
Pediatric endocrinopathies related to COVID-19: an update
2023-11-29 13:47ElmiraHajiEsmaeliMemarReihanehMohsenipourSeyedehTaravatSadrosadatParastooRostami
World Journal of Pediatrics 2023年9期
Elmira Haji Esmaeli Memar · Reihaneh Mohsenipour · Seyedeh Taravat Sadrosadat · Parastoo Rostami
Abstract Background Coronavirus disease 2019 (COVID-19) is a disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),the seventh coronavirus to be linked to human disease.The SARS-CoV-2 virus may have several pathophysiologic interactions with endocrine systems,resulting in disruptions in glucose metabolism,hypothalamus and pituitary function,adrenal function,and mineral metabolism.An increasing amount of evidence demonstrates both the influence of underlying endocrine abnormalities on the outcome of COVID-19 and the effect of the SARS-CoV-2 virus on endocrine systems.However,a systematic examination of the link to pediatric endocrine diseases has been missing.Data sources The purpose of this review is to discuss the impact of SARS-CoV-2 infection on endocrine systems and to summarize the available knowledge on COVID-19 consequences in children with underlying endocrine abnormalities.For this purpose,a literature search was conducted in EMBASE,and data that were discussed about the effects of COVID-19 on endocrine systems were used in the current study.Results Treatment suggestions were provided for endocrinopathies associated with SARS-CoV-2 infection.Conclusions With the global outbreak of COVID-19,it is critical for pediatric endocrinologists to understand how SARSCoV-2 interacts with the endocrine system and the therapeutic concerns for children with underlying problems who develop COVID-19.While children and adults share certain risk factors for SARS-CoV-2 infection sequelae,it is becoming obvious that pediatric responses are different and that adult study results cannot be generalized.While pediatric research gives some insight,it also shows the need for more study in this area.
Keywords Coronavirus disease 2019 (COVID-19) · Endocrine · Infection · Pediatrics
Introduction
Coronavirus disease 19 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),the seventh coronavirus to be linked to human disease.The major receptor for SARS-CoV-2 infection is believed to be angiotensin-converting enzyme 2 (ACE2) [1].The binding of SARS-CoV-2 to ACE2 initiates a cascade that activates the nuclear factor-κB pathway,resulting in very high levels of proinflammatory cytokines and chemokines,which contribute to the development of acute respiratory distress syndrome (ARDS) in severe COVID-19 [2,3].The lethality of ARDS and non-pulmonary consequences in COVID-19 are considered to be caused by a cytokine storm,in which immune and non-immune cells produce massive quantities of proinflammatory cytokines,causing damage both inside and outside the respiratory system [4].A limited but rising body of evidence suggests that underlying endocrine abnormalities may influence the outcome of COVID-19 and that the SARS-CoV-2 may have an effect on endocrine systems.
At first,it was assumed that infection with SARS-CoV-2 would cause similar but less severe symptoms and complications in children and adolescents [5].Multisystem inflammatory syndrome in children (MIS-C) and atypical endocrine responses have been observed in children infected with SARS-CoV-2 [6].Recent understanding concerning the impact of SARS-CoV-2 infection on endocrine systems is summarized here,and current material on COVID-19 pandemic complications in endocrine diseases is reviewed.SARS-CoV-2 and endocrine disorders have been studied extensively in adults,but we have attempted to include all relevant pediatric data from PubMed as of March 2022.If available,we included data from adults,and we made a notation in the text when articles spoke of adult vs.pediatric research teams.SARS-CoV-2 infection in children has been shown to have a wide range of responses in the pediatric population [7].Since children in the COVID-19 period need specific therapy,pediatric endocrinologists must comprehend the disease's symptoms and the limits of current knowledge.
For this purpose,a literature search was conducted in EMBASE,and data that were discussed about the effects of COVID-19 on endocrine systems were used in the current study (Supplementary Table 1).There are few data about the effects of COVID-19 on pediatric endocrine systems,so we tried to discuss related data in adults.
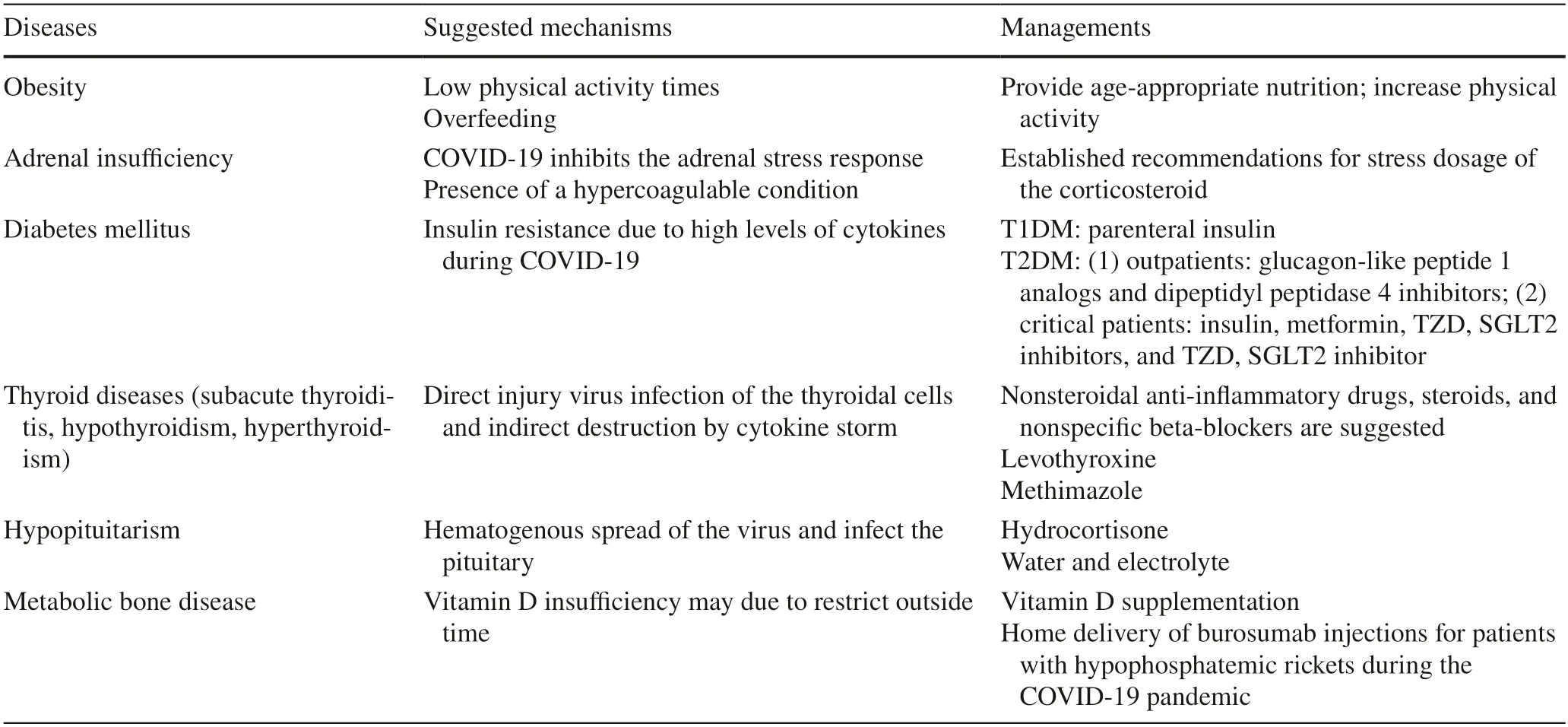
Table 1 The summary of the endocrinopathies in children and adults and their management
SARS-CoV-2 infection and subsequent endocrine dysfunction
The SARS-CoV-2 virus has several pathophysiologic linkages to the endocrine system and hence has the potential to disrupt pituitary,adrenal,and thyroid function,as well as glucose and mineral metabolism.Existing data are mostly favorable in terms of COVID-19-related endocrine problems in children (Table 1).
The similarities between COVID-19,SARS,and Middle Eastern respiratory syndrome show that the virus may enter the central nervous system through the olfactory bulb,including the hypothalamus [8].Adult observational studies have indicated that COVID-19 disrupts posterior pituitary function and causes an immediate onset of syndrome of inappropriate antidiuretic hormone [9–11 ].SARS survivors have been shown to have hypothalamic/pituitary dysfunction[12].However,the only evidence of pituitary involvement in COVID-19 is a magnetic resonance imaging finding of pituitary stalk involvement in two adult patients;there have been no reports of pituitary hormone deficiency in adults or children with COVID-19 thus far [13].
There is evidence that people with COVID-19 may be at risk for adrenal and thyroid problems.In one study,it was shown that acutely unwell people with COVID-19 illness had greater cortisol levels than those without COVID-19,but there was a negative link between the degree of cortisol response and survival rate in those who were COVID-19 positive [14].Computed tomography (acute adrenal infarction) and post-mortem investigations in individuals with severe COVID-19 and SARS-CoV-2 infection have also shown adrenal involvement [15,16].Adults with COVID-19 have been diagnosed with both thyrotoxicosis [as a result of elevated interleukin (IL)-6 levels] and hypothyroidism[17–19].Although ACE2 is extensively expressed in the thyroid and to a lesser amount in adrenal tissue,and thereforechildren may potentially be at risk,thyroid and adrenal pathology in children with COVID-19 and MIS-C have not been documented [20].
Due to the high expression of ACE2 in pancreatic islet cells,SARS-CoV-2 infection may have a diabetogenic impact irrespective of the stress response associated with severe sickness [21].Adults,but not children,with COVID-19 have been reported to develop diabetes mellitus for the first time [22,23].Contrary to expectations,the most critically ill individuals with COVID-19 have low lipid levels.These individuals had very low levels of total cholesterol,low density lipoprotein cholesterol,and high density lipoprotein cholesterol,indicating a strong inflammatory(cytokine) impact.Lipid levels rise concurrently with a decrease in inflammatory markers in recovering intensive care unit (ICU) patients.While the long-term repercussions of this occurrence are unknown,decreased lipid levels in conjunction with higher inflammatory markers do seem to be associated with a poor result [24,25].
COVID-19 does not seem to have a direct effect on the parathyroid glands or on mineral ion balance at the moment.However,research suggests that persons with severe COVID-19 may have a decrease in blood calcium levels [26,27].There are few occurrences of hypocalcemia in pediatric patients with MIS-C;however,there are no systemic findings in children at the moment,and probable reasons remain unknown [28,29].
Complications and management of COVID-19 in children with pre-existing endocrine disorders
The complications of SARS-CoV-2 infection have been predominantly documented in adults with underlying endocrine problems.While adult results should not be generalized to children,the studies clearly indicate potential dangers for the pediatric group.The purpose of this section is to summarize what is currently known about COVID-19 in patients with underlying endocrine problems and how it may affect pediatric patients.
There is currently no evidence that central hormone deficiency increases the risk of contracting SARS-CoV-2.Children and adolescents with multiple pituitary hormone deficiency,on the other hand,have distinct treatment challenges due to the complexity of their medical condition.Infants and toddlers with diabetes insipidus who have respiratory issues as a result of COVID-19 exposure have a significantly increased risk of acquiring abnormal blood salt levels [30].Due to variables including lower fluid intake,higher irreversible losses,and the difficulty for adipsic individuals with diabetes insipidus to tolerate oral desmopressin,patients with diabetes insipidus are at an increased risk of severe hypernatremia,which may be exacerbated by venous thrombosis in the acute illness [31–34].Patients with adrenal insufficiency (including those on corticosteroid replacement therapy) are at greater risk of respiratory and adrenal issues if they get COVID-19,a virus that has not been extensively studied in adults or children.
Currently,there is no evidence that children and adolescents with underlying thyroid abnormalities are at a greater risk of contracting SARS-CoV-2 infection or that their clinical course is changed.It is necessary to bear in mind,however,that patients with Graves' disease who receive antithyroid drug (ATD) treatment are at an increased risk of agranulocytosis and secondary infections [35].This is critical since one study found that more than half of COVID-19 non-survivors had a subsequent infection [36].In adults with COVID-19,underlying thyroid illness,especially hypothyroidism,does seem to be a risk factor for a more severe disease course [37–39].
Adults with diabetes mellitus,obesity,or hypertension are at increased risk of COVID-19 infection and have a greater incidence of complications and mortality [39–43].The T1D Exchange provided data on 64 persons with type 1 diabetes(T1D);33 had COVID-19-positive symptoms but were not tested or had COVID-19-negative symptoms;65.5% of participants were between the ages of 19 and 20 [44].COVID-19-positive individuals had a higher mean glycosylated hemoglobin A1c (HbA1c) (8.5% vs.8%),were more likely to present with diabetic ketoacidosis (DKA) (45.5% vs.13.3%) and needed a greater level of care than COVID-like individuals.In England,a population-based study found that patients with an HbA1c of 86 mmol/mol (10.0%) or greater had an increased risk of COVID-19-related mortality [hazard ratio=2.23,95% confidence interval (CI)=1.50–3.30;P<0.0001 in T1D] [45].
Children with T1D and COVID-19 were shown to have higher HbA1c,higher hospitalization rates,non-Hispanic Black ethnicity,and public insurance,according to T1D Exchange data in the pediatric population (unpublished data).During the coronavirus pandemic,children newly diagnosed with T1D are more likely to develop DKA and have more severe DKA [46].However,evidence suggests that children with T1D and COVID-19 have clinical outcomes that are equivalent to those of children who do not have diabetes [47].Children with diabetes have encountered significant obstacles as a result of the COVID-19 epidemic,most notably due to extensive school and childcare facility closures.In a study from Greece,34 children with T1D who used insulin pumps and continuous glucose monitoring had no significant increase in time in range during lockdown but did have increased blood glucose variability compared to the prelockdown period [48].Additionally,the children in this research had significant alterations in their food routines during lockdown.Restrictions imposed in response to the COVID-19 pandemic have led to reduced physical activity and dietary modifications,as well as changed diabetes management behaviors,all of which may raise the risk of poor nutrition,excessive weight gain,and increased diabetes management stress [47].
Numerous investigations have shown no difference in obesity rates between children with moderate COVID-19 and those with severe COVID-19 [49–51].While obesity is not more prevalent in pediatric patients hospitalized for COVID-19 than in the general pediatric population,the severity of COVID-19 illness may be connected with obesity,as it is in adults.Obesity was found to be a risk factor for mechanical ventilation in one investigation of 50 pediatric patients hospitalized with COVID-19 [52].Additionally,a recent multicenter investigation of COVID-19 infection in 281 hospitalized children under the age of 22 years showed obesity (odds ratio=3.39,95% CI =1.26–9.10;P=0.02)and hypoxia on admission as the only two underlying risk factors for severe respiratory illness [53].In adults,obesityrelated adverse outcomes may be mediated by pre-existing cardiovascular and renal illness,as well as hypertension[54].
Children who have metabolic bone disease or skeletal dysplasia that leads to respiratory insufficiency as a consequence of an irregular chest wall structure may be more susceptible to COVID-19 complications [55].Immunity and autophagy are both influenced by vitamin D;however,it is not known whether vitamin D deficiency enhances the chance of COVID-19 infection or its repercussions.Data from the UK Biobank did not show a correlation between SARS-CoV-2 infection and decreased blood 25-OH-vitamin D concentrations after controlling for confounding factors,despite the findings of certain observational studies of adults[56].
Obesity
Obesity is taken into consideration during the outbreak of COVID-19 for two reasons.First,according to reports from the World Health Organization,during an outbreak of COVID-19,the prevalence of childhood and adolescent obesity due to low physical activity times and overfeeding has increased [57].A large pediatric primary care study showed a significant increase in obesity rates among children ages 2 through 17 since the onset of the COVID-19 pandemic [58],and obesity-related lifestyle behaviors have also changed[59].Second,obesity as a comorbidity likely increases susceptibility and severe COVID-19 infection in pediatrics and adolescents [60].During the COVID-19 outbreak in Canada,obesity was introduced as the third factor among children with severe infection after malignancies and immunosuppression [51].Obesity may be a risk factor regardless of age,gender,and higher body mass index (BMI) related to the risk of requiring invasive mechanical ventilation [61].Furthermore,adult patients with obesity are more likely to have some symptoms,including fever,dyspnea,and caught [62].Because of the lack of enough studies,the impact of obesity on COVID-19 in the pediatric population has not been well explained.Poor immune response,cardiopulmonary disease,and chronic inflammation that link obesity to COVID-19 and have been proven in adult patients have also been shown in children [63].Obesity is associated with overexpression of angiotensin 2 [64].Obesity limits respiratory muscle movement and worsens general conditions in pediatric patients[65].Asthma and obstructive sleep apnea are linked to obesity,which is related to a higher risk of pulmonary infections [66].Cardiac anatomy changes,higher blood pressure and medications [67],intima layer artery thickening [68],endothelial dysfunction,and damage to the endothelium due to leptin perivascular adipose tissue have been explained in obese children.In obese individuals,chronic inflammation impairs the regulation of anticoagulant factors that contribute to venous thromboembolism during COVID-19 [69].Angiotensin converting enzyme converted angiotensin 2 to angiotensin type 1–7.Unlike angiotensin 2,which has inflammatory effects,angiotensin 1–7 acts as an anti-inflammatory [70].Therefore,it is assumed that this imbalance may cause immune response dysregulation [71].In patients with obesity,adipocytokines,such as leptin,may change the function and number of immune cells,leading to an increase in the number of activated macrophages (M1) and effector T helper 1 (Th1) and Th7 cytotoxic T cells and then a decrease in the number of regulatory T cells and M2 macrophages.Macrophages derived from visceral adipose tissue secrete large amounts of inflammatory cytokines,including nitric oxide IL-12,IL-1b,IL-6,and tumor necrosis factor-α (TNFα) [72].In individuals with obesity,SARS-CoV-2 enters fat cells by binding to ACE2,which could lead to increased viral load and prolonged viral spread due to their altered immune responses and cytokine response in adipose tissue[73].There is evidence of endothelial dysfunction in obesity[74] and kidney disease [75].Obesity is usually associated with comorbidities,such as hypertension,hyperinsulinism,type 2 diabetes (T2D),and thrombogenic events,which decrease the body’s ability to overcome COVID-19 [76].Fortunately,these comorbidities are not common in children.It seems that obese individuals spread more enormous amounts of the virus through inhalation and can infect other people [77].Since the effectiveness of the influenza vaccine due to alterations in the immune system decreased in obese people,this phenomenon may also occur in the vaccination against SARS-CoV-2,which leads to decreased immunization against COVID-19 in obese people patients [78].A large retrospective cohort study from the Society of Critical Care Medicine Viral Respiratory Illness Universal Study registry assessed all children hospitalized with COVID-19 from March 2020 to January 2021;31.5% of patients had obesity.In adult patients,obesity was associated with more severe COVID-19 diseases and more extended hospitalization,but unlike adults,the risk of mortality in obese children was not higher than that in non-obese patients.They found no relation between obesity and a higher risk of MIS-C because inflammatory and proinflammatory alterations due to obesity may have less impact on the immune dysregulation response in MIS-C.Furthermore,they have shown a negative correlation between age and high BMI with illness severity from COVID-19 in pediatric patients [60].
Management
Due to social isolation,lack of exercise,and food insecurity in socioeconomically challenged homes,the pandemicrelated closure of schools,camps,and extracurricular sports and activities has dramatically affected children’s and adolescents' health [79].In one of our centers,we have seen a large rise in the number of children under 19 who arrive with new-onset diabetes.The majority of the increase is attributed to the rise in T2D.It is critical to promote good eating habits and provide age-appropriate nutrition and physical activity guidelines.During the COVID-19 pandemic,racial/ethnic and socioeconomic differences exacerbated health inequities,notably concerning weight control.Healthcare practitioners should continue to educate patients about the importance of eating healthily and exercising regularly.We advocate for the use of telemedicine treatments to supplement pediatric weight control.
The likelihood of developing premature atherosclerotic cardiovascular disease (ASCVD) in children who have undergone MIS-C is unknown;however,individuals with a history of Kawasaki disease and persistent aneurysmal dilatation are regarded to be at a high risk of developing ASCVD.Coronary artery aneurysms have been detected in 6%–24% of patients with MIS-C,and Kawasaki disease characteristics have been observed in up to 40% of patients[79–81].Recent evidence suggests that pediatric children with MIS-C who receive intravenous immunoglobulin or an IL-6 antagonist,such as tocilizumab,recover without complications [82].Given the uncertain risk of complications,children who have recovered from MIS-C should receive a longer-term cardiac follow-up.
Adrenal insufficiency
ACE2 is expressed in small amounts in adrenal tissue,but COVID-19 can inhibit the adrenal stress response through different mechanisms.It has been shown that the virus contains amino acids such as adrenocorticotropin hormone.Antibodies against these amino acids and adrenocorticotropin hormone function cause a limited adrenal stress response and adrenal insufficiency [83].Another mechanism may be due to the hypercoagulable condition during the infection leading to acute adrenal infarction [84].On the other hand,patients with previous adrenal insufficiency are at a higher risk of infection because of reduced cortisol secretion,especially during the acute phase of adrenal insufficiency.Adrenocortical necrosis and hemorrhage during severe COVID-19 infection may cause adrenal insufficiency.Medications may cause adrenal insufficiency during COVID-19 infection.Martino et al.[85] showed that the risk of developing COVID-19 in patients with adrenal insufficiency is lower than that in the normal population,which may be due to more attention and care.On the other hand,patients taking supraphysiological doses of glucocorticoids may be more prone to COVID-19 [86].Although adrenal involvement has been shown in adults with COVID-19,significant adrenal disease in children with COVID-19 has not been reported[15].There are limited data available in pediatric patients with adrenal insufficiency and COVID-19.Nevertheless,Raisingani [87] showed that the mortality rate and severe disease increased in children with adrenal insufficiency and COVID-19 compared with children with COVID-19 and no adrenal insufficiency.
Management
Individuals who are steroid-dependent or fear that they may have adrenal suppression should exercise vigilance to prevent infection with SARS-CoV-2.Patients with symptomatic COVID-19 should be handled according to established recommendations for stress dosage [88,89].
Diabetes mellitus and impaired glucose metabolism
Is diabetes mellitus a risk factor for increasing the severity of COVID-19?
Diabetes mellitus,prediabetes mellitus,and hyperglycemia are independent risk factors associated with moderate to severe COVID-19,increased morbidity and mortality,and a significant increase in inflammatory cytokines compared with non-diabetic patients [45,90,91],but diabetes is not related to an increased risk of SARS-CoV-2 [92].Immunological dysregulation associated with hyperglycemia,endothelial damage,and increased levels of cytokines and oxidative stress related to coronavirus infection led to multiple organ dysfunction and thromboembolic risk [93].One cohort study revealed that patients with an HbA1c of 10.0% or higher had increased COVID-19-related mortality[45].Furthermore,antiviral drugs and systemic corticosteroids used for COVID-19 may exacerbate hyperglycemia and the severity of the disease in diabetic patients [94].In human studies,high glucose levels lead to increased SARS duplication,the production of mitochondrial reactive oxygen,and the activation of hepatocyte nuclear factor-1α,and glycolysis maintains this duplication [95].
In patients with T2D,neutrophil,and complement dysfunction,high proinflammatory cytokines,such as TNF-α,IL-6,and IL-1β,and decreased viral clearance can exacerbate the clinical course of COVID-19 [96].During the COVID-19 outbreak,children with new-onset-dependent diabetes may develop DKA but have more severe clinical manifestations.Their prognosis has not been worse than that of patients without diabetes [46,47].On the other hand,one study among adult patients reported a mortality rate of approximately fifty percent among patients with DKA in COVID-19.Although DKA may occur in T2D,a combined DKA/hyperglycemic hyperosmolar state should be considered and has higher mortality than DKA alone [93,97].
Is COVID-19 a risk factor for developing new-onset diabetes mellitus?
High levels of IL-6,IL-1β,TNF-α,monocyte chemoattractant protein-1,and inducible protein-10 during COVID-19 can cause insulin resistance.As mentioned above,obesity associated with T2D exacerbates the cytokine reaction that contributes to lowering insulin sensitivity and worsening hyperglycemia in patients with diabetes and prediabetes.COVID-19,as a viral infection,can trigger the presentation of diabetes in genetically predisposed individuals [98].The expression of ACE2 in β-cells as a receptor for COVID-19 may cause pancreatic damage and result in pancreatic endocrine and exocrine dysfunction [99].In one study,among the patients hospitalized for COVID-19,2.8% had newly diagnosed diabetes,and a systematic review showed 10%newly diagnosed diabetes mellitus among the patients with COVID-19 [93,100].
Management
During COVID-19 infection,regular consultation and monitoring of blood glucose levels (via finger sticks or continuous glucose monitors) are necessary.Insulin doses should be adjusted according to self-monitoring blood glucose.Furthermore,patients should check ketones in addition to blood glucose monitoring,and if ketones are present,increase correction doses of insulin.Adequate hydration of the patient effectively controls blood glucose levels [101].Regular physical activity and correcting eating habits are helpful.
In patients with T2D acute hyperglycemia due to exacerbation of inflammation,insulin resistance must be controlled rapidly and effectively.Some medications are used for glycemic control in patients with T2D,but the choice of medication during COVID-19 infection should be based on the patient’s condition.Glucagon-like peptide 1 analogs and dipeptidyl peptidase 4 inhibitors in mild to moderate symptoms have glucose-lowering efficacy and inflammatory action in outpatient and hospitalized patients.Insulin infusion in critically ill diabetic patients has been suggested for adequate glycemic control and D-dimer and IL-6 levels [94].Metformin,as a lowering glucose agent,had anti-inflammatory action related to significantly lower mortality compared to patients not receiving metformin [102].During severe COVID-19 infection (ICU-admitted patients),metformin,thiazolidinedione (TZD),sodium-glucose cotransporter receptor-2 (SGLT2) inhibitors,and TZD,SGLT2 inhibitors were used in hospitalized patients,but moderate disease has not been recommended to use.[94].
Due to increased insulin resistance and ketone generation,viral infections might be more challenging to control in patients with diabetes [103,104].Given the positive correlation between a higher HbA1c level and the prevalence of DKA in children with T1D,a large proportion of the pediatric T1D population may be at increased risk of developing DKA in the presence of COVID-19 infection [105,106].To reduce the risk of DKA,practitioners should familiarize themselves with sick day guidelines and be available for guidance during times of illness.Patients should be advised to monitor their blood glucose levels more often during COVID-19 illness,either with continuous glucose monitors or with finger sticks[101].Insulin doses may need to be adjusted more often,and additional fast-acting insulin correction boluses may be required to avoid severe hyperglycemia or ketoacidosis[107].Patients should monitor ketones regardless of blood sugar levels and increase correction dosage and fluid intake if ketones are detected.Encouraging remote blood glucose monitoring with continuous glucose monitoring is a great tool that should be made available to all families.
Additional guidelines for children with T2D include those discussed in the obesity section below.All children must engage in regular physical exercise and practice good dietary practices during this epidemic.Telemedicine is a helpful method for maintaining regular contact with the diabetes team and counseling and managing patients with T1D and T2D during COVID-19 infection.However,there are limited data,and further research is needed.A review among patients with T2D and T1D showed that telemedicine could reduce HbA1c by approximately − 0.01% to − 1.13% and− 0.12% to − 0.86%,respectively [108].
Thyroid disease
Thyroid cells express transmembrane protease serine 2 and ACE2 as receptors for COVID-19 even more than the lungs,explaining distinct thyroid manifestations during infection[20].Direct injury virus infection of the thyroidal cells and indirect destruction by cytokine storms during COVID-19 may lead to thyroid gland damage that presents to subacute thyroiditis with three-phase thyrotoxicosis,hypothyroidism,and finally euthyroidism [109].Thyroid hormones act as modulators of the immune system [110].Normal values of T4 and T3 can exacerbate the production and release of inflammatory and proinflammatory cytokines,which develop into a “cytokine storm”.T4 activates human platelets,which can contribute to clotting as a complication of virus infections [111].There is no evidence that thyroid disease predisposes individuals to COVID-19 infection,but uncontrolled hyperthyroidism is a risk factor for complications.Patients with thyroid disease should continue their medication as before [84].Three thyroid disorders,hypothyroidism,subacute thyroiditis,thyrotoxicosis,and nonthyroidal illness,have been described during the COVID-19 pandemic.The severity of COVID-19 is an essential determinant of the type of thyroid disorder [112].One study reported a prevalence of 5.2% hypothyroidism in hospitalized patients with COVID-19,predominantly subclinical hypothyroidism,and another showed 20.2% of patients with thyrotoxicosis [18].Fibrillation in a patient without a history of previous cardiovascular disease may indicate a thyrotoxicosis state [113].Furthermore,lower thyroid stimulating hormone (TSH) and free T3 values correlated with the severity of COVID-19 [114].
Management
All collected data about thyroid damage and COVID-19 have recommended regular monitoring of thyroid function during acute infection and treatment.There are no data on the treatment of thyrotoxicosis and sick euthyroid syndrome in hospitalized patients with COVID-19 [112].Since the clinical course of thyroiditis is benign,a watch-and-wait approach is sufficient,but in severely symptomatic patients,non-steroidal anti-inflammatory drugs,steroids,and nonspecific beta-blockers are suggested [115,116].If hypothyroidism and TSH are >10 mIU/mL,levothyroxine therapy should be started [84].Patients with primary hypothyroidism or hyperthyroidism should be treated as usual.ATDs such as methimazole should be warned about the risk of agranulocytosis and consequent bacterial infection.Because the symptoms of ATDs (fever,sore throat,and cough) are similar to COVID-19,a fast medical check is advised if symptoms emerge.Similar to other viruses,COVID-19 may cause thyroid storms in people with uncontrolled hyperthyroidism.Thyroid cancer patients who underwent surgery with replacement levothyroxine had no increased risk of infection.Immunosuppression may increase the infection risk in a portion of chemo patients.The American Thyroid Association and the American Association of Endocrine Surgeons say that due to the tumor's slow growth,most thyroid cancer operations may be safely deferred [117].
Hypopituitarism
ACE2,as a COVID-19 receptor on central nervous tissues,may play a role in COVID-19 neural invasion [118].In addition,the hematogenous spread of the virus can infect the pituitary [119].Children with hypopituitarism are not at increased risk for COVID-19,and they are not at increased risk of developing severe COVID-19 disease following infection.
Management
During the COVID-19 outbreak,regular monitoring is necessary for children with hypopituitarism to take their medication correctly.They have been taught that increased dose of hydrocortisone according to the severity of their disease.Some reports in adult patients with growth hormone deficiency suggest stopping growth hormone during hospitalization with COVID-19,but there are no data among pediatric patients [120,121].In diabetes insipidus,the water and electrolyte balance should be considered.Children with numerous pituitary hormone deficits may be at a greater risk of COVID-19 complications and death,especially if central adrenal insufficiency is not treated appropriately.In the absence of published data or standards,we propose that children's pituitary hormone deficits be managed according to known protocols.While current guidelines for adults with growth hormone insufficiency suggest discontinuing growth hormone therapy during hospitalization with COVID-19,there is a dearth of research on the impact of growth hormone treatment in children with COVID-19 [120].
Metabolic bone disease
Vitamin D supplementation has not been shown to protect against COVID-19 or its consequences.Randomized experiments are now being conducted to ascertain whether vitamin D supplementation may help prevent or lessen the severity of COVID-19.Prolonged home quarantine to prevent the spread of COVID-19 may restrict outside time,increasing the risk of vitamin D insufficiency and related consequences such as rickets,osteomalacia,and symptomatic hypocalcemia [122,123].Clinicians should continue to adhere to existing vitamin D supplementation guidelines for individuals at risk of insufficiency.The Food and Drug Administration has authorized home delivery of burosumab injections for patients with hypophosphatemic rickets during the COVID-19 pandemic.
The American Society of Bone and Mineral Research,the American Association of Clinical Endocrinology,the Endocrine Society,the European Calcified Tissue Society,and the National Osteoporosis Foundation have issued a joint statement outlining guidelines for managing osteoporosis in adults during the COVID-19 pandemic,some of which may need to be modified for pediatric patients.Essential measures to preserve bone health should be advocated in children with poor bone density,including proper calcium and vitamin D consumption,as well as sex steroid replacement where necessary.Weight-bearing exercise is critical for bone health optimization and should not be overlooked;physical therapy services are readily accessible through telemedicine and can be used to lead treatment in the home when necessary.Advanced therapy should be maintained when practicable,especially in children at high risk of fragility fractures.
Due to the long-acting nature of intravenous bisphosphonates,it is typically regarded as safe to postpone therapy for at least 6–9 months in adults [124].In youngsters,however,continued new bone formation and the emergence of stress risers during intermittent bisphosphonate medication may raise the risk of fracture if treatment is significantly delayed[125].Consider switching patients from pamidronate to zoledronic acid,which is injected over a shorter time period and needs fewer infusions.Clinicians may elect to forego pre-treatment laboratory testing for repeat infusions if the patient has no history of hypocalcemia with previous infusions,is consuming an adequate amount of calcium and vitamin D through diet or supplementation,has no renal disease,and has a stable overall health status.In most patients,DXA scans and other imaging may be postponed if the findings of the dual-energy X-ray absorptiometry (DXA) scan do not need a change in care.
Precocious puberty
There are some reports that represent precocious puberty in girls during COVID-19 [126–128].According to the first report,an increase in diagnoses and a quicker puberty progression were observed.It was hypothesized that these trends were related to an increase in electronic device use,an increase in BMI,and possibly an increase in eating.The second study confirmed the rise in precocious puberty diagnoses as well as the net prevalence of females.
In a study conducted by Turriziani Colonna et al.,children who presented with suspected central precocious puberty(CCP) during the COVID-19 outbreak were assessed.It was observed that among all patients who were referred for CCP,11 (39.3%) new CCP were diagnosed during COVID-19,and 22/45 (48.9%) of the patients showed an increased pubertal progression rate,with more children in the T3 and T4-5 phases [128].In another study,it was mentioned that of 124 patients with idiopathic precocious puberty,46.8%were diagnosed during one year of this pandemic,and the rest were diagnosed during three years before the COVID-19 pandemic [129].Additionally,other studies confirmed that COVID-19 is related to precocious puberty in children[130–133].
Conclusions
SARS-CoV-2 has the capacity to affect the majority of endocrine systems mechanistically.While little is known regarding the association between COVID-19 and endocrine problems in children,published data in adults have indicated pathology associated with diabetes mellitus,obesity,pituitary,adrenal,and thyroid illness.The following aspects of COVID-19 and endocrine diseases in children and adolescents are highlighted by current data: (1) antithyroid medication and continuous corticosteroid therapy are likely to enhance the risk of SARS-CoV-2 infection;patients should be counseled about this risk and advised to take further measures to avoid infection;(2) MIS-C seems to increase the incidence of hypocalcemia in children,and those who develop coronary artery aneurysms may be at increased risk of developing ASCVD later in life;(3) children with T1D and a higher HbA1c are more likely than children with better diabetes management to be hospitalized with COVID-19.The COVID-19 pandemic has produced a variety of difficulties for pediatric diabetes treatment,including school closures,interrupted schedules,and stress associated with diabetes control during lockdown times;(4)obesity does not seem to enhance the incidence of infection with SARS-CoV-2 in children,but it may be a risk factor for COVID-19-related problems in this group;and (5) COVID-19 treatment in children with diabetes insipidus needs special attention to fluid and salt balance.It may necessitate a modification in the method of desmopressin administration if the intranasal version is used.
The COVID-19 pandemic will aggravate obesity,metabolic syndrome,and its related comorbidities if enforced shelter-in-home laws and physical distance limitations are not taken into account,which we believe is very important.There is a direct link between sedentary activity and increased risks of developing T2D and precocious puberty over time [126–136].We must continue to give the necessary assistance to our patients to mitigate the pandemic's health repercussions for the future generation.
Supplementary InformationThe online version contains supplementary material available at https:// doi.org/ 10.1007/ s12519-022-00662-x.
AcknowledgementsWe wish to thank our colleagues in Endocrinology Ward of Children’s Medical Center for their cooperation and helps.
Author contributionsMEHE and SST wrote the first draft of manuscript.MR developed the concept,gathered some data and published article.RP developed the concept,gathered some data and published article,and wrote the first draft of manuscript.All authors read and approved the final version of manuscript.
FundingThe authors received no specific funding for this work.
Data availabilityData of this manuscript are available in the archive of Children’s Medical Center Hospital and will be presented in case of request.
Declarations
Ethical approvalThis research was done under permission of Ethics Committee of Tehran University of Medical Sciences.
Conflict of interestThe authors declare that they have no conflicts of interest.
 World Journal of Pediatrics2023年9期
World Journal of Pediatrics2023年9期
- World Journal of Pediatrics的其它文章
- Fecal microbiota transplantation in childhood: past,present,and future
- Mapping the quality of prenatal and postnatal care and demographic differences on child mortality in 26 low to middle-income countries
- Clinical epidemiology and disease burden of bronchiolitis in hospitalized children in China: a national cross-sectional study
- Serum levels of the novel adipokine isthmin-1 are associated with obesity in pubertal boys
- Effects of fentanyl and sucrose on pain in retinopathy examinations with pain scale,near-infrared spectroscopy,and ultrasonography:a randomized trial
- Maternal and neonatal blood vitamin D status and neurodevelopment at 24 months of age: a prospective birth cohort study