
The effects of hyperbaric oxygen therapy on paroxysmal sympathetic hyperactivity after cardiopulmonary resuscitation: a case series
2023-11-27 10:57:30HongyuWangYihaoLiMengZhaoCaihongRenSisenZhang
Hongyu Wang, Yihao Li, Meng Zhao , Caihong Ren, Sisen Zhang
1 Department of Emergency Medicine, the Fifth Clinical Medical College of Henan University of Chinese Medicine,Zhengzhou 450003, China
2 Department of Emergency Medicine, People’s Hospital of Henan University of Chinese Medicine/People’s Hospital of Zhengzhou, Zhengzhou 450003, China
3 Henan Research Centre of Cardiopulmonary-Cerebral Resuscitation Engineering Technology, Zhengzhou 450003, China
4 Department of Emergency Medicine, Luohe Central Hospital, Luohe 462000, China
The onset of cardiac arrest (CA) is sudden and critical.Due to cerebral ischaemia and hypoxia, the prognosis for post-cardiopulmonary resuscitation (CPR) patients is poor.Paroxysmal sympathetic hyperexcitability (PSH) is a potentially life-threatening condition, which is characterized by episodes of increased heart rate and blood pressure,sweating, hypothermia, and forced posture.[1]Hypoxicischaemic encephalopathy post-CPR can lead to PSH,which often indicates a worse prognosis.Currently, the treatment for PSH focuses on managing its clinical signs with medication; however, the effectiveness is still not satisfactory.To date, the application of hyperbaric oxygen therapy (HBOT) to treat post-CPR PSH has not been reported.Here, we reported four patients with post-CPR PSH who experienced significant relief from symptoms after receiving a combination of conventional treatment and HBOT.Additionally, the patients’ levels of consciousness improved from being in a coma to fully awakening, and none of them experienced a recurrence of PSH-related signs.
METHODS
This study reported on four post-CPR patients from March 2021 to January 2022, whose general information is summarized in Table 1.PSH was diagnosed with the 2014 PSH Assessment Measure (PSH-AM)[2]as its diagnostic criteria, along with the clinical feature scale(CFS) and the diagnosis likelihood tool (DLT).Each diagnostic criterion was assigned one score.The CFS and DLT were summed to derive the PSH-AM score.In this study, PSH was diagnosed when the PSH-AM score was≥17.[3]These four patients had PSH-AM scores of 21,24, 21, and 19, respectively.All four patients who were diagnosed with PSH underwent an electroencephalogram(EEG) to distinguish it from epilepsy according to clinical symptoms, EEG findings, and the response to antiepileptic drugs.Additionally, the EEG was done to rule out other conditions such as central fever, sepsis,pheochromocytoma, and hyperthyroidism.
The general treatment for the four patients included tracheal intubation with ventilator-assisted ventilation,dehydration to reduce intracranial pressure, early mild hypothermia treatment, early initiation of enteral nutrition according to the function of the gastrointestinal tract, maintenance of circulatory and respiratory stability,and symptomatic and supportive treatment.Treatment measures for PSH included minimizing any stimuli that might trigger a PSH attack, mechanical ventilation,analgesia-sedation when necessary, appropriate fluid replacement, nutritional support to ensure the body’s metabolic needs, and early rehabilitation exercises.Medical intervention is the primary treatment for PSH and works by inhibiting central sympathetic output and blocking responses in the peripheral organs of the sympathetic nervous system.For opioid analgesia,morphine is typically used, and remifentanil can be used for patients with hepatic or renal insufficiency.β-blockers were administered to reduce the basic metabolic rate and circulating catecholamine levels.Esmolol was continuously pumped, while propranolol was taken orally once gastrointestinal function had recovered.Baclofen was administered to patients with tonic spasm and dystonia.
HBOT was undertaken in a pure-oxygen single chamber (model: SHC900GD, Shanghai 701 Yang Garden Hyperbaric Oxygen Chamber Co., Ltd, China).The oxygen chamber was 2.6 m in length, 1.3 m in diameter,and approximately 1,500 kg in weight.The airflow rate through the oxygen chamber was 100–300 L/min and the maximum operating pressure was 3.0 standard atmospheres.The treatment pressure was 1.6 ATA (1 ATA=98.067 kPa),with each treatment session lasting 70 min; including 20 min for pressure increase, 30 min for pressure stabilization,and 20 min for pressure reduction.A course of HBOT was administered twice a day for a duration of 10 days.
RESULTS
Following 3–4 courses of HBOT, all four patients’signs of PSH were significantly reduced and the CFS scores had substantially decreased.The time to GCS≥9 in patients 1–4 was 34, 25, 38, and 28 days, respectively.At the three-month follow-up, their PSH had completely disappeared with no recurrent events reported.A brief overview of these four patients and their treatment outcomes is presented below.
Case 1 involved a 32-year-old male who had a CA due to accidental electrocution while working in a factory.On-site CPR was performed for approximately 20 min to return of spontaneous circulation (ROSC).His cranial MRI findings suggested bilateral splenium of the corpus callosum and diffuse white matter damage in the occipital lobe.MRI findings on day 4 are shown in Figure 1.In total, three courses of HBOT were administered.
Case 2 involved a 40-year-old male patient who presented with hypoxaemia and CA due to asphyxia.ROSC was restored after approximately 21 min of CPR.
Case 3 involved a 27-year-old male who was admitted to the hospital >2 h post-CPR following a CA in another hospital due to an anaesthetic accident.ROSC was restored after a total of 24 min of CPR.
Case 4 involved a 41-year-old male who had a CA after drowning, with 18-min bystander CPR prior to ROSC.The cranial CT findings on day 5 and day 14 (day 7 of HBO treatment) are presented in Figure 2.
DISCUSSION
Brain resuscitation is crucial during CPR, as brain damage post-CPR is the primary factor affecting case fatality and disability rates.[4,5]PSH is characterized as sympathetic hyperactivity following severe brain damage.The presence of PSH may prevent early withdrawal from the ventilator and lead to an extension of intensive care unit stay, thereby further aggravating the clinical burden.[6]PSH has been more frequently reported in patients with craniocerebral trauma and stroke.[7]However, reports of PSH post-CPR are rare and can be easily overlooked in the clinical setting.[8]HBOT increases oxygen levels in blood and tissues and has been used to treat an extensive range of diseases by promoting an integrated response of various systems,such as pulmonary capillaries, blood circulation,tissue capillaries, and tissue cells.HBOT also has specific effects on immune and metabolic pathways.Moreover, it has shown positive outcomes in treating carbon monoxide poisoning, sudden deafness, digestive disorders, and neonatal asphyxia.[9-11]
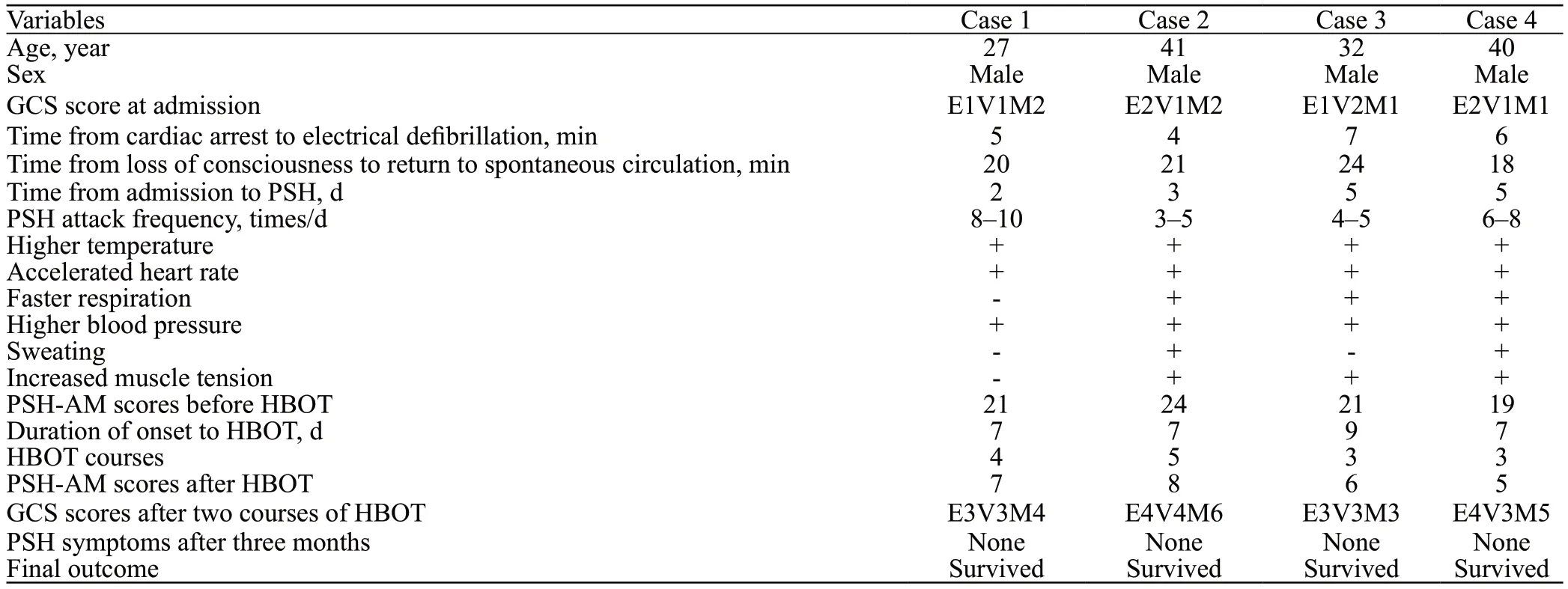
Table 1.Clinical data concerning four patients with PSH
To date, there are no specific medication for PSH,[12]and therapy involves primarily symptomatic treatment and avoiding triggers.Few case studies have reported on the efficacy of HBOT for PSH.Lv et al[13]reported six traumatic brain injury patients with poor drug efficacy recovered from PSH after 3–10 HBOT treatment courses.Choi et al[14]administered HBOT to patients with carbon monoxide poisoning-induced delayed encephalopathy combined with PSH.Three patients exhibited significant improvement in their level of consciousness and with no recurrence.However, few studies have reported on the efficacy of HBOT when treating patients with PSH post-CPR.[15]Therefore, we present our experience with HBOT in treating PSH in four patients.
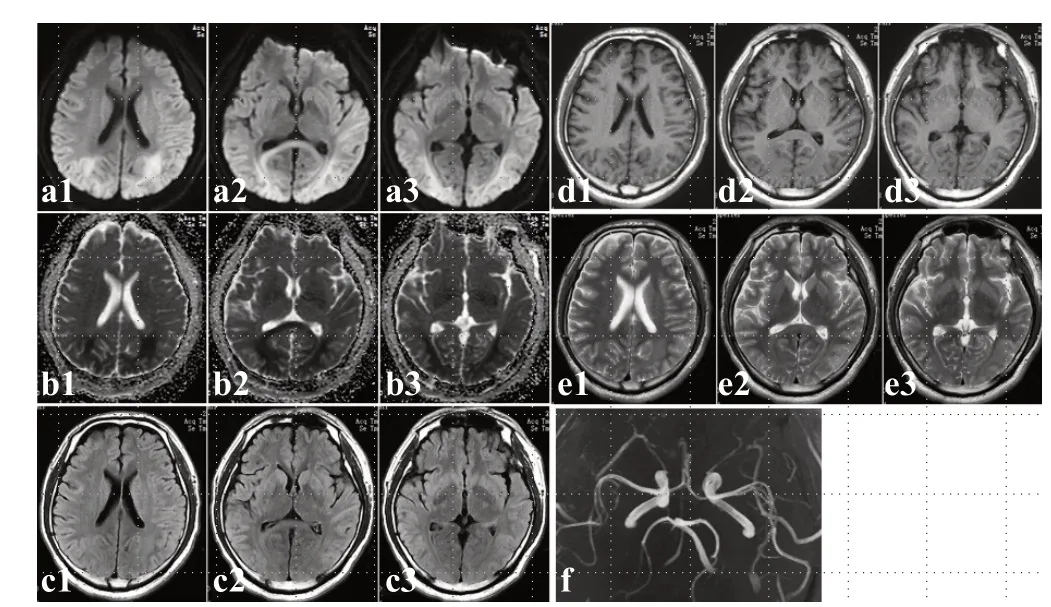
Figure 1.The MRI findings on day 4 in Case 1 indicated symmetrical,patchy, slightly long T1 and slightly long T2 signals, a DW-MRI high signal, changes in the ADC low signal, smooth vessel walls on cranial MRA, and no stenosis.a1–a3 are cranial DW-MRI sequences;b1–b3 are cranial MRI ADC sequences; c1–c3 are cranial MRI flair sequences; d1–d3 are cranial MRI T1 sequences; e1–e3 are cranial MRI T2 sequences; and f is a cranial MRA.ADC: apparent diffusion coefficient; DW-MRI: diffusion-weighted magnetic resonance imaging; MRA: magnetic resonance angiography; MRI: magnetic resonance imaging.
All four patients in this study showed signs of improvement and regained consciousness after HBOT,and achieved good outcomes (GCS≥9).Moreover, no recurrence was observed at follow-up, suggesting that HBOT was an appropriate choice for these patients.This positive outcome may have been due to the patients having undergone an early tracheotomy and ultra-early HBOT, within an opportunistic repair time for cerebral resuscitation.Regarding the possible mechanisms, we hypothesized that the following were involved.First,several studies have suggested that HBOT has antiinflammatory and anti-apoptotic effects on a variety of diseases, including idiopathic sensorineural hearing loss, delayed encephalopathy after carbon monoxide poisoning, necrotizing soft tissue infections, gas gangrene,and traumatic brain damage.[16-18]Patients may suffer from post-CPR syndrome due to ischaemia-reperfusion injury to systemic tissues, which is particularly pronounced in the brain.[19]HBOT could reduce the severity of ischaemia-reperfusion injury, decrease leukocyte adhesion on the endothelium of venules, and reduce inflammatory factor levels.[20]Second, HBOT was effective in reducing brain tissue oedema.Previous evidence indicates that HBOT induces intracranial arterial vasoconstriction and a substantial reduction in cerebral blood flow, thereby resulting in a reduction in cerebral oedema and a decrease in intracranial pressure,and further reducing cerebral oedema.[21]However,the oxygen supply to brain tissues is not compromised due to the increased arterial partial pressure of oxygen and diffusion distance of oxygen.[22]Moreover, HBOT also stabilizes the blood-brain barrier, which promotes revascularization and recovery of neural tissues.[23]Overall, the treatment appears to be effective.
This study had some limitations.First, PSH post-CPR is relatively rare and the number of included cases was limited.Second, this study only provides a clinical observation of HBOT on PSH post-CPR.The possible pathogenesis and timing of HBOT require further investigation.

Figure 2.The cranial CT finding in Case 4.a1–a4: CT images on day 5 of CA onset suggested diffuse cerebral oedema in the cerebral hemispheres with shallow or absent sulci; b1–b4: CT images on day 14 of CA onset (day 7 of HBOT) indicated that the sulci and gyri were evident and that the cerebral swelling had improved.CA: cardiac arrest; CT: computed tomography; HBOT: hyperbaric oxygen therapy.
CONCLUSION
The presence of PSH after CPR is often indicative of critical illness and a worse prognosis.HPOT may be beneficial in relieving symptoms, and further research is needed on the use of HBOT for PSH following CPR.
Funding:This study was funded by the Key Scientific Research Project Plan of Higher Education Institutions in Henan Province(Number: 23A320025) and by the China International Medical Exchange Foundation 2021 Cardiovascular Multidisciplinary Integrated Thinking Research Fund (Number: z-2016-23-2101-37).
Ethical approval:This study was conducted with approval from the Ethics Committee of Zhengzhou People’s Hospital.This study was conducted in accordance with theDeclaration of Helsinki.All study participants provided informed consent.
Conflicts of interest:The authors declare that they have no competing interests.
Author contribution:HYW analyzed the data, drafted the manuscript, and developed the research idea.YHL, MZ, and CHR assisted with data analysis.SSZ revised the manuscript and supervised the entire study.All authors approved the results of the data analysis and the content of the manuscript.All authors read and approved the final manuscript.
 World journal of emergency medicine2023年6期
World journal of emergency medicine2023年6期
- World journal of emergency medicine的其它文章
- The effect of prophylactic antibiotics in acute upper gastrointestinal bleeding patients in the emergency department
- Uterine artery pseudoaneurysm after subtotal hysterectomy: a case report
- Tension urinothorax as a reversible cause of cardiac arrest: a case report
- Hemorrhagic pancreatitis from fenofibrate and metformin toxicity: a case report
- Pyopneumothorax caused by Parvimonas micra and Prevotella oralis: a case report
- A case of pulmonary mucormycosis presented with cardiac arrest