
Interobserver reliability of computed tomography angiography in the assessment of ruptured intracranial aneurysm and impact on patient management
2023-07-26 03:24:48AliElmokademBasmaAbdelmonaemElgedAhmedAbdelRazekLamiaaGalalElSerougyMohamedAliKasemMohamedAliELAdalany
World Journal of Radiology 2023年6期
Ali H Elmokadem, Basma Abdelmonaem Elged, Ahmed Abdel Razek, Lamiaa Galal El-Serougy, Mohamed Ali Kasem, Mohamed Ali EL-Adalany
Abstract
BACKGROUND
Aneurysmal subarachnoid hemorrhage is an emergency that can lead to a high mortality rate and many severe complications. It is critical to make a rapid radiological evaluation of ruptured intracranial aneurysms (RIAs) to determine the appropriate surgical treatment.
AIM
To assess the reliability of computed tomography angiography (CTA) in assessing different features of ruptured intracranial aneurysm and its impact on patient management.
METHODS
The final cohort of this study consisted of 146 patients with RIAs (75 male and 71 female) who underwent cerebral CTA. Their age ranged from 25 to 80, and the mean age ± SD was 57 ± 8.95 years. Two readers were asked to assess different features related to the aneurysm and perianeurysmal environment. Inter-observer agreement was measured using kappa statistics. Imaging data extracted from non-contrast computed tomography and CTA were considered to categorize the study population into two groups according to the recommended therapeutic approach.
RESULTS
The inter-observer agreement of both reviewers was excellent for the detection of aneurysms (K = 0.95, P = 0.001), aneurysm location (K = 0.98, P = 0.001), and (K = 0.98, P = 0.001), morphology (K = 0.92, P = 0.001) and margins (K = 0.95, P = 0.001). There was an excellent interobserver agreement for the measurement of aneurysm size (K = 0.89, P = 0.001), neck (K = 0.85, P = 0.001), and dome-to-neck ratio (K = 0.98, P = 0.001). There was an excellent inter-observer agreement for the detection of other aneurysm-related features such as thrombosis (K = 0.82, P = 0.001), calcification (K = 1.0, P = 0.001), bony landmark (K = 0.89, P = 0.001) and branch incorporation (K = 0.91, P = 0.001) as well as perianeurysmal findings including vasospasm (K = 0.91, P = 0.001), perianeurysmal cyst (K = 1.0, P = 0.001) and associated vascular lesions (K = 0.83, P = 0.001). Based on imaging features, 87 patients were recommended to have endovascular treatment, while surgery was recommended in 59 patients. 71.2% of the study population underwent the recommended therapy.
CONCLUSION
CTA is a reproducible promising diagnostic imaging modality for detecting and characterizing cerebral aneurysms.
Key Words: Computed tomography angiography; Intracranial aneurysm; Subarachnoid hemorrhage;Intracranial hemorrhage; Observer variation
INTRODUCTION
Acute subarachnoid hemorrhage (SAH) is a medical emergency that can lead to a high mortality rate and many severe complications. The most frequent cause of non-traumatic SAH is a ruptured aneurysm. Ruptured aneurysms not only cause subarachnoid bleeding but can also cause subdural or intracerebral hematomas. It is critical to make a rapid radiological evaluation of ruptured intracranial aneurysms (RIAs) to determine the appropriate surgical treatment of SAH[1]. Different imaging modalities are used or have been used to assess intracranial vascular lesions. Digital subtraction angiography (DSA) has been considered the “gold standard” for detecting intracranial aneurysms and therapeutic decision-making. Additionally, intra-arterial cone beam computed tomography angiography (CTA) using a flat panel detector incorporates the high spatial vascular resolution of threedimensional (3D) rotational angiography with computed tomography (CT) postprocessing techniques to increase the contrast resolution[2]. Nevertheless, it is an invasive and time-consuming technique with a reported 0.5% risk of neurological complications[3]. Magnetic resonance (MR) angiography enables visualization of intra-cranial arteries without ionizing radiation or intravenous contrast material. The performance of MR angiography in evaluating acute SAH also has been compared favorably with that of DSA. However, MR angiography can be technically challenging for acutely ill patients. Additionally, aneurysms less than 5 mm in diameter might be missed in MR angiography studies[4].
Compared to DSA, CTA is a safe, relatively inexpensive, and noninvasive imaging. CT angiography is not associated with significant patient risks other than those related to administering iodinated contrast media. Images can be relatively safely obtained without the need for arterial puncture or catheter manipulation that carries the possibility of acquiring a permanent neurologic deficit[5].For these reasons, helical cerebral CT angiography has been widely used in detecting intracranial aneurysms, with a reported sensitivity of 70%-96%[6]. Currently, multidetector CT angiography has the ability to detect most intracranial aneurysms of 5 mm or larger. Multidetector row CT scanners provide increased spatial resolution and decreased scanning time, which should increase the sensitivity of the technique in depicting aneurysms of less than 5 mm in diameter. Currently, CT angiography is accepted as a first-line diagnostic imaging modality for evaluating intracranial aneurysms. Nevertheless, using CT angiography to depict intracranial aneurysms showed variable sensitivity. The reported sensitivity of CTA in detections of small intracranial aneurysms (< 3 mm) varied from 28%-43% in a study that included 99 small aneurysms[7] to 83%-92% in another study had 579 small aneurysms[8].
Deciding whether to perform surgical clipping or endovascular therapy for an intracranial aneurysm is vital. Treatment of intracranial aneurysms depends on clinical features, including age, Hunt and Hess grade, neurological or medical comorbidity, and characters of the aneurysm itself. Advances in imaging technologies have improved our comprehension of the 3D geometry of cerebral aneurysms, which has further affected treatment procedures, and helps neurosurgeons in the diagnosis, planning, and assessment of the therapeutic modalities. Exact information must be obtained preoperatively regarding the location, size, and morphology of the aneurysm and the property of the aneurysmal wall, its relationship with the parent vessel and adjacent branches, vessel incorporation, presence of calcification or thrombus[9]. Perianeurysmal information such as associated vasospasm, vascular variants, presence of vascular malformations, and the relationship of the aneurysm to the bony skull base is also crucial for proper treatment method selection.
This work aims to assess the inter-observer reliability of CTA in assessing different features of RIAs and their impact on patient management.
MATERIALS AND METHODS
Study population
The Institutional review board approved this single-center prospective study. One hundred sixty-one consecutive patients with clinically suspected intracranial aneurysms were recruited. Inclusion criteria were adult patients with imaging signs of SAH by non-enhanced CT. The exclusion criteria were patients with renal insufficiency (n= 6), pregnant or lactating females (n= 2), and non-diagnostic examinations (n= 7). The final cohort of our study included 146 patients (75 male and 71 female). Their age ranged from 25 to 80 years, with a mean age was 57 ± 8.9 years. Once enrolled, all patients were submitted to a contrast-enhanced CTA scan for diagnosis of intracranial aneurysm. The commonest clinical presentation was a headache, neck pain, and depressed consciousness in 130 patients, hemiparesis in 12 patients, cranial nerve palsies, and blurring of vision being less common presenting symptoms in 3 patients. One patient presented in an accident. The flow chart of our study is illustrated in (Figure 1).
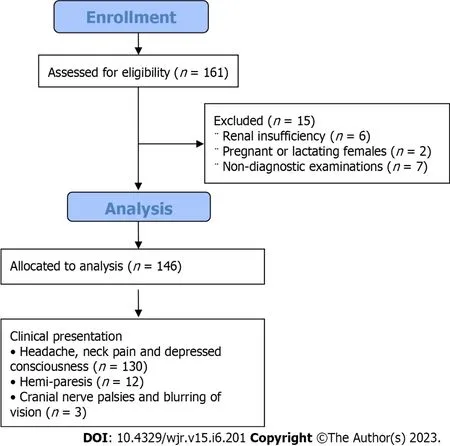
Figure 1 Flow chart of the study.
CTA Technique
All examinations were carried out with 160-slice computed tomography (Toshiba Aquilion Prime 160, Tochigi, Japan). Examinations were performed in a supine position with the arms of the patients beside the body. We first performed a non-contrast CT (NCCT) scan of the whole brain in an axial plane tilted along the orbitomeatal line using the following parameters: tube voltage 100 kVp, field of view (FOV) 220 mm, collimation 0.75 mm, matrix size 512 × 512, slice thickness 3.0 mm, and rotation time 1.0 s. CTA examinations were achieved using the bolus triggering technique for the timing of contrast medium injection. A region of interest (ROI) was centered at the upper end of the common carotid artery and sized to include only the lumen of the artery. The bolus triggering technique started automatically after contrast-medium injection when an attenuation value of 100 HU was reached in ROI. Non-ionic contrast medium Ultravist 370 (370 mgI/mL, Bayer Healthcare Ltd, Guangzhou, China) at a dose of 1 mL/Kg and rate of 4mL/s followed by a 50 mL saline flush administeredviaautomatic injector (Medrad Stellent, Warrendale, PA) through a 20 G intravenous cannula in the antecubital fossa of either upper extremity. The following parameters were used: Tube voltage 120 kVp, automatic tube current modulation, FOV 250 mm, collimation 0.75 mm, matrix size 512 × 512, slice thickness 1.5 mm, rotation time 0.3 s. Scanning was performed in the caudocranial direction and started at the level of the aortic arch up to the vertex. Axial images were stored and transferred into the workstation as source images after reconstruction at 0.625-mm intervals. Multiplanar reformats (MPR), maximum intensity projection (MIP), and 3D volume-rendered images were used for further analysis.
Image analysis
Image analysis was conducted on the PACS system (GE Healthcare, Waukesha, WI). All CTA examinations were revised and interpreted by two experienced neuroradiologists with 14 and 8 years of experience in neurovascular imaging (AHE, BE). They independently reviewed the images blinded to patient data and final diagnosis. The following features obtained at NCCT were individually evaluated for each patient: The degree of SAH using the Fisher scale, associated parenchymal hemorrhage, hydrocephalus, and ischemic changes. Both readers were asked to predict the location of the aneurysm based on the distribution of SAH and Intraparenchymal hematoma (IPH). At CTA, both readers were asked to evaluate the following aneurysm features’: (1) Number; (2) Size; (3) Location (anteriorvsposterior circulation, parent artery, and affected segment); (4) Shape (saccular, fusiform, serpentine or blister); (5) Margin (sharp, irregular/daughter sacs); (6) Presence of calcification and/or thrombus; (7) The presence of branch incorporation; and (8) The orientation of the aneurysm in relation to the parent vessel (e.g., pointing superior/inferior, medial/Lateral, anterior/posterior). Aneurysm size was defined by the maximum measurement of aneurysm width, neck width (the largest cross-sectional diameter of the aneurysm neck), depth (the longest diameter between the neck and dome), and aneurysm neck-todome length. According to size, aneurysms were classified into: (1) Small aneurysms are less than 5 mm; (2) Medium-sized aneurysms are 6-15 mm; (3) Large aneurysms are 16-25 mm; and (4) Giant aneurysms are > 25 mm. The following features related to the perianeurysmal environment were evaluated by both readers: (1) Associated vasospasm; (2) Perianeurysmal cysts; (3) Associated vascular malformations (type and classification based on relation to aneurysm); (4) Vascular variants; and (5) The relationship of the aneurysm to the bony landmarks or related osseous changes (remodeling or fractures).
Management selection
Imaging data extracted from NCCT and CTA were considered to categorize the study population into two groups according to the recommended therapeutic approach. The first group was recommended to proceed to endovascular therapy, and the second group was advised to undergo surgical management (clipping).
Features in favor of endovascular therapy (coiling) were:(1) Absence of parenchymal hematoma; (2) Posterior circulation aneurysm; (3) Small aneurysm neck < 4 mm; (4) Aneurysm diameter < 15 mm; (5) Unilobar shape; (6) Multiple aneurysms; (7) Calcification located at the aneurysm neck that might interfere with clipping; and (8) Presence of vasospasm. Coiling using balloon remolding technique or stent-assisted coiling was recommended with wide-neck aneurysms.
Features favored surgical management (clipping) Were(1) Presence of intra-parenchymal hematoma; (2) Middle cerebral and pericallosal arteries aneurysm; (3) Wide neck of the aneurysm > 4 mm; (4) Aneurysm diameter > 15 mm; (5) Abnormal configuration unsuitable for endovascular therapy; (6) Aneurysmal sac incorporating arterial branches; (7) Presence of intraluminal thrombus; and (8) Vascular variant interferes with endovascular management. Features considered in managing RIAs are listed in Table 1.
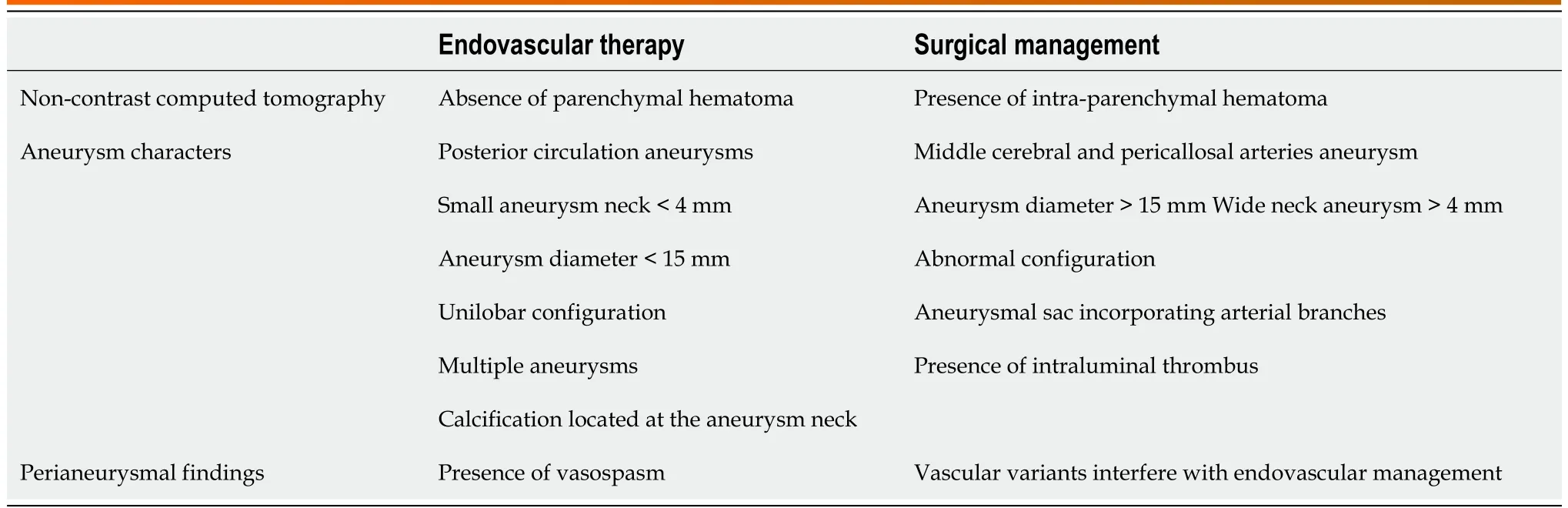
Table 1 Imaging features considered in the management of ruptured intracranial aneurysms
Statistical analysis:
All statistical analyses were performed with software (SPSS, version 16.0; SPSS, Chicago, Ill). The Kolmogorov-Smirnov Z-test was used to test the normality of the continuous variable groups. The CTA image quality scores were ranked and listed as a mean and standard deviation. The kappa statistic (K), including a 95%CI with an intra-class correlation (r), was used to estimate the proportion of interobserver agreement beyond that expected by chance for the image quality grading and depiction of the aneurysm, its neck, parent artery, and associated anomalies. APvalue less than 0.05 was considered to indicate a statistically significant difference. The K values were interpreted as follows: K values between 0.61 and 0.80 represented good; K values between 0.81 and 1.00 represented excellent agreement.
RESULTS
NCCT findings
Both readers used the Fisher scale to assess SAH. The means scores were (3.47 ± 0.6 and 3.33 ± 0.4) with a good interobserver agreement (K = 0.79,P= 0.001). Excellent interobserver agreement between both readers in the detection of IPH (K = 0.1,P= 0.001) as well as in the detection of hydrocephalus (K = 0.92,P= 0.001). A statistically significant strong positive correlation was found between the location of SAH and IPH on NCCT scan and the eventual location of a ruptured cerebral aneurysm in single ones and as a differentiating point of culprit aneurysm in multiple aneurysms confirmed by CTA and surgical or endovascular intervention. The sensitivity of NCCT predicting aneurysms depends on blood distribution of more than 85% in our study. Table 2 shows the inter-observer results of CT and CTA findings.

Table 2 Inter-observer agreement of computed tomography and computed tomography angiography features of aneurysm
Aneurysm characters:
Detection:The first reader detected 166 aneurysms [126 single aneurysms (75.9%) and 40 multiple aneurysms (24.1%)], while 2nd reader detected 169 aneurysms [127 single aneurysms (75.1%) and 42 multiple aneurysms (24.9%)]. An excellent interobserver agreement was found between both readers in detecting an aneurysm [98.8% (K = 0.95,P= 0.001)]. Among multiple aneurysms, 14 were mirror image aneurysms (MA), and the remaining were non-mirror image (NMA). The commonest location of MA in our series was the M1 segment or at the middle cerebral artery (MCA) bifurcation (n= 3), followed by the cavernous portion of internal carotid artery (ICA) (n= 2) (Figure 2), the posterior communicating artery (PCOM) (n= 1), and ICA terminus (n= 1). The sensitivity of CTA compared to DSA in the detection of intracranial aneurysms was 98.8%. DSA identified 89 aneurysms in 80 patients. Among these aneurysms, CTA failed to detect one in a patient with three other aneurysms. The missed aneurysm was located in posterior cerebral artery (PCA) with diameters of 3 mm. In two cases, CTA depicted aneurysms, which DSA missed. An ICA blister and a distal MCA mycotic aneurysm were the two missed aneurysms.
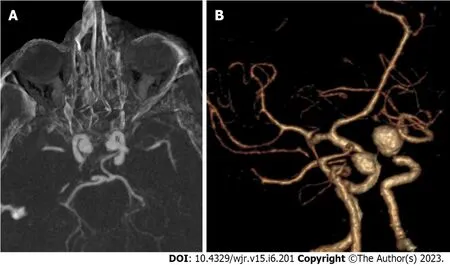
Figure 2 Mirror image intracranial aneurysms. A: Axial computed tomography angiography (CTA) in maximum intensity projection; B: Three-dimensional CTA for mirror image internal carotid artery aneurysm.
Location:For most of the study, the population was harboring anterior circulation aneurysms (94%). Excellent interobserver agreement was found between both readers in the detection of aneurysms in the anterior and posterior circulation (K = 0.95,P= 0.001) as well as its site in parent artery and segment (K = 0.98,P= 0.001), and (K = 0.98,P= 0.001). In this study, Acom was the most affected artery, and Acomleft anterior cerebral artery (ACA) complex was the most affected segment. Both readers successfully detected intracranial aneurysms in relatively rare locations such as basilar perforators (2/L46), distal ACA (4/L46), pericallosal artery (2/L46), and azygous ACA (2/L46). Inter-observer results of the CTA location of the aneurysm are summarized in Table 3.
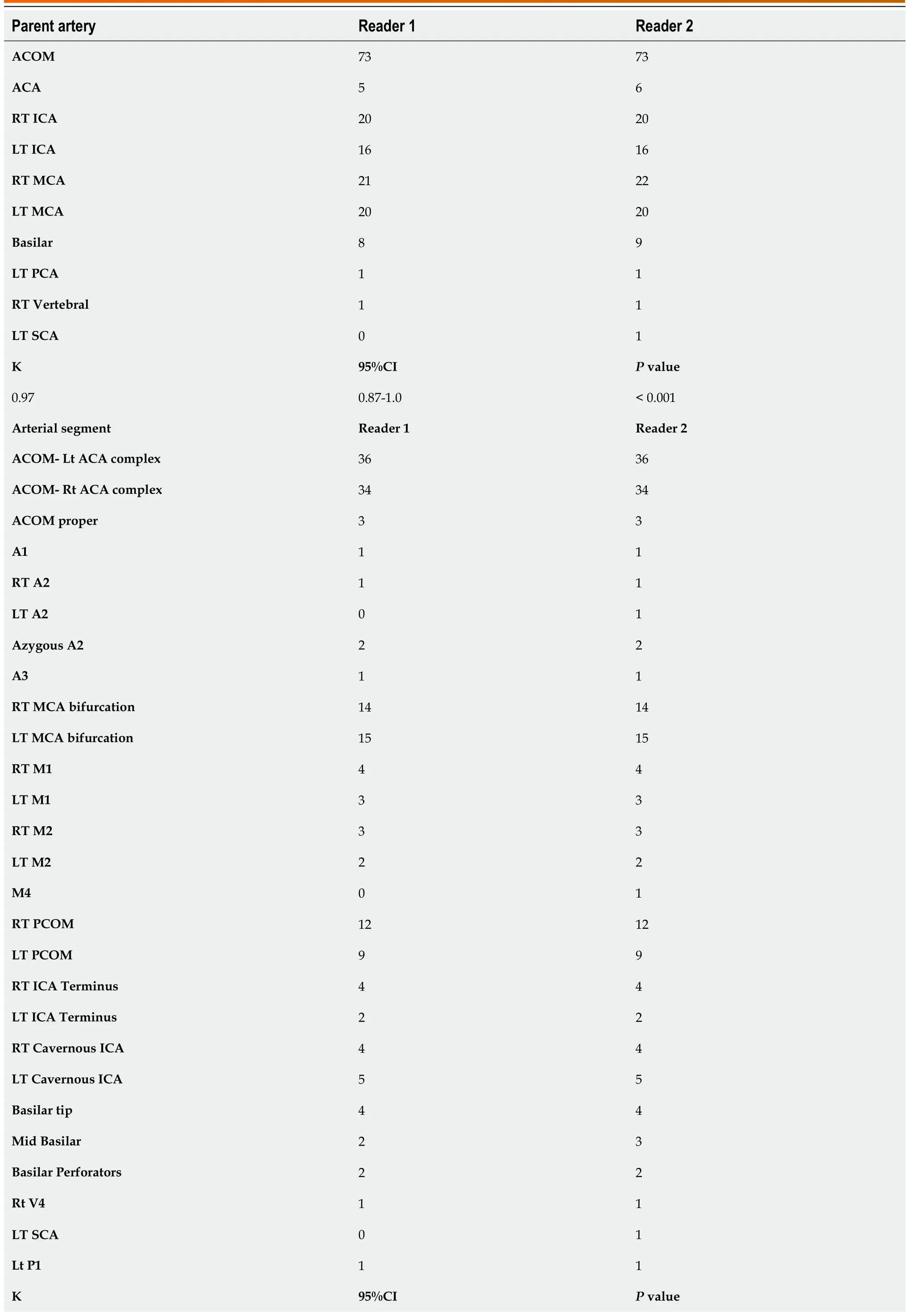
Table 3 Inter-observer agreement of computed tomography angiography locations of aneurysm

ACA: Anterior cerebral artery; RT: Right; ICA: Internal carotid artery; LT: Left; MCA: Middle cerebral artery; PCA: Posterior cerebral artery; SCA: Superior cerebellar artery; PCOM: Posterior communicating artery.
Morphology: Among the assessed aneurysms, (96.4%) were saccular, (2.4%) were fusiform, and (1.1%) were serpentine (Figure 3). Excellent interobserver agreement was found between both readers in the detection of aneurysm shape (K = 0.92,P= 0.001) and for margins (K = 0.95,P= 0.001). Other features such as calcification or thrombus, branch incorporation, and aneurysm orientation also show excellent inter-observer agreement. Calcification and thrombosis were detected in large and giant aneurysms (Figure 4). Branch incorporation was found in association with 55 aneurysms, one of them showed 3rdA2 segment incorporated Acom aneurysm dome (ACA trifurcation), to the best of the author’s knowledge this association is not reported before in the literature (Figure 5).
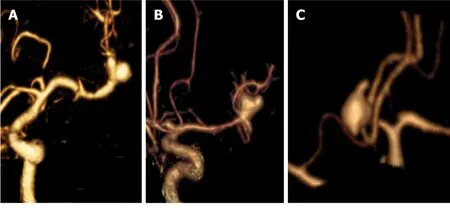
Figure 3 Morphology of intracranial aneurysms. A: Three-dimensional (3D)-computed tomography angiography (3D-CTA) for saccular aneurysm at middle cerebral artery (MCA) bifurcation with smooth margins; B: 3D-CTA for saccular aneurysm at MCA bifurcation with daughter sac; C: 3D-CTA for Acom saccular aneurysm with multiple blebs.
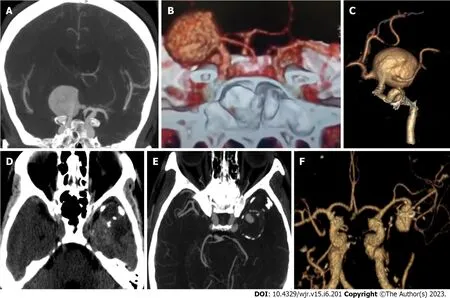
Figure 4 Giant intracranial aneurysms. A: Axial computed tomography angiography (CTA) in maximum intensity projection (MIP); B and C: Three-dimensional (3D)-CTA for giant saccular aneurysm arising from right internal carotid artery and incorporating the origin of anterior cerebral artery and middle cerebral artery (MCA); D: non-contrast computed tomography for another patient shows a well defined lobulated lesion of mixed density in the left temporal lobe with foci of peripheral calcification; E: MIP-CTA axial image shows giant partially thrombosed saccular aneurysm of left MCA; F: 3D-CTA image shows a patent portion of left MCA aneurysm.
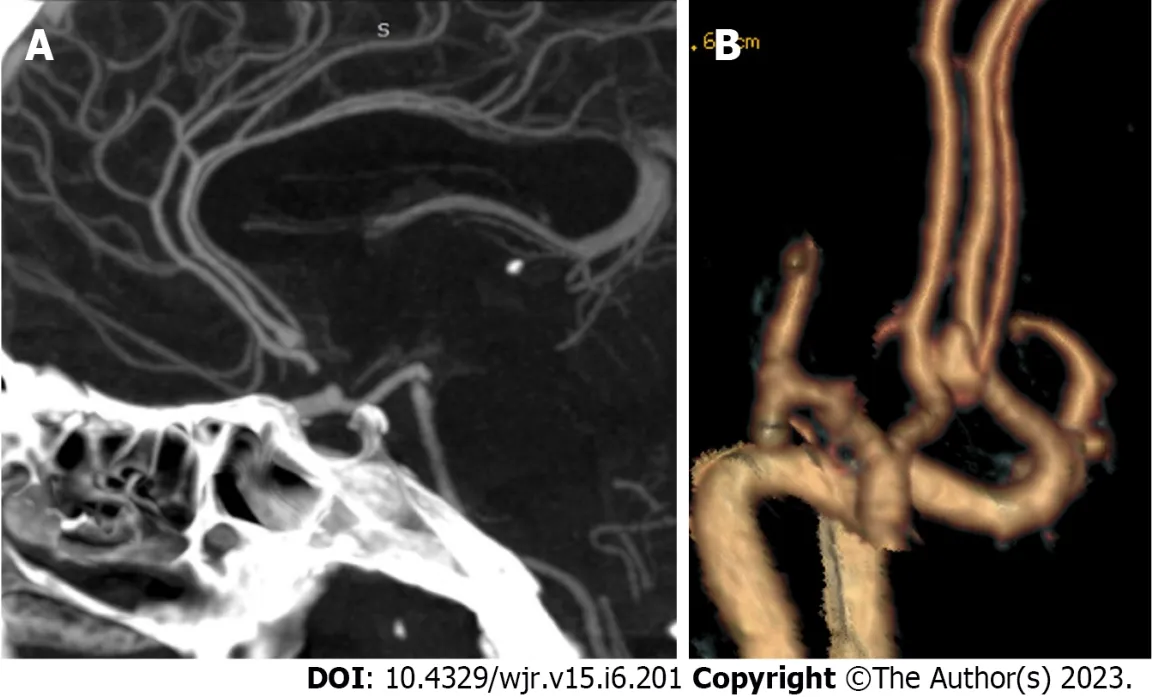
Figure 5 Anatomical variants with intracranial aneurysms. A: Sagittal reformatted maximum intensity projection-computed tomography angiography (CTA); B: Three-dimensional-CTA for a saccular aneurysm at anterior cerebral artery trifurcation.
Measurements:Most cases were medium-sized aneurysms (60.8%), followed by small-sized (30.1%). Both readers measured aneurysm size, neck, and dome-to-neck ratio with an excellent interobserver agreement (K = 0.89,P= 0.001), (K = 0.85,P= 0.001), and (K = 0.98,P= 0.001). Inter-observer results of CTA measurements of an aneurysm are summarized in Table 4.
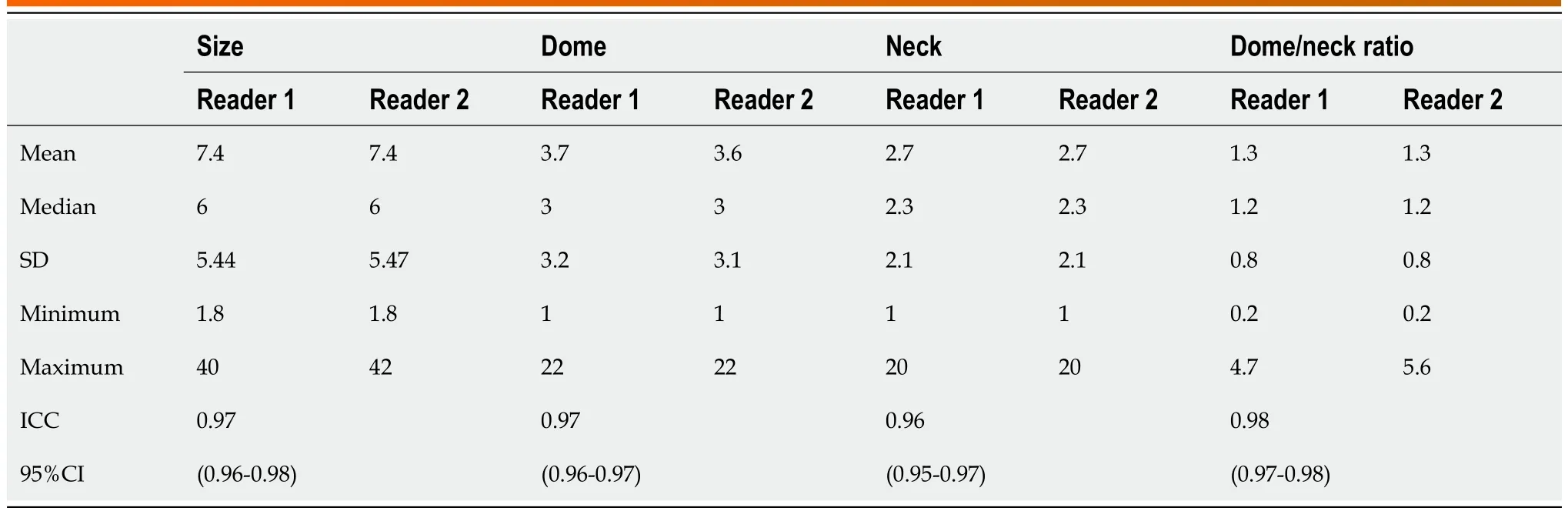
Table 4 Inter-observer agreement of computed tomography angiography measurements of aneurysm
Peri-aneurysm findings:Excellent interobserver agreement was found between both readers in detecting vasospasm in the nearby arterial segment (K = 0.91,P= 0.001) and detection of the perian-eurysmal cyst (K = 1.0,P= 0.001). Associated vascular lesions, including arterio-venous malformation (AVM) and developmental venous anomalies (DVA) (Figure 6), were detected by both readers with an excellent interobserver agreement (K = 0.83,P= 0.001). Vascular variations commonly affected the A1 segment, followed by PCA and MCA. Both readers detected an important bony variant in a case presented with a PCOM aneurysm in the form of a bridging sella turcica which was managed surgically by clitoridectomy (Figure 7).
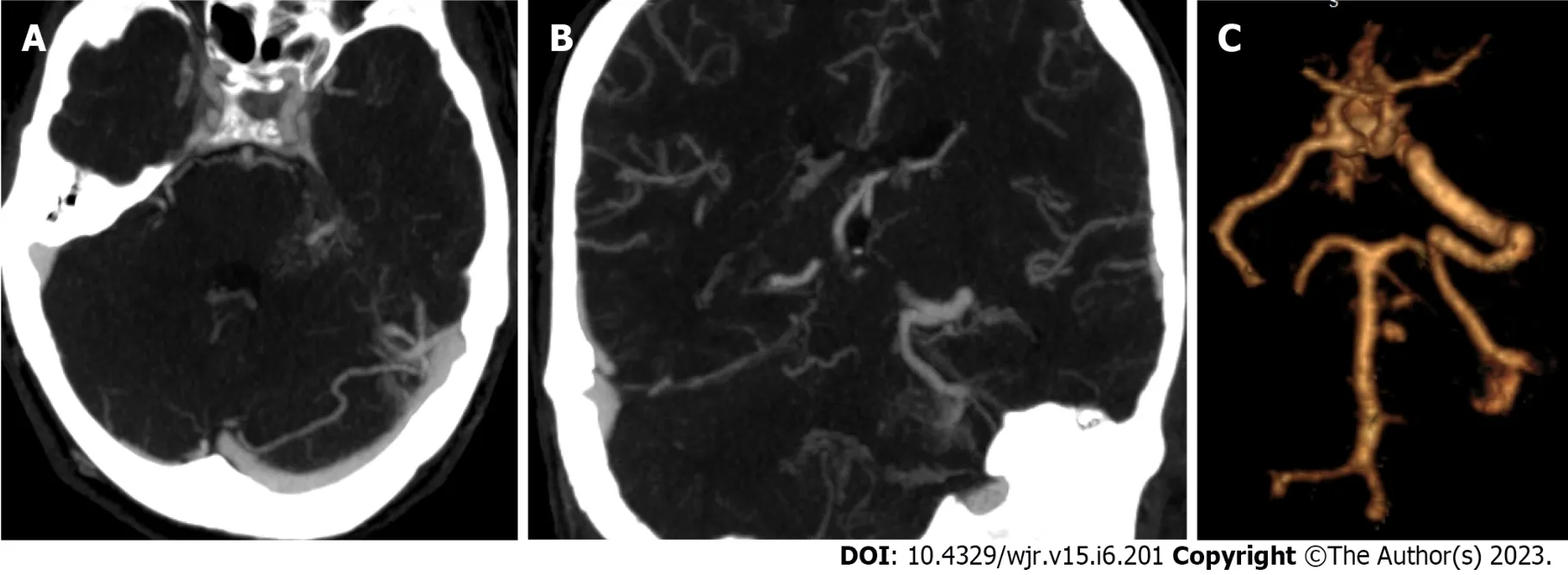
Figure 6 Vascular malformation with intracranial aneurysms. A: Axial maximum intensity projection (MIP)-computed tomography angiography (CTA) shows a small saccular aneurysm that arises from the left basilar artery perforators; B: Coronal reformatted MIP-CTA shows left cerebellar developmental venous anomalies (DVA) drains into the left sigmoid sinus; C: Three-dimensional-CTA shows the basilar perforator aneurysms and the left cerebellar DVA.
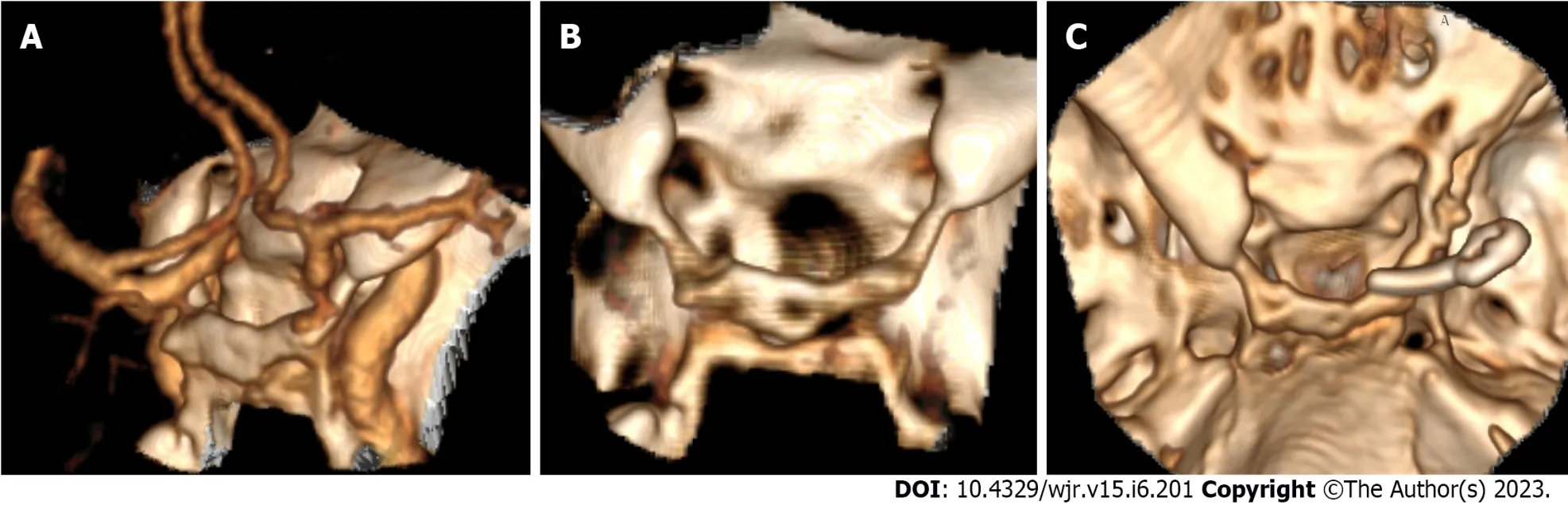
Figure 7 Bony landmarks related to the aneurysm. A: Three-dimensional (3D)-computed tomography angiography shows a posterior communicating artery aneurysm close to the anterior clinoid process; B: 3D-computed tomography (CT) for the skull base shows bridging sella and bony fusion; C: Post-operative 3D-CT shows partial clionoidectomy and metallic clip.
Management:Based on imaging features, 87 patients were recommended to have endovascular treatment, while surgery was recommended in 59 patients. 71.2% of the study population underwent the recommended therapy, as 19 patients did not receive any therapy for the culprit, 66 underwent endovascular treatment, and 61 underwent surgical clipping. Only 15% of the study population needed external ventricular drain (EVD) to manage associated hydrocephalus.
DISCUSSION
This study evaluated the interobserver reliability of CTA in the assessment of ruptured intracranial aneurysm features among 146 patients. Our results showed good to an excellent inter-observer agreement in imaging features related to the aneurysm, aneurysm characters, measurements, and perianeurysmal information. Imaging data extracted from NCCT and CTA guided the multidisciplinary neurovascular team to better treatment approach selection.
Our results showed high sensitivity of NCCT (85%) in predicting aneurysms’ location depending on blood distribution with a good inter-observer agreement regarding the Fischer scale scores for SAH. The combination of NCCT images and CTA is a valuable tool for detecting intracranial aneurysms and predicting outcomes. Aneurysm detection could be expected by assessing the distribution of SAH, the site of the largest clot, the difference in attenuation, and the presence of mural calcification. A recent study performed on patients with SAH and multiple cerebral aneurysms found that NCCT can identify the source of bleeding with high accuracy for ACA, ACom, and MCA aneurysms, especially with the presence of intracranial hemorrhage (ICH)[10]. Our results showed excellent inter-observer agreement for detecting acute hydrocephalus with a variable degree of acute ventricular dilation, yet only 15% of our cases need management by EVD. Our results were close to those of the study performed on 389 patients with aneurysm-associated SAH[11].
We found that CTA has a high sensitivity for detecting intracranial aneurysms and avoids falsenegative results. In a meta-analysis of extracted data from 8 studies, CTA had a pooled sensitivity of 99% and specificity of 94% for detecting and ruling out cerebral aneurysms[12]. Our study had an excellent interobserver agreement for detecting the aneurysms; the first reader detected 166 aneurysms, while the second reader detected 169 aneurysms. Yanget al[8] revealed a similar discrepancy in number detection by two observers, as one reviewer missed three aneurysms[8]. The inter-observer discrepancy usually occurs in a set of multiple small aneurysms in uncommon locations, such as the distal MCA. In this study, we detected mirror MA in 7 patients. Our results concord with the data obtained by a recent study by Rajagopalet al[13].
In our study, the anterior cerebral circulation aneurysms remained the predominant location of all aneurysms detected by CTA, constituting about 94% of the anterior and 6% of the posterior circulation. Acom aneurysm is the most common location of aneurysm in our results followed by ICA and MCA aneurysms, respectively. A similar distribution was reported by previous studies that assessed CTAvsDSA in the detection of intracranial aneurysms[14,15]. Imaging is vitally important to determine the location of the aneurysm and its relationship to the surrounding anatomy. Data from many studies suggest that surgical clipping may be superior in managing anterior circulation aneurysms with low recurrent rates. In contrast, posterior circulation aneurysms may be better treated through an endovascular approach[16]. Both readers successfully detected intracranial aneurysms in relatively rare locations, such as basilar perforators and azygous ACA. These findings aligned with prior studiesstating that basilar perforator aneurysms are sporadic lesions often not recognized on initial imaging[17,18]. Similarly, azygos ACA aneurysm has a low incidence among intracranial aneurysms in literature ranging from 0.38 to 3.7%[19].
In this study, non-saccular intracranial aneurysms were less frequent. The margins were sharp (42.7%), and the rest were lobulated. These results partially agree with Raiet al[15], who reported 91% of saccular aneurysms, with only 22% having lobulated margins[15]. An irregular margin or lobulation along the margin of an aneurysm suggests rupture. It is an important observation in the setting of diffuse SAH and multiple intracranial aneurysms when treatment is directed at the culprit aneurysm[20]. Excellent inter-observer agreement was found in the assessment of branch incorporation and aneurysm orientation. The location of a branch to the aneurysm is a critical finding, as inadvertent occlusion of this branch during aneurysm treatment could have devastating consequences[21]. Therefore, it is essential to have a basic understanding of cerebral circulation and anatomical variants when interpreting CTA studies. Aneurysm orientation, especially Acom aneurysm, is a crucial element in selecting surgicalvsendovascular management. Aneurysms with a more complex surgical approach are often assessed for endovascular therapy rather than surgical management[22].
Excellent agreement was found in this study between both readers regarding aneurysm measurements, including size, neck diameter, and dome-to-neck ratio. As the size of the aneurysm is the most significant predictor of SAH risk, accurate measurement of the aneurysm (s) is imperative for proper management. Aneurysms larger than 12 mm had a 2.6 relative risk of poor outcomes[23]. Kimet al[24] stated that intra-observer and interobserver variability in CTA were considerable in aneurysmal size measurements ranging from 12 to 18%. Therefore, follow-up size changes exceeding 20% in the aneurysm dimension should be considered a true change rather than a measurement error[24]. In contrast to these results, another study reported a poor ability of CTA to identify aneurysm enlargement accurately in assessing an in-vitro model. However, they recommended further human studies to confirm their findings[25]. CTA in this study detected the neck of all saccular aneurysms by both readers. Neck dimension and neck-to-dome ratio are crucial to deciding between surgical or endovascular treatment and simple coiling or adjunctive techniques to facilitate coil embolization through wide neck, such as neck remodeling using balloons or stent-assisted embolization[26].
The majority of our cases were medium-sized aneurysms (60.8%). This finding was in line with results reported by previous studies, which noted that medium-sized aneurysms were the majority of intracranial aneurysms[14,15]. We also observed that the presence of thrombosis and calcification was strongly tied to aneurysm size in large-sized and giant aneurysms compared to the corresponding intraoperative details of each case. Spontaneous thrombosis of intracranial aneurysms may occur in up to 40% of giant aneurysms, eventually becoming symptomatic due to mass effect or stroke. On the contrary, spontaneous thrombosis of a non-giant aneurysm (< 25 mm) is rarer[27]. Calcification appears to be an important pre-operative indicator of poor outcomes[28] and should be considered when deciding treatment options for a patient with a calcified aneurysm.
Perianeurysmal findings such as vasospasm, perianeurysmal cyst, associated vascular lesions or variants, and bony landmarks or pathologic changes are essential factors that might change the treatment decision. Cerebral vasospasm and resultant delayed cerebral ischemia consider a significant etiology of morbidity and mortality in patients with aneurysmal SAH (DCI)[29]. CTA is a fast and reliable tool for detecting decreases in vessel caliber, as demonstrated by excellent interobserver agreement in this study.
The rarity of a perianeurysmal cyst may lead to a false diagnosis of cystic neoplasm and missing the possibility of a ruptured cerebral aneurysm. Interestingly, a perianeurysmal cyst was described in one out of 146 patients in our study. Pedro and Sih[30] reported a case of a sizeable pontine cyst associated with an enhancing mural nodule that was misdiagnosed as a cystic neoplasm. During surgery, an aneurysm of the left PCA was identified and clipped successfully[30].
Our work included four patients with associated vascular anomalies, including AVMs and DVA. The risk of intracranial hemorrhage in patients with coexisted AVM and aneurysm has been reported to be 7% annually, compared with 2%-4% annually for those with AVM alone or isolated intracranial aneurysm[31,32]. To our knowledge, the association between intracranial aneurysms and DVA is infrequent, and few case reports have been published[33].
In our study, both observers noted a sphenoid bone fracture and a nearby aneurysm of paraclinoid ICA secondary to head trauma. It is in agreement with results done on 5532 patients with cerebral aneurysms over 30 years by Junget al[34], who state that traumatic intracranial aneurysm (TIA) after blunt brain trauma is rare and represents (0.23%)[34]. Osseous landmarks such as the optic strut and the tuberculum sellae are considered the anatomical boundary between the intradural and extradural segments of the ICA in the paraclinoid region, which is an important factor in determining treatment strategy[35].
We recommended surgical clipping or endovascular management for the culprit aneurysms based on data extracted from NCCT and CTA. 71.2% of the study population underwent the recommended therapy. The ideal therapeutic approach for RIAs is still controversial. In general, the decision on whether to clip or coil depends on several factors related to the patient, such as age and comorbidities, burden, and location of hemorrhage, aneurysm characteristics such as size, number, location, and morphology, or related procedure such as competence, technical skills and availability[36]. Endovascular treatment has been associated with shorter recovery but with higher retreatment rates and slightly higher rebleeding events[16]. An endovascular approach is indicated in a ruptured intracranial aneurysm with comorbidity, old age, narrow neck, and a posterior circulation aneurysm. Surgery is warranted if the patient is young with an MCA aneurysm and interested in durability.
There are a few limitations to this study. First, there is no correlation with conventional angiography in all cases. Second, the general drawbacks of CT include patient exposure to ionizing radiation and the risks of iodinated contrast medium. Further studies with applications of low-dose CTA, such as the use of automatic tube current modulation and a small amount of contrast medium, are recommended. Additionally, future studies using advanced CT techniques such as higher 320 slices CT scan[37], dualenergy[38] or source CTA, and time-resolved 4D CTA will improve temporal and spatial resolution and the image quality CTA. Also, applications of advanced vascular post-processing packages for analyzing CTA images will give comprehensive image interpretation in different planes and angles. We recommend further studies assessing the inter-observer agreement between neuroradiologists, neurologists, neurosurgeons, and neuro-interventionist.
CONCLUSION
We concluded that CTA is a promising diagnostic imaging modality for assessing intracranial aneurysm features that impact management and patient outcomes.
ARTICLE HIGHLIGHTS
Research background
Aneurysmal subarachnoid hemorrhage (SAH) is an emergency that can lead to a high mortality rate and many severe complications. It is critical to make a rapid radiological evaluation of ruptured intracranial aneurysms (RIAs) to determine the appropriate surgical treatment.
Research motivation
The high morbidity and mortality of RIAs nicissitate rapid diagnosis and management decision.Compared to Digital subtraction angiography, computed tomography angiography (CTA) is a safe,relatively inexpensive, and noninvasive imaging. Computed tomography (CT) angiography is not associated with significant patient risks other than those related to administering iodinated contrast media. Images can be relatively safely obtained without the need for arterial puncture or catheter manipulation that carries the possibility of acquiring a permanent neurologic deficit. Our motivation is to assess the reliability of CTA in assessing different features of ruptured intracranial aneurysm and its impact on patient management.
Research objectives
To assess the reliability of CTA in assessing different features of ruptured intracranial aneurysm and its impact on patient management. We found out that CTA is a promising diagnostic imaging modality for assessing intracranial aneurysm features and help in management decision and patient outcomes. We recommend further studies assessing the inter-observer agreement between neuroradiologists, neurologists, neurosurgeons, and neuro-interventionist.
Research methods
Helical cerebral CT angiography has been widely used in detecting intracranial aneurysms, with a reported sensitivity of 70%-96%. Currently, multidetector CT angiography has the ability to detect most intracranial aneurysms of 5 mm or larger. Multidetector row CT scanners provide increased spatial resolution and decreased scanning time, which should increase the sensitivity of the technique in depicting aneurysms of less than 5 mm in diameter. Currently, CT angiography is accepted as a firstline diagnostic imaging modality for evaluating intracranial aneurysms. Nevertheless, using CT angiography to depict intracranial aneurysms showed variable sensitivity. The reported sensitivity of CTA in detections of small intracranial aneurysms (< 3 mm) varied from 28%-43% in a study that included 99 small aneurysms to 83%-92% in another study had 579 small aneurysms. CTA examinations for 146 patients in the current study were revised and interpreted by two experienced neuroradiologists to assess the inter-observer agreement of CTA findings related to intracranial aneurysms. Data extracted from CT was considered in patient management decision.
Research results
This study evaluated the interobserver reliability of CTA in the assessment of ruptured intracranial aneurysm features among 146 patients. Our results showed good to an excellent inter-observer agreement in imaging features related to the aneurysm, aneurysm characters, measurements, and perianeurysmal information. Imaging data extracted from NCCT and CTA guided the multidisciplinary neurovascular team to better treatment approach selection. There are a few limitations to this study. First, there is no correlation with conventional angiography in all cases. Second, the general drawbacks of CT include patient exposure to ionizing radiation and the risks of iodinated contrast medium.
Research conclusions
We concluded that CTA is a promising diagnostic imaging modality for assessing intracranial aneurysm features that impact management and patient outcomes. We recommend endovascular approach in a ruptured intracranial aneurysm with comorbidity, old age, narrow neck, and a posterior circulation aneurysm, and surgical clipping is warranted if the patient is young with an MCA aneurysm and interested in durability.
Research perspectives
Further studies with applications of low-dose CTA, such as the use of automatic tube current modulation and a small amount of contrast medium, are recommended. Additionally, future studies using advanced CT techniques such as higher 320 slices CT scan, dual-energy or source CTA, and timeresolved 4D CTA will improve temporal and spatial resolution and the image quality CTA. Also, applications of advanced vascular post-processing packages for analyzing CTA images will give comprehensive image interpretation in different planes and angles.
FOOTNOTES
Author contributions:Abdel Razek A and El-Serougy LG proposed the study concept and design; Elged BA searched Database; Kasem MA performed surgical procedures; Elmokadem AH performed DSA; Elged BA, EL-Adalany MA, and El-Serougy LG contributed to analysis and interpretation of data; Elged BA and Elmokadem AH contributed to drafting of the manuscript; Elmokadem AH and Abdel Razek A contributed to Revision of the manuscript; ELAdalany MA and El-Serougy LG supported technical, or material.
Institutional review board statement:The study was approved by Mansoura university institutional review board (IRB).
Informed consent statement:Patients were not required to give a written consent for the study as the analysis used anonymous data.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:All data generated or analyzed during this study are included in this published article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Egypt
ORCID number:Ali H Elmokadem 0000-0001-5119-9548; Basma Abdelmonaem Elged 0000-0002-7442-9673; Ahmed Abdel Razek 0000-0002-9613-5932; Mohamed Ali Kasem 0000-0002-2633-6472; Mohamed Ali EL-Adalany 0000-0001-8226-7814.
S-Editor:Li L
L-Editor:A
P-Editor:Zhao S
 World Journal of Radiology2023年6期
World Journal of Radiology2023年6期
- World Journal of Radiology的其它文章
- Computed tomography angiographic study of surgical anatomy of thyroid arteries: Clinical implications in neck dissection
- Radiological parameters to predict pancreatic texture: Current evidence and future perspectives
- Role of contrast-enhanced serial/spot abdominal X-rays in perioperative follow-up of patients undergoing abdominal surgery:An observational clinical study
- Acute pancreatitis: Structured report template of magnetic resonance imaging