
Effect of special types of bread with select herbal components on postprandial glucose levels in diabetic patients
2024-04-22 00:59:08DraskoGostiljacSrdjanPopovicVesnaDimitrijevicSreckovicSasaIlicJelenaJevtovicDraganNikolicIvanSoldatovic
World Journal of Diabetes 2024年4期
Drasko M Gostiljac,Srdjan S Popovic,Vesna Dimitrijevic-Sreckovic,Sasa M Ilic,Jelena A Jevtovic,Dragan M Nikolic,Ivan A Soldatovic
Abstract BACKGROUND Nutrition recommendations in patients with type 2 diabetes mellitus (T2DM) are to consume rye or integral bread instead of white bread.A positive effect on glucoregulation has been achieved by enriching food with various biologically active substances of herbal origin,so we formulated an herbal mixture that can be used as a supplement for a special type of bread (STB) to achieve better effects on postprandial glucose and insulin levels in patients with T2DM.AIM To compare organoleptic characteristics and effects of two types of bread on postprandial glucose and insulin levels in T2DM patients.METHODS This trial included 97 patients with T2DM.A parallel group of 16 healthy subjects was also investigated.All participants were given 50 g of rye bread and the same amount of a STB with an herbal mixture on 2 consecutive days.Postprandial blood glucose and insulin levels were compared at the 30th,60th,90th and 120th min.A questionnaire was used for subjective estimation of the organoleptic and satiety features of the two types of bread.RESULTS Compared to patients who consumed rye bread,significantly lower postprandial blood glucose and insulin concentrations were found in T2DM patients who consumed STB.No relevant differences were found among the healthy subjects.Subjectively estimated organoleptic and satiety characteristics are better for STB than for rye bread.CONCLUSION STB have better effects than rye bread on postprandial glucoregulation in T2DM patients.Subjectively estimated organoleptic and satiety characteristics are better for STB than for rye bread.Therefore,STB can be recommended for nutrition in T2DM patients.
Key Words: Special types of bread;Postprandial glucoregulation;Insulin;Nutrition;Type 2 diabetes mellitus
INTRODUCTION
Diabetes mellitus (DM) is one of the main health issues worldwide,and its incidence has been increasing for several decades[1,2].Additionally,many people have reduced glucose tolerance[3].A Global Report on Diabetes showed that the number of adult DM patients increased almost fourfold between 1980 and 2014,going from 108 million patients to 422 million patients[4].This dramatic increase is mostly due to type 2 DM (T2DM) and its risk factors,especially obesity[5].
Dietary interventions are the main economic and effective strategies aimed at reducing blood glucose and insulin levels in the population[3,6].Physical activity also improves glucose tolerance as a supplemental treatment for obesity but not as a replacement for dietary measures[7].Controlled nutrition improves glucose tolerance by reducing endogenous glucose production and improving sensitivity to insulin[8].The consumption of foods with a low glycemic index (GI) decreases postprandial blood glucose and insulin levels and their fluctuations[9,10].
One of the basic foodstuffs worldwide is bread.Recommendations for this population include the consumption of rye or whole grain bread with higher dietary fiber (DF) content instead of white bread[11].Several trials have shown that a positive effect on glucoregulation may also be achieved by enriching food with various biologically active substances of herbal origin[12].
TopiGluk bread was patented by the National Intellectual Property Office (registration No.73932) as a supplementary treatment for people with disease.TopiGluk bread is made by adding a mixture of nutrients to whole wheat,oat and buckwheat flour.
We hypothesized that TopiGluk bread would significantly improve glucose tolerance in T2DM patients.The aim of this study was to evaluate the effects of TopiGluk bread on postprandial glucose levels in T2DM patients.Additionally,the insulin levels and organoleptic properties of the examined bread were evaluated as secondary objectives.
MATERlALS AND METHODS
Time and place of study
A prospective study was conducted at the Clinic of Endocrinology,Diabetes and Metabolic Disorders,Clinical Center of Serbia,Belgrade.The study was carried out from 20 May 2016 to 25 March 2017.
Subjects
The trial included 97 patients with T2DM who were treated as outpatients at the Clinic of Endocrinology,Diabetes and Metabolic Disorders,Faculty of Medicine,University of Belgrade.The inclusion criteria were 18 years or older and confirmed T2DM.The exclusion criteria were acute T2DM complications;acute inflammatory conditions;chronic diseases of the liver or gastrointestinal tract;malignant diseases;immunodeficiency;narcotic or alcoholic addictions;and pregnancy (Figure 1).

Figure 1 CONSORT flowchart. T2DM: Type 2 diabetes mellitus.
A parallel group of 16 healthy controls were analyzed;they had no history of metabolic disorders (including DM) and had preserved glucose homeostasis based on their medical history.
All of the subjects provided informed consent for inclusion in the study.The investigation was carried out in accordance with the Declaration of Helsinki and was revised in 2013.The study was carried out in accordance with the EU Directive 20/2001/EC,the Commission Directive 2005/28/EC,and the European Parliament Declaration on Good Clinical Practice,as well as the International Conference on Harmonization ICH-GCP (E6);approval for this research was given by the Ethics Committee,Clinical Center of Serbia,No.105/39 on 19 May 2016.The study is registered in the German Clinical Trials Register DRKS00023611.The clinical trial was registered after completion because the law of the Republic of Serbia does not require registration in the international registry.The authors confirm that all ongoing and related trials for this food supplement have been registered.
Study protocol
Prior to the trial,a detailed history was taken,which included data on physical activity and lifestyle,the duration of T2DM and therapy,chronic complications of T2DM and nutritional habits.Data on anthropometric characteristics,weight and height were obtained from medical records if no significant changes were observed in the last 6 mo.Body mass index was calculated by dividing the body weight in kilograms by the squared body height in meters (kg/m2).All participants were instructed to fast for at least 12 h prior to blood sampling.
A slice of bread weighing 50 g was provided to each participant,which is the usual portion for T2DM patients.The nutritional content of the bread is presented in Table 1.One day,all participants were given a piece of rye bread,and on another day,they were given a piece of special bread.Patients were advised to perform similar activities on both days.Furthermore,patients were required to fast for 12 h prior to each blood sampling.
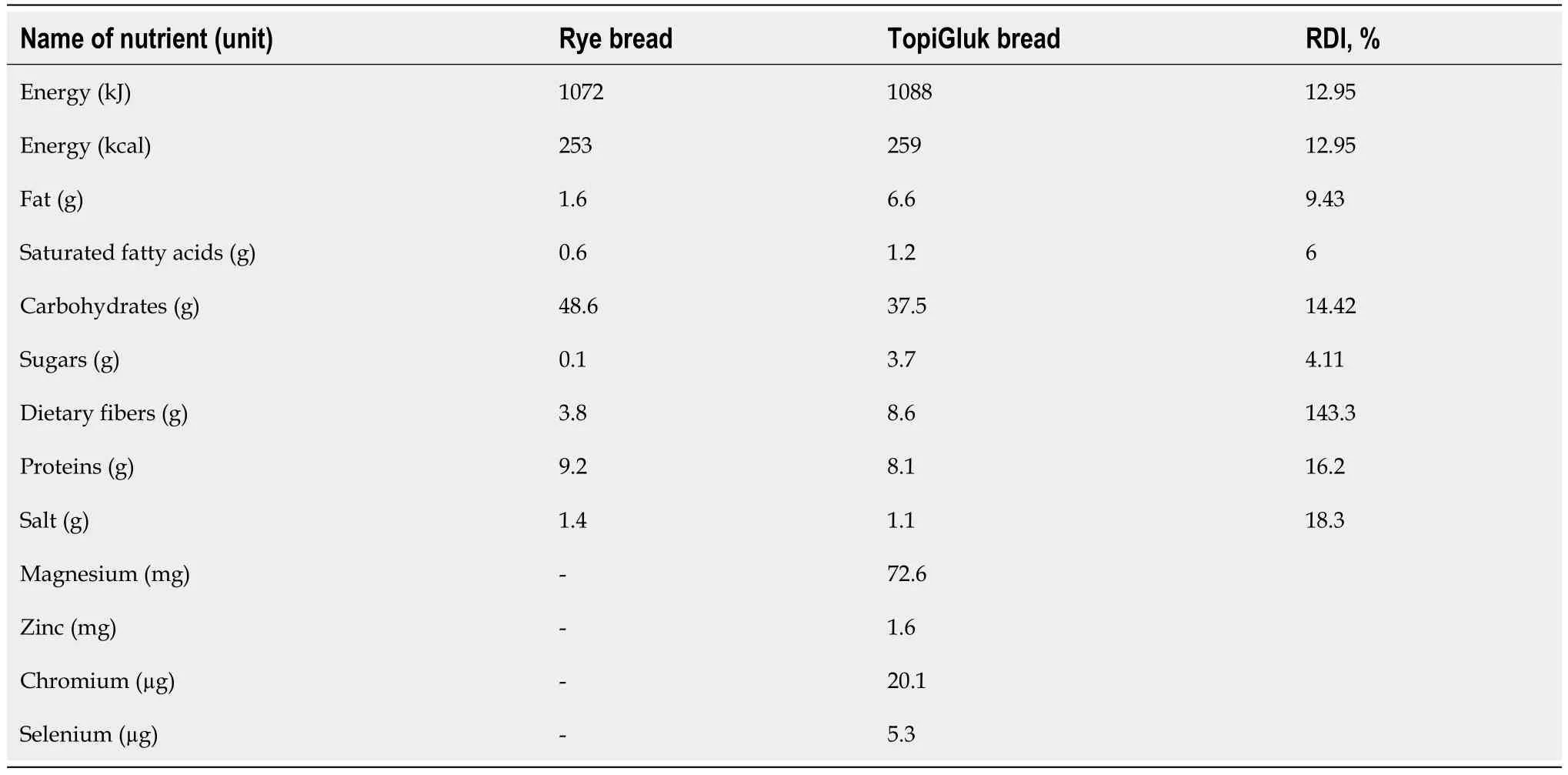
Table 1 Comparative nutritional composition of the rye bread and TopiGluk bread (100 g)
Participants were instructed to complete a questionnaire about the look,smell,taste,quantity,and satiety of the bread.Answers were given on a numerical scale from 1 (worst) to 5 (best).Upon arrival at the clinic at approximately 08:00 in the morning,the responsible researcher accommodated each participant in the laboratory.A venous cannula was inserted in the arm of the patient.The first blood sample was taken before the meal.Next,four blood samples were taken every 30 min after the meal.Healthy subjects were with evaluated with a glucose meter,and blood samples were collected using finger sticks (capillary blood sampling) in the infirmary.
The laboratory analyses of T2DM patients included hemoglobin A1c (HbA1c) and C-peptide levels (at baseline only) and glucose and insulin levels (at baseline and 30 min,60 min,90 min and 120 min after the meal) on both examination days.Blood glucose measurements were performed using the spectrophotometric (hexokinase) method with a COBAS 6000 (Roche Diagnostics,Basil,Switzerland) with a reference range of 3.9-6.1 mmol/L.Insulin and C-peptide levels were measured using an immunoradiometric assay method with a gamma counter forinvitrodiagnosis (LKB-WALLAC ChinGamma Model 1272).
Laboratory analysis of healthy controls included only glucose levels at baseline (before the meal) and at 30 min,60 min,90 min and 120 min after the meal.Blood measurements from capillary blood were performed with an electrochemicalmethod using a Biosen C-Line machine (EKF Diagnostics,Cardiff,United Kingdom) with a reference range of 3.9-6.1 mmol/L.
Due to differences in sampling methods,diabetic and healthy subjects were not compared,except for blood sugar changes from baseline to 120 min (the sampling method did not affect the change).
Differences between 30 min and baseline,60 min and baseline,90 min and baseline and 120 min and baseline levels were calculated (delta glucose and delta insulin).The area under the curve (AUC) was calculated using a trapezoidal model[13].
Ingredients of special type of bread
The bread was a brand of the Delhaize Serbia distributor in cooperation with partners for product development: The international company Puratos and the national bakery products manufacturer Alimpije-and with a partner for product improvement-ZZ Zdravlje (Čačak,Serbia),the inventor of TopiGluk®.
The ingredients of TopiGluk®bread are as follows: Basil (Ocimumbasilicum),garlic (Alliumsativum),Greek seed (Trigonellafoenumgraecum),ginger (Zingiberofficinale),oat (Avenasativa),Jerusalem artichoke (Helianthustuberosus),and cinnamon (Cinnamomumverum).Sunflower and linen seeds are also among the supplements.The nutritional content of 100 g of the special type of bread (STB) with the TopiGluk mixture is presented in Table 1.Approximately one-third of the mentioned mixture contains active principles (TopiGluk),while the remaining two-thirds are equivalent parts buckwheat,oat and whole wheat flour.The representation of the components in TopiGluk was 0.5% garlic,0.5% ginger,2% basil,3% Greek seed,5% cinnamon,8% oat,and 13% Jerusalem artichoke.
Statistical analysis
A sample size of 97 T2DM patients with achieved 90% power to detect a mean difference of 1.0 ± 3.0 mmol/L with a significance level for alpha error of 0.05 using a two-sided paired samplesttest.
The results are presented as counts (%) or means ± SD depending on the data type and distribution.Measurements were compared using parametric (paired samplettest) and nonparametric (Wilcoxon signed rank test) tests.Glucose changes (delta) between healthy subjects and patients were compared using an independent samplesttest.Deltas were calculated as the difference between the 30 min,60 min,90 min and 120 min time points and baseline.The AUC was calculated using the trapezoidal rule.AllPvalues less than 0.05 were considered significant.All the data were analyzed using R 3.4.2.R Core Team (2017).R: A language and environment for statistical computing.R Foundation for Statistical Computing,Vienna,Austria (https://www.R-project.org/).
RESULTS
The majority of participants were males in the 6thto 7thdecade of life,preobese to obese individuals,and physically active individuals.The majority of patients were receiving oral antidiabetic therapy,while one-third were receiving insulin.Coronary disease and neuropathy were present in one-third of patients.The average duration of diabetes was shorter than 10 years.Most of the patients consumed rye bread,for which the median daily intake was 1 slice,while other bread types (whole wheat bread and white bread) were less represented in terms of nutritional status (both medians were 0) (Table 2).
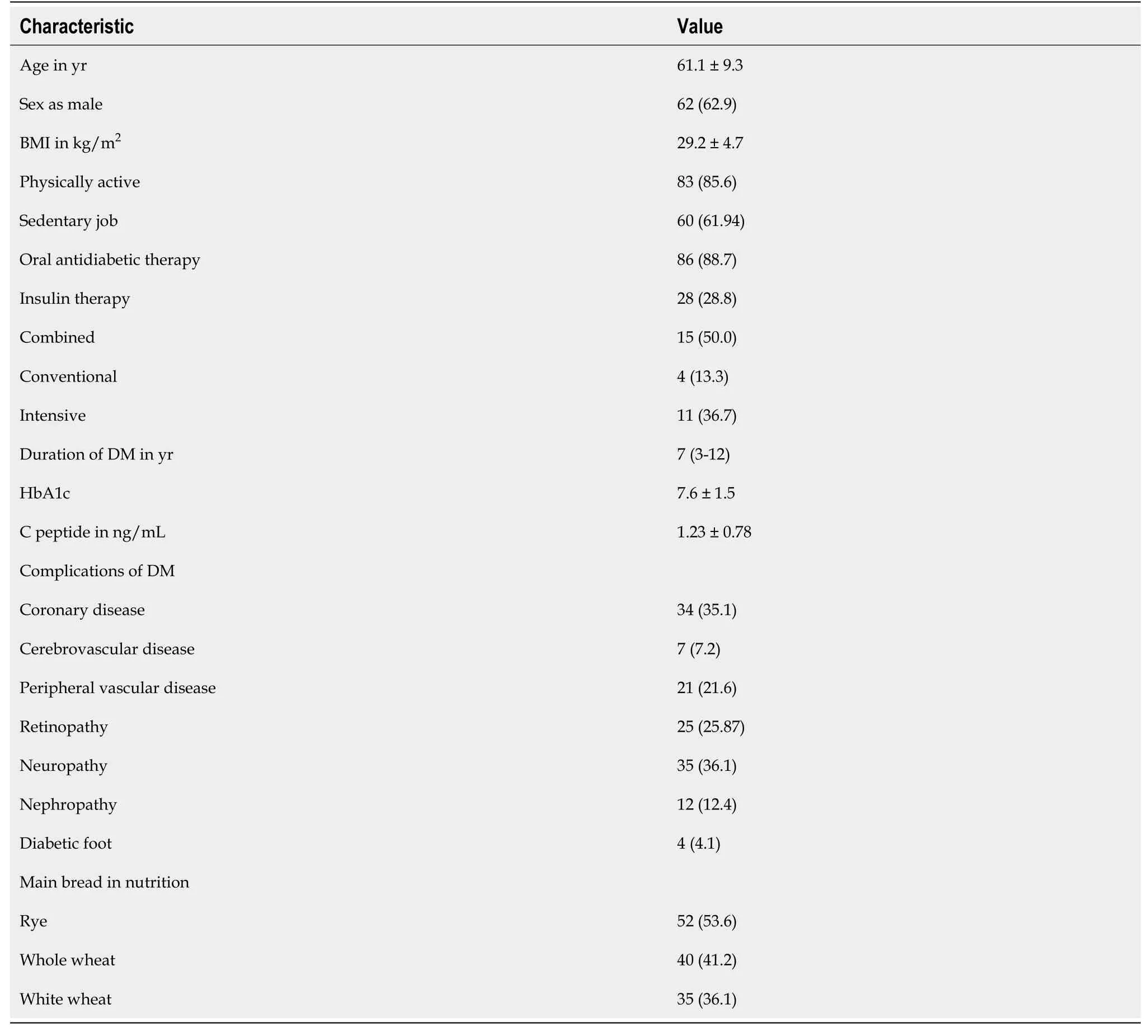
Table 2 Basic characteristics of patients with type 2 diabetes mellitus
All the evaluated characteristics were greater for the STB than for rye bread,as presented in Table 3.

Table 3 Subjective assessment of the quality of bread/scale from 1 to 5
In T2DM patients,we found better glucoregulation after the STB portion than after the rye bread portion.Significantly lower delta values of blood glucose were observed after the STB portion at the 90thand 120thmin than after the rye bread portion.In healthy subjects,no significant differences in blood glucose delta values were observed,except at the 90thmin.Concerning the AUC of blood glucose,a significant difference was found only at the 90thmin.In T2DM patients,the AUC was 21.2% ± 5.1% after the rye bread portion and 19.6% ± 4.5% after the STB with TopiGluk portion (P< 0.001).In healthy subjects,no significant differences in the AUC were found after the two types of bread were consumed (P=0.924) (Figure 2).
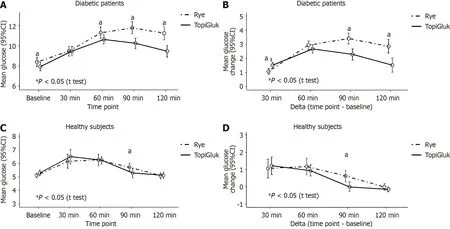
Figure 2 Mean glucose levels and mean glucose change (in mmol/L) after the consumption of rye bread and the special type of bread with TopiGluk® in diabetes mellitus type 2 patients and healthy subjects. A: Absolute values of glucose in diabetic patients;B: Glucose change from baseline in diabetic patients;C: Absolute values of glucose in healthy subjects;D: Glucose change from baseline in healthy subjects.aP < 0.05.
When comparing patients and healthy subjects regarding delta values,all differences were significant at the 0.001 level for both the rye bread and the STB with the TopiGluk®mixture,except for the change from baseline to 30 minutes after the rye (P=0.919) and STB with TopiGluk®(P=0.313) portions (Figure 2).
The insulin levels of the patients were analyzed at each time point (0,30,60,90 and 120 min) and for each type of bread (Figure 3).Initially,the median insulin concentrations were identical.However,significant differences in insulin levels were observed at the 90thmin and the 120thmin after the two types of bread were consumed.After the STB with TopiGluk®was consumed,we found significantly lower median insulin concentrations compared to after rye bread was consumed.A comparison of the deltas revealed significant differences at the same time points.The median value and interquartile range of the AUC of insulin in T2DM patients with was 46.7 (29.7-61.1) after consuming rye bread and 39.9 (30.1-57.0) after consuming the STB with TopiGluk®(P=0.035).
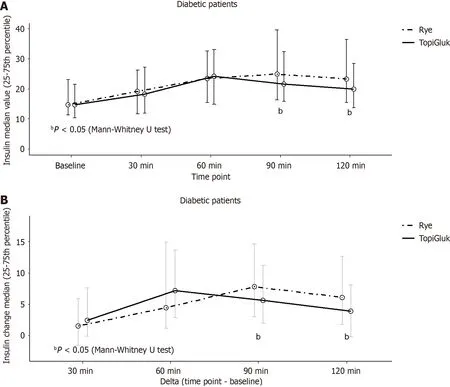
Figure 3 lnsulin levels (µlU/L),median (25-75th percentile) and change after the consumption of rye bread and the special type of bread with TopiGluk® in diabetic patients. A: Absolute values;B: Change compared to baseline.bP < 0.05.
Diabetic patients were divided into two subgroups: patients receiving oral antidiabetic therapy and patients receiving insulin therapy (Figure 4).In patients on oral antidiabetic therapy,significantly higher blood glucose levels were observed at the 60th,90thand 120thmin after the rye bread was consumed than after the STB with TopiGluk®was consumed.Differences in blood glucose changes from baseline were significant at the 90thmin and at the 120thmin.In patients receiving insulin therapy,all mean glucose levels were significantly greater after rye bread was consumed than after the STB with TopiGluk®was consumed,but the changes (deltas) were significantly different only at the 90thmin and at the 120thmin (Figure 4).

Figure 4 lnsulin levels (µlU/L),median (25-75th percentile) and change after the consumption of rye bread and the special type of bread with TopiGluk® in diabetic patients. A: Absolute values in patients with oral antidiabetic therapy;B: Change compared to baseline in patients with insulin therapy;C: Change compared to baseline in oral antidiabetic therapy patients;D: Change compared to baseline in insulin therapy patients.aP < 0.05.
DISCUSSION
This study compared the effects of rye bread and (STB) with TopiGluk®on glucoregulation.Patients subjectively assessed the STB as better than the rye bread regarding appearance,aroma,taste,amount,satiety level and duration of satiety.We observed lower glycemic and insulin levels from baseline to the 120thmin in diabetic patients after the STB was consumed than after the rye bread was consumed.In healthy subjects,this difference was not observed,as expected.
The STB with TopiGluk®can be described as a “functional food” because it may have the following positive effects on glucose metabolism: decreased glucose absorption from the intestine to blood,increased glucose utilization,increased cell sensitivity to insulin,reduced insulin resistance,increased endogenous insulin production and increased glycogen in the liver[14].
Glucose absorption has been evaluated in several studies.Glucose absorption can be reduced using foods rich in DFs.DFs include lignin and a range of polysaccharides derived from cell walls that are poorly digested in the upper intestine[15].DM patients are usually instructed to eat rye bread,which is rich in DF.Viscous and gel-forming soluble DFs inhibit macronutrient absorption and reduce the postprandial glucose response.However,in prospective cohort studies,insoluble cereal DF and whole grains,but not soluble DF,are consistently associated with reduced DM risk,suggesting that further unknown mechanisms are likely involved[16,17].TopiGluk®contains whole wheat flour,buckwheat and oatmeal,which are rich in DF,especially beta glucans.TopiGluk is also rich in the soluble DF inulin from Jerusalem artichoke,which binds water and forms a viscous solution that delays gastric emptying and intestinal transit,thus reducing glucose absorption.This leads to a decreased blood glucose response[16,17].DF also decreases insulin secretion and reduces the chance of reactive hypoglycemia during the postprandial period.On the other hand,this promotes satiety and satiation,increases fat oxidation and decreases fat storage[18].
Several authors have examined the effect of whole-meal and whole-kernel rye breads on glucose metabolism compared to that of white wheat bread.Leinonenetal[19] concluded that whole kernel rye bread has no effect on the glucose response but has an effect on the postprandial insulin response.In healthy subjects,we found no differences in blood glucose levels after consumption of the STB with TopiGluk®or after consumption of rye bread.This is probably due to preserved regulatory mechanisms of glucose metabolism in healthy subjects.
However,in T2DM patients,we found lower blood glucose and insulin levels after the consumption of the STB with TopiGluk®than after the consumption of the rye bread.This approach is very important for individuals with impaired glucose tolerance or an increased risk of diabetes.Starchin bread decomposes during digestion to simple sugars,which affect glucoregulation.TopiGluk is a mixture of natural metabolically active ingredients that play a proven role in metabolic regulation.Studies in diabetic rats revealed the significant effect of basil on glucose metabolism and its potential usefulness in treating T2DM patients[20].This effect is likely mediated by decreased glucose absorption and glucose mobilization in the liver[20].A recent meta-analysis revealed that garlic,in addition to therapy,contributes to improved glucose and lipid control[21,22].Fenugreek is mostly produced in Eastern countries,but in the West,it is often used as a medicinal herb or spice.A recent meta-analysis revealed that fenugreek acutely reduces postprandial glucose levels,but the long-term effect on glucose metabolism has not been sufficiently tested[23].A meta-analysis by Huangetal[24] revealed that ginger has no significant effect on fasting glucose levels but significantly improves HbA1c levels.Another meta-analysis by Houetal[25] revealed the significant effect of oat on fasting blood glucose,HbA1c and lipid levels.Oat is a common choice for people with obesity,digestive problems or diabetes.It is a grain with a low GI and is rich in vitamins and minerals.Jerusalem artichoke is a sunflower plant that favorably affects blood sugar levels.Its most valuable component is inulin.Dry-ground Jerusalem artichoke contains 70% inulin.Fructose is a result of inulin hydrolysis and is an excellent replacement for glucose.A study of diabetic rats revealed that Jerusalem artichoke improved metabolism,microcirculation,and blood vessel conditions and thereby reduced the severity of diabetes complications[26].A recent study of newly diagnosed DM patients revealed a positive effect of Jerusalem artichoke on postprandial glucose levels[27].Cinnamon,a spice with high global consumption,also affects fasting blood glucose levels in T2DM and prediabetic patients[12,28,29].While choosing biologically active substances for TopiGluk®,numerous factors should be considered;the most important are the availability of the substance,its impact on glucoregulation,other favorable metabolic effects,its applicability in the technological process of bread preparation and manufacturing,and the impact of certain phases of the technological procedure;for example,the impact of the bread baking temperature on the active principles of the ingredients (duration),specific aroma and taste at planned concentrations,mutual compatibility and cumulative effect on glucoregulation.
A comparison of the organoleptic properties of two kinds of bread,an STB with TopiGluk®and rye bread,revealed that the former was better than the latter.A number of respondents emphasized the sweet taste of the STB with TopiGluk®,which may be particularly important for DM patients because they are usually not allowed to consume sweet food.
The results of our research are consistent with the latest data from the literature indicating that the plants added to the TopiGluk®bread (Ocimumbasilicum,Alliumsativum,Trigonellafoenumgraecum,Zingiberofficinale,Avenasativa,Helianthus tuberosus,andCinnamomumverum) have antidiabetic properties[30-35].
CONCLUSlON
Based on the present results,we can conclude that postprandial blood glucose levels in T2DM patients are lower after consuming TopiGluk bread than after consuming the same amount of rye bread.Improved glucoregulation was noted in T2DM patients at 90 and 120 min,both in patients who were taking oral antidiabetic drugs and in patients receiving insulin therapy.An STB made with TopiGluk®has better subjectively assessed organoleptic and fine characteristics than rye bread.The STB with TopiGluk®can be recommended as part of the diet in T2DM patients.
ARTlCLE HlGHLlGHTS
Research background
Bread that we are testing is novel,tasty and very effective in populations with compromised glycoregulation.In our study,we compared novel bread with standard hospital rye bread and obtained significant differences regarding glucose metabolism of special type of bread (STB) with TopiGluk compared to rye bread.
Research motivation
All participants were given 50 g of rye bread or STB with herbal mixture on 2 consecutive days.In the continuation of these studies,it would be interesting to increase the amount of tested bread and see how it would affect postprandial glycemia.
Research objectives
To compare organoleptic characteristics of two sorts of bread and their effects on postprandial glucose and insulin levels in type 2 diabetes mellitus (T2DM) patients.
Research methods
Postprandial blood glucose and insulin levels were examined on 2 consecutive days after the consumption of rye bread and a special type of bread with an herbal mixture.A questionnaire was used for comparison of the organoleptic properties of two kinds of bread.
Research results
A special type of bread with an herbal mixture caused significantly lower postprandial blood glucose in T2DM patients than rye bread,and it showed better organoleptic and satiety characteristics.
Research conclusions
Our study showed a significant difference in postprandial blood glucose and insulin levels between patients that consumed rye bread and those that consumed a special type of bread with herbal mixture.This special type of bread has better effects on postprandial glucoregulation in T2DM patients.
Research perspectives
The results of this research can be the basis and incentive for future research that would determine which biochemical substances from plant components added to STB are responsible for the effect of postprandial glycemia.
ACKNOWLEDGEMENTS
The authors wish to thank the Puratos and Delhaize companies for the administrative and technical support.
FOOTNOTES
Author contributions:Gostiljac DM,Popovic SS and Dimitrijevic-Sreckovic V designed the research study;Gostiljac DM,Ilic SM and Jevtovic JA performed the research;Gostiljac DM,Soldatovic IA and Nikolic DM analyzed the data and wrote the manuscript;All authors have read and approve the final manuscript.
lnstitutional review board statement:All subjects provided informed consent for inclusion in the study.The investigation was carried out in accordance with the Declaration of Helsinki and was revised in 2013.
Clinical trial registration statement:The study is registered in the German Clinical Trials Register DRKS00023611.The clinical trial was registered after completion because the law of the Republic of Serbia does not require registration in the international registry.
lnformed consent statement:All study participants,or their legal guardian,provided written consent prior to study enrollment.
Conflict-of-interest statement:All authors agree that there is no conflict of interest.
Data sharing statement:No additional data are available.
CONSORT 2010 statement:The authors have read the CONSORT 2010 Statement,and the manuscript was prepared and revised according to the CONSORT 2010 Statement.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution Non-Commercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Serbia
ORClD number:Drasko M Gostiljac 0000-0002-4361-2141;Srdjan S Popovic 0009-00003996-4323;Vesna Dimitrijevic-Sreckovic 0000-0001-5763-5494;Sasa M Ilic 0009-0006-5748-7341;Jelena A Jevtovic 0009-0000-3304-2942;Dragan M Nikolić 000-0001-5919-1575;Ivan A Soldatovic 0000-0003-4893-1683.
S-Editor:Qu XL
L-Editor:Filipodia
P-Editor:Zhao S
 World Journal of Diabetes2024年4期
World Journal of Diabetes2024年4期
- World Journal of Diabetes的其它文章
- Metabolic syndrome’s new therapy: Supplement the gut microbiome
- Pancreatic surgery and tertiary pancreatitis services warrant provision for support from a specialist diabetes team
- Effect of bariatric surgery on metabolism in diabetes and obesity comorbidity: lnsight from recent research
- Application of three-dimensional speckle tracking technique in measuring left ventricular myocardial function in patients with diabetes
- lcariin accelerates bone regeneration by inducing osteogenesisangiogenesis coupling in rats with type 1 diabetes mellitus
- Long-term effects of gestational diabetes mellitus on the pancreas of female mouse offspring