
Is the Mediterranean diet a good preventive measure for NASH?
2024-05-13 07:26AnnaCaterinaProcopioMariaRosariaParavatiGiuseppeGuidoMariaScarlataMaddalenaParafatiNatasaMiliFrancescoLuzzaLudovicoAbenavoli
Hepatoma Research 2024年2期
Anna Caterina Procopio, Maria Rosaria Paravati, Giuseppe Guido Maria Scarlata, Maddalena Parafati,Natasa Milić, Francesco Luzza, Ludovico Abenavoli
1Department of Health Sciences, University “Magna Graecia” of Catanzaro, Viale Europa, Catanzaro 88100, Italy.
2Department of Pharmacodynamics, University of Florida, 1225 Center Dr, Gainesville, FL 32610, USA.
3University of Novi Sad, Faculty of Medicine, Department of Pharmacy, Novi Sad 21000, Serbia.
Abstract Non-alcoholic steatohepatitis (NASH) is a clinical condition characterized by inflammation and swelling of the hepatocytes.If not adequately treated, NASH can lead to the development of fibrosis and liver cancer.Currently,drug therapies used in the management of NASH patients are deficient and non-specific.Patients’ adherence to a healthy lifestyle with a low-calorie diet is a crucial element in the treatment of NASH.The Mediterranean diet is a diet that, more than any other, has indicated beneficial effects in this pathology.The proposed review summarizes the evidence regarding the beneficial effects of consuming the Mediterranean diet typical foods in NASH.
Keywords: Liver diseases, polyphenols, extra virgin olive oil, onion, fish, bergamot.
INTRODUCTION
Non-alcoholic steatohepatitis (NASH) presents a pejorative form of non-alcoholic fatty liver disease(NAFLD); the main manifestations of NASH are inflammation of the liver and damage of hepatocytes[1].The development of this condition is associated with an unregulated diet, a sedentary lifestyle, and a genetic predisposition[2].The term NAFLD includes various states of the syndrome that starts from simple steatosis passing to NASH characterized by inflammation and swelling of the hepatocytes, if not adequately treated,up to fibrosis and liver carcinoma[3].NAFLD, by definition, is not caused by alcohol abuse, but many factors predispose to its onset, including the accumulation of fat in the liver.Although alcohol is not directly involved in NAFLD, great care must be taken with its intake.The World Health Organization (WHO)advises against any level of alcohol consumption[4].It is safe to say that fat accumulation in the liver alone does not induce the transition from NAFLD to NASH[5].More recently, the multiple-hit theory has been proposed, which suggests the combined action of at least two predisposing factors determining NASH[6].The early stages of this disease present with aspecific and mild symptoms, including tiredness and pain in the upper right abdomen[7].However, diagnosing this condition becomes challenging as it can only be diagnosed in advanced stages in a few cases[8].Thiazolidinediones (or glitazones) are a class of oral hypoglycemic agents used for the treatment of NASH due to their insulin-sensitizing effects.The main target of thiazolidinediones is Peroxisome Proliferator-Activated Receptor gamma (PPAR-γ), a nuclear receptor involved in several biological pathways, especially adipogenesis, glucose metabolism, and carcinogenesis[9].Indeed, glitazones exert an insulin-sensitizing action by promoting the differentiation of large insulin-resistant pre-adipocytes into small insulin-sensitive adipocytes.Furthermore, these compounds are able to induce lipogenesis, lipoprotein lipase and increase the synthesis and absorption of fatty acids in adipose tissues[10].The identification of targeted pharmacological treatments and the identification of a healthy diet present crucial elements for the management of NASH patients.In this regard, the Mediterranean diet presents the dietary approach that, more than any other, has demonstrated beneficial effects in this pathology.The Mediterranean diet was described for the first time by Ancel Keys[11].The definition of the Mediterranean diet originated from the observation of Rom, Montegiorgio,and Crevalcore (Italy) diets compared to that of North Karelian (Finland) men.Keys observed a strong correlation between the diet and cardiovascular diseases.In fact, the rural people of Central-North Italy showed better health conditions when compared with the population of New York and their own relatives,who had emigrated to the United States decades earlier.To validate this hypothesis, Keys conducted a wellknown “Seven Countries Study”[12].This project involved seven nations (Finland, Netherlands, Italy, United States, Greece, Japan, and Yugoslavia), analyzing a total of 12,000 men between 40 and 60 years of age.The data effectively indicated that a healthy lifestyle and a Mediterranean diet reduced the incidence of cardiovascular diseases (without autopsy).It is important to note a few considerations: the study was conducted in the ‘60s, the subjects observed were highly heterogeneous in terms of lifestyle and anthropometric parameters, the amount of daily alcohol consumption (mean 84 g/day) was given later, and cigarette smoke was underestimated.However, it was only assumed that olive oil consumption was high,but animal lard was most frequently used in Montegiorgio and in Crevalcore in the post-war time.Furthermore, it is necessary to clarify how fish (sardines and salted cod) were rarely consumed in the two sites and the body mass index of the men was that of the actual Japanese people.Currently, international guidelines report that the Mediterranean diet is a more effective alimentary regimen to treat patients with NAFLD[13].The Mediterranean diet is graphically presented through the use of a food pyramid,characterized by a gradually reduced consumption of the foods positioned at the top of the pyramid.In this regard, the Mediterranean diet is characterized by poorly processed seasonal foods, high consumption of plant foods such as fruit, vegetables, and cereals (not very refined), high consumption of virgin or extra virgin olive oil (EVOO), reduced consumption of dairy products and red meat, and moderate consumption of fish, poultry, and wine.Specifically, it is recommended to include a daily consumption of whole grains,bread, legumes, nuts, fruits, vegetables, and EVOO (located at the bottom of the pyramid), a weekly consumption of fish, sea foods, dairy products, eggs, poultry and yogurt (located at the central part of the pyramid), and an occasional consumption of red meat and sweets (located at the highest part of the pyramid).In this way, the total proper amount of daily calories is the most relevant focus.In addition, the second relevant aim is the use of fiber-rich food, and the third is the use of vegetal fat (olive oil), but also in controlled amounts, as it also contains many calories[14].Table 1 reports the average daily intake of Mediterranean diet foods in comparison to Western diet (WD)[15].Concerning alcohol consumption, theMediterranean diet indicates moderate consumption, about one to two glasses of red wine at each meal (10 g to < 50 g per day for men and 5 g to < 25 g per day for women)[16].As for the Western diet, there are no restrictions.Studies on alcohol consumption reported in the literature are controversial.Red wine is the main alcoholic beverage in the Mediterranean diet, and resveratrol is the major polyphenol present.Resveratrol confers cardioprotective and antioxidant effects[17,18].However, it cannot be ignored that the ethanol found in wine is a dangerous agent when abused.Studies by Farchi et al.on Italian rural cohorts from the Seven Countries have shown that there is a correlation between alcohol consumption and mortality, especially by cardiovascular events.This correlation is particularly evident in cases of excessive alcohol consumption[19,20].Currently, WHO advises against the consumption of alcohol at any dosage[21].In addition, alcohol intake is prohibited for NASH patients[22].For all these reasons, red wine was not considered in this review.Furthermore, in the two sites of Crevalcore and Montegiorgio, alongside cancer,liver cirrhosis was also found as a cause of death[12].In the years 2015-2020, the Mediterranean diet was included in the Dietary Guidelines for Americans as one of the healthiest eating models, underlining its beneficial aspects.Furthermore, in 2010, UNESCO included the Mediterranean diet in the list of the intangible cultural heritage of humanity[23].UNESCO’s decision to include the Mediterranean diet among its heritages was determined by several factors.The first among them is the possibility of raising awareness among the population towards healthier lifestyle habits, which include diet.In addition, the traditional and convivial character associated with the Mediterranean diet was taken into account[24].The proposed review summarizes the evidence regarding the beneficial effects of consuming the Mediterranean diet typical foods in NASH.
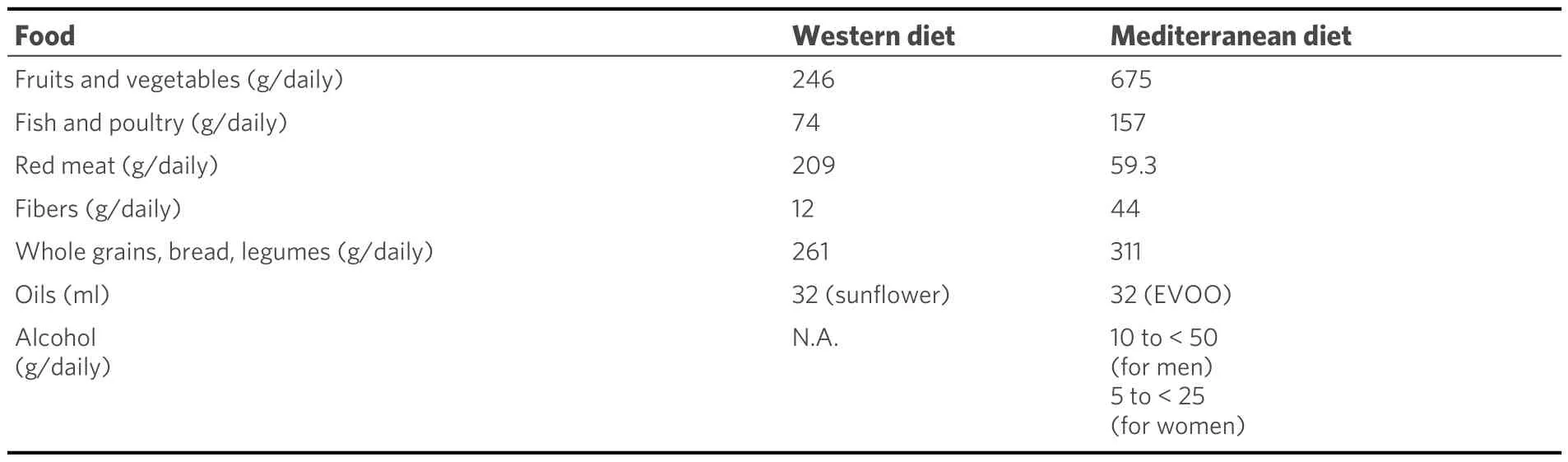
Table 1.Average daily intake of food between Mediterranean diet and Western diet
EXTRA VIRGIN OLIVE OIL
EVOO is at the base of the food pyramid in the Mediterranean diet, with a recommended daily consumption of about 20/30 g.Its use is preferred to animal fats, such as butter and lard found in the WD[15].Olea europaea is the most widespread cultivar in Europe and its presence in the Mediterranean basin dates back more than 5500 years[25].EVOO is characterized by a peculiar chemical composition,consisting of approximately 97%-99% lipids, with the remaining fraction equal to 1%-3% of compounds with antioxidant and bioactive properties.Among these minor components, there are sterols, hydrocarbons(squalene, ß-carotene), flavonoids, carotenoids, terpenoids, tocopherols and polyphenols such as hydroxytyrosol, oleocanthal (OC) and oleuropein (OL).OL constitutes a secoiridoid, particularly abundant in EVOO, characterized by a chemical structure composed of three distinct subunits: hydroxytyrosol,elenolic acid, and a glucose molecule [Figure 1][26].
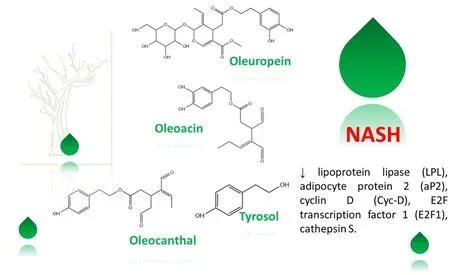
Figure 1.2D chemical structures of EVOO polyphenols.
OL has been the subject of several studies with the aim of identifying its beneficial effects in the treatment of metabolic syndrome and particularly in NASH.In a study carried out by Park et al., the male C57BL/6N mice were treated for ten weeks with a standard diet, high-fat diet (HFD), or HFD + OL[27].The study reported that OL supplementation reversed HFD-induced upregulation of lipogenic liver genes such as PPARγ2, liver X receptor (LXR), lipoprotein lipase (LPL), adipocyte protein 2 (aP2), cyclin D (Cyc-D), E2F transcription factor 1 (E2F1), cathepsin S (CTSS), frizzled-related sequence secreted protein 5 (SFRP5),Dickkopf homolog 2 (DKK2), and fibroblast growth factor receptor 1 (FGFR1) in the liver.In a study by Kim et al., the 38 mice were treated for 6 months with a regular diet and a HFD and they were subsequently supplemented with OL for additional 6 months (supplementation was evaluated after 3 and 6 months)[28].The results showed that the mean serum levels of total cholesterol (TC) and triglycerides (TG) in the OLsupplemented group were lower than in the HFD group.Furthermore, the fibrotic score showed a decrease of approximately 47% in the supplemented group compared with the HFD group after 3 months and of approximately 65% after 6 months (P < 0.05).Subsequently, Gabbia et al.evaluated the hepatic antifibrotic effect of OC[29].Briefly, the 18 BalB/C mice were examined and treated as indicated in Table 2.The results showed that OC significantly downregulated the mRNA expression of pro-fibrogenic markers such as alpha-smooth muscle actin (α-SMA), collagen type 1 alpha 1 chain (COL1A1), the metalloproteinases MMP2, MMP3, MMP7, the vascular endothelial growth factor A (VEGF-A), and the pro-oxidant NADPH oxidase genes (NOX1 and 4).
ONION
Another important component of the Mediterranean diet is onion (Allium cepa L.).As a vegetable, it is included at the bottom of the Mediterranean diet food pyramid with a recommended consumption of 19.9 g/day[15].Onion is a biennial herbaceous plant whose bulbs are used as food.A particular variety is the Tropea, more commonly known as the red onion of Tropea whose production is concentrated in Calabria region, Southern Italy.The European Union has awarded this variety the Protected Geographical Indication(PGI) as “Red Onion of Tropea Calabria-PGI”.Knowledge relating to this vegetable dates back to the Middle Ages, but it was during the Renaissance that it reached its maximum prevalence as food.In addition to its nutritional characteristics, onion is also rich in intriguing phytochemical compounds.Indeed, it contains high concentrations of flavonoids, fructo-oligosaccharides, sulfur compounds, and saponins[30].In this regard, the red onion of Tropea would seem to acquire greater relevance among other cultivars, since analyses of its extracts have demonstrated a high content of flavonoids, approximately 29.35 ± 0.03 mg/mL[31,32].One of the main flavonoids present in onion is quercetin (Q) (3,5,7,3-4-pentahydroxyflavone),chemically characterized by a fifteen-carbon skeleton containing two hydroxylated aromatic rings, linked bya fragment of three carbon atoms which form a pyran ring with a ketone function at position four.Q is mainly known for its antioxidant properties[33].Marcolin et al.analyzed the beneficial effects of Q on 64 male C57BL/6 mice[34].During the study, the mice were divided into four groups: control group (CO),CO+Q group, NASH group (methionine- and choline-deficient diet, MCD), and NASH+Q group.Q supplementation included a dose of 50 mg/kg.The mice were analyzed 2 and 4 weeks after the beginning of the experiment.The results indicated that there was a reduction in steatosis, inflammation, and swelling in the NASH+Q group compared with the NASH group.Furthermore, the NASH+Q group had a significant reduction in the gene expression of inflammatory proteins such as Toll-like receptor 4 (TLR-4), Highmobility group box 1 (Hmgb1), interleukin-6 (IL-6), tumor necrosis factor (TNF), and cyclooxygenase 2.Among the analyzed antifibrotic effects, it was observed that Q had counteracted the gene overexpression of profibrotic factors such as MMP9 and tissue inhibitor of MMP1 (Timp1).In a study by Ying et al., the beneficial effects of Q were analyzed on 48 male gerbils (Meriones unguiculatus)[35].The study involved the preparation of 6 groups: CO, HFD, HFD + lovastatin (3.3 mg/kg, PC), HFD and low doses of Q (15 mg/kg,QL), HFD and intermediate doses of Q (30 mg/kg, QM), and HFD and high doses of Q (60 mg/kg, QH).In the QM and QH groups, a reduction in serum levels of TC, TG, low-density lipoprotein cholesterol (LDLC), alanine aminotransferase (ALT), aspartate aminotransferase (AST), TNF-α and IL-6 were observed compared with the HFD group.Furthermore, it was observed that the QM and QH groups had increased expression of Sirtuin 1 (Sirt1) compared with the HFD group.While the expression of the p65 component of the Nuclear Factor kappa-light-chain-enhancer of activated B cells (NF-κB p65) and inducible nitric oxide synthase (iNOS) were reduced compared with the HFD group (P < 0.01).The study carried out by Mohan et al.analyzed the effects of Q, pioglitazone, and hydroxycitric acid (HCA) on NASH[36].The experiment was conducted for 8 weeks on 48 male Wistar rats divided into eight groups: CO, NASH group,CO + pioglitazone (4 mg/kg from the fifth week of treatment), CO + Q (20 mg/kg from the fifth week), CO+ HCA (150 mg/kg from the fifth week of treatment), NASH + pioglitazone group (4 mg/kg from the fifth week of treatment), NASH + Q group (20 mg/kg from the fifth week), and NASH + HCA group (150 mg/kg from the fifth week of treatment).The study highlighted that the NASH + Q group showed reduced serum levels of TC, free cholesterol, esterified cholesterol, TG, and FFA compared with the NASH group(P < 0.001).Table 3 summarizes the pre-clinical trials of the supplementation with Q.In a study by Shi et al.,the effects of the use of quercetin, isoquercetin and rutin on the gut microbiota in NAFLD mice wereevaluated[37].The results highlighted that at a microbial level, the three flavonoid compounds induced a regulation of the gut microflora, especially in the Akkermansia, Bifidobacterium, and Lactobacillus genera which were particularly compromised in NAFLD mice.Subsequently, Juárez-Fernández et al.evaluated the effect of a synbiotic compound of Akkermansia muciniphila and quercetin in 21 NAFLD rats[38].The results of the study indicated that the use of the synbiotic promoted a greater abundance of Cyanobacteria and Oscillospira and lower levels of Actinobacteria, Lactococcus, Lactobacillus, and Roseburia.The obtained data show how the typical compounds of the Mediterranean diet not only act as antioxidants and antiinflammatories, but also play a crucial role in modulating the intestinal microbiota, leading to an improvement in NAFLD.
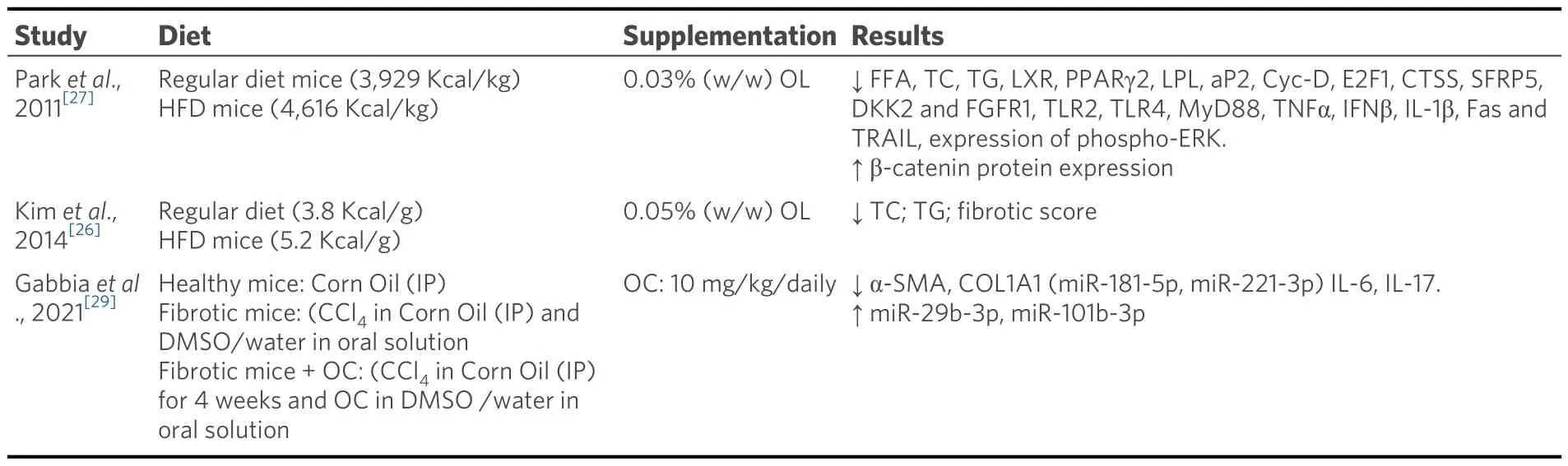
Table 2.Supplementation with EVOO polyphenols in the regression of NASH
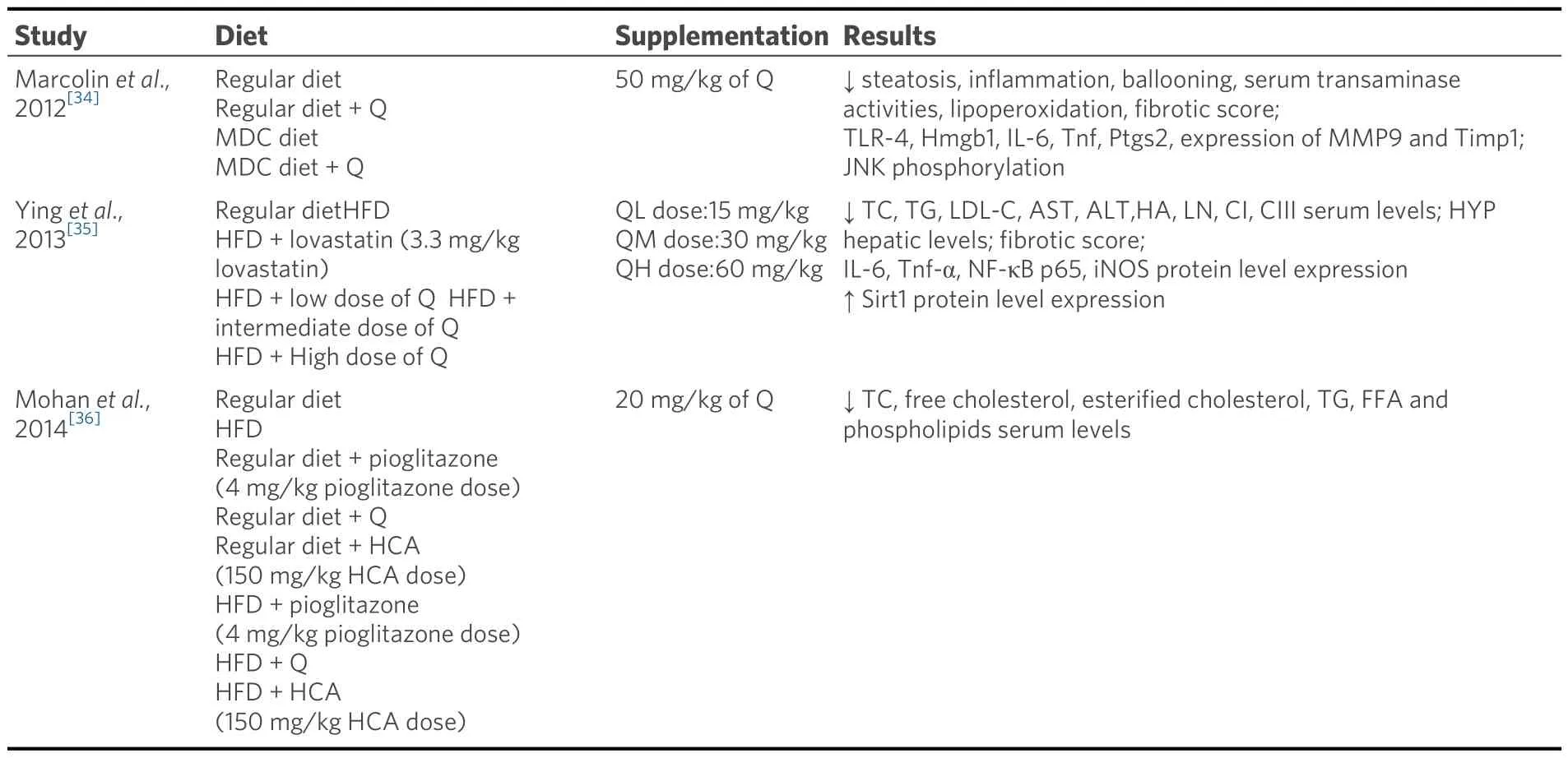
Table 3.Supplementation with Q in the regression of NASH
FISH
Among the main foods, the Mediterranean diet consists of a lot of fish.Fish is located centrally in the food pyramid, with a recommended consumption of twice a week[15].The nutritional importance of consuming fish lies in their lipid profile, in particular owing to the high content of polyunsaturated fatty acids (PUFA),which present fundamental nutrients for human health.Among the various PUFAs, eicosapentaenoic acid(EPA) and docosahexaenoic acid (DHA) stand out, classified as ω-3 PUFA[39].Furthermore, it is also possible to find smaller quantities of ω-6 PUFA, particularly linoleic acid and linolenic acid.Generally, ω-6 PUFAs are mainly present in plants and fish assuming they feed on algae.This means that the ω-6 PUFA content is highly variable in relation to the various species analyzed and the type of feeding[40].Furthermore,the lipid composition of fish is extremely variable depending on the type of water, whether fresh or salty and seasonality.In fact, some studies have shown that freshwater fish contain lower percentages of ω-3 PUFA than marine fish[39].In particular, it has been observed that fish from the Ionian Sea are particularly rich in ω-3 PUFA.Despite all these variables, it is possible to state that, among the most widespread species in the Mediterranean Sea, those that show a higher PUFA content are the leaner fish, such as salpa, red mullet,black goby, sea bream, and sea bass.In more detail, the highest percentages of PUFA ω-3 were found in red mullet (20.81%) and sea bream (26.96%), while the highest percentages of ω-6 PUFA were found in salpas(4.80%) and black goby (9.51%).EPA appears to be present in greater quantities in milk bream (8.6%), while DHA in salpa (17.4%) and sea bream (17.2%)[41].A study carried out by Antraco et al.analyzed the preventive effects of ω-3 PUFAs in NASH using C57BL/6 mice treated for 16 weeks[42].In the first eight weeks (period I), the mice were divided into two groups: CO and HFD.From the ninth week (period II),half of the mice in the HFD group were treated with fish oil (OF) rich in ω-3 PUFA, mainly EPA and DHA.Supplementation (2 g/kg) was carried out three times a week per os.In period I, all mice in the HFD group had a 30% increase in body mass compared with the CO group.In period II, animals in the HFD and HFD+OF groups had an increase in body mass of 48% and 29%, respectively.These results indicate that OF treatment reversed the increase in body mass, promoting a 27% reduction compared with the HFD group.Furthermore, inguinal white adipose tissue, which acts as a lipid depot, was analyzed and a significant increase in depot mass of 40% was observed for the HFD group.On the contrary, in the HFD+OF group,this increase was partially reversed, resulting in a 20% reduction compared with the HFD group.Regarding the plasma lipid and glycemic profile, the HFD group showed an increase in fasting blood glucose values(+26%), TC (+15%), LDL-C (+25%), TG (+16%), and non-esterified fatty acids (NEFA, +27%) and a reduction in high-density lipoprotein cholesterol (HDL-C) (-16%) compared with the CO group.On the contrary, the HDF+OF group showed a positive effect on fasting blood glucose values (-29%), TC (-37%),LDL-C (-50%), TG (-36%), and NEFA (-27%) and on HDL-C values (+30%) compared with the HFD group.Li et al.carried out a randomized study on 78 patients diagnosed with NASH.The participants were mainly overweight or obese men for whom the presence of secondary causes of NASH was excluded[43].The participants were randomly divided into two groups: CO, subjected to the administration of normal saline solution, and PUFA group, treated with 50 mL of PUFA with a 1:1 ratio of EPA and DHA.The experiment lasted 6 months, during which all participants were advised to carry out modest physical activity and follow a low-calorie diet.Evaluations of the participants were carried out at baseline and at the end of the experiment.At the initial evaluation, the two groups had similar baseline conditions.In particular, elevated serum levels of liver function and lipid profile, such as AST, ALT, TG, TC, and LDL-C, were observed.Markers of inflammation (C-reactive protein, CRP), oxidation (malondialdehyde, MDA), and fibrosis(collagen type IV and pro-collagen type III pro-peptide, P-III-P) were also higher to the normal range for both groups.After 6 months of treatment, an improvement in liver function was observed in the PUFA group with a reduction in serum ALT and AST levels compared with CO.Furthermore, in the PUFA group,the lipid profile also improved with the reduction in serum TC and TG levels.Finally, in the PUFA group, a reduction in serum levels of CRP, MDA, type IV collagen, and P-III-P was highlighted compared with the CO group.Subsequently, Nogueira et al.carried out a randomized, double-blind study on 60 adult outpatients aged between 18 and 75 with a proven diagnosis of NASH[44].The enrolled patients were randomized into two groups: the ω-3 PUFA group (32 patients) and the placebo group (28 patients).The ω-3 PUFA group involved the administration of 3 capsules per day, each containing 0.315g of PUFA (64% αlinolenic acid (ALA), 16% EPA and 21% DHA).The placebo group, however, took three identical capsules daily, but containing 2 ml of mineral oil.The study was conducted for 6 months, during which 10 patients dropped out, 5 for each group.The results of the study indicated that the ω-3 PUFA group showed a significant reduction in serum TG in comparison with a baseline (P < 0.01) after three months of treatment.Furthermore, in the ω-3 PUFA group, a correlation was observed between the increase in individual plasma levels of ALA and EPA and the percentage of patients who had relative improvements in hepatic lobular inflammation (ALA, P = 0.02; EPA, P = 0.002); steatosis (ALA, P = 0.04; EPA, P = 0.05) and ballooning(ALA, P = 0.01; EPA, P = 0.02).Table 4 summarizes the trials of the supplementation with PUFA.

Table 4.Supplementation with PUFA in the regression of NASH
BERGAMOT
Bergamot (Citrus bergamia Risso & Poiteau) is an endemic plant of the Calabria region (Italy) belonging to the Rutaceae family[45].As a fruit, it is included at the bottom of the food pyramid in the Mediterranean diet,with recommended daily consumption[15].Bergamot essential oil is obtained by rasping and cold pressing the peel of the fruit and is widely used in the production of fragrances, cosmetics, and sweets.In addition to its industrial applications, bergamot has been the subject of studies for its antioxidant, anti-carcinogenic,and anti-inflammatory activities[46-50].Its beneficial activities are traced back to its unique polyphenolic composition.Among the main components of bergamot, there are glycosylated flavanones like naringin,neoeriocitrin, hesperidin, and flavones such as diosmetin and apigenin[51,52].Recent evidence suggests that bergamot might exert beneficial effects in the prevention and regression of NASH.In a study carried out by Parafati et al., the effects of a bergamot polyphenolic fraction (BPF) were evaluated on rats in which NAFLD/NASH was induced[53].During the study, 21 rats were fed the “cafeteria” (CAF) diet (15% protein,70% carbohydrates, and 15% fat) and 5 rats the Standard chow (SC) diet for 15 weeks.Over the next 11 weeks, the 21 obese rats were divided into three groups: CAF/CAF group, CAF/SC group, and CAF/SC+BPF group.The CAF/CAF group continued to be fed the CAF diet, while the CAF/SC and CAF/SC+BPF groups switched to the SC diet with and without BPF, while the 5 rats (SC/SC group) continued the treatment with SC.Study results showed that CAF/CAF rats had massive accumulation of lipid droplets and Kupffer cell infiltration, indicating a histological severity consistent with NASH.Furthermore, it was shown that fasting plasma insulin concentrations of CAF/SC/BPF rats were significantly lower than those of CAF/SC rats.Moreover, the Homeostatic Model Assessment for Insulin Resistance index was also significantly lower in the CAF/SC+BPF group compared with the CAF/SC group.Musolino et al.analyzed the effects of a polyphenolic formulation of bergamot (BPF99) for the treatment of NASH[54].During the study, the 8-week-old mice were randomly assigned to receive a chow diet, or a WD.After 16 weeks of WD diet, mice were further randomized and treated with WD, or WD + BPF99 (50 mg/kg) by gavage.At the end of the experiment, the mice were sacrificed and the results indicated that the supplementation with BPF99 reduced ALT (average 71.6 vs.44.6 IU/l, P < 0.01), TG (38.8 vs.28.1 mg/dl, P < 0.05), and LDL-C (39.2 vs.23.7 mg/dl,P < 0.001) compared with the WD group.
ROSEMARY
Rosemary (Rosmarinus Officinalis L.), belonging to the Lamiaceae family, is a native shrub typical of the Mediterranean.As a vegetable, it is included at the bottom of the food pyramid in the Mediterranean diet,with a recommended consumption of 2.5 g/day[15].Its use has been known since ancient times and it is rooted in the cultures and traditions in many Italian regions.Rosemary is used as an ornamental and aromatic plant, above all owing to its organoleptic characteristics.Its aerial parts are used as a spice or for the extraction of crude oil used in the pharmaceutical, cosmetic, and perfume industries.Rosemary extract is known for its antioxidant, anti-inflammatory, anticancer, digestive, and diuretic activities[55-59].Rosemary extract is rich in carnosic acid (CA) and rosmarinic acid (RA).RA is an ester of caffeic acid and 3,4-dihydroxyphenyllactic acid and has many beneficial activities such as astringent, antioxidant, antiinflammatory, antimutagenic, antibacterial, and antiviral[60,61].Several studies have analyzed the effects of using rosemary components in the prevention of NASH.In this regard, a study carried out by Komeili-Movahhed et al.analyzed the beneficial effects of RA on 24 C57/BL6 mice in which NASH was induced[62].During the study, mice were divided into four groups: CO group (standard diet), RA group (standard diet and RA (10 mg/kg), NASH group (MCD), and NASH+RA group MCD and RA (10 mg/kg).In this study, it emerged that the NASH group had a significant increase in serum levels of AST and ALT, while the NASH+RA group showed a significant reduction in both transaminases (P < 0.05).The CO and RA groups had a regular and healthy liver structure, while the NASH group had an enlargement of liver cells with the formation of collagen deposits.In contrast, in the NASH+RA group, liver cell size was reduced with less collagen deposition compared with the NASH group.Finally, it emerged that in the NASH group, the gene expression of the fibrotic markers tumor growth factor(TGF)-β and α-SMA was significantly increased,while the NASH+RA group showed a significant reduction in the gene expression of TGF-β and α-SMA (P <0.05).Komeili-Movahhed et al.carried out a new study on 24 C57/BL6 mice treated for 8 weeks[63].During the experiment, the mice were divided into four groups: CO group (standard diet), RA group (standard diet and RA (10 mg/kg), NASH group (MCD diet), and NASH+ RA group (MCD + RA diet (10 mg/kg).The results of the study showed that the NASH group presented a significant increase in serum levels of ALT,AST, TG, and cholesterol; on the contrary, these parameters showed a significant reduction in the NASH+RA group.Furthermore, it emerged that the NASH+RA group, compared with the NASH group,showed a significant reduction in Sterol regulatory element-binding protein 1 and FAS gene expression and an increased expression of PPARα (P < 0.001 and P < 0.01, respectively).Regarding the inflammatory process, the NASH+RA group reported a reduction in lumbar inflammation and a reduction in the expression of NF-kB, TNF-α, and IL-6.Finally, in the NASH+RA group, a marked reduction in the expression of tumor protein P53, the Bax/Bcl2 ratio, and the protein expression of caspase3 was highlighted compared with the NASH group (P < 0.05; P < 0.01 and P < 0.001, respectively).
CONCLUSION
NASH is a serious pathological condition that can progress into liver cirrhosis and hepatocellular carcinoma if not adequately treated.At the moment, there are no specific pharmacological therapies for NASH, so adopting a healthy lifestyle, a low-calorie diet, and moderate physical activity are the main strategies to improve the patient's pathological condition.There are several clinical studies in the literature that evaluated the preventive action of the Mediterranean diet in NAFLD[64,65].However, these studies lack a better definition of the preventive actions of the Mediterranean diet in NASH patients.
DECLARATIONS
Authors’ contributions
Wrote, reviewed, and edited the manuscript: Procopio AC, Paravati MR
Provided figures and tables: Procopio AC, Paravati MR
Reviewed and approved the final manuscript as submitted: Procopio AC, Paravati MR, Scarlata GGM, Milic N, Abenavoli L
Read and approved the final manuscript: Parafati M, Luzza F, Abenavoli L
Conceptualized and designed the review: Abenavoli L
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2024.