
Effects of fentanyl and sucrose on pain in retinopathy examinations with pain scale,near-infrared spectroscopy,and ultrasonography:a randomized trial
2023-11-29 13:47NursuKaraDidemArmanZeynepSeymenAdemSerdarmert
World Journal of Pediatrics 2023年9期
Nursu Kara · Didem Arman · Zeynep Seymen · Adem Gül · Serdar Cömert
Abstract Background This study aimed to compare the efficacy of intravenous,intranasal fentanyl and oral sucrose in reducing the pain response during retinopathy of prematurity examinations using premature infant pain profile (PIPP) scores.Method The study included 42 infants who underwent retinopathy screening examinations.The infants were divided into three groups: oral sucrose,intranasal fentanyl,and intravenous fentanyl.Vital signs (heart rate,arterial oxygen saturation,and mean arterial pressure) were recorded.The PIPP was used to determine pain severity.Cerebral oxygenation and middle cerebral artery blood flow were evaluated using near-infrared spectroscopy and Doppler ultrasonography,respectively.The data obtained were compared between groups.Results There was no significant difference between the three groups regarding postconceptional and postnatal ages or birth weights and weight at the time of examination.All babies had moderate pain during the examination.No correlation was observed between analgesia method and pain scores (P =0.159).In all three groups,heart rate and mean arterial pressure increased,whereas oxygen saturation decreased during the exam compared with pre-examination values.However,heart rate (HR),mean arterial pressure (MAP) and arterial oxygen saturation (sPO 2) values did not differ between groups (HR,P =0.150;MAP,P =0.245; sPO2,P =0.140).The cerebral oxygenation (rSO2) values between the three groups were found to be similar [rSO2 : P =0.545,P =0.247,P =0.803;fractional tissue oxygen extraction (FTOE): P =0.553,P =0.278].Regarding cerebral blood flow values,we also did not find any difference between the three groups [mean blood flow velocity (Vmean): P =0.569,P =0.975;maximum flow velocity (Vmax): P =0.820,P =0.997].Conclusions Intravenous and intranasal fentanyl and oral sucrose were not superior to each other in preventing pain during the examination for retinopathy of prematurity (ROP).Sucrose may be a good alternative for pain control during ROP examination.Our findings suggest that ROP exam may not affect cerebral oxygenation or cerebral blood flow.Larger scale studies are needed to determine the best pharmacological option to reduce pain during ROP exams and evaluate the effects of this procedure on cerebral oxygenation and blood flow.
Keywords Analgesia · Cerebral blood flow · Cerebral oxygenation · Neonate · Retinopathy of prematurity
Introduction
Newborn babies initially perceive pain with the development of communication between the cortex and thalamus after the 20th gestational week,and the fetus senses pain starting from the second trimester [1].Babies provide physiological,behavioral,and hormonal responses to pain [2].Newborns hospitalized in the neonatal intensive care unit(NICU) experience various repetitive painful interventions,such as heel blood sampling,insertion of nasogastric tubes,and intubation.Ineffective pain control may cause neurological,cognitive,and behavioral problems as a long-term consequence.Hence,it is crucial to evaluate and manage the pain status of infants [3–6].
Retinopathy of prematurity (ROP) exam is a painful critical procedure that newborns experience in the NICU.There are many studies comparing the effectiveness of nonpharmacologic and pharmacologic methods in pain control during exam and laser treatment [7–9].However,there is still no consensus on the methods to be used for pain control in preterm babies during ROP examinations [10–13].
During ROP examinations,physiological responses such as an increase in heart rate,respiratory rate,blood pressure,and intracranial pressure and a decrease in oxygen saturation are observed in infants as a result of pain [14–17].These changes are not specific to pain alone and should be evaluated together with the behavioral state [18–21].Many studies have compared methods to prevent pain during ROP examinations using pain assessment scales [8–10,22,23].
Near-infrared spectroscopy (NIRS) and Doppler ultrasonography (US) are non-invasive methods commonly used for neuromonitoring in NICUs.Doppler US is a very sensitive imaging technique for assessing changes in cerebral blood flow.The regional blood flow changes measured using Doppler US have been reported to be associated with cerebral oxygenation and indicate a high correlation with NIRS in newborns [24].In recent years,the use of NIRS has gained importance in evaluating evoked cerebral activation in response to pain and determining tissue oxygenation variability during pain [25–27].
There is still no consensus on the method of pain control among preterm infants during ROP examination.Data on the effects of widely used methods for pain control on vital signs,cerebral blood flow and oxygenation are limited.By comparing these three methods,we aimed to investigate a relatively effective and less invasive method to be used in pain control.
This study was conducted to compare the effectiveness of intravenous,intranasal fentanyl and oral sucrose treatments in reducing pain response during ROP examination using the PIPP scale.We also evaluated the effects of ROP examination on cerebral blood flow and oxygenation.
Methods
This randomized,double-blind trial was conducted in a level III NICU between October 2020 and October 2021.Ethics committee approval was obtained from the Clinical Research Ethics Committee of our hospital (Decree no: 2741).Written informed consent was collected from the parents of all infants included in the study.
Forty-two infants with a gestational age below 34 weeks and/or a birth weight of less than 2000 g who had no need for respiratory support at the time of the examination and who underwent the initial retinopathy screening examination were included.The patients were randomized into three groups according to the type of analgesia used during the examination: the sucrose,intranasal and intravenous fentanyl groups,using a web-based randomization program (Group 1:sucrose,Group 2: intranasal fentanyl,Group 3: intravenous fentanyl).Since the use of analgesics is strongly advised for pain control during ROP exams,we did not include a control group for ethical reasons.The exclusion criteria were as follows: congenital anomaly,hemodynamic instability,intraventricular hemorrhage,mechanical ventilation support,anticonvulsant therapy and/or analgesics for pain or a different indication.
Physiologic responses [heart rate (HR),arterial oxygen saturation (sPO2),mean arterial pressure (MAP)] were monitored,and premature infant pain profile (PIPP) pain scores,cerebral NIRS,and middle cerebral artery flow changes in Doppler US were measured and recorded before,during,and after ROP examination.The results were compared statistically.The patients’ demographic data were recorded from the medical files.
Routine screening and follow-up examinations for ROP were performed in accordance with the guidelines of the American Academy of Pediatrics,the American Academy of Ophthalmology,and the American Association for Pediatric Ophthalmology and Strabismus [28].
Study interventions
Ophthalmologic examination
For pupil dilation,one drop of 2.5% phenylephrine and 0.5%tropicamide was instilled three times at five-min intervals one hour before the examination.Two minutes before the examination,the analgesic substance (1 mL/kg 24% oral sucrose,2 μg/kg intranasal fentanyl,1 μg/kg intravenous fentanyl) determined according to randomization was administered by the neonatal nurse.The researchers and the examining ophthalmologist were blinded to the analgesia to be applied and the method of administration.The examination was performed with 20 and 28 diopter lenses using a binocular indirect ophthalmoscope.Eyes were kept open using a sterile eyelid speculum,and the retina was evaluated in different eye positions with a scleral depressor.The examination was performed by a single ophthalmologist (ZS) who was experienced in ROP examinations.The baby was held still by a neonatal nurse during the examination.
Physiological changes
Significant changes were observed in vital signs during retinopathy examination.The most frequently affected vital signs during retinopathy examination are heart rate,arterial oxygen saturation,and blood pressure [23,29–31].Vital signs (heart rate,oxygen saturation,and mean arterial pressure values) were recorded continuously,starting 60 minutes before the procedure,during the procedure,and until 60 minutes after examination.During monitoring,data were recorded on the device continuously.Then,these data were transferred for evaluation through a program compatible with the device.The results given as “before” were calculated as an average of 60 minutes before the procedure.To calculate the result given as “during”,we evaluated the data starting from the marker set at the beginning of the examination to the marker set at the end of the examination.While the result given as “minute 0” was calculated as an average of data recorded within two minutes after the procedure;the 30th minute and 60th minute were calculated as an average of data recorded at 30 ± 2 minutes and 60 ± 2 minutes after examination,respectively.
Premature infant pain profile (PIPP)
Video recordings were shot for two minutes before and after the examination to assess behavioral changes.Two neonatologists (NK,DA) independently determined PIPP scores by evaluating the images.The PIPP was selected,because it is the most frequently and validated tool used to measure pain related to ROP eye examination [12,32–35].The PIPP scale evaluates seven parameters,such as gestational age,heart rate,lowest oxygen saturation value,forehead wrinkling,squinting and widening of the nose wings,and behavioral status.Each item is scored as 0,1,2,and 3 points (33).Physiologic variables followed using a monitor were recorded by the researcher.The baby's pain was evaluated according to the total pain score.Pain was considered mild,moderate and severe if the PIPP score was between 0–6 points,7–12 points and 13–21 points,respectively.
Near-infrared spectroscopy (NIRS) measurements
Regional oxygen saturation (rScO2) was measured using NIRS (INVOS 5100;Covidien Somanetics,Troy,MI).Cerebral tissue oxygenation was monitored using the probe attached to the forehead skin.Data were recorded 60 minutes before the pre-examination preparation (before the instillation of eye drops for pupil dilation) began.The recording was continued without interruption during the examination and until 1 hour after the examination.The baseline value was recorded before the preparation process started.A marker indicating the interventional status was placed on the NIRS monitor at the beginning and at the end of the examination.
rScO2was recorded before,during,and after the examination.Fractional tissue oxygen extraction (FTOE)was calculated using the arterial oxygen saturation value measured using pulse oximetry simultaneously (FTOE:SpO2− rScO2/SpO2).
NIRS data recording was started 60 min before the examination.The average of the data was calculated and accepted as the rScO2value before the examination.The average of the data recorded during the examination was accepted as the rScO 2 value during the examination.After the examination,averages of rScO 2 values between minute 0 and the 2nd minutes,0 and the 30th minutes,and the 30th–60th minutes were taken.Additionally,0,30th,and 60th minute rScO2values after the examination were recorded by calculating the averages of 0 ± 2 minutes,30 ± 2 minutes,and 60 ± 2 minutes values,respectively.All NIRS data were stored for later of f-line analysis.
Doppler ultrasonography measurements
Flow imaging and blood flow velocities were obtained using a color Doppler unit (Philips En Visor C HD ultrasound,Royal Philips Electronics,Amsterdam,the Netherlands).A multifrequency 12-MHz sector probe was used.Two investigators who were blinded to the previous results performed all measurements.The authors had a training course on cranial ultrasonography,including Doppler ultrasonography.A minimum of three sequential homogenous cardiac cycles of optimal quality were subjected to real-time spectral analysis to maintain accuracy.
The infants underwent blood flow analysis just before and after the ocular examinations.Mean velocity measurements were made through the left and right middle cerebral arteries (MCAs).Doppler flow measurements of the MCA were performed by scanning through the sphenoid fontanelle (temporal window).The transducer was placed above the ear,1 cm superior and anterior to the external auditory meatus,posterior to the orbit and zygomatic arch,with the marker in a horizontal position [36].The angle between the US beam and the direction of blood flow was kept below 15° [37].Peak systolic flow velocity (PSV) and mean flow velocity (MV) were measured.Doppler US measurements were made while the babies were in the supine position in the incubator 30 minutes before the intervention,just before,and 5 minutes after the intervention.
Randomization
Stratified block randomization was used in this study.Stratification was based on the type of analgesia.Randomization was generated from a website (http:// www.rando mizat ion.com).The person who generated the random sequence was not involved in any other aspect of the trial.
Allocation concealment and blinding
The drugs were prepared by the Clinical Pharmacy Department in our institution.The drugs were prepared and serially numbered in one-mL volumes.The drugs were prepared in opaque vials with similar color and viscosity.The investigators who made all measurements and examinations and the pharmacists were blinded.
Study outcomes
The primary outcome measure of the study was variation in PIPP score and crying time regarding the type of analgesia used before the ROP exam.The secondary outcome measure was absolute change in rScO2 and MCA blood flow measurements before and after the examination with NIRS and Doppler US,respectively. Apnea was accepted as an adverse event,and those infants’ data were not analyzed.All subjects were followed until discharge or death,whichever was earlier.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Sample size estimation and statistical analyses
Since there are no reported data about the effects of fentanyl and sucrose on pain in ROP examination using NIRS and Doppler US,we calculated the power analysis on the basis of previous studies on PIPP scores.The primary outcome measure of our study was absolute change in PIPP score and crying time.In the background of a pre-existing standard pain management practice,we considered a threepoint reduction in the PIPP score during ROP examination between groups to be clinically significant.To detect this difference in the score,assuming a standard deviation of 2 and a 10% attrition rate,we estimated a sample size of 13 patients in each group to achieve a study power of 95% and a 5% two-sided significance level [12,38,39].
Statistical analysis was performed using SPSS 22.0 software.Compliance of the variables with normal distribution was examined through visual (histogram and probability charts) and analytical methods (Shapiro–Wilk test).Descriptive statistics were expressed as the mean ± standard deviation (SD) for the normally distributed variables.The paired-sample t test was used to compare the data before and after treatment because FTOE and NIRS values were normally distributed.Correlation coefficients and statistical significance were calculated using the Pearson test.P<0.05 values were considered statistically significant.
Results
A total of 47 neonates were screened for eligibility,of whom 42 met the eligibility criteria and were randomized(Fig. 1).No difference in adverse outcomes was observed between the groups.
The patients' gestational age,birth weight,postnatal and postconceptional ages,weights,and gender were not significantly different between groups (Table 1).
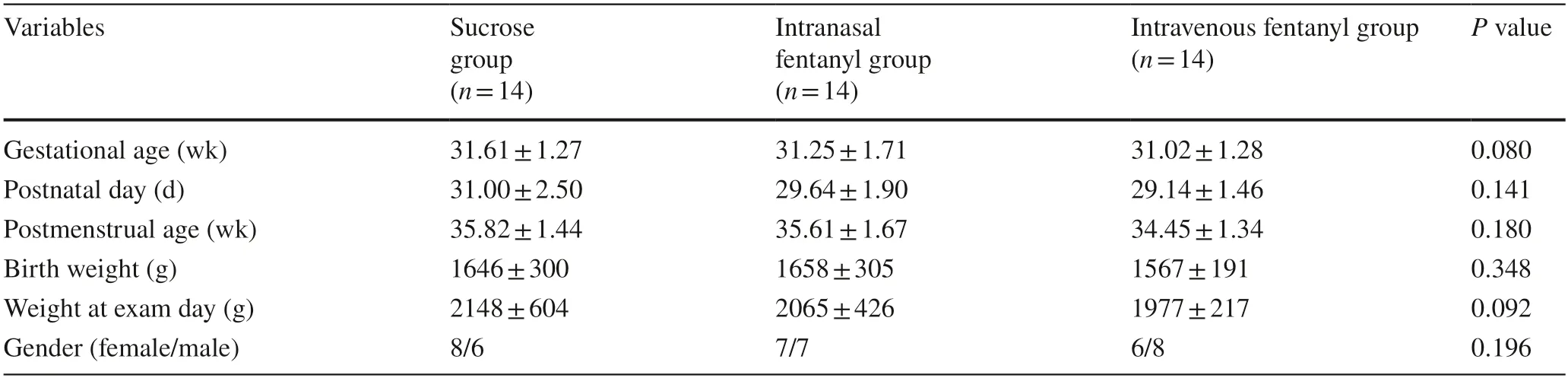
Table 1 Demographic data of patients
Vital signs
When the vital signs before vs.during the examination were evaluated for each group,HR and MAP values were significantly increased and SpO2was significantly decreased for sucrose,intranasal fentanyl and intravenous fentanyl groups(HR,P=0.02,P=0.02,P=0.03;MAP,P<0.01,P<0.01,P=0.04; SpO 2,P=0.029,P=0.01,P=0.027,respectively).We found that while HR and MAP decreased,SpO 2 increased after the examination as a physiological response(HR:P<0.01,P<0.01,P<0.01;MAP:P=0.07,P=0.038,P=0.003; SpO2:P=0.016,P=0.002,P=0.004,respectively).Before,during,and at minute 0,the 30th and 60th minute after the examination,no difference was observed between the three groups regarding HR,SpO2and blood pressure measurements (Table 2).Since the power calculation was not designed for comparison of these parameters,the conclusion is limited.
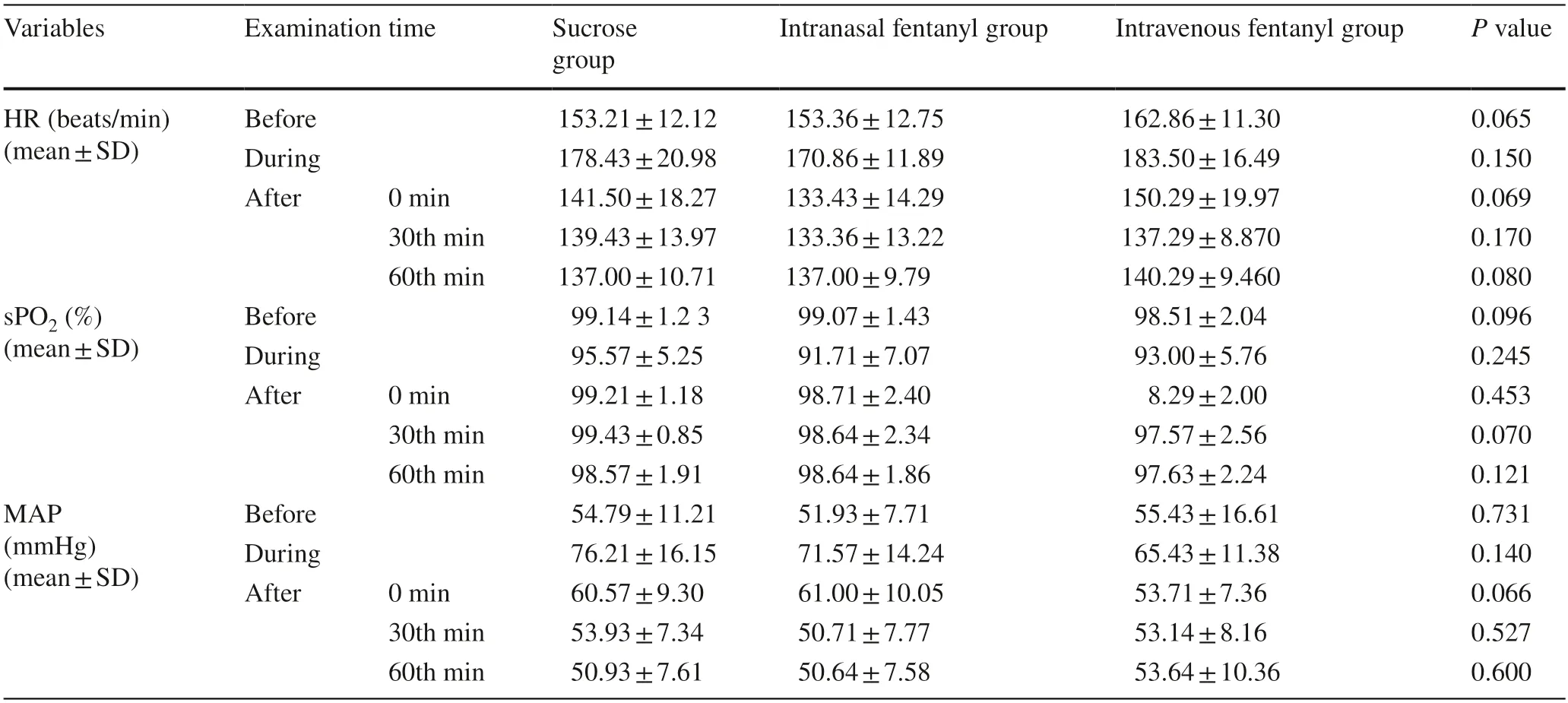
Table 2 Heart rate,oxygen saturation,mean arterial blood pressure values before,during,and after retinopathy examinations
PIPP score
All of the infants administered sucrose,intranasal fentanyl,or intravenous fentanyl experienced moderate pain during the examination.There was no statistically significant difference between the groups in terms of pain severity(P=0.159).Crying duration was also similar between the three groups (P=0.407) (Table 3).

Table 3 PIPP scores during retinopathy examination,duration of cry,examination time
Variation in tissue oxygenation (NIRS values)
When three groups were compared,no difference was determined in cerebral NIRS rScO2measurements before,during,and after (at minute 0,and the 30th and 60th minutes) the examination (P=0.545,P=0.275,P=0.803,P=0.170,P=0.332,respectively).Fractional tissue oxygen extraction values were similar between the three groups before,during,and after (at minute 0 and the 30th and 60th minutes) the examination (P=0.553,P=0.278,P=0.800,P=0.292,P=0.335,respectively)(Table 4).
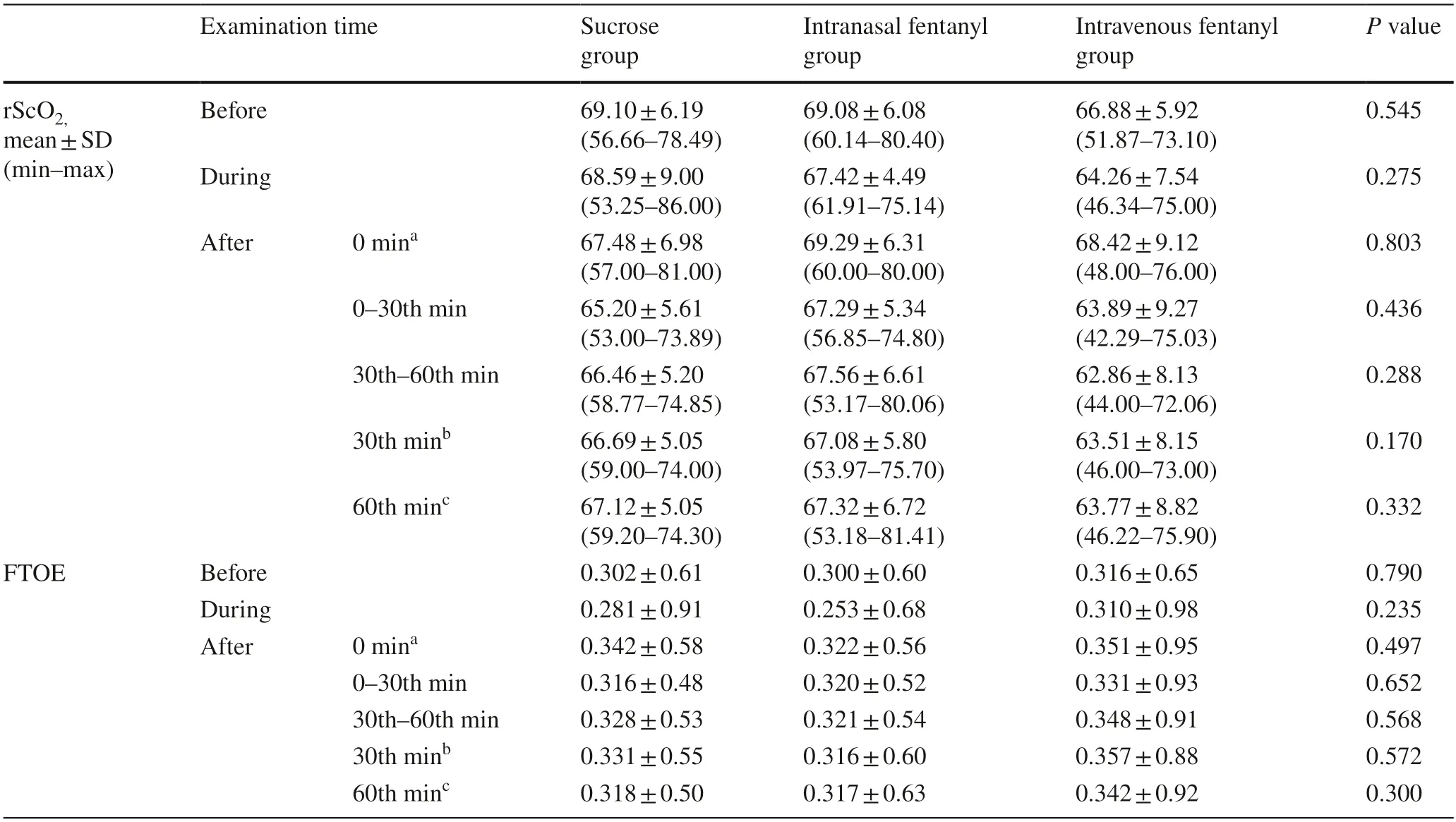
Table 4 Regional oxygen saturation and cerebral FTOE values before,during,and after retinopathy examination
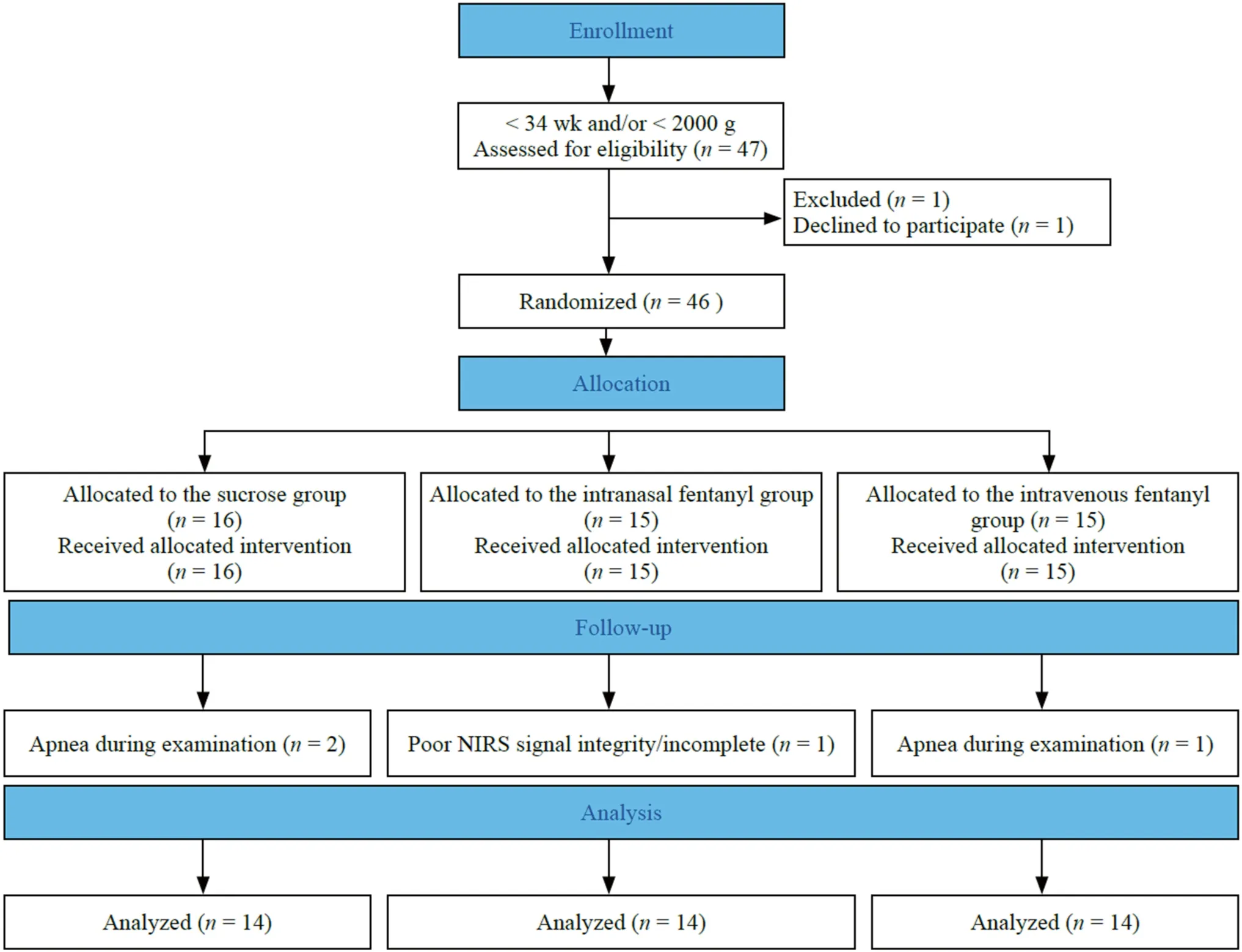
Fig.1 Flow diagram of the study
Middle cerebral artery blood flow changes
Regarding MCA blood flow measurements,no statistically significant difference was observed in Vmax and Vmean measurements before or after the examination between the three groups (Vmax,P=0.820,P=0.997;Vmean,P=0.569,P=0.975,respectively) (Table 5).
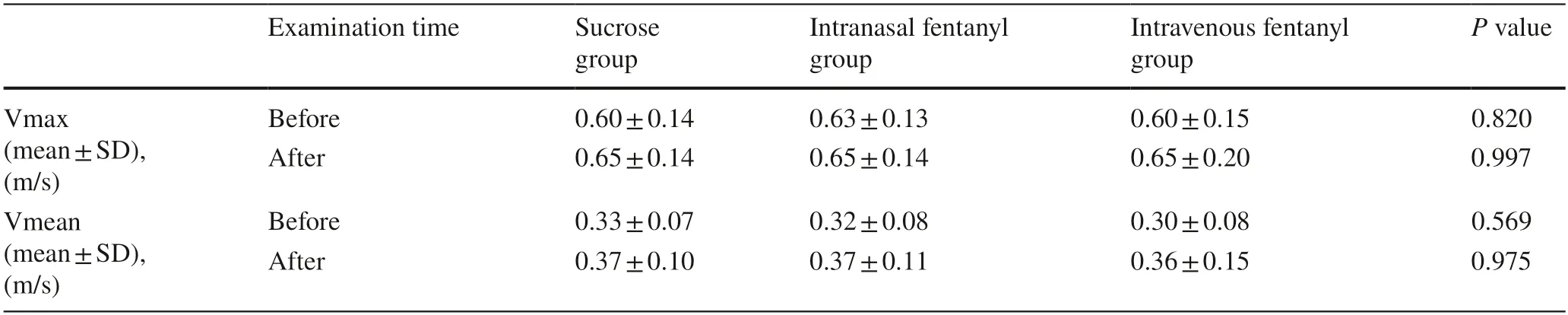
Table 5 Blood flow velocity measurements before and after retinopathy examinations
Discussion
In this study,although moderate pain was detected during the exam in all three groups,there was no significant difference in pain severity between groups.We determined an increase in heart rate and mean blood pressure and a decrease in oxygen saturation values duringthe retinopathy exam.The cerebral oxygenation values between the three groups were found to be similar.Regarding cerebral blood flow values,no difference was found among the three groups.
During ROP exams,which are painful procedures newborns are exposed significant changes in vital signs are observed [40–42].Rush et al.demonstrated a significant increase in heart rate and a decrease in oxygen saturation in infants who underwent ROP examinations,but no significant changes in blood pressure,body temperature,or respiratory rate were observed [29].Tan et al.found that the heart rate increased significantly during ROP examinations and returned to normal values two minutes after the procedure,but no significant change was observed in SpO2values[14].Jang et al.evaluated vital sign changes during ROP examinations and showed that heart rate and oxygen saturation values were significantly affected in babies given breast milk,sucrose,and distilled water.However,there was no significant difference between the three groups [23].Grabska et al.also compared the effects of sucrose and sterile water during the procedure and showed a significant increase in heart rate and blood pressure values and a decrease in oxygen saturation but found no difference between groups in terms of vital signs [30].In this study,we concluded that vital signs were significantly affected by the ROP exam,but there was no significant difference between groups regarding the type of analgesia applied.
It is recommended to use scoring systems that include physiologic and behavioral changes in evaluating pain in newborns [19,21,32].In many studies,while an increase in PIPP pain scores was determined during ROP examination,inconclusive results were reported regarding the effect of various pharmacologic and non-pharmacologic methods on pain scores [8–10,22,23].Nayak et al.evaluated pain severity during ROP examinations by comparing three groups given 10% dextrose,expressed breast milk,and sterile water,and they showed that all babies experienced moderate pain.Nevertheless,there was no significant difference in analgesic efficiency between the groups [9].Nesargi et al.compared the effectiveness of oral 25% dextrose and topical proparacaine and concluded that these did not provide effective analgesia during ROP screening [43].In another study,the effects of non-nutritive sucking,oral sucrose,and sterile water were compared,and the pain score was observed tobe significantly lower in the sucrose group [44].In a randomized trial comparing intranasal fentanyl and saline,PIPP pain scores were significantly lower in the fentanyl group,and it significantly reduced pain during the examination[39].Although moderate pain was detected during exams in all three groups in our study,there was no significant difference between groups regarding PIPP scores,duration of crying or pain severity.
There is no consensus on the ideal method to be used to determine pain severity [45,46].Studies indicate that painful stimuli cause hemodynamic and metabolic changes in certain regions of the brain [47–50].In recent years,it has been reported that the evaluation of cortical activity with NIRS,together with physiologic and behavioral parameters,will give more accurate results in detecting pain [51].Roue et al.evaluated the pain response during venous blood collection in term infants and determined a significant correlation between the Neonatal Facial Coding System (NFCS)and changes in the NIRS parameters [25].In another study comparing the analgesic effect of glucose and breastfeeding during the heel-stick procedure,changes in NIRS were evaluated using Neural Information Processing Systems (NIPS).It was concluded that glucose might affect the pain-related response at the cortical level and that breastfeeding could reduce the perception of pain [52].Another study using NIRS revealed that interventional pain caused a decrease in tissue oxygenation in the frontal cortex,and an artificial platform that mimicked skin-to-skin contact had a corrective effect on tissue oxygenation [53].In the literature,there is no study evaluating the effect of pain on cerebral hemodynamics during ROP examinations.Tan et al.evaluated mesenteric tissue oxygenation during ROP examination and found a significant decrease in mesenteric rScO2,but cerebral oxygenation was not evaluated in this study [14].In our study,no difference was observed in terms of rScO2and FTOE before,during or after the exam among the three groups.
Activation of the sympathetic nervous system in response to painful stimuli causes changes in cerebral blood flow and cerebral blood volume [53–55].Although systemic alterations occurred due to pain during ROP examinations,we determined that this did not lead to a change in indicators of cerebral blood flow.Despite an increase in heart rate and blood pressure,no difference was observed in MCA blood flow velocities.Qui et al.used low-dose fentanyl infusion in premature babies under 32 weeks,revealed no significant changes in cerebral hemodynamics [26].We did not find any change in cerebral blood flow after ROP examination.Since we could not perform Doppler US measurements just during the procedure,we propose that this procedural obstacle may influence cerebral blood flow measurements.
The limitation of our study is that non-pharmacological methods were not used in our study.Therefore,we could not compare pharmacologic and non-pharmacologic methods for pain relief during ROP examination.Another major limitation is the absence of a true control group.We did not include a control group for ethical reasons.Although the number of infants included in the study provides the number calculated with power analysis,the small sample size may be a limitation for our study.Since the power calculation was not designed for comparison of vital signs,NIRS and MCA Doppler measurements,the conclusions about these parameters may have not been powered to detect significant differences.
There is still no consensus on the method to be used for pain control among preterm infants during ROP examination.Our study is the first to compare the effects of fentanyl and sucrose on pain responses in ROP examinations using PIPP scores,cerebral NIRS monitoring,and Doppler US.Fentanyl is the mainstay of analgesia in moderately painful procedures in neonates,but little is known about its effect on cerebral metabolism and circulation [26,56,57].
In conclusion,the lack of difference in pain control between oral sucrose and fentanyl administration indicates that sucrose may be a good alternative for pain management during ROP examination.Our findings suggest that ROP exam may not affect cerebral oxygenation or cerebral blood flow.Larger scale studies are needed to determine the best pharmacological option to reduce pain during ROP exams and evaluate the effects of this procedure on cerebral oxygenation and cerebral blood flow.
Author contributionsKN: conceptualization,data curation,formal analysis,writing–original draft.AD: conceptualization,formal analysis,writing–review and editing.SZ: data curation,writing–review and editing.GA: data curation.CS: data curation,writing–review and editing.All authors approved the final manuscript for submission.
Data availabilityThe datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Conflict of interestNo financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Ethical approvalEthics committee approval was obtained from the Istanbul Training and Research Hospital Clinical Research Ethics Committee (Decree no: 2741).
 World Journal of Pediatrics2023年9期
World Journal of Pediatrics2023年9期
- World Journal of Pediatrics的其它文章
- Fecal microbiota transplantation in childhood: past,present,and future
- Pediatric endocrinopathies related to COVID-19: an update
- Mapping the quality of prenatal and postnatal care and demographic differences on child mortality in 26 low to middle-income countries
- Clinical epidemiology and disease burden of bronchiolitis in hospitalized children in China: a national cross-sectional study
- Serum levels of the novel adipokine isthmin-1 are associated with obesity in pubertal boys
- Maternal and neonatal blood vitamin D status and neurodevelopment at 24 months of age: a prospective birth cohort study