
Hem-o-lok clip migration to the common bile duct after laparoscopic common bile duct exploration: A case report
2022-12-19 08:08:26DaRenLiuJinHongWuJiangTaoShiHuanBingZhuChaoLi
World Journal of Clinical Cases 2022年19期
关键词:机会
Da-Ren Liu,Jin-Hong Wu,Jiang-Tao Shi,Huan-Bing Zhu, Chao Li
Abstract
Key Words: Laparoscopic cholecystectomy; Laparoscopic common bile duct exploration; Surgical clip; Postoperative migration; Case report
lNTRODUCTlON
Gallbladder stone combined with common bile duct (CBD) stone is a common disease in developed countries, with a prevalence ranging from 8% to 18%[1]. Laparoscopic cholecystectomy (LC) and laparoscopic common bile duct exploration (LCBDE) are widely used procedures for the treatment of cholelithiasis combined with choledocholithiasis. Clearly dissecting the Carlo’s triangle and properly closing the cystic artery and cystic duct are the key steps of this surgery. Hem-o-lok clips are commonly used to ligate gallbladder blood vessels and cystic ducts. Complications of LCBDE include bile leakage, stone recurrence, infection, bleeding, and postoperative clip migration.
Postoperative clip migration is a rare but well-established complication of laparoscopic biliary surgery. The clip may migrate to CBD[2-12], T-tube sinus wall[11,13], duodenum[8,14], or the pulmonary artery[15]. Herein, we report a case of clip migration after LC and LCBDE and review cases of clip migration reported in literatures after LC or LCBDE, hoping to draw lessons from these cases.
CASE PRESENTATlON
Chief complaints
A 59-year-old woman presented to the emergency department of our hospital complaining of fever and right upper abdominal pain for 3 d.
History of present illness
The patient’s symptoms started 3 d ago with fever and acute right upper abdominal pain, which had worsened in the last 24 h.
History of past illness
The patient had a history of LC and LCBDE surgery 2 mo ago.
Personal and family history
The patient has no personal and family history.
Physical examination
The patient’s temperature was 38.9 °C, heart rate was 93 bpm, respiratory rate was 18 breaths per minute, blood pressure was 105/60 mmHg, and oxygen saturation in room air was 99%. Physical examination revealed that the abdomen was soft, but tenderness was present in the right upper quadrant of abdomen without rebound tenderness.
左达拿过徐艺面前的两万放在自己面前,盯着徐艺说:“你看,我的赌注变四万了,刺激吧?这么赌下去,你的机会可越来越少了。”
Laboratory examinations
Laboratory examination showed aspartate aminotransferase 639 U/L, alanine aminotransferase 681 U/L, and total bilirubin 74 μmol/L. Blood routine examination showed a white cell count of 16.1 × 109/L, a neutrophil percentage of 89%, and a hemoglobin of 135 g/L.
Imaging examinations
Computed tomography scan demonstrated a slightly dilated common bile duct with a high-density shadow at the distal CBD, which was considered as migrated clips (Figure 1). Therefore, endoscopic retrograde cholangiopancreatography (ERCP) was performed, which confirmed that Hem-o-lok clips migrated into the CBD (Figure 2A).
FlNAL DlAGNOSlS
Acute cholangitis caused by migrated Hem-o-lok clips applied in the LC and LCBDE surgery.
TREATMENT
Two displaced Hem-o-lok clips were removed by stone basket after sphincterotomy through ERCP (Figure 2B and C).
OUTCOME AND FOLLOW-UP
No fever or abdominal pain was presented after the operation, and the patient was discharged 3 d later in a stable condition. There was no abdominal pain, jaundice, abdominal pain, or other discomfort during the follow-up period.
DlSCUSSlON
Choledocholithiasis is a common disease, with an incidence increasing year by year. Comparing to open surgery, the LCBDE is safe, effective, minimally invasive, and has an faster recovery rate[16]. Advances in laparoscopy have made LC and LCBDE a widely accepted strategy for patients with gallstones and choledocholithiasis. In our practice, the Carlo's triangle was initially dissected to expose cystic duct and cystic artery, and they were separated and clipped with three and one Hem-o-lok clips, respectively. Secondly, the CBD was exposed, and the anterior aspect wall of CBD was cut with electroacupuncture 1 cm below the confluence of cystic duct and CBD, and the cholesterol crystals were removed by basket under direct view. Thirdly, a 24# Silicone T-tube was placed into the CBD, which was then sutured with a 4-0 Vicryl. Finally, the gallbladder was resected using electroacupuncture, and T-tube was set on the right abdominal through the incision of rectus abdominis. Postoperative clip migration is a rare complication of laparoscopic cystic and biliary operation, which has been occasionally presented as case report. Migrated clips in the bile duct may function as a nidus for gallstone formation, leading to biliary obstruction, acute pancreatitis, duodenal ulcer, biliary-colonic fistula, and subdiaphragmatic abscess. Any type of surgical clip has a risk of migration. If a patient with a history of receiving LC or LCBDE presents with features of recurrent upper quadrant pain, with or without sepsis or liver function test derangement, clip displacement must be considered as one of the differential diagnosis.
We searched through MEDLINE, PubMed, Scopus, Web of Science, Google Scholar, and the CNKI databases using the keywords ’clip migration and laparoscopic cholecystectomy (LC) or clip migration and laparoscopic common bile duct exploration (LCBDE)’ from 1990 to 2021. A total of 14 articles including 36 cases about clip migration after LC or LCBDE have been reported[2-15] (Table 1). Twentyfive cases received LC and LCBDE (69.4%) and 11 cases received LC (30.6%) as previous laparoscopic surgery. The age of patients ranged from 31-years-old to 83-years-old. Symptoms occurred from 1 mo to 7 years after laparoscopic surgery. Nineteen patients remained asymptomatic that were mainly diagnosed by choledochoscopy through T-tube sinus tract. The most common manifestations due to clip migration were abdominal pain, fever, and jaundice, which were similar to those of non-iatrogenic choledocholithiasis. In 27 cases, the clips wedged into the CBD (75%), while the clips became a part of Ttube sinus in 6 cases (16.7%) and the clips migrated into duodenum in 2 cases (5.6%). The types of clips include Hem-o-lok (61.1%), metallic (16.7%), and absorbable (8.3%). Initial treatment included removing clips by basket in ERCP, endoscopic removal, and observation, while surgical treatment was required in 6 cases.
The mechanism of postoperative clip migration remains controversial; however, some possible hypotheses of pathogenesis were suggested. Firstly, inappropriate application of surgical clips, including improper placement of clips and incomplete closure of cyst duct may lead to the formation of biloma, which would be reabsorbed later into the bile duct and leave the clips behind[2]. Secondly, the compression of clips to the bile duct wall caused by the surrounding structures or a pulled cystic duct during operation may result in clip corroding into the lumen of CBD[17]. Additionally, the number of clips used in surgery is also an important factor[5,18]. Thirdly, bile leakage caused by an intraoperative bile tract injury and the subsequent inflammation make surrounding tissues brittle, which may induce clips to invade into the biliary tract through the incision of CBD mechanically[17]. In addition, the pressure exerted from abdominal organ movements accelerates the process of clip migration[10,18]. Finally, the rejection response by the immune system to clips as a foreign body may also contribute to the displacement of surgical clips[4].
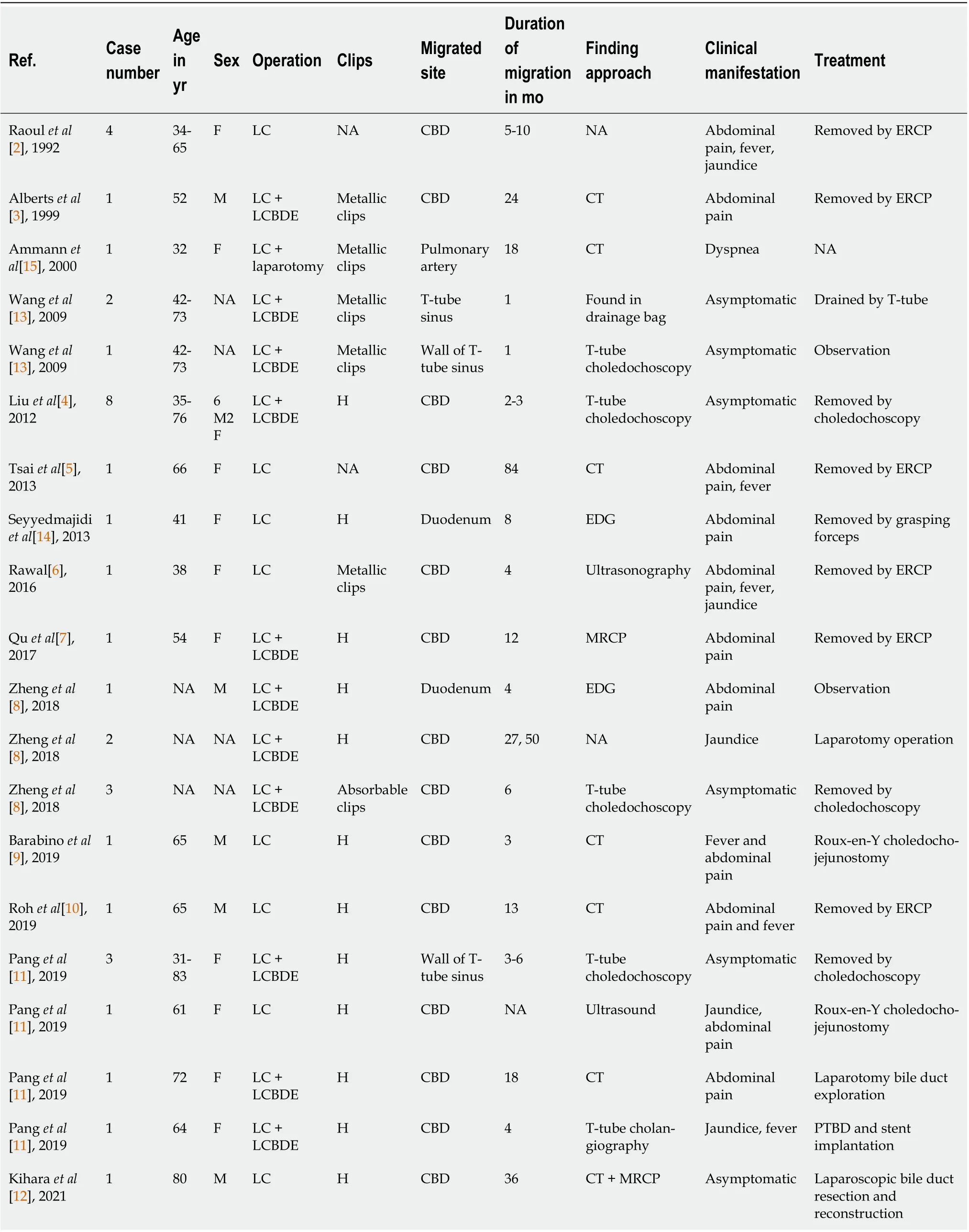
Table 1 Summary of cases of surgical clips migration after laparoscopic biliary surgery

Figure 2 Migrated Hem-o-lok clips were detected and removed by endoscopic retrograde cholangiopancreatography. A: Endoscopic retrograde cholangiopancreatography (ERCP) showed the filling-defect in the common bile duct corresponding to the migrated Hem-o-lok clips (red arrow); B and C: Hem-o-lok clips were removed by stone basket by ERCP.
In order to reduce the incidence of postoperative clip migration, all technical factors in surgery should be considered. During the operation, the relationship of Calot’s triangle should be carefully confirmed, and the placement of surgical clips should not be too close to the CBD; the number of clips should be minimized, and unnecessary surgical procedures should be avoided, such as the blind application of clips to control bleeding[19]. It has also been suggested that the risk of postoperative clip migration can be lowered by using absorbable clips when compared with non-absorbable clips; however, reports about absorbable clip migration still exists[4,8], including a report by Cettaet al[20], which suggested that absorbable clips could also cause postoperative clip migration and be a nidus of stone formation. Furthermore, new vessel and duct sealing technologies such as a Harmonic scalpel can be applied as an alternative to clips in laparoscopic operation. The Harmonic scalpel is well accepted as a reasonable alternative for closure of cystic duct, which occupies the advantages of shorter operation time, fewer complications, and avoiding clip migration[21].
CONCLUSlON
In summary, although postoperative clip migration is rare, it is a well-recognized phenomenon and cannot be ignored. Any type of surgical clip has a risk of displacement. Using clips properly and correctly, as well as exploring new methods to occluded cystic duct may help to reduce the incidence of postoperative clip migration. If patients with a past history of LC with or without CBD exploration present with features of sepsis and recurrent upper quadrant pain, with or without derangement of liver function test, clip migration may be considered as one of the differential diagnoses.
FOOTNOTES
Author contributions:Liu DR, Wu JH, and Shi JT were the patient’s surgeons, reviewed the literature, and drafted the manuscript (contributed equally to this article); Zhu HB and Li C reviewed the literature and contributed to manuscript drafting; Liu DR and Li C were responsible for the revision of the manuscript for important intellectual content; All authors issued final approval for the version to be submitted.
Supported byMedical and Health Technology Plan of Zhejiang Province, No. 2019RC179.
lnformed consent statement:Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:The authors declare that they have no conflict of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Da-Ren Liu 0000-0001-9551-8854; Jin-Hong Wu 0000-0001-6415-0508; Jiang-Tao Shi 0000-0002-4500-7762; Huan-Bing Zhu 0000-0003-0359-5057; Chao Li 0000-0003-3319-8896.
S-Editor:Gong ZM
L-Editor:Filipodia
P-Editor:Gong ZM
猜你喜欢
大众健康(2020年8期)2020-08-26 07:50:47
学生天地(2020年26期)2020-06-01 02:17:26
海峡姐妹(2020年3期)2020-04-21 09:27:40
NBA特刊(2018年17期)2018-11-24 02:45:44
现代营销(创富信息版)(2018年6期)2018-09-05 03:14:40
海峡姐妹(2018年6期)2018-06-26 07:27:20
儿童时代·快乐苗苗(2017年6期)2018-03-09 20:19:20
散文诗(2017年22期)2017-06-09 07:55:27
高中生·青春励志(2016年12期)2017-03-01 11:41:27
新高考(英语进阶)(2016年12期)2016-02-28 21:58:11
 World Journal of Clinical Cases2022年19期
World Journal of Clinical Cases2022年19期
- World Journal of Clinical Cases的其它文章
- Preliminary evidence in treatment of eosinophilic gastroenteritis in children: A case series
- Identification of risk factors for surgical site infection after type II and type III tibial pilon fracture surgery
- Sustained dialysis with misplaced peritoneal dialysis catheter outside peritoneum: A case report
- Delayed-onset endophthalmitis associated with Achromobacter species developed in acute form several months after cataract surgery: Three case reports
- Diagnostic accuracy of ≥ 16-slice spiral computed tomography for local staging of colon cancer: A systematic review and meta-analysis
- Family relationship of nurses in COVID-19 pandemic: A qualitative study