
Anti-EGFR antibody monotherapy for colorectal cancer with severe hyperbilirubinemia: A case report
2024-03-07 08:19:00ToshiakiTsuruiYuyaHirasawaYutaroKubotaKiyoshiYoshimuraTakuyaTsunoda
Toshiaki Tsurui,Yuya Hirasawa,Yutaro Kubota,Kiyoshi Yoshimura,Takuya Tsunoda
Abstract BACKGROUND Hyperbilirubinemia with hepatic metastases is a common complication and a poor prognostic factor for colorectal cancer (CRC).Effective drainage is often impossible before initiating systemic chemotherapy,owing to the liver’s diffuse metastatic involvement.Moreover,an appropriate chemotherapeutic approach for the treatment of hyperbilirubinemia is currently unavailable.CASE SUMMARY The patient,a man in his 50s,presented with progressive fatigue and severe jaundice.Computed tomography revealed multiple hepatic masses with thickened walls in the sigmoid colon,which was pathologically confirmed as a welldifferentiated adenocarcinoma.No RAS or BRAF mutations were detected.The Eastern Cooperative Oncology Group (ECOG) performance status (PS) score was 2.Biliary drainage was impossible due to the absence of a dilated bile duct,and panitumumab monotherapy was promptly initiated.Subsequently,the bilirubin level decreased and then normalized,and the patient’s PS improved to zero ECOG score after four cycles of therapy without significant adverse events.CONCLUSION Anti-EGFR antibody monotherapy is a safe and effective treatment for RAS wildtype CRC and hepatic metastases with severe hyperbilirubinemia.
Key Words: Colorectal neoplasms;Panitumumab;Chemotherapy;Hyperbilirubinemia;Jaundice;Case report
lNTRODUCTlON
Metastatic colorectal cancer (CRC) is the leading cause of cancer-related deaths worldwide[1].The liver is the most common site of metastasis in CRC owing to the draining system of the portal vein.Hyperbilirubinemia is a serious consequence of hepatic metastasis and is a poor prognostic factor[2].Biliary drainage is often difficult because of diffuse hepatic involvement.Clinical decision-making in these settings is challenging,because chemotherapeutic agents that are metabolized in the liver require dose adjustments and are contraindicated in severe hepatic failure.As more major clinical trials exclude the patients with severely impaired organ function,little evidence supports an optimal regimen and dose of chemotherapy for severe hyperbilirubinemia.Although the use of cytotoxic chemotherapy in patients with hepatic metastases and severe hyperbilirubinemia has been reported in a few case series,most cases did not achieve satisfactory outcomes and severe treatment-related adverse events were also reported.Therefore,no appropriate chemotherapeutic approach has yet been established for these patients.Herein,we report a case of CRC with hepatic metastases and severe hyperbilirubinemia that was successfully treated using panitumumab monotherapy.We suggest this approach as a novel treatment option for hyperbilirubinemia caused by hepatic metastases when biliary drainage is impossible.
CASE PRESENTATlON
Chief complaints
A patient in his 50s experienced weight loss and progressive fatigue.
History of present illness
Laboratory tests revealed elevated transaminase and bilirubin levels,prompting a prompt referral to our hospital.
History of past illness
He had a history of type 2 diabetes mellitus,hypertension,and dyslipidemia.
Personal and family history
The patient denied any family history of malignant tumors.
Physical examination
The patient was afebrile on admission.The Eastern Cooperative Oncology Group (ECOG) performance status (PS) was 2.Physical examination revealed scleral icterus and yellow skin.The patient’s abdomen was flat and non-tender,with no palpable masses.
Laboratory examinations
The results of laboratory blood tests revealed the following: Serum total bilirubin level: 8.4 mg/dL,conjugated bilirubin level: 6.2 mg/dL,aspartate aminotransferase: 141 U/L,alanine aminotransferase: 240 U/L,lactate dehydrogenase: 372 U/L,alkaline phosphatase: 447 U/L,gamma glutamyl transferase: 959 U/L,albumin: 3.3 g/dL,and prothrombin time: 99%.Carcinoembryonic antigen (CEA) was markedly elevated at 396 ng/mL.
Imaging examinations
A computed tomography (CT) scan demonstrated multiple hepatic masses with a thickened wall at the sigmoid colon (Figure 1).
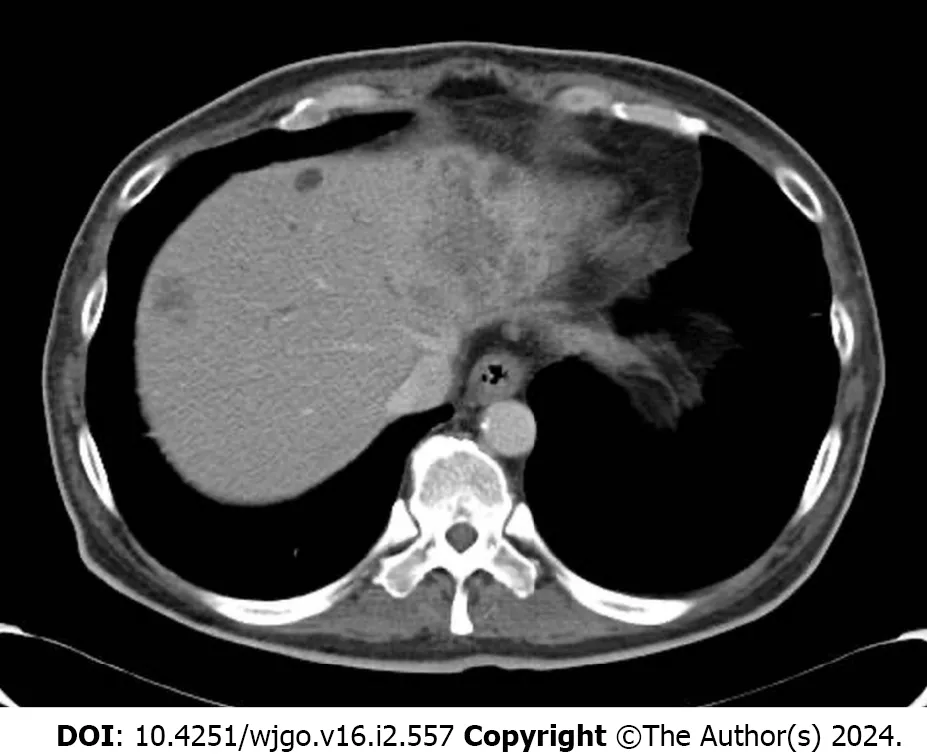
Figure 1 lmage of hepatic metastases on admission.Contrast-enhanced computed tomography scan showing multiple hepatic masses.
FlNAL DlAGNOSlS
Metastatic CRC was diagnosed,and obstructive jaundice with liver metastasis was suspected.Biomarker expression was as follows:RASwild-type,BRAFwild-type,and microsatellite stable.
TREATMENT
Endoscopic or percutaneous biliary drainage failed,owing to the diffuse involvement of the liver and the absence of a bile duct dilated enough to drain.These findings indicated the need for anticancer therapies.Consequently,panitumumab monotherapy (6 mg/kg,every two weeks) was initiated.
OUTCOME AND FOLLOW-UP
After two cycles of panitumumab monotherapy,the bilirubin level decreased markedly and completely normalized after four cycles (Figure 2).The patient’s ECOG PS improved to 0 and CEA levels decreased to 71 ng/mL.A CT tomography revealed shrinking hepatic masses (Figure 3).Therefore,fluorouracil plus leucovorin and oxaliplatin (a modified FOLFOX6 regimen) were added to panitumumab therapy.The patient received 22 cycles of this regimen over a year until the disease progressed.Thereafter,the patient declined further chemotherapy and received palliative care at a hospice.

Figure 2 Clinical course of the patient.Bilirubin and carcinoembryonic antigen levels markedly decreased after four cycles of panitumumab monotherapy.CEA: Carcinoembryonic antigen.
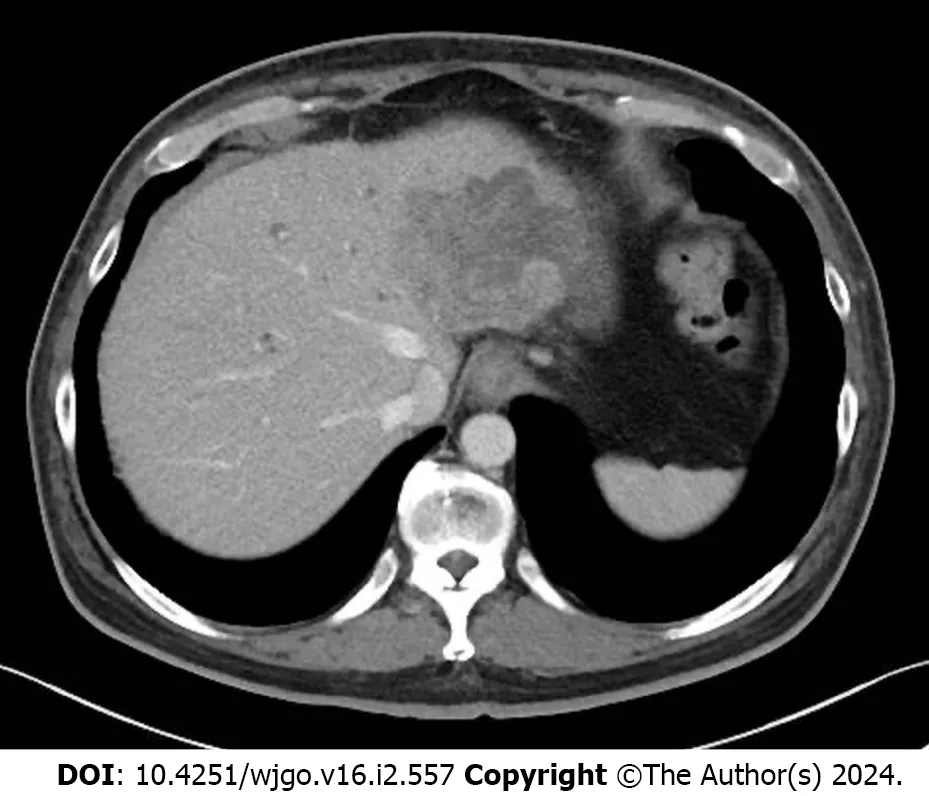
Figure 3 lmage of hepatic metastases after 4 cycles of panitumumab monotherapy. Contrast-enhanced computed tomography revealed decreased sizes of the hepatic masses.
DlSCUSSlON
Anti-EGFR antibody monotherapy was found to be a safe and effective treatment approach for patients withRASwildtype CRC and hepatic metastases with severe hyperbilirubinemia.
In general,selecting a chemotherapy regimen for hyperbilirubinemia is particularly challenging.This is because hepatic dysfunction affects the pharmacokinetics of chemotherapeutic agents and may worsen their toxicity.Cytotoxic agents against CRC include fluoropyrimidines such as oxaliplatin and irinotecan.Fluoropyrimidines are mostly eliminated by hepatic metabolism,and some experts have suggested that they are contraindicated in patients with severe hepatic dysfunction[3].Platinum derivatives are predominantly excreted through the renal tract.Although a doseescalating pharmacological study showed that oxaliplatin can be administered without dose reduction in patients with severe liver dysfunction,several cases of oxaliplatin-induced hepatotoxicity have been reported[4,5].Activation of irinotecan and detoxification of its metabolite,SN-38,occur predominantly in the liver;moreover,the toxicity of this drug may be increased in patients with reduced biliary excretion[5,6].
Recently,several studies have reported the use of cytotoxic chemotherapy in patients with hepatic metastases and severe hyperbilirubinemia[7-10].Some cases showed reasonable and durable responses;however,most had an average OS of only several months,and some experienced severe treatment-related adverse events.In addition,cytotoxic chemotherapy often requires dose reduction.This is a considerable concern,because intensive chemotherapy is required to achieve a sufficient response to alleviate hyperbilirubinemia[5,8].Furthermore,the PS of patients with severe hyperbilirubinemia is often poor at the time of diagnosis and progressively worsens,making them more vulnerable to chemotherapy toxicity.
By contrast,mAbs are mostly eliminatedviaintracellular catabolism,and are relatively unaffected by hepatic or renal functions[11].Anti-EGFR antibodies,such as panitumumab and cetuximab,are recommended as first-line treatments for patients withRAS/BRAFwild-type and left-sided CRCs[12,13].Although panitumumab is usually administered in combination with cytotoxic chemotherapy,monotherapy with this antibody has shown a reasonable response rate.Even in patients with refractory disease,the response rate reached 30% in those withRASwild-type CRC[14].Recently,the efficacy and safety of panitumumab monotherapy in frail or elderly patients who are considered unsuitable for intensive chemotherapy has been reported.One of these reports showed a considerably high response rate (up to 65%) toRASwild-type left-sided CRC as initial therapy[15].Several studies have supported the use of anti-EGFR monoclonal antibodies in patients with severe hyperbilirubinemia[5,16] (Table 1).

Table 1 Previous case reports of patients with colorectal cancer and hyperbilirubinaemia treated with anti-EGFR antibodies with or without cytotoxic agents
However,the role of anti-EGFR antibodies in patients with right-sided CRCs remains unclear.While patients with right-sided CRC do not benefit as much from anti-EGFR antibodies as those with left-sided CRC in the setting of first-line treatment,the use of anti-EGFR antibodies as a later treatment is a widely accepted approach[12].Thus,our approach to initial anti-EGFR monotherapy in the setting of severe hyperbilirubinemia requires careful consideration of right-sided CRC owing to its possible lower response rate[15].
Further studies should be conducted to validate this approach on both sides of the CRC.
CONCLUSlON
This case demonstrates the safety and efficacy of anti-EGFR antibody monotherapy in a patient with CRC and hepatic metastases with severe hyperbilirubinemia.Anti-EGFR antibody monotherapy should be considered a treatment option for patients withRASwild-type CRC with hyperbilirubinemia due to hepatic metastases when biliary drainage is impossible.
FOOTNOTES
Author contributions:Tsurui T designed the case report and drafted the manuscript;Hirasawa Y coordinated the study;Kubota Y revised the manuscript;Yoshimura K organized the manuscript;Tsunoda T supervised the manuscript;all authors have read and approve the final manuscript.
lnformed consent statement:Written informed consent for medical treatment was obtained from the patient.
Conflict-of-interest statement:The authors declare no conflicts of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Japan
ORClD number:Toshiaki Tsurui 0000-0002-6167-8953;Yutaro Kubota 0000-0002-2917-8764;Takuya Tsunoda 0000-0002-6416-8211.
S-Editor:Lin C
L-Editor:A
P-Editor:Yuan YY
 World Journal of Gastrointestinal Oncology2024年2期
World Journal of Gastrointestinal Oncology2024年2期
- World Journal of Gastrointestinal Oncology的其它文章
- Does enhanced recovery after surgery programs improve clinical outcomes in liver cancer surgery?
- Cardiotoxicity induced by fluoropyrimidine drugs in the treatment of gastrointestinal tumors
- Effect of screening colonoscopy frequency on colorectal cancer mortality in patients with a family history of colorectal cancer
- Preoperative controlling nutritional status as an optimal prognostic nutritional index to predict the outcome for colorectal cancer
- Tumour response following preoperative chemotherapy is affected by body mass index in patients with colorectal liver metastases
- Expression of cyclin-dependent kinase 9 is positively correlated with the autophagy level in colon cancer