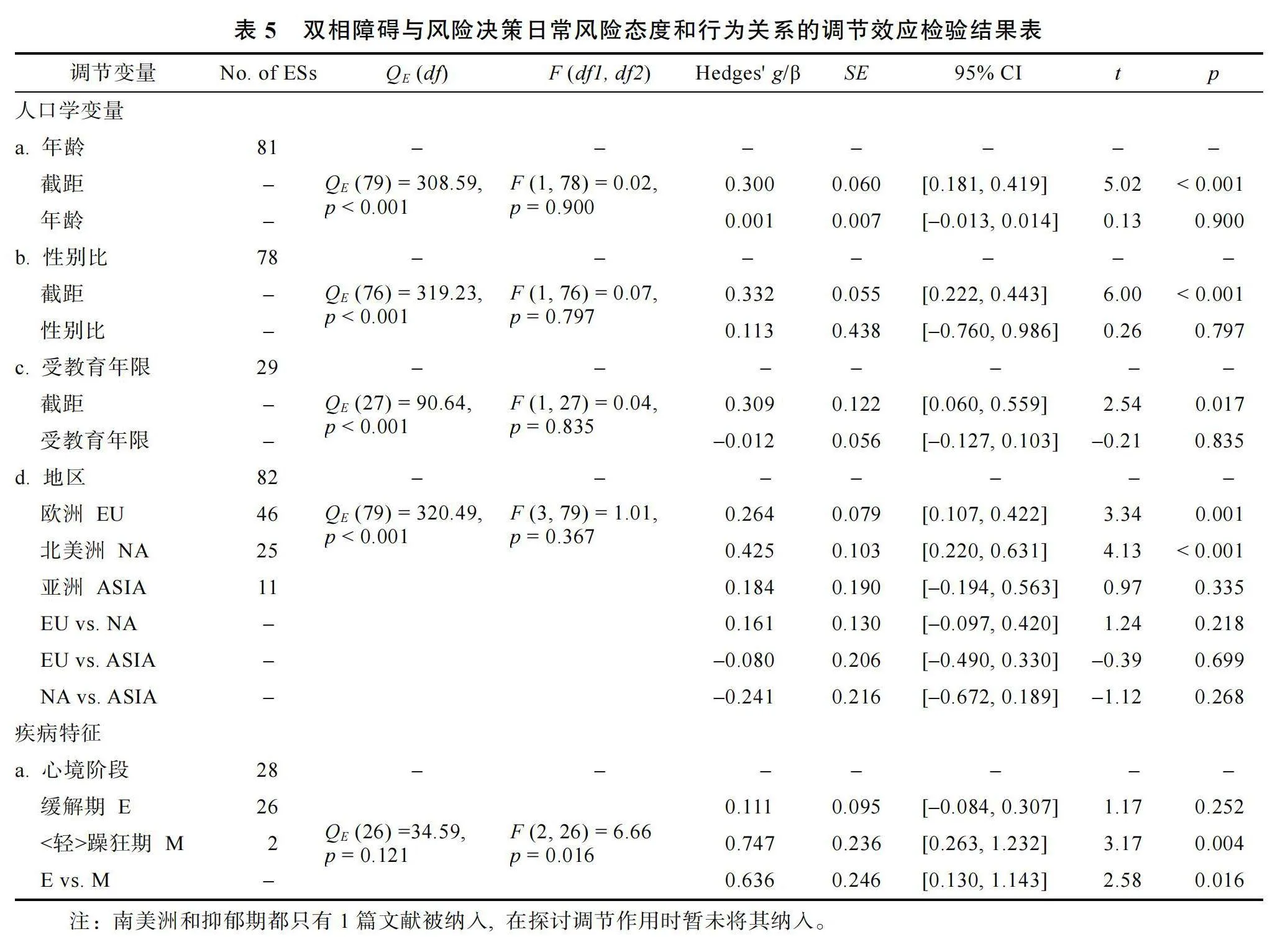
最后, 除了上文已检验的领域类型, 本研究在日常态度和行为中再次检验样本特征的调节作用(见表5)。结果仅心境阶段的调节作用显著(p"= 0.016), lt;轻gt;躁狂期患者(Hedges' g = 0.747, p = 0.004)在日常态度和行为中比健康个体更偏好风险寻求, 且其效应量显著大于缓解期患者(β"= 0.636,p = 0.016)。虽然其他样本特征的作用不显著, 但在地区中部分亚组的主效应显著, 即以欧洲个体(Hedges' g = 0.264, p = 0.001)和北美洲个体(Hedges' g = 0.425, p lt; 0.001)为样本的效应量显著。由于日常态度和行为模型中仅心境阶段的调节作用显著, 继而无需进行多调节变量回归分析。
4 "讨论
双相患者在生活中确实容易做出许多风险行为, 如风险性行为、过度消费等(如Bodur et al., 2023; Di Nicola et al., 2010)。DSM-V也将“参与有灾难性后果的高风险活动”纳入lt;轻gt;躁狂期的诊断标准中。大量实证研究发现, 双相障碍和风险决策有关(如Adida et al., 2008; Fletcher et al., 2013; Gu et al., 2020; Ramírez-Martín et al., 2024)。但因研究设计的不同(如, 采用不同风险偏好测量类型, 选取不同心境阶段患者等), 研究结果有所差异。那么, 双相障碍如何影响风险决策偏好(风险寻求还是风险规避)尚不明确。因此, 本研究采用三水平元分析, 囊括风险态度量表、行为实验任务、日常风险行为等研究类型, 对双相障碍与风险决策的关系进行系统梳理, 并发现一些有价值的结果。
4.1""双相障碍与风险决策偏好的关系
研究发现, 双相患者比健康个体更偏好风险寻求(Hedges' g"= 0.301), 该结果与Edge等人(2013)、Richard-Devantoy等人(2016)以及Ramírez-Martín等人(2020)中IGT任务的元分析结果一致, 也与大多实证研究结果相同(如Malloy-Diniz et al., 2011; Mason et al., 2014), 这回答了本研究第一个问题, 即“双相患者与健康个体的风险偏好有无差异”。研究者基于模糊痕迹理论(Fuzzy-Trace Theory, FTT; Brainerd amp; Reyna, 1990)推测双相患者风险寻求增加可能有2种途径(Lukacs et al., 2021):一是患者在强烈情绪影响下可能改变其对信息的加工方式(Rivers et al., 2008), 变得不再像健康个体那样倾向于要义加工(Gist processing), 而是过度依赖字面加工(Verbatim processing)。这可能使得他们对风险和价值的感知发生变化, 最终改变其风险偏好(Reyna et al., 2015); 二是患者依然依赖要义加工但可能赋予事件不恰当的要义, 潜在创造一个“预加载反应” (Pre-load response), 使其未来面对同一决策时再次做出不恰当反应(如, 躁狂期患者易赋予风险行为积极要义和“风险寻求”反应)。然而, 目前仅Sicilia等(2020)发现双相患者的要义加工偏好下降, 但尚无研究直接验证上述推论是否成立, 因此仍需未来进一步研究来检验。
4.2""双相障碍与风险决策关系的调节因素
本研究考察了样本特征和测量特征对双相障碍与风险决策关系的调节作用, 尝试回答了本研究第二个问题, 即潜在因素如何调节双相障碍与风险决策偏好的关系。
4.2.1 "人口学特征的调节作用
本研究发现年龄的调节作用显著, 即随着年龄增长, 双相患者与健康个体的风险寻求差异随之增加。然而, 这一正向作用仅在行为实验任务中显著, 在日常态度和行为中不显著。我们推测这可能与行为实验任务除了反映风险偏好外还涉及认知能力有关。例如, IGT任务与个体的工作记忆、策略学习等认知能力有关(蔡厚德 等, 2012; 徐四华 等, 2013)。当个体随年龄增长, 他们的认知能力往往缓慢下降(Hartshorne amp; Germine, 2015), 变得更难以正确感知风险和奖赏, 也更难以识别和优化决策策略, 因而呈现出风险寻求增加的趋势。有研究表明, 双相障碍会损伤双相患者的认知能力(Sparding et"al., 2015), 甚至会加剧认知能力的衰退(Cullen et"al., 2016; da Silva et al., 2013; Diniz et al., 2017), 尤其是老年人群(John et al., 2019)。那么, 双相患者与健康个体的认知能力差异便可能随着年龄增大, 导致两者在行为实验任务中的风险偏好差异也随之增大。
本研究在总体模型中并未发现地区的调节作用, 但无论地区如何, 患者都表现出比健康个体更高风险寻求的趋势(欧洲: Hedges' g"= 0.333; 北美洲: Hedges' g"= 0.189; 南美洲: Hedges' g"= 0.415; 亚洲: Hedges' g"= 0.220, p"=.087)。然而, 细分测量类型后结果有所差异。在行为实验任务中, 地区的调节作用显著, 欧洲和南美洲的效应量显著且显著大于北美洲, 而北美洲和亚洲的效应量不显著; 在日常态度和行为中, 地区的调节作用不显著, 但欧美的效应量显著而亚洲的效应量不显著。对于亚洲研究, 或许因研究数量不足(48篇行为任务研究中7篇亚洲研究, 27篇日常态度和行为研究中2篇亚洲研究)削弱了统计检验力(42.70%和10.90%), 掩盖了亚洲患者与亚洲健康个体的风险偏好差异。随着未来亚洲研究的积累, 其统计检验力有望提升, 结果可能有所变化。对于北美洲在行为实验任务研究中的效应量不显著, 尽管其统计检验力也较低(8.18%), 但现有趋势表明, 增加研究可能不足以改变结果, 因此我们推测这可能与行为实验任务选用有关。不同地区选用任务类型不同(χ2(9, N"= 48) = 25.40, p"= 0.003)。相较欧洲研究多采用IGT和CGT任务、南美洲研究都采用IGT任务, 北美洲研究选用任务更平衡。加之, 不同任务的效应量不同。据此, 北美洲效应量不显著或许与不同任务融合有关, 这表明未来需积累不同地区的研究并均衡选用任务, 才能更准确分析地区的作用。
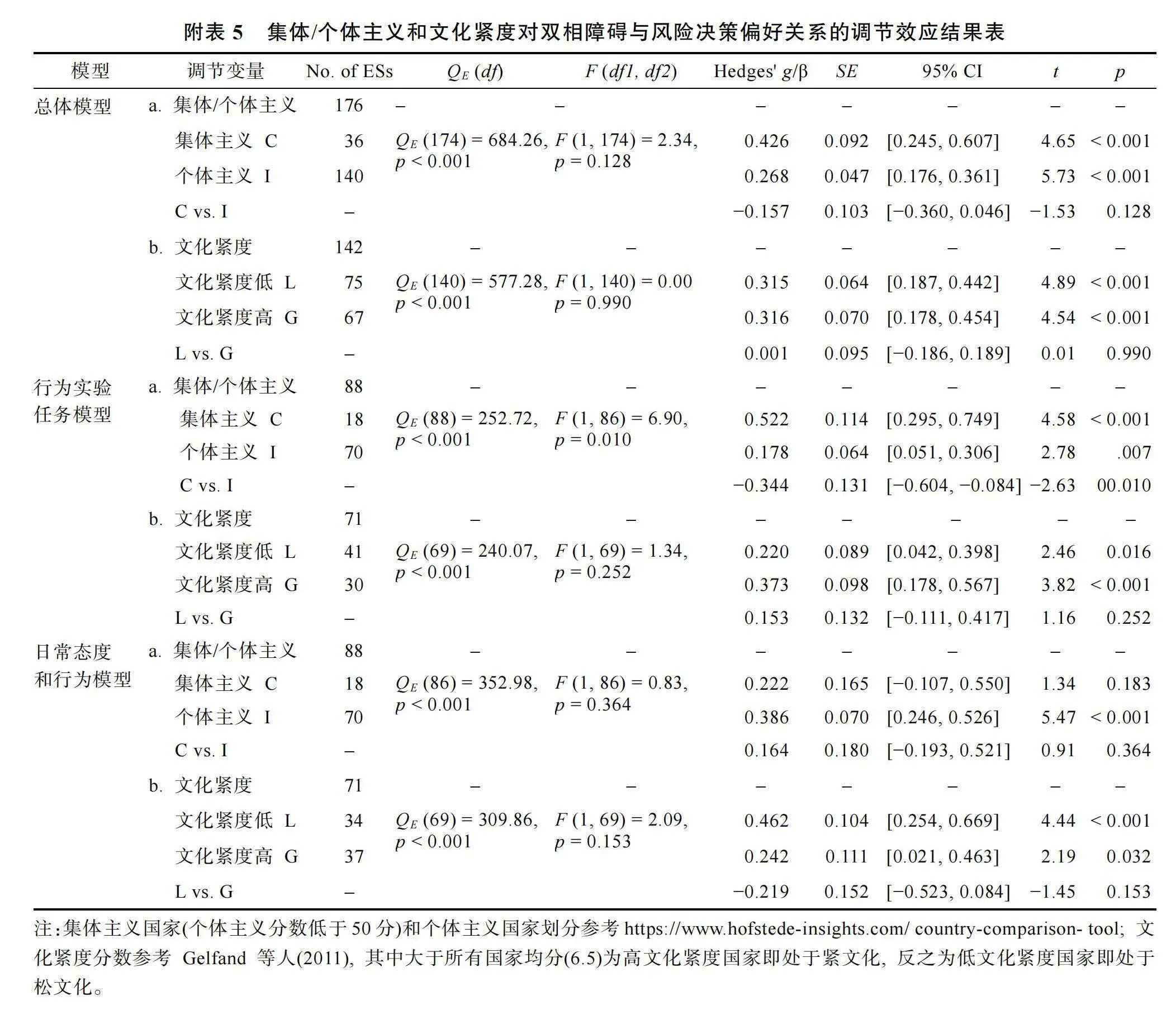
上述地区差异深层次上可能与文化差异有关。一方面, 当前研究主要涉及风险性行为、物质滥用等行为。基于文化松紧度(Gelfand et al., 2011), 相较欧美国家, 亚洲国家往往处于“紧”文化, 通常有较严格的社会规范, 对越轨行为的容忍度低、惩罚度高。因此欧美文化对风险性行为、物质滥用(尤其是大麻等毒品)等行为的接受度和常见度比亚洲文化更高(Arria et al., 2017; Bragazzi et al., 2021; Jia et al., 2018; Kandel et al., 1981)。即便是双相患者也可能存在这一文化差异。我们尝试根据文化紧度将研究所涉国家分为“高”和“低”2种类型, 然后比较2种文化下患者与健康个体的风险偏好差异是否不同。结果表明(见网络版附表5), 不论处于“紧”文化还是“松”文化的患者均比健康个体更偏好风险寻求, 但我们发现在日常态度和行为测量中, “松”文化的效应量(Hedges' g"= 0.462)确实大于“紧”文化的效应量(Hedges' g"= 0.242), 这初步验证了我们的推测, 但仍需更多研究检验。另一方面, 亚洲与欧美个体在风险偏好上可能存在固有差异。亚洲个体通常比欧美个体更偏好风险寻求(Chen et al., 2020; Du et al., 2002), 这可能与集体主义文化有关。因为集体主义文化能给个体提供强大的社会支持, 即使冒险失败也可能因他人的帮助而得到“缓冲” (Hsee amp; Weber, 1999)。因此, 不同地区健康个体的基线差异可能导致亚洲患者与亚洲健康个体间的差异变得不明显。我们将现有研究所涉国家分为“集体主义国家”和“个体主义国家”进行比较。结果发现(见网络版附表5), 在日常态度和行为中, 仅个体主义国家的效应量显著(Hedges' g"= 0.386), 这与前述研究结果相符。但在行为实验任务中却发现集体主义(Hedges' g"= 0.522)和个体主义国家(Hedges' g"= 0.178)的效应量均显著, 且集体主义国家的效应量显著更大, 这与前述研究结果不符, 值得未来进一步探索。总之, 未来需积累更多关于双相患者风险决策的地区和文化差异的研究, 更深入探究文化差异与地区效应的关系。
4.2.2""心境阶段的调节作用
本研究发现心境阶段的调节作用显著, 不论心境阶段如何, 双相患者均比健康个体更偏好风险寻求(缓解期: Hedges' g"= 0.245; lt;轻gt;躁狂期: Hedges' g"= 0.604; 抑郁期: Hedges' g"= 0.417)。区分测量类型后, 这一作用在日常态度和行为模型中显著, 而在行为实验模型中不显著。然而, lt;轻gt;躁狂期患者与缓解期患者的风险偏好差异稳定存在, 这为双相患者风险偏好变化与心境阶段有关提供证据。
值得注意的是, 不论在总体模型、行为实验任务模型还是日常态度和行为模型中, lt;轻gt;躁狂期患者均比健康个体更偏好风险寻求(总体模型: Hedges' g"= 0.604; 行为实验任务: Hedges' g"= 0.553; 日常态度和行为: Hedges' g"= 0.747)。这一发现与躁狂/轻躁狂发作的诊断标准“过度地参与那些很可能产生痛苦后果的高风险活动”相符(APA, 2013)。研究表明, 行为趋近系统会调节个体对奖励和目标的趋近行为, 往往与风险寻求有关(Braddock et al., 2011)。而lt;轻gt;躁狂期患者恰巧对这一系统异常敏感, 对趋近线索会有过度反应, 进而易表现出比健康个体更高的风险寻求程度(Katz et al., 2021)。
有趣的是, 缓解期患者虽然总体与健康个体有显著差异, 但存在于行为实验任务中(Hedges' g"= 0.291, p"lt; 0.001)而非日常态度和行为中(Hedges' g"= 0.111, p"= 0.252)。由此推测或许缓解期患者可能在生活中不再偏好风险寻求, 但其难以恢复原有水平的认知能力使其在依靠认知能力的行为实验任务中依然有与常人的差异(Mann-Wrobel et al., 2011)。这一推测也间接证明了测量类型的差异可能引发结果偏差。应指出的是, 由于对发病期患者的研究难度大, 目前研究数量还较匮乏, 基于现有研究样本得出心境阶段调节作用的结论还需审慎, 未来需积累研究以检验风险偏好跨心境变化的结论。
4.2.3""测量特征的调节作用
本研究还考察了双相障碍与风险决策偏好关系是否因测量特征不同而有所差异。首先确实发现不同风险偏好测量类型间的结果不同, 主要是风险态度量表和行为实验任务间的结果有显著差异。但稳定的是, 不论在哪种测量类型中, 双相患者均比健康个体更偏好风险寻求(风险态度量表: Hedges' g"= 0.624; 行为实验任务: Hedges' g"= 0.252; 日常风险行为: Hedges' g"= 0.312), 仅仅在程度上有所差异。这种程度差异或许不仅源于测量形式不同, 还和测量内容有关。风险态度量表将风险偏好定义为一般性风险态度或对特定领域的风险态度, 行为实验任务将风险偏好抽象为选择高风险高收益选项的倾向, 而日常风险行为则将风险偏好具象为具体风险行为的频率。这些操作定义的差异及其具体选取的指标差异都可能使得个体对备择选项或风险行为的感知发生变化(如, 风险大小、后果性质等), 最终影响其风险偏好。因此, 探索双相患者在不同测量类型上表现出差异背后的原因, 即探究双相患者风险寻求增加的潜在心理机制是未来研究的重要方向之一。
本研究在日常态度和行为上未发现领域类型的调节作用, 仅揭示总体态度(Hedges' g"= 0.733)、健康领域(Hedges' g"= 0.308)和经济领域(Hedges' g"= 0.331)的主效应显著。尽管这些效应量方向一致,"但大小差异明显, 尤其是总体态度的效应远大于其他两者。这表明双相患者可能在一般风险偏好上变化显著, 但在特定领域内的变化程度各异。这与Frey等人(2017)提出的双因子模型相符, 包括一般风险偏好的总因子和健康、经济等7个不同方面的子因子。此外, 鉴于风险决策有领域特异性(岳灵紫 等, 2018), 双相障碍对风险决策的影响可能会因领域而异。然而, 目前研究集中于健康和经济领域, 因此, 未来需积累更多双相患者在不同领域的风险决策研究进一步检验领域特异性的存在。
本研究在行为实验任务上未发现任务类型的调节作用, 仅观察到IGT和CGT任务效应量显著。这可能是由于BART和RC任务的研究数量有限(48篇行为实验任务研究中, 8篇采用BART任务, 7篇采用RC任务), 削弱了它们的统计检验力(BART: 27.80%; RC: 5.51%), 使得双相患者与健康个体的差异难以被探测。随着这些任务研究增加, 统计检验力有望提升, 研究结果可能随之改变。因此, 未来需进一步积累相关行为实验任务的研究, 以重新检验这一调节作用。
尽管本研究未直接揭示任务类型对结果的影响, 但基于对重性抑郁障碍患者风险决策的元分析, 我们对任务效应提出“操作化–机制–测量”特异性(Operationalization-Mechanism-Measure Specificity)的理论框架(见图3, Lu et al., 2024)。在此框架下, 本研究结果可能受两方面因素影响:首先是操作化特异性, 即不同行为实验任务的操作化定义涉及到风险决策构念的不同成分, 其中的独特成分可能导致任务间风险偏好的差异(Buelow amp; Blaine, 2015)。本研究中, IGT和CGT任务主效应显著, 而BART和RC任务不显著。这可能反映了这些任务涉及的风险决策构念成分有所区别, 也强调了任务选择在全面评估双相患者风险决策中的重要性。二是机制特异性, 即不同任务可能反映了双相患者受损的不同心理机制。如, RC任务可能与风险感知和价值感知有关(Chan amp; Saqib, 2021; Hosker–Field et al., 2016; Kahneman amp; Tversky, 1979); 而IGT任务除了反映风险偏好, 还涉及工作记忆、抑制控制、策略学习等认知能力(蔡厚德 等, 2012)。因此, 本研究中IGT任务的效应量显著大于RC任务, 可能预示着患者在与IGT相关的认知能力上受损, 而非风险感知和价值感知。此外, 即便任务间损伤机制相同也可能造成不同的外显行为。如, IGT任务需要个体学会识别并更多选择有利卡牌(最优策略), 若其无法识别可能更多选择不利卡牌而表现出风险寻求(徐四华 等, 2013); BART任务的最优策略要求个体在权衡风险和收益的同时适当冒险, 否则会按压次数较少即表现出风险规避(Lejuez et al., 2002)。那么, 若患者因病无法习得策略将在IGT和BART任务中表现出不同的外显行为, 继而被判定为不同的风险偏好。目前结果支持了IGT任务的推测但在BART任务中未发现显著效应。因此, 未来研究不能只关注个体的外显行为, 而要结合其背后的心理机制, 不断积累有关双相障碍影响风险决策心理机制的研究, 以厘清风险决策乃至行为实验任务和双相障碍受损机制间的关系。上述推测, 不仅值得双相患者风险偏好研究的重视, 也是所有决策研究应注意的。它提醒我们仅凭单一行为任务的结果得出风险偏好的普遍性结论并不严谨, 而应该关注跨任务范式的一致性。这也是有必要采用元分析梳理以往研究结果的重要原因之一。未来需基于多种不同行为实验任务乃至不同测量类型的结果综合判断双相患者的风险偏好, 并挖掘这背后的心理机制。
4.3""不足与展望
本研究还存在以下几点不足:(1)不同亚组的样本分布不够均衡, 本研究的部分结果可能会受一定影响。例如, 关于心境阶段的调节作用, 大多以往研究并未区分患者所处的心境阶段, 而区分的研究则多集中于缓解期患者, 躁狂和抑郁等发病期患者的研究相对匮乏。尽管这与研究难度有关, 但也不可避免地造成个别心境阶段的主效应以及各心境阶段间的效应量差异难以被探查。(2)本研究考察了人口学特征、心境阶段和测量特征的调节作用, 但受文献限制, 可能会忽略其他潜在的调节变量。例如, 服用药物情况可能是潜在调节变量。有研究发现, 服用抗精神病药物的双相患者比未服用的患者认知能力更弱(Arts et al., 2011; Torrent et al., 2011), 进而其风险偏好可能不同(Pålsson et al., 2013)。(3)鉴于目前双相障碍影响风险决策的研究侧重于揭示现象, 鲜有探究现象背后的心理机制, 因此本元分析着重梳理了主效应而未能探究其心理机制。(4)本研究尽可能全面搜索和筛选了相关文献, 但是一些数据不全的文献较难被纳入。
基于本研究发现, 我们认为未来研究可关注以下方面:
第一, 未来研究应关注双相患者风险偏好的跨心境差异。以往研究多集中缓解期患者, 缺乏对发病期患者的研究, 尤其是抑郁期。更应指出的是, 部分研究直接将双相患者与健康个体比较, 而忽略患者中混杂着不同心境, 这可能造成研究结果的偏差。如, 本研究发现lt;轻gt;躁狂期患者的风险寻求程度显著大于缓解期患者, 但若将两类患者混合与健康个体比较, 就无法明确各心境阶段的主效应, 还会产生有偏结果。而且, 即便都是缓解期患者, 其前一个心境阶段的不同(即抑郁期、lt;轻gt;躁狂期或缓解期)也可能影响当下的风险偏好。因此, 未来研究应尽可能区分患者的心境阶段, 尤其应重视对发病期患者的研究, 以进一步探索双相障碍和风险决策的跨心境差异。
第二, 未来应重视跨测量类型的研究和一致性分析。本研究虽然在不同风险偏好测量类型中都得到双相患者更偏好风险寻求的结论, 但是行为实验任务与风险态度量表的效应量差异显著, 而且不同行为实验任务下也有所差异。据此, 未来探究双相患者乃至健康个体的风险偏好时, 应重视跨任务范式和跨测量类型的差异。行为实验任务范式因能将风险决策抽象化, 并可动态测量个体风险偏好, 成为当下风险决策研究的主流方式。但是, 一些相对复杂的行为实验任务也易引入其他干扰因素。如, IGT任务中表现出的风险偏好可能涉及记忆和策略学习能力, 而BART任务中表现出的风险偏好可能涉及动机水平, 因此两者虽都自称是对风险偏好的测量, 但测得的心理本质并不完全相同, 都难以完全刻画个体的风险偏好, 与真实生活中的风险行为也有所出入。这启示了未来研究应采用多样化的测量类型, 并重视考察跨测量类型的一致性, 以得出关于双相障碍与风险决策关系更纯粹的结论, 这也有利于对潜在的心理机制挖掘。除了关注测量类型的多样性, 未来研究还要注重测量内容的广泛性。目前多数行为实验任务聚焦于经济领域的赌博任务, 而对安全、社交等决策领域的风险态度和行为鲜有关注。即便在真实风险行为的测量中, 也主要局限于健康领域的抽烟、喝酒等, 以及经济领域的赌博和消费行为等。这一局限使得现有数据难以全面揭示双相患者真实的风险决策状况。因此, 未来采用多样化测量类型时应拓展测量内容的范围, 延伸至更多决策领域。
第三, 未来研究应重视多地域样本的均衡和比较。目前双相障碍和风险决策研究多集中于欧美样本, 而双相患者的风险决策也可能存在一定地域和文化差异。如, 本研究发现欧美患者均比健康个体更偏好风险寻求, 但亚洲患者的风险偏好与健康个体却并无差异。我们还发现, 在行为实验任务的选择上, 欧洲国家多选择IGT和CGT任务, 南美洲国家全部选择IGT任务, 北美洲国家选择任务较平衡, 而亚洲国家则多选择IGT和BART任务。因此, 未来研究一方面需多积累亚洲、非洲等地区的样本, 同时也需要考虑测量类型上的多样性和均衡性。
第四, 未来研究应重视探究双相障碍影响风险决策的心理机制。目前双相障碍与风险决策间关系的研究多停留在现象揭示, 直接探究现象背后心理机制的研究相对匮乏。有研究者基于FTT理论提出, 双相患者在强烈情绪状态下既可能过度依赖字面加工, 改变其风险感知或价值感知, 进而影响其风险偏好; 也可能赋予事件不恰当要义, 使其未来面对同一决策时仍做出不恰当行为(Lukacs et al., 2021)。也有研究者认为, lt;轻gt;躁狂期患者因对行为趋近系统超敏继而比健康个体更偏好风险寻求(Katz et al., 2021)。还有研究者从动机强度(Hershenberg et al., 2016)、损失厌恶(Lasagna et al., 2022)等角度提出原因推测。但目前只有一些间接证据(如Collett, 2016; Sicilia et al., 2020)支持上述推测。因此, 未来研究有必要检验这些推测以揭示双相障碍影响风险决策的心理机制。这不仅有助于描绘患者风险决策的心理过程, 还能为干预其风险决策提供理论依据和实践指导。
最后, 未来应重视纵向追踪研究, 以弥补当前双相障碍与风险决策关系研究中依赖横断研究在因果推断上的局限。横断研究虽能揭示双相患者与健康个体在风险偏好上的差异, 但受限于个体间差异, 当样本量较小时尤其如此。而纵向追踪研究不仅能消除部分个体间差异的影响, 追踪患者风险决策随时间的变化, 构建患者风险决策的动态发展模型, 还能从被试内角度比较同一患者随心境阶段转换的风险偏好变化, 更深入地理解心境阶段的作用。因此, 未来研究应重视对双相患者队列的长期随访。
5 "结论
本研究采用三水平元分析的方法, 系统梳理以往双相障碍和风险决策研究, 得出以下主要结论:
(1)相较于健康个体, 双相患者总体上更偏好风险寻求。
(2)在样本特征上, 年龄(总体及行为实验任务模型)、地区(行为实验任务模型)和心境阶段(总体及日常态度和行为模型)起调节作用。具体而言, 双相患者随年龄增长与健康个体的风险寻求差异也随之增加; 欧洲和南美洲患者在行为实验任务中的效应量显著且显著大于北美洲患者; 所有心境阶段患者均比健康个体更偏好风险寻求, 其中lt;轻gt;躁狂期患者的效应最为稳定, 且显著大于缓解期患者。
(3)在测量特征上, 无论采用何种风险偏好测量类型, 双相患者均比健康个体更偏好风险寻求。特别是风险态度量表与行为实验任务中的差异显著。在行为实验任务中, 双相患者在IGT和CGT任务中比健康个体更偏好风险寻求, 且IGT任务效应量显著大于RC任务; 而在日常态度和行为中, 患者在健康、经济领域及总体态度上均比健康个体更偏好风险寻求, 且总体态度的效应量显著大于健康领域。
参""考""文""献
*标记为纳入元分析的文献
*Adida, M., Clark, L., Pomietto, P., Kaladjian, A., Besnier, N., Azorin, J. M., Jeanningros, R., amp; Goodwin, G. M. (2008). Lack of insight may predict impaired decision making in manic patients. Bipolar Disorders, 10(7), 829−837. https://doi.org/10.1111/j.1399-5618.2008.00618.x
*Adida, M., Jollant, F., Clark, L., Besnier, N., Guillaume, S., Kaladjian, A., ... Courtet, P. (2011). Trait-related decision-making impairment in the three phases of bipolar disorder. Biological Psychiatry, 70(4), 357–365. https://doi."org/10.1016/j.biopsych.2011.01.018
American Psychiatric Association. (2013)."Diagnostic and statistical manual of mental disorders"(5th ed.). Arlington, VA: American Psychiatric Publishing. https://doi.org/10."1176/appi.books.9780890425596
Amlung, M., Marsden, E., Holshausen, K., Morris, V., Patel, H., Vedelago, L., ... McCabe, R. E. (2019). Delay discounting as a transdiagnostic process in psychiatric disorders: A meta-analysis. JAMA Psychiatry, 76(11), 1176–1186. https://doi.org/10.1001/jamapsychiatry.2019.2102
*Anderson, Z., Fairley, K., Villanueva, C. M., Carter, R. M., amp; Gruber, J. (2021). No group differences in traditional economics measures of loss aversion and framing effects in bipolar i disorder. Plos One, 16(11), e0258360. https://"doi.org/10.1371/journal.pone.0258360
Arria, A. M., Caldeira, K. M., Allen, H. K., Bugbee, B. A., Vincent, K. B., amp; O'Grady, K. E. (2017). Prevalence and incidence of drug use among college students: An 8-year longitudinal analysis. The American Journal of Drug and Alcohol Abuse, 43(6), 711−718. https://doi.org/10.1080/"00952990.2017.1310219
Arts, B., Jabben, N. E. J. G., Krabbendam, L., amp; van Os, J. (2011). A 2-year naturalistic study on cognitive functioning in bipolar disorder. Acta Psychiatrica Scandinavica, 123(3), 190−205. https://doi.org/10.1111/j.1600-0447.2010.01601.x
Assink, M., amp; Wibbelink, C. J. M. (2016). Fitting three-level meta-analytic models in R: A step-by-step tutorial. The Quantitative Methods for Psychology, 12(3), 154–174. https://doi.org/10.20982/tqmp.12.3.p154
*Ayidaga, T., Ozel-Kizil, E.T., Çolak, B., amp; Akman-Ayidaga, E. (2022). Detailed analysis of risk-taking in association with impulsivity and aggression in euthymic patients with bipolar disorder type I. Journal of Cognitive Psychology, 34(7), 917−929. https://doi.org/10.1080/20445911.2022."2098303
Azorin, J. M., Belzeaux, R., Kaladjian, A., Adida, M., Hantouche, E., Lancrenon, S., amp; Fakra, E. (2013). Risks associated with gender differences in bipolar I disorder. Journal of Affective Disorders, 151(3), 1033–1040. https://doi.org/10.1016/j.jad.2013.08.031
*Bauer, I. E., Diniz, B. S., Meyer, T. D., Teixeira, A. L., Sanches, M., Spiker, D., Zunta-Soares, G., amp; Soares, J. C. (2018). Increased reward-oriented impulsivity in older bipolar patients: A preliminary study. Journal of Affective Disorders, 225, 585–592. https://doi.org/10.1016/j.jad.2017."08.067
*Bauer, I. E., Meyer, T. D., Sanches, M., Spiker, D., Zunta-Soares, G., amp; Soares, J. C. (2017). Are self-rated and behavioural measures of impulsivity in bipolar disorder mainly related to comorbid substance use problems? Cognitive Neuropsychiatry, 22(4), 298–314. https://doi.org/"10.1080/13546805.2017.1324951
Benazzi, F. (2003). The role of gender in depressive mixed state. Psychopathology, 36(4), 213–217. https://doi.org/"10.1159/000072792
Birmaher, B. (2013). Bipolar disorder in children and adolescents. Child and Adolescent Mental Health, 18(3), 140–148. https://doi.org/10.1111/camh.12021
Blais, A. -R., amp; Weber, E. U. (2006). A Domain-Specific Risk-Taking (DOSPERT) scale for adult populations. Judgment and Decision Making, 1(1), 33–47. https://doi."org/10.1017/s1930297500000334
Blankenstein, N. E., Peper, J. S., Crone, E. A., amp; van Duijvenvoorde, A. C. K. (2017). Neural mechanisms underlying risk and ambiguity attitudes. Journal of Cognitive Neuroscience, 29(11), 1845–1859. https://doi."org/10.1162/jocn_a_01162
*Bodur, B., Doğanavşargil Baysal, G. Ö., amp; Erdoğan, A. (2023). Comparison of behavioral addictions between euthymic bipolar disorder patients and healthy volunteers. Neuropsychiatric Investigation, 6(1), 1–5. https://doi.org/"10.5152/NeuropsychiatricInvest.2023.22028
Bolton, S., Warner, J., Harriss, E., Geddes, J., amp; Saunders, K. E. A. (2021). Bipolar disorder: Trimodal age-at-onset distribution. Bipolar Disorders, 23(4), 341–356. https://doi."org/10.1111/bdi.13016
Bora, E., Yucel, M., amp; Pantelis, C. (2009). Cognitive endophenotypes of bipolar disorder: A meta-analysis of neuropsychological deficits in euthymic patients and their first-degree relatives. Journal of Affective Disorders, 113(1-2), 1–20. https://doi.org/10.1016/j.jad.2008.06.009
Braddock, K. H., Dillard, J. P., Voigt, D. C., Stephenson, M. T., Sopory, P., amp; Anderson, J. W. (2011). Impulsivity partially mediates the relationship between BIS/BAS and risky health behaviors. Journal of Personality, 79(4), 793–810. https://doi.org/10.1111/j.1467-6494.2011.00699.x
Bragazzi, N. L., Beamish, D., Kong, J. D., amp; Wu, J. (2021). Illicit drug use in Canada and implications for suicidal behaviors, and household food insecurity: Findings from a large, nationally representative survey. International Journal of Environmental Research and Public Health, 18(12), 6425. https://doi.org/10.3390/ijerph18126425
Brainerd, C. J., amp; Reyna, V. F. (1990). Gist is the grist: Fuzzy-trace theory and the new intuitionism. Developmental Review, 10(1), 3–47. https://doi.org/10."1016/0273–2297(90)90003–M
*Brambilla, P., Perlini, C., Bellani, M., Tomelleri, L., Ferro, A., Cerruti, S., ... Frangou, S. (2013). Increased salience of gains versus decreased associative learning differentiate bipolar disorder from schizophrenia during incentive decision making. Psychological Medicine, 43(3), 571–580. https://doi.org/10.1017/S0033291712001304
Brener, N. D., Kann, L., Kinchen, S. A., Grunbaum, J. A., Whalen, L., Eaton, D., Hawkins, J., amp; Ross, J. G. (2004). Methodology of the youth risk behavior surveillance system. MMWR. Recommendations and reports: Morbidity and mortality weekly report. Recommendations and Reports, 53(RR-12), 1–13.
Buelow, M. T., amp; Blaine, A. L. (2015). The assessment of risky decision making: A factor analysis of performance on the Iowa Gambling Task, Balloon Analogue Risk Task, and Columbia Card Task. Psychological Assessment, 27(3), 777−785. https://doi.org/10.1037/a0038622
Butler, S., Rosman, A., Seleski, S., Garcia, M., Lee, S., Barnes, J., amp; Schwartz, A. (2012). A medical risk attitude subscale for DOSPERT. Judgment and Decision Making, 7(2), 189−195. https://doi.org/10.1017/s1930297500003028
Byrnes, J. P., Miller, D. C., amp; Schafer, W. D. (1999). Gender differences in risk taking: A meta-analysis. Psychological Bulletin, 125(3), 367–383. https://doi.org/10.1037/0033–"2909.125.3.367
Cai, H. D., Zhang, Q., Cai, Q., amp; Chen, Q. R. (2012). Iowa Game Task and cognitive neural mechanisms on decision-making. Advances in Psychological Science, 20(9), 1401−1410. https://doi.org/10.3724/SP.J.1042.2012.0140
[蔡厚德, 张权, 蔡琦, 陈庆荣. (2012). 爱荷华博弈任务(IGT)与决策的认知神经机制. 心理科学进展, 20(9), 1401−1410. https://doi.org/10.3724/SP.J.1042.2012.0140]
*Caletti, E., Paoli, R. A., Fiorentini, A., Cigliobianco, M., Zugno, E., Serati, M., ... Altamura, A. C. (2013). Neuropsychology, social cognition and global functioning among bipolar, schizophrenic patients and healthy controls: Preliminary data. Frontiers in Human Neuroscience, 7, 661. https://doi.org/10.3389/fnhum.2013.00661
Chan, E. Y., amp; Saqib, N. U. (2021). The moderating role of processing style in risk perceptions and risky decision making. Journal of Behavioral Decision Making, 34(2), 290–299. https://doi.org/10.1002/bdm.2210
Charness, G., amp; Gneezy, U. (2012). Strong evidence for gender differences in risk taking. Journal of Economic Behavior and Organization, 83(1), 50–58. https://doi.org/10.1016/"j.jebo.2011.06.007
Chen, X. J., Ba, L., amp; Kwak, Y. (2020). Neurocognitive underpinnings of cross-cultural differences in risky decision"making. Social Cognitive and Affective Neuroscience, 15(6),"671–680. https://doi.org/10.1093/scan/nsaa078
Cheung, M. W. L. (2014). Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychological Methods, 19(2), 211–229. https://doi.org/10.1037/a0032968
*Clark, L., Iversen, S. D., amp; Goodwin, G. M. (2001). A neuropsychological investigation of prefrontal cortex involvement in acute mania. American Journal of Psychiatry, 158(10), 1605−1611. https://doi.org/10.1176/"appi.ajp.158.10.1605
Collett, J. (2016). It's not all about that bas: Trait bipolar disorder vulnerability weakly correlated with trait bas and not predictive of risky decision–making"[Unpublished doctoral dissertation]. Swinburne University of Technology.
Croson, R., amp; Gneezy, U. (2009). Gender differences in preferences. Journal of Economic Literature, 47(2), 448–"474. https://doi.org/10.1257/jel.47.2.448
Cullen, B., Ward, J., Graham, N. A., Deary, I. J., Pell, J. P., Smith, D. J., amp; Evans, J. J. (2016). Prevalence and correlates of cognitive impairment in euthymic adults with bipolar disorder: A systematic review. Journal of Affective Disorders, 205, 165−181. https://doi.org/10.1016/j.jad."2016.06.063
da Silva, J., Gonçalves-Pereira, M., Xavier, M., amp; Mukaetova-Ladinska, E. B. (2013). Affective disorders and risk of developing dementia: Systematic review. The British Journal of Psychiatry, 202(3), 177−186. https://doi.org/10."1192/bjp.bp.111.101931
Defoe, I. N., Dubas, J. S., Figner, B., amp; van Aken, M. A. (2015). A meta–analysis on age differences in risky decision making: Adolescents versus children and adults. Psychological Bulletin, 141(1), 48–84. https://doi.org/10."1037/a0038088
Dekkers, T. J., Popma, A., van Rentergem, J. A. A., Bexkens, A., amp; Huizenga, H. M. (2016). Risky decision making in Attention-Deficit/Hyperactivity Disorder: A meta-regression"analysis. Clinical Psychology Review, 45, 1–16. https://"doi.org/10.1016/j.cpr.2016.03.001
*de Moraes, P. H. P., Neves, F. S., Vasconcelos, A. G., Lima, I. M. M., Brancaglion, M., Sedyiama, C. Y., ..."Malloy-Diniz, L. F. (2013). Relationship between neuropsychological and clinical aspects and suicide attempts in euthymic bipolar patients. Psicologia: Reflexao e Critica, 26(1), 160–167. https://doi.org/10.1590/S0102-79722013000100017
*Dickerson, F., Schroeder, J., Katsafanas, E., Khushalani, S., Origoni, A. E., Savage, C., ... Yolken, R. H. (2018). Cigarette smoking by patients with serious mental illness, 1999-2016: An increasing disparity. Psychiatric Services, 69(2), 147–153. https://doi.org/10.1176/appi.ps.201700118
*Dickerson, F., Stallings, C. R., Origoni, A. E., Vaughan, C., Khushalani, S., Schroeder, J., amp; Yolken, R. H. (2013). Cigarette smoking among persons with schizophrenia or bipolar disorder in routine clinical settings, 1999-2011. Psychiatric Services, 64(1), 44–50. https://doi.org/10.1176/"appi.ps.201200143
*Di Nicola, M., Tedeschi, D., Mazza, M., Martinotti, G., Harnic, D., Catalano, V., ... Janiri, L. (2010). Behavioural addictions in bipolar disorder patients: Role of impulsivity and personality dimensions. Journal of Affective Disorders, 125(1-3), 82–88. https://doi.org/10.1016/j.jad.2009.12.016
Diniz, B. S., Teixeira, A. L., Cao, F., Gildengers, A., Soares, J. C., Butters, M. A., amp; Reynolds III, C. F. (2017). History of bipolar disorder and the risk of dementia: A systematic review and meta-analysis. The American Journal of Geriatric Psychiatry, 25(4), 357−362. https://doi.org/10."1016/j.jagp.2016.11.014
Dir, A. L., Coskunpinar, A., amp; Cyders, M. A. (2014). A meta-analytic review of the relationship between adolescent risky sexual behavior and impulsivity across gender, age, and race. Clinical Psychology Review, 34(7), 551–562. https://doi.org/10.1016/j.cpr.2014.08.004
Du, W., Green, L., amp; Myerson, J. (2002). Cross-cultural comparisons of discounting delayed and probabilistic rewards. Psychological Record, 52(4), 479–492. https://doi."org/10.1007/BF03395199
Duffy, A. (2009). The early course of bipolar disorder in youth at familial risk. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 18(3), 200–205.
Duval, S., amp; Tweedie, R. (2000). Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56(2), 455–"463. https://doi.org/10.1111/j.0006-341X.2000.00455.x
*Edge, M. D., Johnson, S. L., Ng, T., amp; Carver, C. S. (2013). Iowa gambling task performance in euthymic bipolar I disorder: A meta-analysis and empirical study. Journal of Affective Disorders, 150(1), 115–122. https://doi.org/10."1016/j.jad.2012.11.027
*Ernst, M., Dickstein, D. P., Munson, S., Eshel, N., Pradella, A., Jazbec, S., Pine, D. S., amp; Leibenluft, E. (2004). Reward-related processes in pediatric bipolar disorder: A pilot study."Journal of Affective Disorders, 82, S89−S101. https://doi.org/10.1016/j.jad.2004.05.022
Fernandes, A. C., amp; Garcia-Marques, T. (2020). A meta-"analytical review of the familiarity temporal effect: Testing assumptions of the attentional and the fluency-attributional accounts. Psychological Bulletin, 146(3), 187–217. https://"doi.org/10.1037/bul0000222
Fischhoff, B., amp; Broomell, S. B. (2020). Judgment and decision making. Annual Review of Psychology, 71(1), 331−355. https://doi.org/10.1146/annurev-psych-010419-"050747
*Fletcher, K., Parker, G. B., amp; Manicavasagar, V. (2013). Coping profiles in bipolar disorder. Comprehensive Psychiatry, 54(8), 1177−1184. https://doi.org/10.1016/"j.comppsych.2013.05.011
*Frangou, S., Kington, J., Raymont, V., amp; Shergill, S. S. (2008). Examining ventral and dorsal prefrontal function in bipolar disorder: A functional magnetic resonance imaging study."European Psychiatry, 23(4), 300−308. https://doi."org/10.1016/j.eurpsy.2007.05.002
Frey, R., Pedroni, A., Mata, R., Rieskamp, J., amp; Hertwig, R. (2017). Risk preference shares the psychometric structure of major psychological traits. Science Advances, 3(10), e1701381. https://doi.org/10.1126/sciadv.1701381
Gao, S., Assink, M., Cipriani, A., amp; Lin, K. (2017). Associations between rejection sensitivity and mental health outcomes: A meta-analytic review. Clinical Psychology Review, 57, 59–74. https://doi.org/10.1016/"j.cpr.2017.08.007
Gelfand, M. J., Raver, J. L., Nishii, L., Leslie, L. M., Lun, J., Lim, B. C., … Yamaguchi, S. (2011). Differences between tight and loose cultures: A 33-nation study. Science, 332(6033), 1100–1104. https://doi.org/10.1126/science.1197754
*Goldberg, J. F., Wenze, S. J., Welker, T. M., Steer, R. A., amp; Beck, A. T. (2005). Content‐specificity of dysfunctional cognitions for patients with bipolar mania versus unipolar depression: A preliminary study. Bipolar Disorders, 7(1), 49−56. https://doi.org/10.1111/j.1399-5618.2004.00165.x
*Gomide Vasconcelos, A., Sergeant, J., Corrêa, H., Mattos, P., amp; Malloy-Diniz, L. (2014). When self-report diverges from performance: The usage of BIS-11 along with neuropsychological tests. Psychiatry Research, 218(1–2), 236–243. https://doi.org/10.1016/j.psychres.2014.03.002
*Gu, Y. T., Zhou, C., Yang, J., Zhang, Q., Zhu, G. H., Sun, L., Ge, M. H., amp; Wang, Y. Y. (2020). A transdiagnostic comparison of affective decision‐making in patients with schizophrenia, major depressive disorder, or bipolar disorder. PsyCh Journal, 9(2), 199−209. https://doi.org/10."1002/pchj.351
*Haatveit, B., Westlye, L. T., Vaskinn, A., Flaaten, C. B., Mohn, C., Bjella, T., ... Ueland, T. (2023). Intra- and inter-individual cognitive variability in schizophrenia and bipolar spectrum disorder: An investigation across multiple cognitive domains."Schizophrenia, 9(1), 89. https://doi.org/"10.1038/s41537-023-00414-4
*Hariri, A. G., Karadag, F., Gokalp, P., amp; Essizoglu, A. (2011). Risky sexual behavior among patients in Turkey with bipolar disorder, schizophrenia, and heroin addiction. The Journal of Sexual Medicine, 8(8), 2284−2291. https://doi."org/10.1111/j.1743-6109.2011.02282.x
*Hart, K. L., Brown, H. E., Roffman, J. L., amp; Perlis, R. H. (2019). Risk tolerance measured by probability discounting among individuals with primary mood and psychotic disorders. Neuropsychology, 33(3), 417–424. https://doi."org/10.1037/neu0000506
Hartshorne, J. K., amp; Germine, L. T. (2015). When does cognitive functioning peak? The asynchronous rise and fall of different cognitive abilities across the life span. Psychological Science, 26(4), 433–443. https://doi.org/10."1177/0956797614567339
Hershenberg, R., Satterthwaite, T. D., Daldal, A., Katchmar, N., Moore, T. M., Kable, J. W., amp; Wolf, D. H. (2016). Diminished effort on a progressive ratio task in both unipolar and bipolar depression."Journal of Affective Disorders, 196, 97–100. https://doi.org/10.1016/j.jad.2016."02.003
Hertwig, R., Barron, G., Weber, E. U., amp; Erev, I. (2004). Decisions from experience and the effect of rare events in risky choice. Psychological Science, 15(8), 534–539. https://doi.org/10.1111/j.0956-7976.2004.00715.x
*Hıdıroğlu, C., Esen, Ö. D., Tunca, Z., Yalçìn, Ş. N. G., Lombardo, L., Glahn, D. C., amp; Özerdem, A. (2013). Can risk-taking be an endophenotype for bipolar disorder? A study on patients with bipolar disorder type I and their first-degree relatives. Journal of the International Neuropsychological Society, 19(4), 474−482. https://doi."org/10.1017/S1355617713000015
*Holmes, M. K., Bearden, C. E., Barguil, M., Fonseca, M., Monkul, E. S., Nery, F. G., … Glahn, D. C. (2009). Conceptualizing impulsivity and risk taking in bipolar disorder: Importance of history of alcohol abuse. Bipolar Disorders, 11(1), 33–40. https://doi.org/10.1111/j.1399-5618."2008.00657.x
Hosker–Field, A. M., Molnar, D. S., amp; Book, A. S. (2016). Psychopathy and risk taking: Examining the role of risk perception. Personality and Individual Differences, 91, 123–132. https://doi.org/10.1016/j.paid.2015.11.059
Hox, J. J., Moerbeek, M., amp; van de Schoot, R. (2010). Multilevel analysis: Techniques and applications."Routledge.
Hsee, C., amp; Weber, E. U. (1999). Cross-national differences in risk preference and lay predictions. Journal of Behavioral Decision Making, 12(2), 165–179. https://doi.org/10.1002/"(SICI)1099-0771(199906)12:2lt;165::AID-BDM316gt;3.0.CO;2-N
Huang, Y., Wang, Y., Wang, H., Liu, Z., Yu, X., Yan, J., … Wu, Y. (2019). Prevalence of mental disorders in China: A cross-sectional epidemiological study. The Lancet Psychiatry,"6(3), 211–224. https://doi.org/10.1016/S2215-0366(18)30511-X
*Ibanez, A., Cetkovich, M., Petroni, A., Urquina, H., Baez, S., Gonzalez-Gadea, M. L., ... Manes, F. (2012). The neural basis of decision-making and reward processing in adults with euthymic bipolar disorder or attention-deficit/"hyperactivity disorder (ADHD). PloS One, 7(5), e37306. https://doi.org/10.1371/journal.pone.0037306
Isen, A. M., amp; Patrick, R. (1983). The effect of positive feelings on risk taking: When the chips are down. Organizational Behavior and Human Performance, 31(2), 194–202. https://doi.org/10.1016/0030–5073(83)90120–4
Ji, C. Y. (2007). Adolescent health risk behavior. Chinese Journal of School Health, 28(4), 289–291.
[季成叶. (2007). 青少年健康危险行为. 中国学校卫生, 28(4), 289–291.]
*Ji, S., Ma, H., Yao, M., Guo, M., Li, S., Chen, N., ... Hu, B. (2021). Aberrant temporal variability in brain regions during risk decision making in patients with bipolar I disorder: A dynamic effective connectivity study. Neuroscience, 469, 68−78. https://doi.org/10.1016/j."neuroscience.2021.06.024
Jia, Z., Jin, Y., Zhang, L., Wang, Z., amp; Lu, Z. (2018). Prevalence of drug use among students in mainland China: A systematic review and meta-analysis for 2003-2013. Drug and Alcohol Dependence, 186, 201–206. https://doi."org/10.1016/j.drugalcdep.2017.12.047
*Jogia, J., Dima, D., Kumari, V., amp; Frangou, S. (2012). Frontopolar cortical inefficiency may underpin reward and working memory dysfunction in bipolar disorder. The World Journal of Biological Psychiatry, 13(8), 605−615. https://doi.org/10.3109/15622975.2011.585662
John, A., Patel, U., Rusted, J., Richards, M., amp; Gaysina, D. (2019). Affective problems and decline in cognitive state in older adults: A systematic review and meta-analysis. Psychological Medicine, 49(3), 353–365. https://doi.org/10."1017/S0033291718001137
Johnson, E. J., amp; Tversky, A. (1983). Affect, generalization, and the perception of risk. Journal of Personality and Social Psychology, 45(1), 20–31. https://doi.org/10.1037/"0022–3514.45.1.20
Josef, A. K., Richter, D., Samanez-Larkin, G. R., Wagner, G. G., Hertwig, R., amp; Mata, R. (2016). Stability and change in risk-taking propensity across the adult life span. Journal of Personality and Social Psychology, 111(3), 430–450. https://doi.org/10.1037/pspp0000090
Kahneman, D., amp; Tversky, A. (1979). Prospect theory: An analysis of decision under risk. Econometrica, 47(2), 263–292. https://doi.org/10.2307/1914185
Kandel, D. B., Adler, I., amp; Sudit, M. (1981). The epidemiology of adolescent drug use in France and Israel. American Journal of Public Health, 71(3), 256–265. https://doi.org/10.2105/ajph.71.3.256
Kathawalla, U., amp; Syed, M. (2021). Discrimination, life stress, and mental health among Muslims: A preregistered systematic review and meta-analysis. Collabra: Psychology, 7(1), 28248. https://doi.org/10.1525/collabra.28248
Katz, B. A., Naftalovich, H., Matanky, K., amp; Yovel, I. (2021). The dual-system theory of bipolar spectrum disorders: A meta-analysis. Clinical Psychology Review, 83, 101945. https://doi.org/10.1016/j.cpr.2020.101945
Kepes, S., amp; Thomas, M. A. (2018). Assessing the robustness of meta-analytic results in information systems: Publication bias and outliers. European Journal of Information Systems, 27(1), 90−123. https://doi.org/10.1080/0960085X.2017."1390188
*Kollmann, B., Scholz, V., Linke, J., Kirsch, P., amp; Wessa, M. (2017). Reward anticipation revisited- evidence from an fMRI study in euthymic bipolar I patients and healthy first-degree relatives. Journal of Affective Disorders, 219, 178–186. https://doi.org/10.1016/j.jad.2017.04.044
*Kollmann, B., Yuen, K., Scholz, V., amp; Wessa, M. (2019). Cognitive variability in bipolar I disorder: A cluster-"analytic approach informed by resting-state data. Neuropharmacology, 156, 107585. https://doi.org/10.1016/"j.neuropharm.2019.03.028
Krantz, M., Goldstein, T., Rooks, B., Merranko, J., Liao, F., Gill, M. K., ... Birmaher, B. (2018). Sexual risk behavior among youth with bipolar disorder: Identifying demographic and clinical risk factors. Journal of the American Academy of Child and Adolescent Psychiatry, 57(2), 118–124. https://doi.org/10.1016/j.jaac.2017.11.015
*Lamy, M. (2009)."Neural correlates of impulsivity and risk taking in bipolar disorder"[Unpublished doctoral dissertation]. University of Cincinnati.
Lapomarda, G., Pappaianni, E., Siugzdaite, R., Sanfey, A. G., Rumiati, R. I., amp; Grecucci, A. (2021). Out of control: An altered parieto-occipital-cerebellar network for impulsivity in bipolar disorder. Behavioural Brain Research, 406, 113228. https://doi.org/10.1016/j.bbr.2021.113228
Lasagna, C. A., Pleskac, T. J., Burton, C. Z., McInnis, M. G., Taylor, S. F., amp; Tso, I. F. (2022). Mathematical modeling of risk-taking in bipolar disorder: Evidence of reduced behavioral consistency, with altered loss aversion specific to those with history of substance use disorder. Computational Psychiatry, 6(1), 96–116. https://doi.org/10."5334/cpsy.61
*Le, V., Kirsch, D. E., Tretyak, V., Weber, W., Strakowski, S. M., amp; Lippard, E. T. C. (2021). Recent perceived stress, amygdala reactivity to acute psychosocial stress, and alcohol and cannabis use in adolescents and young adults with bipolar disorder. Frontiers in Psychiatry, 12, 767309. https://doi.org/10.3389/fpsyt.2021.767309
Lejuez, C. W., Read, J. P., Kahler, C. W., Richards, J. B., Ramsey, S. E., Stuart, G. L., Strong, D. R., amp; Brown, R. A. (2002). Evaluation of a behavioral measure of risk taking: The Balloon Analogue Risk Task (BART). Journal of Experimental Psychology: Applied, 8(2), 75–84. https://doi."org/10.1037//1076-898x.8.2.75
*Levy, B. (2013). Autonomic nervous system arousal and cognitive functioning in bipolar disorder. Bipolar Disorders, 15(1), 70–79. https://doi.org/10.1111/bdi.12028
Lewandowski, K. E., Sperry, S. H., Malloy, M. C., amp; Forester, B. P. (2014). Age as a predictor of cognitive decline in bipolar disorder. The American Journal of Geriatric Psychiatry, 22(12), 1462–1468. https://doi.org/10.1016/j."jagp.2013.10.002
*Linke, J., King, A. V., Poupon, C., Hennerici, M. G., Gass, A., amp; Wessa, M. (2013). Impaired anatomical connectivity and related executive functions: Differentiating vulnerability and disease marker in bipolar disorder. Biological Psychiatry, 74(12), 908–916. https://doi.org/10.1016/j."biopsych.2013.04.010
*Lippard, E. T. C., Kirsch, D. E., Kosted, R., Le, V., Almeida, J. R. C., Fromme, K., amp; Strakowski, S. M. (2023). Subjective response to alcohol in young adults with bipolar disorder and recent alcohol use: A within-subject randomized placebo-controlled alcohol administration study. Psychopharmacology, 240(4), 739–753. https://doi.org/10."1007/s00213-023-06315-9
Lu, J., Zhao, X., Wei, X., amp; He, G. (2024). Risky decision-"making in major depressive disorder: A three-level meta-"analysis. International Journal of Clinical and Health Psychology, 24(1), 100417. https://doi.org/10.1016/j.ijchp."2023.100417
Lukacs, J. N., Sicilia, A. C., Jones, S., amp; Algorta, G. P. (2021). Interactions and implications of Fuzzy-trace theory for risk taking behaviors in bipolar disorder. Journal of Affective Disorders, 293, 305–313. https://doi.org/10.1016/j.jad.2021."06.035
Lüdecke, D. (2019). ESC: Effect size computation for meta analysis"(Version 0.5.1). https://CRAN.R-project.org/"package=esc.
*Malloy-Diniz, L. F., Neves, F. S., Abrantes, S. S. C., Fuentes, D., amp; Corrêa, H. (2009). Suicide behavior and neuropsychological assessment of type I bipolar patients. Journal of Affective Disorders, 112(1-3), 231−236."https://"doi.org/10.1016/j.jad.2008.03.019
*Malloy-Diniz, L. F., Neves, F. S., de Moraes, P. H. P., De Marco, L. A., Romano-Silva, M. A., Krebs, M. O., amp; Corrêa, H. (2011). The 5-HTTLPR polymorphism, impulsivity and suicide behavior in euthymic bipolar patients. Journal of Affective Disorders, 133(1-2), 221−226. https://doi.org/10.1016/j.jad.2011.03.051
Mann-Wrobel, M. C., Carreno, J. T., amp; Dickinson, D. (2011). Meta-analysis of neuropsychological functioning in euthymic bipolar disorder: An update and investigation of moderator variables. Bipolar Disorders, 13(4), 334–342. https://doi.org/10.1111/j.1399-5618.2011.00935.x
*Marengo, E., Martino, D. J., Igoa, A., Fassi, G., Scápola, M., Baamonde, M. U., amp; Strejilevich, S. A. (2015). Sexual risk behaviors among women with bipolar disorder. Psychiatry Research, 230(3), 835−838."https://doi.org/10.1016/j."psychres.2015.10.021
*Martin, K., Woo, J., Timmins, V., Collins, J., Islam, A., Newton, D., amp; Goldstein, B. I. (2016). Binge eating and emotional eating behaviors among adolescents and young adults with bipolar disorder."Journal of Affective Disorders, 195, 88–95. https://doi.org/10.1016/j.jad.2016.02.030
*Martino, D. J., amp; Strejilevich, S. A. (2014). A comparison of decision making in patients with bipolar i disorder and schizophrenia. Schizophrenia Research, 156(1), 135−136. https://doi.org/10.1016/j.schres.2014.03.019
*Martino, D. J., Strejilevich, S. A., Torralva, T., amp; Manes, F. (2011). Decision making in euthymic bipolar I and bipolar II disorders. Psychological Medicine, 41(6), 1319–1327. https://doi.org/10.1017/S0033291710001832
*Martyn, F. M., McPhilemy, G., Nabulsi, L., Quirke, J., Hallahan, B., McDonald, C., amp; Cannon, D. M. (2023). Alcohol use is associated with affective and interoceptive network alterations in bipolar disorder. Brain and Behavior, 13(1), e2832. https://doi.org/10.1002/brb3.2832
*Mason, L., O'Sullivan, N., Montaldi, D., Bentall, R. P., amp; El-Deredy, W. (2014). Decision-making and trait impulsivity in bipolar disorder are associated with reduced prefrontal regulation of striatal reward valuation. Brain, 137(8), 2346−2355. https://doi.org/10.1093/brain/awu152
Meertens, R. M., amp; Lion, R. (2008). Measuring an individual's tendency to take risks: The risk propensity scale. Journal of Applied Social Psychology, 38(6), 1506–1520. https://doi."org/10.1111/j.1559-1816.2008.00357.x
Mellers, B., Schwartz, A., amp; Ritov, I. (1999). Emotion-based choice. Journal of Experimental Psychology: General, 128(3), 332–345. https://doi.org/10.1037/0096-3445.128.3."332
Merikangas, K. R., Jin, R., He, J. P., Kessler, R. C., Lee, S., Sampson, N. A., ... Zarkov, Z. (2011). Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Archives of General Psychiatry, 68(3), 241–251. https://doi.org/10.1001/archgenpsychiatry."2011.12
Miklowitz, D. J., amp; Johnson, S. L. (2006). The psychopathology and treatment of bipolar disorder. Annual Review of Clinical Psychology, 2, 199–235. https://doi.org/"10.1146/annurev.clinpsy.2.022305.095332
Miller, J. N., amp; Black, D. W. (2020). Bipolar disorder and suicide: A review. Current Psychiatry Reports, 22(2), 6. https://doi.org/10.1007/s11920-020-1130-0
*Murphy, F. C., Rubinsztein, J. S., Michael, A., Rogers, R. D., Robbins, T. W., Paykel, E. S., amp; Sahakian, B. J. (2001). Decision-making cognition in mania and depression. Psychological Medicine, 31(4), 679−693."https://doi.org/"10.1017/s0033291701003804
*Naiberg, M. R., Newton, D. F., Collins, J. E., Bowie, C. R., amp; Goldstein, B. I. (2016). Impulsivity is associated with blood pressure and waist circumference among adolescents with bipolar disorder. Journal of Psychiatric Research, 83, 230–239. https://doi.org/10.1016/j.jpsychires.2016.08.019
National Institutes of Health. (2014). Study quality assessment tools."Retrieved from: https://www.nhlbi.nih.gov/health-"topics/study-quality-assessment-tools
*Obeid, S., Chok, A., Sacre, H., Haddad, C., Tahan, F., Ghanem, L., Azar, J., amp; Hallit, S. (2021). Are eating disorders associated with bipolar disorder type I? Results of a Lebanese case-control study. Perspectives in Psychiatric Care, 57(1), 326–334. https://doi.org/10.1111/ppc.12567
*Ono, Y., Kikuchi, M., Hirosawa, T., Hino, S., Nagasawa, T., Hashimoto, T., Munesue, T., amp; Minabe, Y. (2015). Reduced prefrontal activation during performance of the Iowa Gambling Task in patients with bipolar disorder. Psychiatry Research: Neuroimaging, 233(1), 1−8. https://doi.org/10."1016/j.pscychresns.2015.04.003
Pålsson, E., Figueras, C., Johansson, A. G., Ekman, C. J., Hultman, B., Östlind, J., amp; Landén, M. (2013). Neurocognitive function in bipolar disorder: A comparison between bipolar I and II disorder and matched controls. BMC Psychiatry, 13(1), 1−9."https://doi.org/10.1186/1471-"244X-13-165
Paluckaitė, U., amp; Žardeckaitė-Matulaitienė, K. (2017). Adolescents' perception of risky behaviour on the Internet. In Z. Bekirogullari, M. Y. Minas, amp; R. X. Thambusamy (Eds.), Health and Health Psychology - icHamp;Hpsy 2017, Vol 30. European Proceedings of Social and Behavioural Sciences"(pp. 284–292). Future Academy. https://doi.org/10."15405/epsbs.2017.09.27
*Pavlickova, H., Turnbull, O., amp; Bentall, R. P. (2014). Cognitive vulnerability to bipolar disorder in offspring of parents with bipolar disorder. British Journal of Clinical Psychology, 53(4), 386–401. https://doi.org/10.1111/bjc."12051
Plana-Ripoll, O., Weye, N., Knudsen, A. K., Hakulinen, C., Madsen, K. B., Christensen, M. K., ... McGrath, J. J. (2023). The association between mental disorders and subsequent years of working life: A Danish population-based cohort study. The Lancet Psychiatry, 10(1), 30–39. https://doi.org/"10.1016/S2215-0366(22)00376-5
Plans, L., Barrot, C., Nieto, E., Rios, J., Schulze, T. G., Papiol, S., ... Benabarre, A. (2019). Association between completed suicide and bipolar disorder: A systematic review of the literature. Journal of Affective Disorders, 242, 111–122. https://doi.org/10.1016/j.jad.2018.08.054
Pleskac, T. J. (2008). Decision making and learning while taking sequential risks. Journal of Experimental Psychology: Learning, Memory, and Cognition, 34(1), 167–185. https://doi.org/10.1037/0278-7393.34.1.167
*Powers, R. L., Russo, M., Mahon, K., Brand, J., Braga, R. J., Malhotra, A. K., amp; Burdick, K. E. (2013). Impulsivity in bipolar disorder: Relationships with neurocognitive dysfunction and substance use history. Bipolar Disorders, 15(8), 876−884. https://doi.org/10.1111/bdi.12124
Prietzel, T. T. (2020). The effect of emotion on risky decision making in the context of prospect theory: A comprehensive literature review. Management Review Quarterly, 70, 313–353. https://doi.org/10.1007/s11301–019–00169–2
Rai, S., Mishra, B. R., Sarkar, S., Praharaj, S. K., Das, S., Maiti, R., Agrawal, N., amp; Nizami, S. H. (2018). Higher impulsivity and HIV-risk taking behaviour in males with alcohol dependence compared to bipolar mania: A pilot study. Community Mental Health Journal, 54(2), 218–223. https://doi.org/10.1007/s10597-017-0139-2
Ramírez-Martín, A., Ramos-Martín, J., Mayoral-Cleries, F., Moreno-Küstner, B., amp; Guzman-Parra, J. (2020). Impulsivity, decision-making and risk-taking behaviour in bipolar disorder: A systematic review and meta-analysis. Psychological Medicine, 50(13), 2141–2153. https://doi."org/10.1017/S0033291720003086
*Ramírez-Martín, A., Sirignano, L., Streit, F., Foo, J. C., Forstner, A. J., Frank, J., ... Guzmán-Parra, J. (2024). Impulsivity, decision-making, and risk behavior in bipolar disorder and major depression from bipolar multiplex families. Brain and Behavior, 14(2), e3337. https://doi.org/"10.1002/brb3.3337
*Reddy, L. F., Lee, J., Davis, M. C., Altshuler, L., Glahn, D. C., Miklowitz, D. J., amp; Green, M. F. (2014). Impulsivity and risk taking in bipolar disorder and schizophrenia. Neuropsychopharmacology, 39(2), 456–463. https://doi.org/"10.1038/npp.2013.218
Reyna, V. F., Weldon, R. B., amp; McCormick, M. (2015). Educating intuition: Reducing risky decisions using Fuzzy-"trace theory. Current Directions in Psychological Science, 24(5), 392–398. https://doi.org/10.1177/0963721415588081
*Richard-Devantoy, S., Olié, E., Guillaume, S., amp; Courtet, P. (2016). Decision-making in unipolar or bipolar suicide attempters. Journal of Affective Disorders, 190, 128–136. https://doi.org/10.1016/j.jad.2015.10.001
Richards, J. B., Zhang, L., Mitchell, S. H., amp; de Wit, H. (1999). Delay or probability discounting in a model of impulsive behavior: Effect of alcohol. Journal of the Experimental Analysis of Behavior, 71(2), 121–143. https://doi.org/10.1901/jeab.1999.71-121
Rivers, S. E., Reyna, V. F., amp; Mills, B. (2008). Risk taking under the influence: A Fuzzy-trace theory of emotion in adolescence. Developmental Review, 28(1), 107–144. https://doi.org/10.1016/j.dr.2007.11.002
Roberts, D. K., Alderson, R. M., Betancourt, J. L., amp; Bullard, C. C. (2021). Attention-deficit/hyperactivity disorder and risk-taking: A three-level meta-analytic review of behavioral, self-report, and virtual reality metrics. Clinical Psychology Review, 87, 102039. https://doi.org/10.1016/"j.cpr.2021.102039
Rodgers, M. A., amp; Pustejovsky, J. E. (2020). Evaluating meta-analytic methods to detect selective reporting in the presence of dependent effect sizes. Psychological Methods, 26(2), 141−160. https://doi.org/10.1037/met0000300
*Rubinsztein, J. S., Michael, A., Underwood, B. R., Tempest, M., amp; Sahakian, B. J. (2006). Impaired cognition and decision-making in bipolar depression but no 'affective bias' evident. Psychological Medicine, 36(5), 629−639. https://doi.org/10.1017/S0033291705006689
*Salarvan, S., Sparding, T., Clements, C., Rydén, E., amp; Landén, M. (2019). Neuropsychological profiles of adult bipolar disorder patients with and without comorbid attention-"deficit hyperactivity disorder. International Journal of Bipolar Disorders, 7(1), 1−8. https://doi.org/10.1186/s40345-"019-0149-9
*Saunders, K. E., Goodwin, G. M., amp; Rogers, R. D. (2016). Insensitivity to the magnitude of potential gains or losses when making risky choices: Women with borderline personality disorder compared with bipolar disorder and controls. Journal of Personality Disorders, 30(4), 530−544."https://doi.org/10.1521/pedi_2015_29_216
*Saxena, K., Simonetti, A., Verrico, C. D., Janiri, D., Nicola, M. D., Catinari, A., ... Soares, J. C. (2023). Neurocognitive correlates of cerebellar volumetric alterations in youth with pediatric bipolar spectrum disorders and bipolar offspring. Current Neuropharmacology, 21(6), 1367–1378. https://doi."org/10.2174/1570159X21666221014120332
Schaffer, A., Isometsä, E. T., Tondo, L., Moreno, D. H., Turecki, G., Reis, C., ... Yatham, L. N. (2015). International society for bipolar disorders task force on suicide: Meta-analyses and meta-regression of correlates of suicide attempts and suicide deaths in bipolar disorder. Bipolar Disorders, 17(1), 1–16. https://doi.org/10.1111/bdi.12271
*Scholz, V., Houenou, J., Kollmann, B., Duclap, D., Poupon, C., amp; Wessa, M. (2016). Dysfunctional decision-making related to white matter alterations in bipolar i disorder. Journal of Affective Disorders, 194, 72–79. https://doi.org/"10.1016/j.jad.2015.12.019
Sicilia, A. C., Lukacs, J. N., Jones, S., amp; Perez Algorta, G. (2020). Decision-making and risk in bipolar disorder: A quantitative study using fuzzy trace theory. Psychology and Psychotherapy, 93(1), 105–121. https://doi.org/10.1111/"papt.12215
*Simonetti, A., Kurian, S., Saxena, J., Verrico, C. D., Soares, J. C., Sani, G., amp; Saxena, K. (2021). Cognitive correlates of impulsive aggression in youth with pediatric bipolar disorder and bipolar offspring. Journal of Affective Disorders,"287, 387–396. https://doi.org/10.1016/j.jad.2021.03.044
Sparding, T., Silander, K., Pålsson, E., Östlind, J., Sellgren, C., Ekman, C. J., ... Landén, M. (2015). Cognitive functioning in clinically stable patients with bipolar disorder I and II. PloS One, 10(1), e0115562. https://doi.org/10.1371/journal."pone.0115562
*Taylor Tavares, J. V., Clark, L., Cannon, D. M., Erickson, K., Drevets, W. C., amp; Sahakian, B. J. (2007). Distinct profiles of neurocognitive function in unmedicated unipolar depression and bipolar II depression. Biological Psychiatry, 62(8), 917–924. https://doi.org/10.1016/j.biopsych.2007.05."034
*Thomas, J., Knowles, R., Tai, S., amp; Bentall, R. P. (2007). Response styles to depressed mood in bipolar affective disorder. Journal of Affective Disorders, 100(1–3), 249–252. https://doi.org/10.1016/j.jad.2006.10.017
Tinner, L., Caldwell, D., Hickman, M., MacArthur, G. J., Gottfredson, D., Lana Perez, A., ... Campbell, R. (2018). Examining subgroup effects by socioeconomic status of public health interventions targeting multiple risk behaviour in adolescence. BMC Public Health, 18(1), 1180. https://doi.org/10.1186/s12889-018-6042-0
Torrent, C., Martinez-Arán, A., Daban, C., Amann, B., Balanzá-Martínez, V., del Mar Bonnín, C., ... Vieta, E. (2011). Effects of atypical antipsychotics on neurocognition"in euthymic bipolar patients. Comprehensive Psychiatry, 52(6), 613−622."https://doi.org/10.1016/j.comppsych.2010."12.009
*Urošević, S., Youngstrom, E. A., Collins, P., Jensen, J. B., amp; Luciana, M. (2016). Associations of age with reward delay discounting and response inhibition in adolescents with bipolar disorders. Journal of Affective Disorders, 190, 649−656."https://doi.org/10.1016/j.jad.2015.11.005
*Vancampfort, D., Hagemann, N., Wyckaert, S., Rosenbaum, S., Stubbs, B., Firth, J., ... Sienaert, P. (2017). Higher cardio-respiratory fitness is associated with increased mental and physical quality of life in people with bipolar disorder: A controlled pilot study."Psychiatry Research, 256, 219–224. https://doi.org/10.1016/j.psychres.2017.06.066
*Vancampfort, D., Sienaert, P., Wyckaert, S., De Hert, M., Stubbs, B., Soundy, A., De Smet, J., amp; Probst, M. (2015). Health-related physical fitness in patients with bipolar disorder vs. healthy controls: An exploratory study. Journal of Affective Disorders, 177, 22–27. https://doi.org/10.1016/"j.jad.2014.12.058
*van Enkhuizen, J., Henry, B. L., Minassian, A., Perry, W., Milienne-Petiot, M., Higa, K. K., Geyer, M. A., amp; Young, J. W. (2014). Reduced dopamine transporter functioning induces high-reward risk-preference consistent with bipolar disorder. Neuropsychopharmacology, 39(13), 3112–3122. https://doi.org/10.1038/npp.2014.170
Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1–48. https://doi.org/10.18637/jss.v036.i03
Wang, X. T., Zheng, R., Xuan, Y. H., Chen, J., amp; Li, S. (2016). Not all risks are created equal: A twin study and meta-analyses of risk taking across seven domains. Journal of Experimental Psychology: General, 145(11), 1548–1560. https://doi.org/10.1037/xge0000225
*Wei, G. X., Kan, B., Wu, J., amp; Wang, K. (2018). Decision-"making behavior in manic and euthymic bipolar disorder under uncertain risk conditions. Journal of Chifeng University (Natural Science Edition), 34(8), 97–101. https://doi.org/10.13398/j.cnki.issn1673-260x.2018.08.035
[魏格欣, 阚博, 吴娟, 汪凯. (2018). 躁狂期和缓解期双相情感障碍患者在风险不明确情境下决策行为的研究与探讨. 赤峰学院学报(自然科学版), 34(8), 97–101. https://doi.org/10.13398/j.cnki.issn1673-260x.2018.08.035]
*Williams, S. C., Davey-Rothwell, M. A., Tobin, K. E., amp; Latkin, C. (2017). People who inject drugs and have mood disorders—A brief assessment of health risk behaviors. Substance Use and Misuse, 52(9), 1181–1190. https://"doi.org/10.1080/10826084.2017.1302954
*Wong, S. C. Y., Ng, M. C. M., Chan, J. K. N., Luk, M. S. K., Lui, S. S. Y., Chen, E. Y. H., amp; Chang, W. C. (2021). Altered risk-taking behavior in early-stage bipolar disorder with a history of psychosis. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.763545
World Health Organization (WHO). (2022). Mental disorders."Retrieved Feb 12, 2023, from https://vizhub.healthdata."org/gbd-compare/
Xu, S. H., Fang, Z., amp; Rao, H. Y. (2013). Real or hypothetical monetary rewards modulates risk taking behavior. Acta Psychologica Sinica, 45(8), 874−886. https://doi.org/10."3724/SP.J.1041.2013.00874
[徐四华, 方卓, 饶恒毅. (2013). 真实和虚拟金钱奖赏影响风险决策行为. 心理学报, 45(8), 874−886. https://doi."org/10.3724/SP.J.1041.2013.00874]
*Yechiam, E., Hayden, E. P., Bodkins, M., O'Donnell, B. F., amp; Hetrick, W. P. (2008). Decision making in bipolar disorder: A cognitive modeling approach. Psychiatry Research, 161(2), 142–152. https://doi.org/10.1016/j.psychres.2007."07.001
Yue, L. Z., Li, S., amp; Liang, Z. Y. (2018). New avenues for the development of domain-specific nature of risky decision making. Advances in Psychological Science, 26(5), 928−"938. https://doi.org/10.3724/SP.J.1042.2018.00928
[岳灵紫, 李纾, 梁竹苑. (2018). 风险决策中的领域特异性. 心理科学进展, 26(5), 928−938. https://doi.org/10.3724/"SP.J.1042.2018.00928]
*Zeng, B. E. (2019). The relationship between college students'"suicide behavior and risk decision-making"[Unpublished master's thesis]. Southern Medical University, Guangzhou.
[曾宝尔. (2019). 大学生自杀行为与风险决策的关系研究"(硕士学位论文). 南方医科大学, 广州.]
Zhang, D. C., Highhouse, S., amp; Nye, C. D. (2019). Development and validation of the general risk propensity scale (GRiPS). Journal of Behavioral Decision Making, 32(2), 152–167. https://doi.org/10.1002/bdm.2102
Zhu. C. G. (2020). Analysis of the investment risk preference of bipolar disorder-mania patients in remission and healthy first-degree relatives (siblings) [Unpublished master's thesis]. Anhui Medical University, China.
[朱承刚. (2020). 缓解期双相躁狂患者及其健康一级亲属(同胞)投资风险偏好的研究 (硕士学位论文). 安徽医科大学.]
*Zhu, Q., Liang, W. J., Zhang, G. C., Wu, X. H., amp; Guan, N. H. (2019). Social cognition and its impact on social functioning in patients with euthymic bipolar disorder. Guangdong Medical Journal, 40(18), 2671−2677. https://"doi.org/10.13820/j.cnki.gdyx.20190901
[朱麒, 梁文靖, 张桂灿, 吴秀华, 关念红. (2019). 缓解期双相障碍患者社会认知及对社会功能的影响. 广东医学, 40(18), 2671−2677. https://doi.org/10.13820/j.cnki.gdyx."20190901]
Risky decision-making in bipolar disorder: Evidence from a three-level meta-analysis
LU Jiaqi1,2, LI Yusi1, HE Guibing1
(1"Department of Psychology and Behavioral Sciences, Zhejiang University, Hangzhou 310058,"China)(2"Jing Hengyi School of Education, Hangzhou Normal University, Hangzhou 311121, China)
Abstract
Bipolar disorder (BD), one of six major mental disorders in China, manifests as recurrent episodes of (hypo)mania and major depression. Recently, researchers have increasingly focused on the cognitive and behavioral characteristics of BD patients. Notably, increased risk-taking might emerge as a typical symptom of BD, supported by evidence from BD patients' daily behaviors, empirical research, and neuroimaging studies. However, contradictory findings have been reported, with some studies failing to find differences in risk preferences between BD patients and healthy controls (HCs) and a few studies even indicating increased risk aversion among BD patients. Consequently, whether and to what extent BD is associated with alterations in risk preference remain unclear. Thus, this study involved a three-level meta-analysis to examine the relationship between BD and risky decision-making, encompassing studies utilizing various measures of risky decision-making (i.e., risk attitude scales, behavioral tasks, and daily risk behaviors). Moreover, we aimed to uncover potential moderators, including sample and measurement characteristics, to better address inconsistent findings.
A systematic literature search"was conducted with the Web of Science, PubMed, Scopus, PsycINFO, CNKI (China National Knowledge Infrastructure), and WFD (Wan Fang Data) databases up to April 15, 2024, to identify studies investigating risky decision-making in BD patients and HCs. We calculated the standard mean differences (Hedges' g) in risky decision-making between BD patients and HCs. We conducted a three-level random-effects meta-analysis, including heterogeneity analysis, moderation analyses for sample and measurement characteristics, and assessments of publication bias.
Across 176 effect sizes in 71 cross-sectional studies, BD patients exhibited greater risk-seeking than HCs (Hedges' g"= 0.301), regardless of whether it was measured via risk attitude scales (Hedges' g"= 0.624), behavioral tasks (Hedges' g"= 0.252) or daily risk behaviors (Hedges' g"= 0.312). Moreover, this difference was also moderated by age (β"= 0.009) and mood phase, where BD patients in any mood phase preferred more risk-seeking than HCs (euthymic: Hedges' g"= 0.245; (hypo)mania: Hedges' g"= 0.604; major depression: Hedges' g"= 0.417). For behavioral tasks, age (β = 0.012) and region were found to have significant moderating effects. Specifically, significant effect sizes were observed for samples originating from Europe (Hedges' g"= 0.419) and South America (Hedges' g"= 0.420). Moreover, effect sizes were significant in studies using the Iowa Gambling Task (IGT; Hedges' g"= 0.396) and Cambridge Gambling Task (Hedges' g = 0.220), and effect sizes in IGT studies were larger than in those employing the Classic Risky Choice Tasks. Regarding. With respect to daily attitudes/behaviors, mood phase was identified as a significant moderator. Notably, effect sizes for (hypo)manic patients (Hedges' g"= 0.747) were significantly larger than those for euthymic patients. Moreover, compared with HCs, BD patients exhibited increased risk-seeking across the health (Hedges' g"= 0.308), financial (Hedges' g"= 0.331), and overall attitude (Hedges' g"= 0.733) domains.
This study comprehensively explored the relationship between BD and risky decision-making via various measures, revealing a consistent pattern of increased risk-seeking among BD patients. These findings suggest that increased risk-taking might be a noteworthy symptom of BD and propose potential utility for its application in clinical management and psychoeducation. Furthermore, future studies should consider factors such as mood phase and task type and try to uncover the underlying psychological mechanisms through which BD affects risky decision-making.
Keywords "Bipolar disorder, risky decision-making, meta-analysis, decision task, cross-mood specificity
附录新增参考文献
Bechara, A., Damasio, A. R., Damasio, H., amp; Anderson, S. W. (1994). Insensitivity to future consequences following damage to human prefrontal cortex. Cognition, 50(1-3), 7–15. https://doi.org/10.1016/0010-0277(94)90018-3
Rogers, R. D., Everitt, B. J., Baldacchino, A., Blackshaw, A. J., Swainson, R., Wynne, K., ... Robbins, T. W. (1999). Dissociable deficits in the decision-making cognition of chronic amphetamine abusers, opiate abusers, patients with focal damage to prefrontal cortex, and tryptophan-depleted normal volunteers: evidence for monoaminergic mechanisms."Neuropsychopharmacology, 20(4), 322–339. https://doi."org/10.1016/S0893-133X (98)00091-8
猜你喜欢
软科学(2017年2期)2017-04-01 21:34:31
职教论坛(2017年3期)2017-03-07 22:45:59
心理技术与应用(2016年10期)2016-12-13 14:04:37
心理与行为研究(2016年3期)2016-09-07 00:36:11
中国远程教育(2016年5期)2016-06-29 09:54:14
科教导刊·电子版(2016年15期)2016-06-25 23:44:31
会计之友(2016年8期)2016-04-20 15:13:54
心理技术与应用(2015年10期)2015-10-09 10:19:52
华南理工大学学报(社会科学版)(2015年3期)2015-08-21 14:57:03
心理与行为研究(2014年4期)2015-05-04 12:43:37