
Prognostic nutritional index in predicting survival of patients with gastric or gastroesophageal junction adenocarcinoma: A systematic review
2024-03-07 08:18:52StylianosFiflisGrigoriosChristodoulidisMenelaosPapakonstantinouAlexandrosGiakoustidisStergosKoukiasParaskeviRoussosMarinaNektariaKouliouKonstantinosEleftheriosKoumarelasDimitriosGiakoustidis
Stylianos Fiflis,Grigorios Christodoulidis,Menelaos Papakonstantinou,Alexandros Giakoustidis,Stergos Koukias,Paraskevi Roussos,Marina Nektaria Kouliou,Konstantinos Eleftherios Koumarelas,Dimitrios Giakoustidis
Abstract BACKGROUND Gastric cancer is the third most common cause of cancer related death worldwide.Surgery with or without chemotherapy is the most common approach with curative intent;however,the prognosis is poor as mortality rates remain high.Several indexes have been proposed in the past few years in order to estimate the survival of patients undergoing gastrectomy.The preoperative nutritional status of gastric cancer patients has recently gained attention as a factor that could affect the postoperative course and various indexes have been developed.The aim of this systematic review was to assess the role of the prognostic nutritional index (PNI) in predicting the survival of patients with gastric or gastroesophageal adenocarcinoma who underwent gastrectomy with curative intent.AIM To investigate the role of PNI in predicting the survival of patients with gastric or gastroesophageal junction adenocarcinoma.METHODS A thorough literature search of PubMed and the Cochrane library was performed for studies comparing the overall survival (OS) of patients with gastric or gastroesophageal cancer after surgical resection depending on the preoperative PNI value.The PRISMA algorithm was used in the screening process and finally 16 studies were included in this systematic review.The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO).RESULTS Sixteen studies involving 14551 patients with gastric or esophagogastric junction adenocarcinoma undergoing open or laparoscopic or robotic gastrectomy with or without adjuvant chemotherapy were included in this systematic review.The patients were divided into high-and low-PNI groups according to cut-off values that were set according to previous reports or by using receiver operating characteristic curve analysis in each individual study.The 5-year OS of patients in the low-PNI groups ranged between 39% and 70.6%,while in the high-PNI groups,it ranged between 54.9% and 95.8%.In most of the included studies,patients with high preoperative PNI showed statistically significant better OS than the low PNI groups.In multivariate analyses,low PNI was repeatedly recognised as an independent prognostic factor for poor survival.CONCLUSION According to the present study,low preoperative PNI seems to be an indicator of poor OS of patients undergoing gastrectomy for gastric or gastroesophageal cancer.
Key Words: Prognostic nutritional index;Gastric adenocarcinoma;Gastroesophageal junction cancer;Prognosis;Overall survival
lNTRODUCTlON
Gastric cancer (GC) is one of the most common malignancies and the third most common cause of cancer-related deaths.In 2018,there were approximately 1033701 new cases of GC reported worldwide,resulting in 783000 associated deaths[1-3].Surgery with or without chemotherapy remains the cornerstone in the management,as it may have curative results.Despite advancements in surgical procedures,chemotherapy,radiotherapy,and targeted treatments,postoperative complications and mortality rates remain high,leading to a poor prognosis for patients[4].
Pathological characteristics such as tumor stage,nodal status,and resection margin are thought to be crucial in determining cancer patient survival[5].However,it is now obvious that tumor pathology is not the only factor that influences cancer survival;muscle mass,nutritional profile,immunological conditions,and other variables could significantly affect surgical outcomes[6,7].Malnutrition is particularly common among this group of patients and is attributed to inadequate oral intake,protein-losing gastropathy,ongoing bleeding due to tumors,and ineffective nutritional pathways.Numerous studies have revealed that malnutrition relates to a poor prognosis and multiple postoperative complications in cancer patients,as a result of worsening overall health and increased treatment challenges,emphasizing the need for proper perioperative management to improve the nutritional status of each individual[8-10].Therefore,early evaluation and management of a patient’s nutritional status may enhance the prognosis and outcomes for those undergoing curative surgery for GC[11].
Historically,tumor-node-metastasis (TNM) classification has been the most prevalent and reliable indicator for patient prognosis.However,there is an increasing number of cases where patients classified at the same stage exhibit significantly different prognoses[12,13].Recent studies have demonstrated that perioperative inflammation-based prognostic scores can predict overall survival (OS) in patients with diverse forms of cancer[14].Albumin levels are a key indicator of a patient’s nutritional status.Several scores based on albumin levels have been developed,such as the nutritional index (NI),Glasgow Prognostic Score,Nutrient Profiling System,and Controlling Nutritional Status score[11,15].The prognostic NI (PNI) has gained popularity as a means of predicting the surgical risk of patients with GC.It is calculated by multiplying 10 times the serum albumin value (g/dL) plus 0.005 times the lymphocytes count (/mm3).It utilizes nutritional and inflammation status instead of tumor growth,node invasion,and metastasis stage[1,16,17].PNI has been used as a prognostic tool for patients with solid organ tumors with significant prognostic value regarding survival and postoperative complications,paving the way for individualized perioperative management[12,17,18].In this systematic review,we aimed to assess the role of PNI in predicting the survival of patients undergoing curative intent surgery for gastric or gastroesophageal adenocarcinoma.
MATERlALS AND METHODS
Study selection
A thorough literature search of PubMed and the Cochrane library was conducted for articles comparing the OS of patients with gastroesophageal cancer after surgical resection depending on their preoperative PNI over the past 10 years.The terms “prognostic nutritional index”,“PNI”,“gastric cancer”,“gastroesophageal cancer”,“gastric adenocarcinoma”,and “survival” were used in various combinations.The PubMed search yielded 788 results that were scrutinized against the predetermined inclusion and exclusion criteria (Table 1).After title and abstract screening and exclusion of duplicates and irrelevant articles,71 were eligible for further assessment.After full text screening,finally 16 studies were included in our systematic review.The search and screening processes were completed by two independent reviewers using the PRISMA algorithm and any conflict was resolved through discussion (Figure 1)[19].The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO ID CRD42023461282).
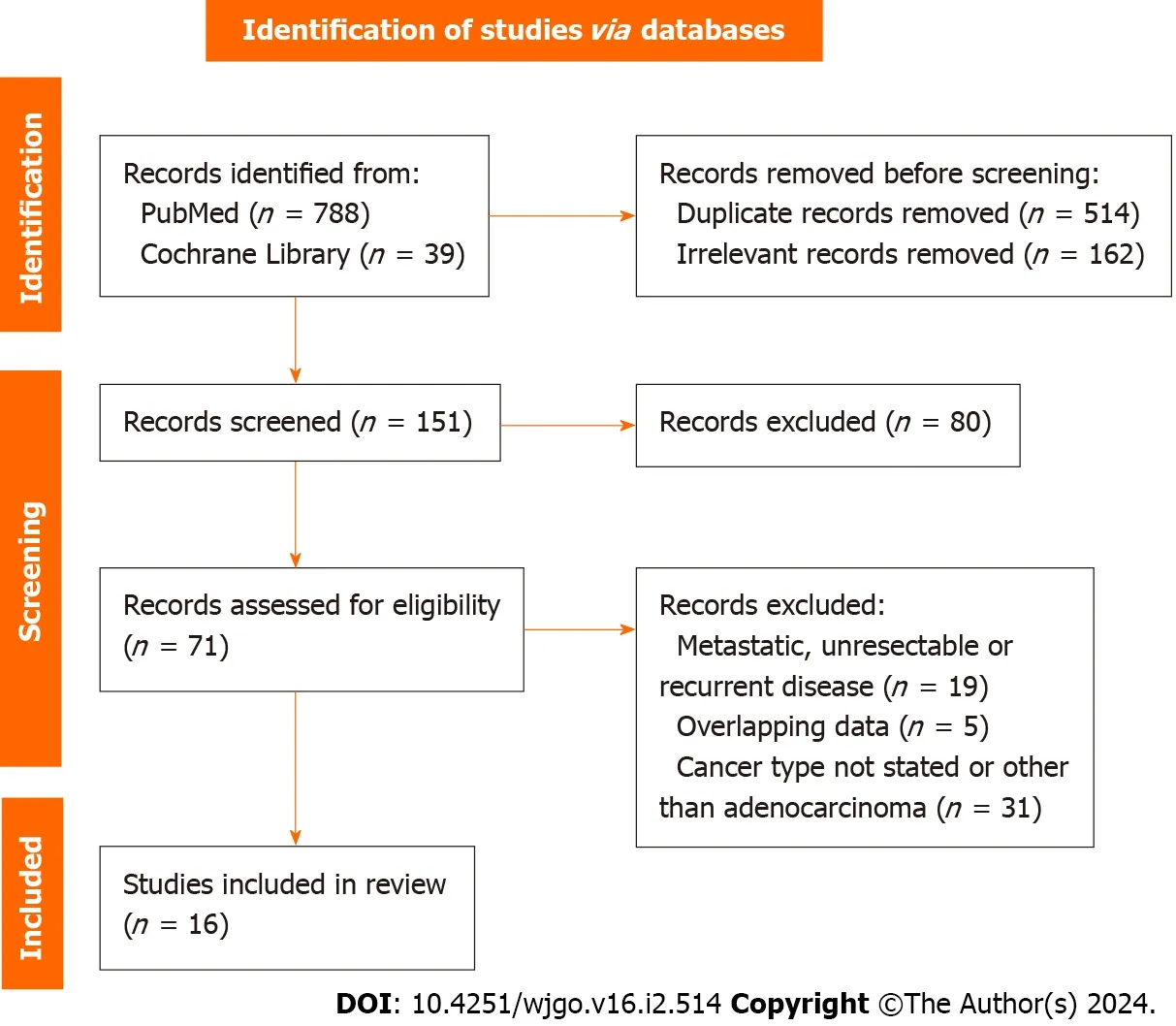
Figure 1 PRlSMA flowchart.
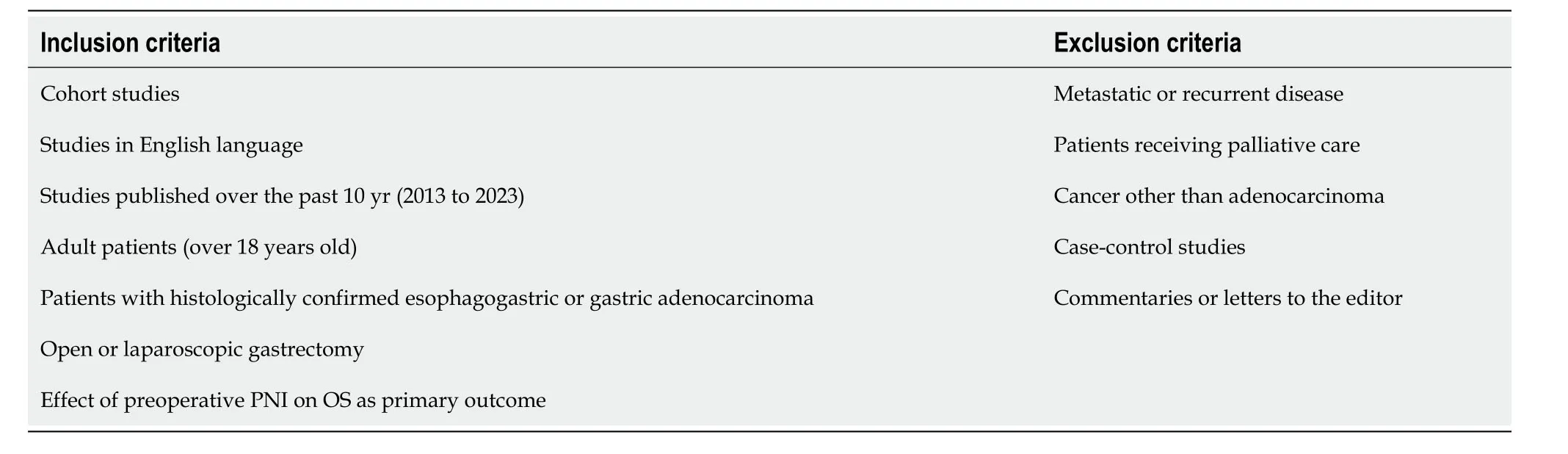
Table 1 lnclusion and exclusion criteria
Risk of bias and quality assessment
Only cohort studies were included in our systematic review.The risk of bias and the quality of each individual study were assessed using the Cochrane Tool to assess Risk of Bias in Cohort studies and the Newcastle-Ottawa quality assessment scale (NOS),respectively[20].The Cochrane Tool consists of seven questions and according to the answers a cohort study was categorized as of low or of high risk of bias.The NOS consists of three categories (Selection,Comparability,and Outcome) and eight items.A maximum of one star can be awarded for each item within the selection and outcome categories and a maximum of two stars for the comparability[1,12,13,15,17,21-31] (Table 2).A study with a score of over six stars is considered to be of high quality.
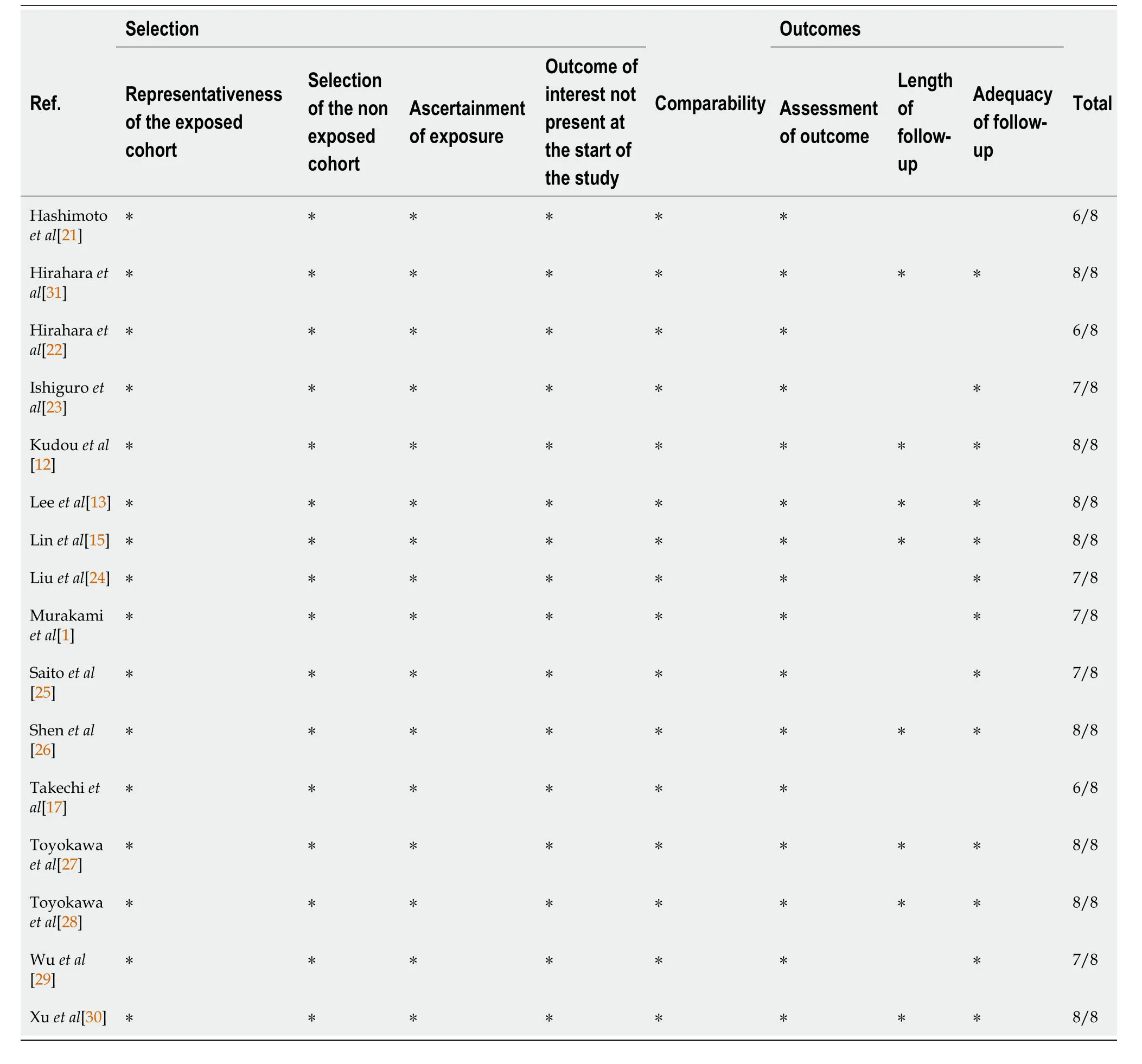
Table 2 Newcastle-Ottawa scale scores for the included studies

Table 3 lnstitute,period,and patient demographics
Data extraction
The following data were extracted: Year of publication,institution,study period,number of participants,patient diagnosis and operation,PNI cut-off value,patient age,sex,body mass index,albumin and lymphocyte count,tumor location and TNM stage,follow-up period,OS,and the univariate and multivariate analysis results.Data extraction was completed by four of the reviewers.Any disagreement during that phase was resolved by consulting a senior reviewer.
RESULTS
Sixteen studies involving 14551 patients with non-metastatic gastric or gastroesophageal adenocarcinoma who underwent surgery with curative intent between 1997 and 2021 were included in our systematic review.The clinical and pathological characteristics of the patients are shown in Tables 2 and 3.
The PNI cut-off values used in the studies and the survival outcomes are shown in Table 4.PNI was calculated as 10 × albumin (g/dL)+0.005 × total lymphocyte count (/mm3) and its thresholds ranged between 44.2 and 47 in the majority of the studies;however,three studies used the cut-off values 42.3,49.2,and 52,respectively.There were 10864 patients in the high PNI group and 3687 in the low PNI group.The patients were submitted to total or partial gastrectomy and lymphadenectomy with or without adjuvant or neoadjuvant chemotherapy.The primary endpoint of our study was OS and the results of univariate and multivariate analyses of the studies that were included are shown in Tables 5 and 6.
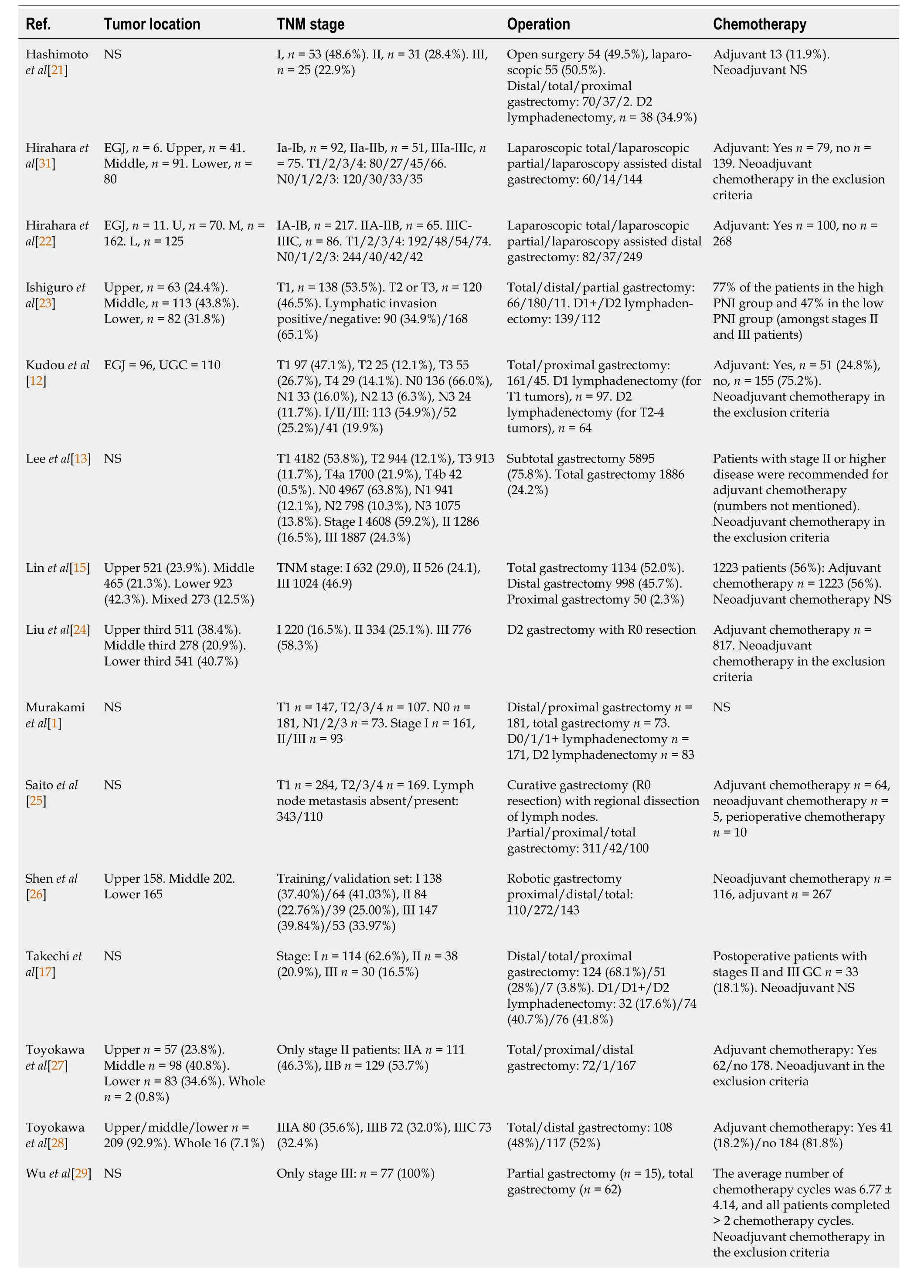
Table 4 Patient clinical characteristics

Table 5 Prognostic nutritional index cut-off value calculation method,threshold value and range,follow-up,and survival of the patients
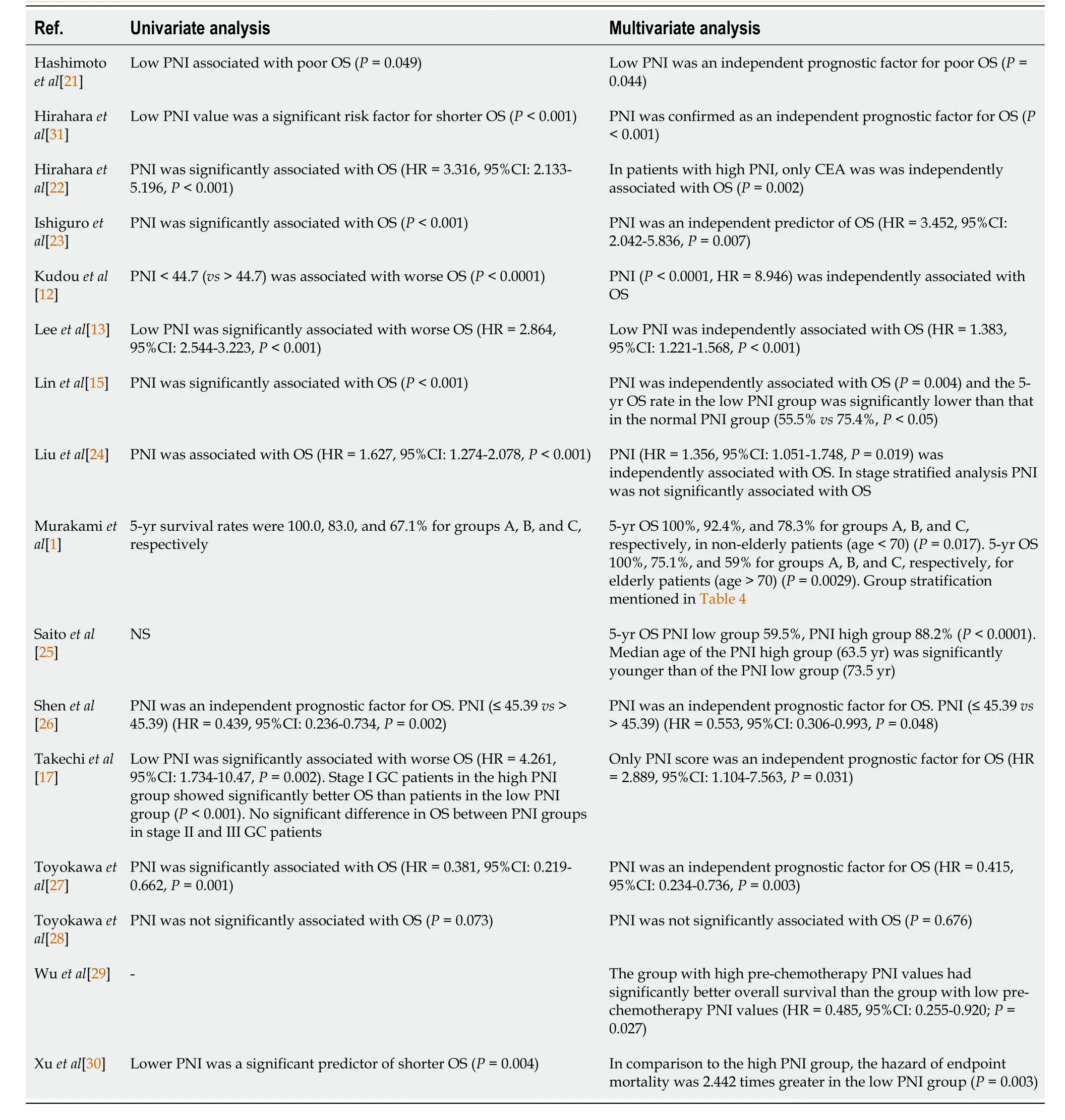
Table 6 Univariate and multivariate analysis results
OS
PNI was significantly associated with the OS in all of the studies included except for Toyokawaet al[27] enrolled 225 patients with stage III only gastric adenocarcinoma;184 of them were submitted to adjuvant chemotherapy and PNI was not associated with OS.Hiraharaet al[22] included 368 patients that were submitted to laparoscopic or laparoscopy assisted gastrectomy and 100 of them were also submitted to adjuvant chemotherapy.The authors demonstrated in univariate analysis that PNI was significantly associated with OS;however,the same result was not reached in multivariate analysis which showed that only carcinoembryonic antigen was significantly associated with OS.
Of 258 patients who underwent curative resection for GC and were included in Ishiguroet al[23]’s study,adjuvant chemotherapy was not administered to patients with stage I GC but only to patients with stage II or III.The authors demonstrated that PNI was independently associated with OS.
Linet al[15] included 632 patients with stage I GC,526 with stage II,and 1024 with stage III who underwent curative gastrectomy;56% of them received adjuvant chemotherapy.The authors showed that PNI was independently associated with OS.Saitoet al[24] included 111 GC patients with and 343 without lymphatic invasion;64 patients received adjuvant and 5 neoadjuvant chemotherapy.The authors demonstrated that high PNI was significantly associated with better OS.
Hashimotoet al[21] included only elderly patients between 80 and 94 years of age.Fifty-four of them were submitted to open surgery and fifty-five to laparoscopic surgery;however,it was not stated whether neoadjuvant chemotherapy was administered.The authors demonstrated that PNI was an independent prognostic factor for OS and reported a cumulative 3-year OS rate of 74.7%.Xuet al[30] included younger patients (mean age 43.68 ± 4.62) and they also showedthat low PNI was significantly associated with lower OS.
Shenet al[26] included 525 patients with stages I-III GC in their study who were submitted to robotic gastrectomy,116 of them to neoadjuvant chemotherapy and 267 of them to adjuvant chemotherapy,and they randomly divided the patients to a training and a validation set.The authors showed that PNI was significantly associated with OS in both sets and that PNI was an independent prognostic factor for OS.
Wuet al[29],Liuet al[24],and Toyokawaet al[27] also showed that PNI was significantly associated with OS.Of note,Wuet al[29] included only patients with stage III adenocarcinoma in their study.Toyokawaet al[28],who also included only stage III patients,demonstrated that PNI was not significantly associated with OS in those patients.In another study,which included stage II only GC patients,Toyokawaet al[27] showed that PNI was an independent prognostic factor for OS.Takechiet al[17] confirmed a significant association of PNI and OS only for stage I patients but not for stage II or III patients.Finally,Leeet al[13] and Kudouet al[12] showed that PNI was significantly associated with OS in stage-stratified analysis for stage I,stage II,and stage III gastric adenocarcinoma patients.
Murakamiet al[1] reported a 5-year OS rate of 70% and 95.8% in preoperatively low-and high PNI groups,respectively (P< 0.0001).In this study,postoperative PNI values were also recorded at 1 month after surgery.The authors demonstrated that the patients with preoperative and postoperative PNI higher than the threshold had a better 5-year OS (100%) compared to those who had preoperative or postoperative PNI lower than the threshold (5-year OS 83%) andcompared to the patients with preoperative and postoperative low PNI (5-year OS 67.1%).The authors also compared the 5-year OS rates of these groups in elderly (age over 70 years old) and non-elderly patients (age under 70 years old) and they reported lower OS rates for elderly patients (100%vs75.1%vs59% for elderly patients and 100%vs92.4%vs78.3% for non-elderly patients).Hiraharaet al[31] also examined the 5-year OS in low-and high-PNI groups in elderly and nonelderly patients.A greater difference in 5-year OS was reported between the low-and high-PNI groups in elderly patients (52.5%vs82.5%) compared to non-elderly patients (46.6%vs54.7%).
The next morning, I carried a bulging7 kitchen sack outside. My heart wrenched8 as I lifted the lid of the trash can and saw Susan s carpet lying among the other discarded items. Hesitating only a moment, I reached in and plucked it from amid the debris9. After giving it a light brushing, I brought it into the house and tucked it away in the hall closet. Overshadowed by the business of daily living, the carpet was soon forgotten.
DlSCUSSlON
In the present study,we assessed the role of PNI in the prognosis of patients with gastric or gastroesophageal junction cancer.However,there are discrepancies in the literature depending on cancer stage.For instance,according to Migitaet al[32],a low PNI is a significant predictor of poor OS in patients with GC at stages I and III,but not at stages II and IV.In the study of Sakuraiet al[33],a low PNI was found to be a negative prognostic factor in stages I and II,but not in stage III.This disparity could be explained by the fact that,in addition to cancer stage,other clinicopathological factors,including but not limited to patient’s age,nutritional status,or lymphatic or vessel invasion,could influence the survival of patients with different stages of GC[34-36].Of note,the data are still not conclusive as to whether PNI has better prognostic value in early or advanced GC stage[36-38].
Undoubtedly,there is a link between the nutritional status and the prognosis of patients with GC.Many studies have shown that malnutrition has a negative impact on the prognosis of cancer patients due to its effects on the immune system function resulting in impaired general health and increased treatment complications[9,36].PNI is a systemic inflammatory marker that has been shown to be useful in cancer prognosis.However,there has been little research into the impact of inflammation on the tumor microenvironment[15].It is unclear whether a low preoperative PNI is a cause or a result of tumor progression.A low preoperative PNI,according to a meta-analysis of Liet al[39],was significantly associated with poor OS,as well as increased postoperative mortality.Therefore,assessing nutritional status is critical because it allows for the identification of malnourished patients at high risk and the implementation of appropriate nutritional interventions that could possibly improve prognosis and reduce complications.However,Migitaet al[40] showed that preoperative oral nutritional supplementation did not improve low preoperative PNI,therefore more research needs to be done regarding the optimal means of preoperative nutritional support.
The PNI cut-off values varied between the studies that were included in this systematic review and the methods that were used to calculate the PNI cut-off value are mentioned in Table 4.An optimal cut-off value for predicting long-term outcomes has not been established in the literature[36].Future research should focus on standardizing the PNI thresholds by performing receiver operating characteristic curve analysis in prospective studies that include patients with minimum clinicopathological characteristics heterogeneity in order to identify the PNI cut-off value with the maximum sensitivity and specificity,as a standardized PNI cut-off value may have significant impact in daily clinical practice and decisionmaking.For instance,in the study of Kosugaet al[41],it was shown that preoperative PNI may help clarify the extent of lymphadenectomy in patients undergoing gastrectomy for GC.
In our study,there are some limitations that need to be addressed.First,all of the included studies were retrospective cohort studies,which are prone to selection or recall bias.Furthermore,not all patients included in this study had the same stage of cancer.Also,some of them received neoadjuvant therapy prior to surgery,which possibly affected the overall course of the disease.Patients were not divided according to specific tumor characteristics,such as the TNM stage,the size or depth or the tumor,the Siewert type,or the tumor differentiation,therefore a correlation between the PNI and the survival depending on the multiple tumor characteristics could not be established.It would be of interest if future studies would stratify patients and assess the prognostic significance of the PNI based on those characteristics.Due to high heterogeneity of the recorded data,a meta-analysis could not be performed.Of note,the fact that not all deaths were confirmed cancer-related deaths is something to take into account.Furthermore,the studies that we included in our study were all performed in Eastern Asia countries and there were no studies performed in Western countries that matched our inclusion criteria.This could be attributed to the fact that East Asia has the highest prevalence of GC (20-25 patients per 100000,less than 5 patients per 100000 in Northern America)[42].Finally,patients underwent operations in different institutions by different surgical teams of variable experience,which may have had an impact on the postoperative events.
CONCLUSlON
In conclusion,all of the studies that we included showed that patients with higher preoperative PNI demonstrate better survival than those with lower PNI after surgery for gastric or gastroesophageal cancer with or without chemotherapy regardless of the tumor stage,patients age,total or partial gastrectomy,and open or laparoscopic gastrectomy,except for one study that included stage III GC patients.Future studies should focus on stratifying patients based on tumor stage,as well as on standardizing the PNI cut-offs.Moreover,more research needs to be done in terms of preoperative nutritional support as it could increase PNI and therefore improve short-and long-term outcomes.Moreover,more studies should be performed in Western countries in order to examine whether the association between PNI and survival persists in those patients who undoubtedly present different genetic factors.Finally,PNI could be a useful clinical tool,as it is easy to calculate with standard everyday labs and may lead to individualized patient care and clinical decisions with optimal results.
ARTlCLE HlGHLlGHTS
Research background
Gastric cancer (GC) is a major health problem worldwide.Patients with GC that are eligible for surgery are submitted to gastrectomy with lymphadenectomy followed or not by adjuvant chemotherapy.It is important to identify prognostic factors that could predict the survival of those patients.The prognostic nutritional index (PNI) is an indicator of the nutritional and immune status of GC patients that could assist in identifying patients that will benefit the most from being submitted to surgery and that will present better survival rates.
Research motivation
GC patients with high preoperative PNI seem to present higher survival rates than those with lower PNI.PNI is easy to calculate and low-cost but in order to be used in everyday clinical practice,future research should be conducted to establish a standardized PNI threshold for GC patients that could be submitted to surgery.
Research objectives
Research methods
We performed a thorough literature search of PubMed,the Cochrane library,andReference Citation Analysisfor cohort studies that included patients with gastric adenocarcinoma who were submitted to gastrectomy.The keywords that we used for our search were “Prognostic nutritional index”,“survival”,and “gastric cancer” in combinations,which lead to the retrieval of 16 studies that matched our inclusion criteria.We performed risk of bias assessment and quality assessment of each individual study and our study was prospectively registered in PROSPERO.
Research results
Our systematic review showed that the PNI could be an important prognostic marker in patients undergoing surgery for gastric adenocarcinoma.All of the studies that we included demonstrated that preoperative PNI is significantly associated with survival in GC patients except for one study which included stage III only gastric adenocarcinoma patients.However,two of the studies that we included showed that PNI is significantly associated with survival in patients with stage III gastric adenocarcinoma.Further studies should aim to identify a standardized PNI threshold for gastric adenocarcinoma patients.Moreover,future studies should analyze the correlation between PNI and the stage of disease and whether PNI is associated with survival regardless of the disease stage.
Research conclusions
PNI could be an important prognostic marker that could assist in predicting the survival of patients submitted to gastrectomy.
Research perspectives
Future research should aim at identifying a standardized PNI cut-off value.Furthermore,the correlation between PNI and tumor stage,Lauren classification,and patients’ clinicopathological characteristics should be analyzed.
FOOTNOTES
Author contributions:Fiflis S and Papakonstantinou M contributed equally to this work and wrote most of the manuscript;Fiflis S,Papakonstantinou M,and Giakoustidis A designed the research study,performed the research,and analyzed the data;Christodoulidis G offered guidance and assisted as the corresponding author;Koukias S and Roussos P assisted in writing part of the Results and Discussion sections;Kouliou MN and Koumarelas KE assisted in writing part of the Introduction section;Giakoustidis A and Giakoustidis D offered guidance,assisted in writing part of the Discussion section,and performed manuscript revisions;and all authors have read and approved the final manuscript.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
PRlSMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Greece
ORClD number:Stylianos Fiflis 0000-0003-0427-6859;Grigorios Christodoulidis 0000-0003-3413-0666;Menelaos Papakonstantinou 0000-0001-5030-7009;Alexandros Giakoustidis 0000-0002-3786-4609;Stergos Koukias 0009-0001-6443-548X;Paraskevi Roussos 0009-0005-2986-8043;Marina Nektaria Kouliou 0000-0002-2055-2297;Konstantinos Eleftherios Koumarelas 0000-0002-5614-4770;Dimitrios Giakoustidis 0000-0002-6023-4744.
S-Editor:Wang JJ
L-Editor:Wang TQ
P-Editor:Yu HG
 World Journal of Gastrointestinal Oncology2024年2期
World Journal of Gastrointestinal Oncology2024年2期
- World Journal of Gastrointestinal Oncology的其它文章
- Does enhanced recovery after surgery programs improve clinical outcomes in liver cancer surgery?
- Cardiotoxicity induced by fluoropyrimidine drugs in the treatment of gastrointestinal tumors
- Effect of screening colonoscopy frequency on colorectal cancer mortality in patients with a family history of colorectal cancer
- Preoperative controlling nutritional status as an optimal prognostic nutritional index to predict the outcome for colorectal cancer
- Tumour response following preoperative chemotherapy is affected by body mass index in patients with colorectal liver metastases
- Expression of cyclin-dependent kinase 9 is positively correlated with the autophagy level in colon cancer