
Efficacy of haptic sutured in-the-bag intraocular lens for intraocular lens-capsule complex stability: a comparison of three insertion methods
2022-09-14 06:50:50YangKyungChoAndrewThomsonBalamuraliAmbati
INTRODUCTION
In eyes predisposed to intraocular lens (IOL) dislocation due to zonular insufficiency, devices such as standard and modified capsular tension rings (CTR) with transscleral fixation through the ciliary sulcus are used to add stability of IOL-capsule complex during cataract surgery
. Recently, late in-the-bag IOL subluxation or dislocation due to zonulolysis has been reported with increasing frequency and has been reported as 0.2% to 3%
.
Risk factors for postoperative IOL dislocation include pseudoexfoliation syndrome, prior vitreoretinal surgery, history of trauma, long axial length, uveitis, retinitis pigmentosa, and connective tissue disorders, such as Marfan syndrome
.Certain measures to prevent IOL-bag complex luxation have been proposed in these predisposing eyes: postoperative relaxing cuts of anterior capsulorhexis margin with Nd:YAG laser, intraoperatively, aspiration of cortex directed in a tangential fashion, and preference of a 3-piece hydrophobic acrylic IOL which may reduce continuous curvilinear capsulotomy (CCC) shrinkage through a combination of decreased anterior capsule fibrosis and greater haptic rigidity than a single piece IOL
.
The primary objective of this study was to evaluate the anatomical stability of IOL capsular bag complex; CCC area contracture, CCC shape and IOL tilt. And the secondary objective was to evaluate the resultant refractive stability,refractive change, and ACD.
据介绍,6月份,哈国家磷肥厂宣布投资80亿坚戈(约合2200万美元)用于现代化改造,预计到2020年扩大磷肥产量至50万吨,远期目标为100万吨。今年1~8月,该厂的产品主要销往美国、中国、阿富汗、俄罗斯、乌克兰、塔吉克斯坦和乌兹别克斯坦。同时,哈产氮肥已开始向阿根廷、罗马尼亚、捷克、保加利亚和伊朗出口。
At risk eyes with zonular insufficiency may require transscleral suture fixation which is utilized for both transscleral fixation of IOLs as well as endocapsular supporting devices, such as modified CTR and capsular anchoring devices
.
微网逆变器的VSG转动惯量和阻尼系数自适应控制//温春雪,陈丹,胡长斌,朴政国,周京华//(17):120
SUBJECTS AND METHODS
Institutional Review Board (IRB)/Ethics Committee approval of St. Vincent’s Hospital was obtained(VC21RISI0078). All research was conducted in accordance with the tenets of the Declaration of Helsinki.
A retrospective cohort study with 60 eyes was performed using records of 60 patients undergoing cataract surgery between January 2015 and May 2020 at St. Vincent’s Hospital. Surgeries were performed by one surgeon (Cho YK).Inclusion criteria for patients consisted of 50 or more years of age, clinically significant cataracts with zonular instability,less than 120° (4 clock hours) of zonulolysis, and over 1y of postoperative follow up results. Zonular instability was determined preoperatively by the presence of phacodonesis with or without visible zonular dehiscence in full mydriasis and intraoperatively by marked difficulty in performing the CCC due to lens movement with the presence of zonular dehiscence less than 4 clock hours detected under the operating microscope. Intraoperatively just before IOL insertion, the extent of zonulolysis in clock hours was measured with corneal radial marker with degree gauge. The eyes with phacodonesis in performing the CCC as well as eyes with visible anterior or posterior capsular wrinkling or centripetal movement of anterior capsular margin less than 120° were regarded as eyes with zonulolysis less than 4 clock hours.
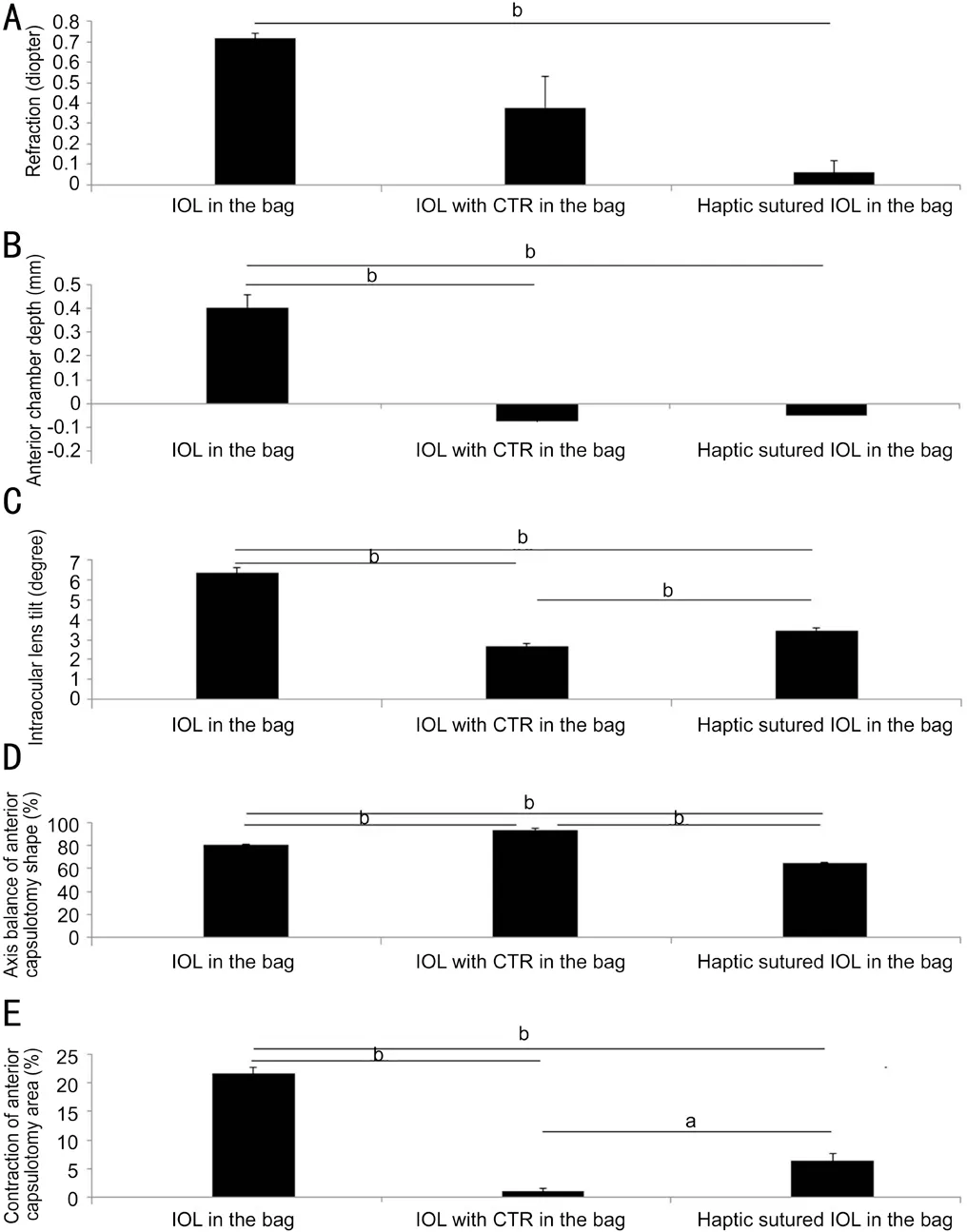
The refractive change between 1mo and 1y for Group 1 was 0.71±0.02 D and showed significant hyperopic change compared to 0.37±0.15 D for Group 2 (
=0.009), and 0.05±0.05 D for Group 3 (
=0.007). There was no significant difference in refractive stability between Groups 2 and 3(Figure 6A).
Surgical patients underwent one of three techniques for IOL (YA60BBR
, Hoya Corp., Tokyo, Japan) insertion(Figure 1) by surgeon’s preference according to the operative situation, such as patient’s cooperation including eye movement, hearing ability, availability of CTR, and reimbursement of medical insurance. Group 1 (IOL in the bag) utilized a three-piece IOL inserted in the bag with haptics oriented toward the areas of zonulolysis. Group 2(IOL with CTR in the bag) had a three-piece IOL inserted after injection of a 12 mm standard CTR (Ophtec, Groningen,The Netherlands). Group 3 (Haptic sutured IOL in the bag)received a three-piece IOL inserted in the bag with novel scleral suture fixation at optic-haptic junction.
下面我们将从国务院及其下属部门,如国家发展和改革委员会、科技部、工业和信息化部、财政部、中国人力资源和社会保障部、自然资源部、生态环境部、水利部、农业农村部、商务部、国家卫生健康委员会、国家市场监督管理总局等各个部委发布的政策、新规、通知等方面来总结一下在2018年我国都出台了哪些政策法规。
At postoperative 1mo and 1y follow-ups,refractive change, anterior chamber depth (ACD), IOL tilt, and CCC were obtained and compared between groups. Refractive changes (reported as spherical equivalent) were measured using an autorefractor keratometer (RK-F1, Canon, Japan).ACD was measured as the distance between the central corneal anterior surface and the anterior surface of the IOL using A-scan ultrasound (AVISO, Carl Zeiss Meditec Ag, France).Negative and positive values between that of preoperative and postoperative 1-year ACD results indicate forward or backward axial movement of the IOL.
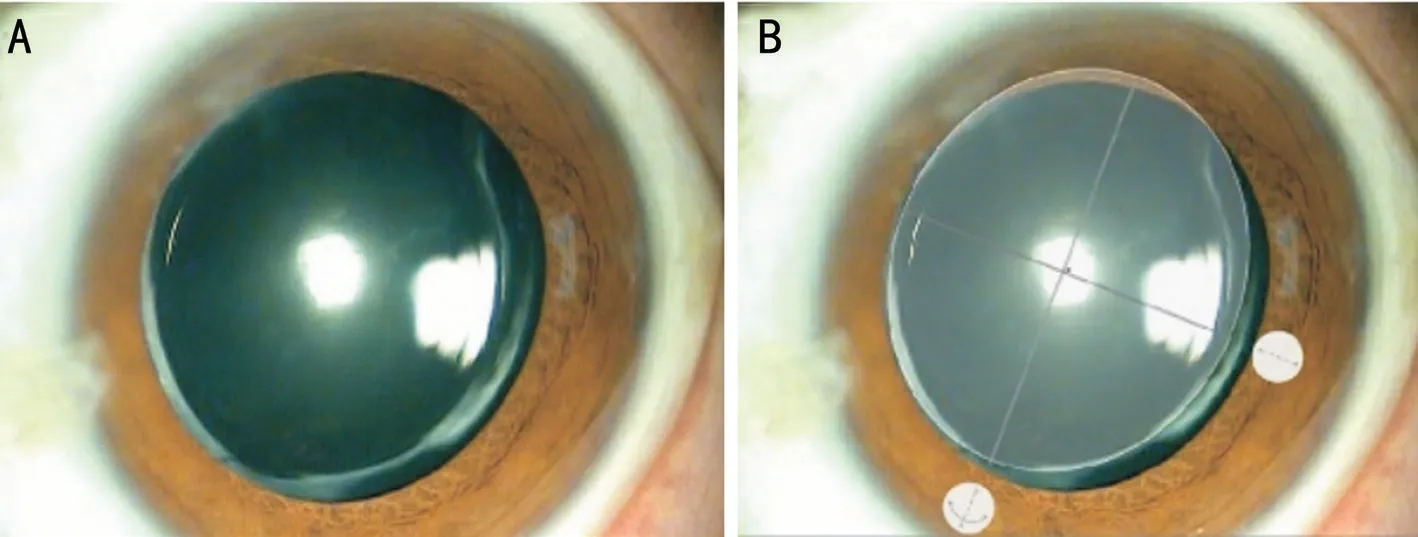
With sufficiently dilated pupils, IOL position was measured using the Oculus Pentacam (Oculus Optikgeräte, Inc., Germany).These measurements were performed by an ophthalmic technician who was blinded to patient IOL insertion method.Two vertical Scheimpflug images of total 25 cross section of the target eye 90° apart were selected, and the mean value of tilt in perpendicular directions was recorded as IOL tilt.
山东威海海洋经济发展示范区的主要任务是发展远洋渔业和海洋牧场,传统海洋渔业转型升级以及与海洋医药、生物制品业融合集聚发展模式创新。日照海洋经济发展示范区则是推动国际物流与航运服务创新发展,开展海洋生态文明建设示范。
The line between the anterior chamber angle (red line in Figure 2B) and the line between the IOL edges (yellow line in Figure 2B) were marked on imaging. The IOL tilt angle between red line and yellow line was measured using the reference line of Scheimpflug image (dotted line in Figure 2A and 2B).
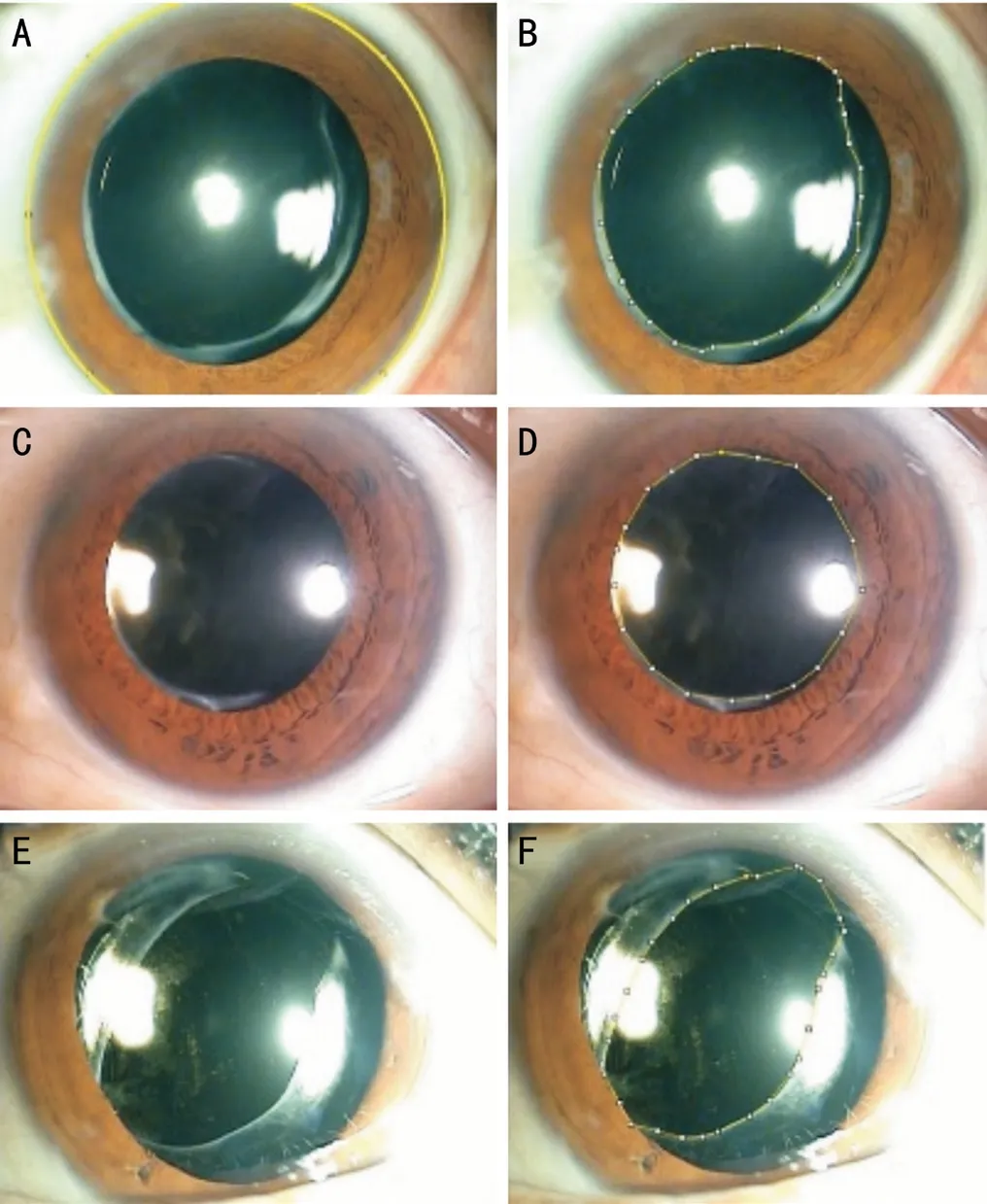
Two aspects of CCC contraction, shape and area, were measured. The shape was evaluated by calculating the CCC axis balance. An ellipse was drawn from the outer tangent lines of the CCC margin and the shortest axis (X axis) and the vertical, longest axis (Y axis) of the ellipse were measured. The axis balance of CCC was calculated (length of X axis ×100%/length of Y axis) and describes the similarity between axes as a percentage. A percentage of 100% denotes a perfect circle, and a smaller percentage nearing 0 denotes a flatter, ovoid shape due to CCC contraction (Figure 3).
从区域分布上看,内蒙古地区“草原丝绸之路”可分为西部段和东部段两部分。西部段以呼和浩特、乌兰察布、包头、鄂尔多斯为重要支点,向西经宁夏、青海与新疆丝绸之路相连;东部段由呼伦贝尔、通辽、赤峰等重要节点城市为依托,连接着俄罗斯、蒙古国,是通往欧洲丝绸之路的重要通道。
SPSS Statistics for Windows software(version 11.5, SPSS Inc, Chicago, IL, USA) was used for the statistical analysis. An analysis of variance test was applied to compare data between Groups, and a post hoc analysis was performed when statistical differences were noted between visits.To compare the causes of zonular dehiscence and postoperative 1-year PCO according to each group, the Chi-square test and Fisher exact test were used, respectively. In all cases, a
value less than 0.05 was considered statistically significant.


The cause of zonular dehiscence was determined by retrospective chart review including history taking, tonometry, slit lamp examination and visual field test.
Here, we describe a simple technique involving a modification to the IOL haptic suture fixation locations. The efficacy of this technique to maintain capsular bag stability was then compared with two other traditional methods, namely, in-thebag IOL insertion with haptics oriented toward areas of zonular dehiscence and in-the-bag IOL insertion with a standard CTR.
After local anesthetization (sub-tenon injection of lidocaine) and sterile draping, the procedure begins with an anterior CCC approximately 5.0-6.5 mm in diameter using a capsule forcep. In eyes with severe phacodoensis,capsular stability was maintained using disposable iris hook(Synergetics
O’Fallon, MO, USA) placed at the anterior capsular margins. Iris hooks were used in eyes with poor mydriasis. Next, routine phacoemulsification cataract surgery was performed and IOL insertion was accomplished by one of three methods. Group 1 receive a three-piece IOL alone with haptics oriented toward areas of zonulolysis, and Group 2 received CTR coimplantation. The novel method used in Group 3 was performed as follows: After irrigation and aspiration and injection of viscoelastics into the capsular bag and prior to IOL insertion, a 10-0 polypropylene double-armed suture was inserted at the 2 and 8 o’clock position (or the 4 and 10 o’clock position) according to the direction of zonulolysis,about 2 mm from the limbus, and docked in a 30-gauge needle in the anterior chamber. The 10-0 polypropylene suture was retrieved through the main incision and cut in half. Next, each end of the polypropylene suture was tied near the three-piece IOL optic-haptic junction. The IOL, now with both haptics tied with polypropylene sutures, was then inserted into the capsular bag. The opposite end of the polypropylene suture was placed through a trans-scleral tunnel, tied, and adjusted (Video 1,online supplementary).
The posterior capsular opacity (PCO) at postoperative 1-year follow up were measured using slit lamp microscopic examination according to the grading by Congdon
as follows: absent (Grade 0), no opacity or opacity limited to the peripheral capsule; Grade 1, any wrinkling or opacity of the capsule affecting a circle 4 mm in diameter and centered on the visual axis ; Grade 2, central/paracentral opacity as described above sufficient to degrade details of the macula slightly;Grade 3, central/paracentral opacity as defined above, but sufficient to make ascertainment of the cup/disc ratio difficult;Grade 4, central/paracentral opacity as defined above, but sufficient to make visualization of fundus details difficult or impossible.
RESULTS
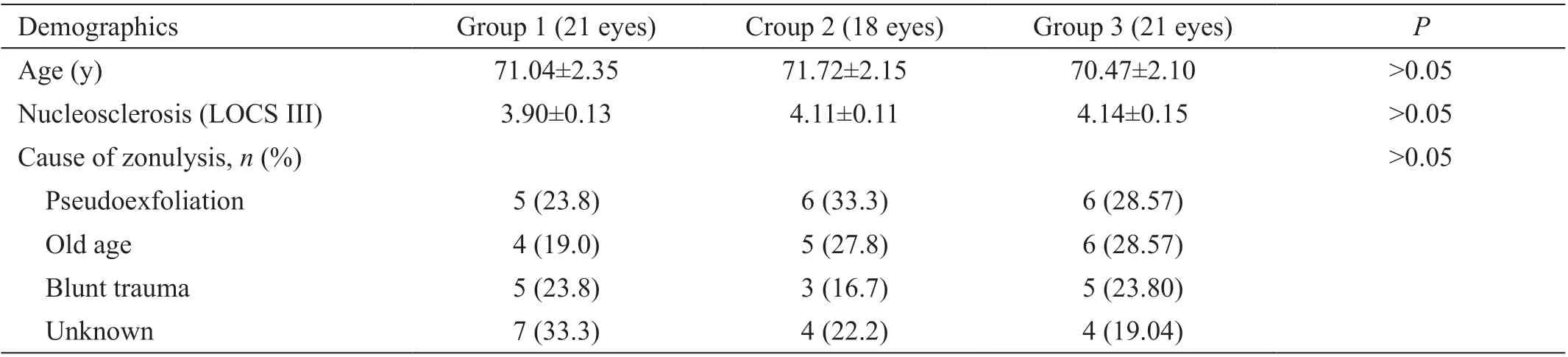
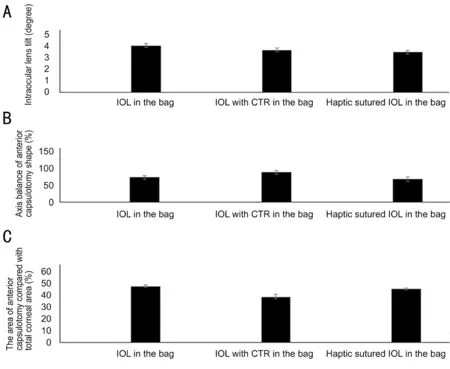
Table 1 shows the preoperative demographics of three groups.At postoperative 1mo, there was no difference between groups in comparison of IOL tilt, axis balance of anterior capsulotomy area and the percentage area of anterior capsulotomy compared with total corneal area (Figure 5).
Exclusion criteria were congenital zonular laxity (
, Marfan syndrome), previous ocular surgery, intraoperative posterior capsule rupture, greater than 2.00 D of corneal cylinder by keratometry, abnormal corneal topographic patterns, and extreme axial length (less than 21.0 mm or longer than 25.0 mm).
For ACD changes between 1mo and 1y, Group 1 (0.40±0.05 mm) showed a significant ACD increase compared to Group 3 (-0.04±0.01 mm,
=0.005). There was no significant difference in ACD change between Group 2 (-0.07±0.01 mm)and Group 3 (Figure 6B).
As for IOL tilt, Group 2 (2.66°±0.11°) showed significantly less IOL tilting than Group 1 (6.35°±0.28°,
=0.005) and Group 3 (3.47°±0.11°,
=0.006). Group 3 showed significantly less tilt than the Group 1 (
=0.007; Figure 6C).
Comparing of shapes of CCC, Group 2 (93.13%±1.00%)showed the largest axis balance (the least disparity), and Group 3 (64.13%±0.55%) showed the largest disparity between X and Y axis (Figure 6D). For change in area due to CCC contraction,Group 1 (21.62%±1.06%) showed significant CCC contraction compared to the Group 2 (1.00%±0.52%,
=0.005) and Group 3 (6.32%±1.36%,
=0.007). Group 2 showed less CCC contraction than Group 3 (
=0.010; Figure 6E).
Comparing of PCO, there was no eye with PCO Grade 3 or above. There was no difference of PCO incidence between groups (Table 2).
As a result, Group 3 showed the superior anatomical (CCC area, IOL tilt) and refractive stability (ACD, refraction) to Group 1 and showed superior anatomical stability (CCC area,CCC shape, and IOL tilt) to Group 2.
DISCUSSION
Given the rising prevalence of pseudophakia due to increased life expectancy and earlier surgical intervention for cataracts,the incidence of late in-the-bag IOL dislocation may increase over time
. Surgeons need to consider preoperative risk factors and various surgical techniques to prevent this dangerous complication.
大部分国家和地区的教师开展教学活动时,比较依赖教材的探究活动。这就对教材中探究活动的实用性提出了较高要求。情境的创设是十分重要的,建议多创设学生感兴趣的真实情境,甚至有关地理原理和过程的学习也可以结合真实情境展示。
Cataract surgery in the presence of zonulysis can make the surgery difficult, and it is not uncommon for surgeons to miss zonulysis less than 4 clock hours preoperatively due topoorly dilated pupil or a subtle phacodonesis. In eyes with microscopically visible zonulysis found during surgery,surgeons must determine the appropriate location and IOL insertion methods according to the extent of zonulysis.
CTRs can serve to support the capsular bag during surgery and provide long-term IOL stabilization
. The centrifugal force that CTR creates at capsule equator can maintain tension and the circular contour of the capsular bag
. However,CTRs carry a risk for iatrogenic damage to capsular bag with insertion
.
Typically, CTRs are utilized in cases of mild, diffuse zonular weakness or small, localized zonular dialysis (
, less than 4 clock hours). When the degree of zonular dehiscence is 120°or greater, however, the stability of IOL-capsule-CTR complex cannot be guaranteed
.
SPO主要用于矢状面脊柱畸形的矫形[6],冠状位亦适用[7],由于截骨不多,SPO适用于畸形程度轻的患者。据报道,SPO治疗侧凸角度< 70°,柔韧性> 40%的脊柱畸形都能获得满意效果[8]。对于矢状位偏移(SVA)6 ~ 8 cm的患者,推荐应用SPO[9]。SPO技术风险较小,操作相对简单[10],对于不能熟练开展三柱截骨手术的年轻脊柱外科医师是第一选择。
For large areas of zonulysis, surgeons generally cannot insert IOLs without special devices with sutured fixation, such as modified CTRs or capsular tension segments. In situations where special devices are lacking, insertion of IOL into the sulcus with scleral fixation is the traditional approach to zonulysis confronted during cataract surgery.
With respect to refractive stability, Group 1 (IOL in the bag)showed significant hyperopic changes compared to Group 2 (IOL with CTR in the bag) (
<0.01) and Group 3 (haptic sutured IOL in the bag) (
<0.01). This finding signifies greater ACD deepening from capsular contracture and subsequent posterior movement of the IOL in Group 1. In our study,Group 2 showed superior stability in all parameters (refraction,anterior chamber depth, CCC contracture, and IOL tilt) than Group 1.
The CCC area was measured using Image J software as the percentage area of the CCC in reference to the total corneal area. The total corneal area was defined as the area contained by the corneal limbus (Figure 4A). CCC contraction was then calculated by subtracting the percentage areas obtained at the two postoperative visits at 1mo and 1y.
In contrast to our results, one study on co-implantation of CTR showed hyperopic change in eyes with CTR compared with eyes without CTR
. Belov
compared refractive outcomes in myopic eyes between IOL implantation with and without a CTR, and found no statistically significant difference in the mean absolute refractive prediction error between the CTR group and controls. These results may be due to differences in the total follow up period and inclusion criteria of each study as our study included eyes with zonulysis of less than 120°. The capsular contraction syndrome itself can cause postoperative hyperopic change, due to posterior bowing of IOL-capsule complex
.
But we assume that the difference in refractive changes in each study depends on the degree of zonular weakness with accompanying progressive changes with time. Moreover, CTR cannot entirely prevent capsule contraction
.
When considering IOL tilt, Group 2 showed less tilt than Group 1. These results concur with a study by Lee
,who evaluated the impact of the CTR on postoperative IOL position using Scheimpflug imaging and found that eyes with both an IOL and a CTR had significantly lower anatomic IOL decentration and physical tilt than eyes with IOLs alone.
However, the opposite was reported. Page
found the use of CTRs caused an increase in tilt aberration after cataract surgery and does not seem to improve the optical performance of conventional IOL after uneventful cataract surgery. In a study of Takimoto
, there was no reported difference in IOL tilt between the CTR group and control at 6mo postoperatively. The observation period of these two studies were different from ours, so further long-term study may provide a better understanding of postoperative IOL tilt.
通过CT或者MRI对110例患者进行了排查,确定都为脑梗塞患者,其派出的标准为认知功能缺陷患者、生活无法自理者以及心肝肾等功能障碍患者[1]。
Group 3 showed comparable ACD and refractive stability to Group 2. This is notable because an effective sutured haptic technique may offer additional advantages over CTR-based methods as this novel technique can be done without special devices, such as the modified CTR. Sutured haptic IOLs would also resist late IOL-capsular bag dislocation that pose a risk to standard CTR co-implantation.
Considering the significant complication such as extension of a zonular dialysis, violation of the capsular bag, displacement of the CTR into the vitreous, misplacement into the sulcus,or the anterior chamber which might occur during CTR implanatation, this novel technique can be an alternative choice for eyes with zonular insufficiency
.
目前如何定义慢加急性肝衰竭(ACLF)在国际上存在很大分歧,影响国际间的交流。分歧的核心主要有两大方面,一是肝脏基础疾病究竟应该包括哪些;二是急性打击是否必须有肝脏功能的衰竭,且衰竭的界定标准是什么 [1-2]。世界胃肠病组织(WGO)提出的ACLF概念试图融合东西方的差异,将不同肝脏基础疾病全部纳入,同时提出分类管理,即A型ACLF-非肝硬化型 (A型);B型ACLF-肝硬化代偿型 (B型);C型 ACLF-肝硬化失代偿型(C型)[3]。我国最常见的是HBV-ACLF[4-5],本文将探讨此分类在我国患者中的应用价值。
When using CTR, if the zonulopathy is a non-progressive zonulopathy, such as traumatic or iatrogenic zonular dialysis,these cases are well suited for standard CTR, as the remaining zonules are typically of normal tension. In cases of progressive or advanced zonulopathy, such as advanced pseudoexfoliation syndrome, a standard CTR is unlikely to provide the capsular support needed, and will most likely allow the IOL to dislocate postoperatively
. The modified Cionni CTR can prevent the late IOL-capsular bag dislocation, but this Cionni CTR needs scleral fixation, too. So with suture related problems and iris chafing exist with using the Cionni rings
. This novel,haptic sutured in the bag IOL technique can be used safely in progressive zonulopathy.
In all postoperative values (ACD, refraction, CCC area, IOL tilt) except CCC shape, Group 3 showed significantly superior stability than Group 1. When analyzing Group 3’s CCC shape(axis balance), we found the suture point of optic-haptic junction has the potential to elongate the long axis (Y axis),creating a CCC shape that may be more ovoid than those of the other groups.
A well-known technique for IOL insertion in the setting of zonular dehiscence is orienting IOL haptics toward the area of zonulysis. The IOL haptics will extend the capsule in the direction of zonulysis and help maintain the CCC shape. In our study Group 1 was shown to maintain a more circular shape than Group 3. However, using an IOL alone appeared to poorly resist CCC contraction as the CCC contraction was highest in this group.
控制措施:①正确选用焊接材料。②按照工艺要求,焊前预热,冬季施工时采取保温措施,必要时进行焊后加热缓冷。③严格控制组对应力,避免强力组对。④避免其他焊接缺陷的产生,如:未焊透、长条状夹渣、咬边等。⑤选择经验丰富、技术高、责任心强的焊工进行根焊作业。根部焊道焊接时,由2名或3名焊工从两侧对称焊接,一旦出现缺陷,不允许进行返修,须切掉重焊。⑥焊接过程中可在上爬坡最容易焊接操作的位置留一段(100~200mm)不焊,便于焊接过程中观察焊道内部的焊缝成形情况,发现有质量问题可及时解决,同时有利于焊道在焊接过程中的应力释放,以减小焊道根部裂纹的产生,待其他地方根焊道全部完成后再把预留处焊完(见图6)。
This novel technique we introduce here involves a modification to the IOL fixation location. Historically, scleral suture fixation
of IOLs is accomplished by suturing IOL haptics at one-third from each end (or through premade holes in the haptics) followed by insertion into the sulcus with or without optic capture. In this novel technique, we modified the location of sutures in the IOL haptic to be nearer to the optic-haptic junction to facilitate insertion of the IOL easily into the bag
.Additionally, the CCC was made larger than the usual optic size of a commercial three-piece IOL (typically 6.0 mm or less), so the fixation knot point on the haptic will be minimally affected by the capsulorhexis margin.
Because we included only cases of less than 4 clock hours of zonulysis, we did not perform or include cases of traditional scleral sulcus fixation, which is more appropriate for case of larger zonulysis. This study was further limited by its retrospective nature and lack of randomization in choice of IOL insertion methods.
Although the traditional scleral sulcus fixation technique with or without optic capture was not included, we believe this novel technique of in-the-bag haptic sutured IOL will prove to be superior in several regards (a manuscript in preparation).
Our approach preserves anatomical stability of the IOLcapsular bag complex with both optic and haptics in the bag.Retaining the haptics in the bag can stretch the capsular bag(especially toward the direction of zonulysis) according to the total length of the planned IOL. In traditional sulcus scleral fixation methods, total capsular phimosis or bag shrinkage or bag distortion can be caused by an absence of the IOL haptics in the bag
. This technique can also prevent total capsular phimosis or bag shrinkage due to an absence of the IOL haptics as seen in traditional scleral sulcus fixation.
3b 1H NMR(CDCl3) δ:8.23-8.21(m,2 H),7.75-7.71(m,1 H),7.58-7.55(m,1 H),7.36-7.27(m,2 H),7.08-7.03(m,2 H),3.87(s,3 H).
In conclusion, the in-the-bag haptic sutured IOL technique can improve the IOL-capsular bag complex stability without additional devices. This easy and simple technique we introduce here has the potential to play an effective role in preventing late IOL decentration in eyes at risk, such as those with partial zonulysis or phacodonesis.
证明 类似地,独占暂存性离散资源分配的最优方法应该满足极大相容公理组ESCA4,即要求分配方法满足{Ax.4,Ax.5,Ax.6,Ax.7}.
None;
None;
None.
1 Weber CH, Cionni RJ. All about capsular tension rings.
2015;26(1):10-15.
2 Shahid SM, Flores-Sánchez BC, Chan EW, Anguita R, Ahmed SN,Wickham L, Charteris DG. Scleral-fixated intraocular lens implantsevolution of surgical techniques and future developments.
(
)2021;35(11):2930-2961.
3 Guo L, Wang C, Yang X. A novel technique for the surgical management of intraocular lens-capsular bag-capsular tension ring complex dislocation.
2019;17(4):2785-2788.
4 Lee GI, Lim DH, Chi SA, Kim SW, Han J, Shin DW, Chung TY.Incidence and characteristics of intraocular lens dislocation after phacoemulsification: an eight-year, nationwide, population-based study.
2021;10(17):3830.
5 Hayashi K, Hirata A, Hayashi H. Possible predisposing factors for In-the-bag and out-of-the-bag intraocular lens dislocation and outcomes of intraocular lens exchange surgery.
2007;114(5):969-975.
6 Blecher MH, Kirk MR. Surgical strategies for the management of zonular compromise.
2008;19(1):31-35.
7 Hasanee K, Ahmed II. Capsular tension rings: update on endocapsular support devices.
2006;19(4):507-519.
8 Miyoshi T, Fujie S, Yoshida H, Iwamoto H, Tsukamoto H, Oshika T. Effects of capsular tension ring on surgical outcomes of premium intraocular lens in patients with suspected zonular weakness.
2020;15(2):e0228999.
9 Chee SP, Ti SE, Chan NS. Management of the subluxated crystalline lens: a review.
2021;49(9):1091-1101.
10 Por YM, Lavin MJ. Techniques of intraocular lens suspension in the absence of capsular/zonular support.
2005;50(5):429-462.
11 Dalby M, Kristianslund O, Drolsum L. Long-term outcomes after surgery for late In-the-bag intraocular lens dislocation: a randomized clinical trial.
2019;207:184-194.
12 Subasi S, Yuksel N, Karabas VL, Yilmaz Tugan B. Late in-the-bag spontaneous IOL dislocation: risk factors and surgical outcomes.
2019;12(6):954-960.
13 Tekin K, Inanc M, Elgin U. Monitoring and management of the patient with pseudoexfoliation syndrome: current perspectives.
2019;13:453-464.
14 Haripriya A, Ramulu PY, Schehlein EM, Shekhar M, Chandrashekharan S, Narendran K, Venkatesh R, Sithiq M, Ramakrishnan R, Ravindran RD, Robin AL. The aravind pseudoexfoliation study: 5-year postoperative results. The effect of intraocular lens choice and capsular tension rings.
2020;219:253-260.
15 Congdon N, Fan H, Choi K, Huang W, Zhang L, Zhang S, Liu K, Hu IC, Zheng Z, Lam DSC. Impact of posterior subcapsular opacification on vision and visual function among subjects undergoing cataract surgery in rural China: study of Cataract Outcomes and Up-Take of Services (SCOUTS) in the Caring is Hip Project, Report 5.
2008;92(5):598-603.
16 Kristianslund O, Råen M, Østern AE, Drolsum L. Late in-the-bag intraocular lens dislocation: a randomized clinical trial comparing lens repositioning and lens exchange.
2017;124(2):151-159.
17 Page TP Sr, Werner L, Ellis N, Heczko JB. ‘S’ means stop! Critical examination of capsular tension ring movements with Miyake-Apple video analysis.
2021;47(3):379-384.
18 Park HJ, Lee H, Kim do W, Kim EK, Seo KY, Kim TI. Effect of coimplantation of a capsular tension ring on clinical outcomes after cataract surgery with monofocal intraocular lens implantation.
2016;57(5):1236-1242.
19 Belov D, Nikolaenko V, Potemkin V. Effect of capsular tension ring implantation during phacoemulsification on postoperative refraction.
2021:11206721211051920.
20 Kim TG, Moon SW. Hyperopic shift caused by capsule contraction syndrome after microincision foldable intraocular lens implantation:case series.
2019;19(1):116.
21 Yang S, Jiang H, Nie K, Feng L, Fan W. Effect of capsular tension ring implantation on capsular stability after phacoemulsification in patients with weak zonules: a randomized controlled trial. CTR implantation in cataract patients with weak zonules.
2021;21(1):19.
22 Bochmann F, Stürmer J. Chronic and intermittent angle closure caused by in-the-bag capsular tension ring and intraocular lens dislocation in patients with pseudoexfoliation syndrome.
2017;26(11):1051-1055.
23 Takimoto M, Hayashi K, Hayashi H. Effect of a capsular tension ring on prevention of intraocular lens decentration and tilt and on anterior capsule contraction after cataract surgery.
2008;52(5):363-367.
24 Xie T, Liu X, Zhu J, Li X. Effect of capsular tension ring on optical and multifunctional lens position outcomes: a systematic review and a meta-analysis.
2021;41(12):3971-3984.
25 Rohart C, Gatinel D. Influence of a capsular tension ring on ocular aberrations after cataract surgery: a comparative study.
2009;25(1 Suppl):S116-S121.
26 Page Sr TP, Werner L, Ellis N, Heczko JB. Capsular tension ring explant complication rate comparison using Miyake-Apple video analysis.
2021;47(6):786-791.
27 Vounotrypidis E, Schuster I, Mackert MJ, Kook D, Priglinger S, Wolf A.Secondary intraocular lens implantation: a large retrospective analysis.
2019;257(1):125-134.
28 Cho YK, Brown GT, Ambati BK. Location of intraocular lens sutures at optic-haptic junction in scleral fixation technique.
2020;46(11):1578.
29 Kemer Atik B, Altan C, Agca A, Kirmaci A, Yildirim Y, Genc S,Taskapili M. The effect of intraocular lens tilt on visual outcomes in scleral-fixated intraocular lens implantation.
2020;40(3):717-724.
30 Hayashi K, Hirata A, Hayashi H. In-the-bag scleral suturing of intraocular lens in eyes with severe zonular dehiscence.
2012;26(1):88-95.
31 Marianelli BF, Mendes TS, de Almeida Manzano RP, Garcia PN,Teixeira IC. Observational study of intraocular lens tilt in sutureless intrascleral fixation versus standard transscleral suture fixation determined by ultrasound biomicroscopy.
2019;5:33.
猜你喜欢
福建中学数学(2023年5期)2024-01-25 17:41:36
中学生数理化·中考版(2022年10期)2022-11-10 09:37:46
肝博士(2020年4期)2020-09-24 09:21:36
当代音乐(2018年4期)2018-05-14 06:47:13
解放军健康(2017年5期)2017-08-01 06:27:34
琴童(2017年7期)2017-07-31 18:33:48
小学科学(2017年5期)2017-05-26 18:25:53
护士进修杂志(2017年3期)2017-02-14 07:19:35
小学生作文(中高年级适用)(2016年3期)2016-11-11 06:30:23
中国卫生标准管理(2015年4期)2016-01-14 05:16:45
 International Journal of Ophthalmology2022年9期
International Journal of Ophthalmology2022年9期
- International Journal of Ophthalmology的其它文章
- What can we learn from negative results in clinical trials for proliferative vitreoretinopathy?
- Suggestions on gut-eye cross-talk: about the chalazion
- A novel mutation of RPGR in a Chinese family with X-linked retinitis pigmentosa
- Novel technique of penetrating keratoplasty in high-risk grafts with significant corneal neovascularization
- COVlD-19 infection with keratitis as the first clinical manifestation
- Corneal histomorphology and electron microscopic observation of R124L mutated corneal dystrophy in a relapsed pedigree