
Pramipexole,a dopamine D3/D2 receptor-preferring agonist,attenuates reserpine-induced fibromyalgia-like model in mice
2022-08-08 02:11:36CarlosPereiraMartinsRodrigoSebbenPaesGabrielaMantovaniBaldassoEduardaGomesFerrariniRahisaScusselRubyaPereiraZaccaronRicardoAndrezMachadodevilaPauloCesarLockSilveiraRafaelCyprianoDutra
中国神经再生研究(英文版) 2022年2期
Carlos Pereira Martins,Rodrigo Sebben PaesGabriela Mantovani BaldassoEduarda Gomes Ferrarini,Rahisa Scussel,Rubya Pereira Zaccaron,Ricardo Andrez Machado-de-Ávila,Paulo Cesar Lock Silveira,Rafael Cypriano Dutra,
Abstract Fibromyalgia (FM) is a complex pathology described as persistent hyperalgesia including somatic and mood dysfunctions,depression and anxiety. Although the etiology of FM is still unknown,a significant decrease in biogenic amines is a common characteristic in its pathogenesis. Here,our main objective was to investigate the role of dopamine D3/D2 receptor during the reserpine-induced pain in mice. Our results showed that pramipexole (PPX) - a dopaminergic D3/D2 receptor agonist - inhibited mechanical allodynia and thermal sensitivity induced by reserpine. Relevantly,PPX treatment decreased immobility time and increased the number of grooming in the forced swimming test and splash test,respectively. Animals that received PPX remained longer in the open arms than the reserpine group using elevated plusmaze apparatus. The repeated PPX administration,given daily for 4 days,significantly blocked the mechanical and thermal allodynia during FM model,similarly to pregabalin,although it failed to affect the reserpine-induced thermal nociception. Reserpine administration induced significant downregulation of dopamine concentration in the central nervous system,and repeated treatment with PPX restored dopamine levels in the frontal cortex and spinal cord tissues. Moreover,PPX treatment inhibited oxidants production such as DCFH (2′,7′-dichlorodihydrofluorescein) and nitrite,also decreased oxidative damage (carbonyl),and upregulated the activity of superoxide dismutase in the spinal cord. Together,our findings demonstrated the ability of dopamine D3/D2 receptor-preferring agonist in reducing pain and mood dysfunction allied to FM in mice. All experimental protocols were approved by the Universidade Federal de Santa Catarina (UFSC) Ethics Committee (approval No. 2572210218) on May 10,2018.
Key Words: dopamine; dopaminergic system; fibromyalgia; hyperalgesia; pain; pramipexole; reserpine
Introduction
Recent evidence illustrates fibromyalgia (FM) as musculoskeletal pain syndrome associated with comorbidities such as chronic fatigue,sleep,and mood disorders,joint pain,and irritable bowel syndrome (Maletic and Raison,2009; Sluka and Clauw,2016; Nagakura et al.,2018; Fischer et al.,2020). Approximately 2-4% of the world population is affected by FM,with a slight predominance in women. To date,both etiology and pathways involved in the maintenance of FM are not fully understood. However,clinical evidence indicates that the “fibromyalgic” phenotype is a consequence of the environmental (such as chronic stress) and genetic factors,including downregulation of biogenic monoamines such as catecholamines,which are responsible for nociceptive modulation (Staud and Rodriguez,2006; Nagakura et al.,2009; Sluka and Clauw,2016). Concomitantly,there is an increase in glutamate,an excitatory neurotransmitter,and in inflammatory mediators,such as interleukin (IL)-8,IL-6,and IL-1β in patients (Nagakura et al.,2009; Sluka and Clauw,2016). Additionally,during the development of FM,decreases in the activation of the descending inhibitory pathway of pain are found in the anterior rostral cingulate cortex,periaqueductal gray substance,rostral ventromedial medulla,and thalamus (Jensen et al.,2012a,b; Harper et al.,2018; Ji et al.,2018; Lesnak and Sluka,2019). Previous data showed that serotonin (5-HT) and noradrenaline (NA) reuptake inhibitors effectively treat symptoms associated with FM,probably due to their ability to decrease functional connectivity in the periaqueductal gray substance and anterior rostral cingulate cortex. Still,neuronal activities related to these areas have been associated with chronic pain and depression during FM progression (Serafini et al.,2020). Flodin and collaborators also report moderate evidence of response in pain-related regions,including the cerebellum,insula,and anterior cingulate cortex in patients diagnosed with FM,compared to an individual’s healthy (Flodin et al.,2014). Besides altering neurotransmitters,Shibrya and colleagues reported antioxidant dysfunctions in patients with FM,with higher levels of reactive oxygen species (ROS) in mononuclear cells from FM patients,and reduction of glutathione reductase (GSH) activity (Shibrya et al.,2017).
The mesolimbic dopaminergic system (ML-DA) plays a fundamental role in executive,affective,motivational function and,lately,in cognitive and sensorial processes. Furthermore,dopamine-containing neurons clustered within major mesencephalic groups,including ventral tegmental area,retrorubral field,and substantia nigra (SN),supramammillary region of the hypothalamus,periaqueductal gray,and the dorsal raphe,besides amygdala,prefrontal cortex,and nucleus accumbens (Alcaro et al.,2007; Serafini et al.,2020). Dopamine can bind to five closely related G protein-coupled receptors. However,functionally distinct,which are divided into two main groups: i) D1 family,which includes D1R and D5R,coupled to stimulatory G proteins (Gs),while,ii) the second is composed of D2R,D3R,and D4R receptors,which are associated with Gαi/o protein - called D2-type receptors (Li et al.,2019). Emerging evidence evaluated the role of the mesolimbic system in the perception and modulation of chronic pain,and patients with FM showed reduced activity of the ventral tegmental area during anticipation of pain as well as reduced binding of the dopaminergic D3/D2 receptor (Mitsi and Zachariou,2016; Serafini et al.,2020). Martikainen and colleagues described that striatal D2 receptor and D3 (ventral striatum) receptors play essential roles in dopaminergic modulation in brain pain control (Martikainen et al.,2018). Interestingly,activation of type-D1 receptors contributes to pain maintenance and persistence,whereas type-D2 receptors,when activated,promoted analgesia (Liu et al.,2019; Puopolo,2019). Pramipexole (PPX),a dopaminergic D3/D2 receptor agonist,is clinically used to treat motor symptoms of neurodegenerative diseases,like as Parkinson’s disease and Willis-Ekbom disorder. Moreover,preclinical and clinical evidence showed that PPX could demonstrate the antidepressant-like effect during depression model,in patients who do not respond to classic antidepressants drugs,respectively (Lieberknecht et al.,2017a; Wang et al.,2018),and the neuroprotective effect of PPX could be associated with brain-derived neurotrophic factor induction (Lieberknecht et al.,2017a). Otherwise,PPX modulated immune cell responses in experimental autoimmune encephalomyelitis-induced,abolishing the motor symptoms,like as multiple sclerosis disease,and other immuno-mediated inflammatory disorders (Lieberknecht et al.,2017b). Extending this idea,Malikowska-Racia and colleagues showed that PPX abolished posttraumatic stress disorder during chronic stress model in mice (Malikowska-Racia et al.,2019). Additionally,a previous randomized,double-blind trial showed that PPX treatment mitigated motor and sensory symptoms,and its showed safety and well-tolerated,in FM patients after 14 weeks. However,additional investigation is necessary to determine its action mechanism during FM condition (Holman and Myers,2005).
According to the discussion above,it was hypothesized that PPX could produce antinociceptive effects through interaction with dopaminergic D3/D2 receptor. The present study was designed to evaluate the antihyperalgesic,anxiolytic,and antidepressant-like properties of PPX in the reserpine-induced FM-like model,and investigate the mechanisms underlying the effects of dopaminergic D3/D2 receptor agonist.
Materials and Methods
Animals
The experiments were carried out in 222 female Swiss mice (body weight 30-50 g,45-120 days of age) from Universidade Federal de Santa Catarina. Mice were housed under a 12-hour light/dark cycle (artificial light on at 7:00 a.m.) and temperature (22 ± 2°C) with food and waterad libitum. The animals were used only once throughout the experiments. All protocols used in this project followed the ARRIVE (Animal Research: ReportingIn VivoExperiments),“Principles of laboratory animal care” guidelines (NIH publication no. 85-23) (McGrath and Lilley,2015; Percie du Sert et al.,2020a,b),and the Universidade Federal de Santa Catarina (UFSC) Ethics Committee (Committee on Ethics in the Use of Animals (CEUA)/UFSC - approval No. 2572210218 - approved on 10 May 2018) - based on the principles of the 3Rs (replace,reduce,and refine). Behavioral evaluations were performed by a blind operator between 8:00 a.m. and 5:00 p.m,and mice were adapted to the laboratory for at least 60 minutes before evaluation. All efforts were made to reduce animal suffering during noxious stimuli. Animals were randomly assigned to groups before treatments,and behavioral evaluations were measured manually,and the observer was blinded to the experimental protocols.
Reserpine administration
FM model was induced according to Nagakura and colleagues for rats (Nagakura et al.,2009),posteriorly adapted to mice (de Souza et al.,2013; Klein et al.,2014; Li et al.,2016; Brusco et al.,2019). Reserpine [0.25 mg/kg,subcutaneously (s.c.)] was administrated daily for 3 consecutive days (days 1,2,and 3) to induce the biogenic amines depletion. Reserpine was dissolved in a 0.5% tween 80 solutions in PBS (v/v). Control group (untreated - reserpine group) received reserpine injection plus vehicle (10 mL/kg,s.c.; 0.5% tween 80 in PBS).
Experimental design
To verify the participation of dopaminergic D3/D2 receptors in the progression of the behavioral changes during FM model,mice were therapeutically treated with PPX [0.1,1,and 5 mg/kg,intraperitoneally (i.p.)],once a day,from day 4 to day 14 (therapeutic treatment). Negative control groups received vehicle solution (10 mL/kg,s.c.; 0.5% Tween 80 in PBS) at the same administration schemes (Figure 1A). Next,we accessed the preventive effects of PPX (1 mg/kg,i.p.),which repeated administrations were performed during reserpine administration (days 1,2 and 3) 30 minutes after reserpine injection. On the 4thday,PPX or vehicle (0.5% tween 80 in PBS,s.c.,10 mL/kg) or positive control (pregabalin,30 mg/kg,oral route [p.o.]) were administrated 60 minutes before behavior tests (Figure 1B). The PPX injections were administered between 07:30 and 10:00 a.m. (Breuer et al.,2009; Peres Klein et al.,2016). Behavior tests were performed in all groups before day 0 to obtain the basal tactile and thermal threshold. Afterward,on days 0,3,4,5,6,9,11,13,and 14 post-reserpine-induction,animals were subjected to the following behavioral tests: i) open field test - days 4 and 14,ii) mechanical hypersensitivity - days 0,3,4,9 and 14,iii) thermal stimulus - days 0,3,4,9,and 14,iv) forced swim test - days 6 and 11,v) elevated plus-maze - days 5 and 13,and vi) splash test - days 5 and 13. Weight and observation of clinical signs occurred daily for up to 15 days post-reserpineadministration. Pilot experiments were performed to define the dose of each (results not shown) and from another studies on literature (Klein et al.,2014; Lieberknecht et al.,2017a,b; Brusco et al.,2019). On day 15 of the protocol,mice were euthanized through cervical dislocation to evaluate biochemical assays,as described below. Reserpine was acquired from Sigma-Aldrich Chemical Company (St. Louis,MO,USA); Pramipexole hydrochloride was obtained from Aché Laboratory Pharmaceutics SA (Guarulhos,São Paulo,SP,Brazil); Lyrica® (pregabalin) was purchased from Pfizer (New York,NY,USA). Reserpine was diluted in 0.5% tween 80 (v/v in phosphate-buffered solution; PBS),and pregabalin in saline solution (0.9% NaCl).
Behavioral tests
Mechanical hyperalgesia
For evaluation of mechanical hyperalgesia,we used the von Frey test (0.4 g filament - ventral surface of the right hind paw) (Bortalanza et al.,2002; Goncalves et al.,2021; Navratilova et al.,2020) at different time points (0,3,4,9,and 14 days post-induction) as demonstrated inFigure 1.
Tail-flick test
The test consists of a briefly immersing of the tail in hot water (48 ± 1°C) to measure the thermal threshold’s latency (Trevisan et al.,2009; Dalenogare et al.,2019). The test’s application occurred at different times (0,3,4,9,and 14 days post-induction),as demonstrated inFigure 1. For the animal that did not show nociceptive behavior after 15 seconds,the stimulus was suspended to avoid tissue damage. Baseline latency (10 seconds) was determined before testing,and withdrawal latencies were measured manually.
Forced swimming test
The forced swimming test was used according to the methoddescribed by Lieberknecht and coauthors (Lieberknecht et al.,2017a). Mice were forced to swim in a transparent glass jar (height: 25 cm,diameter: 10.2 cm) filled with water (depth: 19 cm) at 23 ± 2°C. The test was conducted for 6 minutes,with a habituation period of two minutes. Time and number of immobility behavior were measured through observation of the absence of scape-oriented behavior.
Splash test
This test is based on the evaluation of self-cleaning behavior. Briefly,sucrose solution (200 μL of a 10%) was squirted on each mouse’s dorsal coat inducing grooming behavior. The time and numbers of grooming were recorded for 5 minutes as the ratio of self-care and motivational behaviors (Diaz et al.,2016; Vieira et al.,2020).
Elevated plus maze test
The elevated plus maze (EPM) was execute according to the protocol previously described (Bourin,2015; Fraga et al.,2018). The apparatus consisted of two open arms (35 cm × 5 cm),and two closed arms (35 cm × 5 cm × 15 cm) that extended from a central platform (6 cm × 6 cm). The entire maze was elevated to a height of 50 cm above floor. Mice were individually allocated in an open arm facing the center of the maze (Colla et al.,2015),and the number of entries and time spent in both arms were recorded for 5 minutes. The increase in the percentage of entries and time spent in the open arms was considered anxiolytic profiles (Lapmanee et al.,2013). The apparatus was cleaned out after each animal was evaluated with 10% ethanol solution.
Open field test
To investigate the possibility of PPX treatment developing nonspecific muscle-relaxing and sedative effects during FM model,we used open-field apparatus (40 cm × 60 cm × 50 cm). The time spent in ambulation and rearing behavior were counted manually for 5 minutes (Machado et al.,2012; Vieira et al.,2020). The maze was wiped clean after each animal was evaluated with 10% ethanol solution.
Determination of biogenic amine content
Dopamine concentration in the frontal cortex (prelimbic,infralimbic,and anterior cingulate areas) and spinal cord were evaluated according to the protocol previously described (Brusco et al.,2019). The dopamine (DA) content was evaluated after treatment with PPX,pregabalin or vehicle. Frontal cortex and spinal cord tissues were homogenized with perchloric acid 0.2 M,following centrifugation (12,000 ×g,10 minutes,4°C),and posteriorly analyzed by high-performance liquid chromatography (LC-20AT pump coupled to a SIL-20AHT autosampler,RF-20A fluorescence detector,and LC Solution Shimadzu software,Kyoto,Japan) using 320 nm with excitation at 279 nm. Results were expressed as monoamine levels (in ng) by μL of a sample (De Benedetto et al.,2014).
Biochemical assays
Intracellular determination of ROS and nitric oxide
The reactive oxygen and nitrogen species levels were evaluated in the frontal cortex (prelimbic,infralimbic,and anterior cingulate areas) and spinal cord through superoxide production,2′,7′-dichlorofluorescin diacetate (DCFH-DA) oxidation,and nitric oxide (NO) concentration. The DCFH data were expressed as fluorescence intensity (Dong et al.,2010). The final concentration of NO was expressed in μmol nitrite/mg protein (Chae et al.,2004).
Oxidative damage to proteins
Carbonyl content was measured according to the protocol previously described (Levine et al.,1990) using 2,4-dinitrophenyl hydrazine,and expressed as nmol per milligram of protein. Total thiol level was evaluated through 5,5′-dithiobis (2-nitrobenzoic acid) incorporation,the amount of TNB formed (equivalent to the amount of sulfhydryl (SH) groups) was calculated (Aksenov and Markesbery,2001).
Antioxidant activity
Superoxide dismutase (SOD) activity was carried out according to the method previously described (Bannister and Calabrese,1987),and results expresses as SOD units per milligram of protein.
Statistical analysis
The data were expressed as the mean ± SEM. Results were analyzed with GraphPad Prism 8.2.1 software (GraphPad Software Inc.,San Diego,CA,USA). Repeated measurements were considered within-subject random factors. Normality and homoscedasticity were calculated using Shapiro-Wilk’s and Levene’s tests,respectively. Data were calculated using a mixed-model one-way or two-way analysis of variance (ANOVA) followed by Newman-Keuls test or Bonferroni’spost hoctest,respectively. A level ofP< 0.05 was considered as statistically significant. The percentage of inhibition was calculated from the area under the curve (AUC).
Results
Effects of therapeutic treatment with dopaminergic D3/D2 receptor agonist on reserpine-evoked mechanical hyperalgesia
Primarily,to evaluate the therapeutic effect of dopaminergic D3/D2 receptor agonist in nociception of reserpinized animals,the tactile threshold was measure using the Von Frey test. In this study,reserpine administration (0.25 mg/kg,s.c.) induced in a pronounced mechanical hypersensitivity persisting for up to 14 days. The PPX treatment (1 and 5 mg/kg,i.p.) reduced the mechanical hyperalgesia induced by reserpine on the 9thand 14thdays after onset of reserpine administration (Figure 2A) with inhibitions (area under the curve) of 62.5% and 74.5% (one-way ANOVA treatment effect:F(5,18)= 6.859,P< 0.001),respectively (Figure 2B). However,it did not significantly affect the assessment at a dose of 0.1 mg/kg.
Effects of therapeutic treatment with PPX on reserpinerelated thermal nociception
Reserpine administration induced significant decline of the thermal nociceptive threshold compared to the vehicle control group on the 3rd,4th,9th,and 14thdays after injection (Figure 3). Therefore,aiming to investigate whether PPX might revert the thermal nociception induced by reserpine,we performed the tail-flick test. The systemic treatment with PPX significantly reverted thermal nociception induced by reserpine injection at the 9thand 14thdays after FM induction (Figure 3; two-way ANOVA showed interaction [F(20,254)= 3.446,P< 0.001],row [F(4,254)= 42.10,P< 0.001],and column [F(5,254)= 9.795,P< 0.001]),although PPX (0.1 mg/kg) has not shown significant effects in the tail-flick test (Figure 3).
Antidepressant-like and anxiolytic effects of PPX during FM model
Herein,we evaluated whether PPX could block depressive and anxiety behaviors during the FM model. PPX treatment (1 mg/kg,i.p.) significantly inhibited the immobility time (one-way ANOVA treatment effect:F(5,102)= 6.423,P< 0.001) when compared to the reserpine group in the tail suspension test at the 6thand 11thdays after FM induction (Figure 4A). Interestingly,PPX (1 mg/kg,i.p.) markedly increased the grooming number (one-way ANOVA treatment effect:F(5,76)= 2.292,P< 0.05) in the ST on the 5thday after FM induction (Figure 4D),although PPX has not been able to affect the anhedonic-like effect after reserpine administration during ST (Figure 4BandC).Figure 5shows the effect of therapeutical treatment with PPX (0.1,1 and 5 mg/kg) in the EPM. One-way ANOVA demonstrated an important effect of PPX treatment both in number of entries in open arms (F(5,96)= 5.337,P< 0.001;Figure 5A) and in the percentage of time spent in open arms (F(5,96)= 5.191,P< 0.001;Figure 5B). Considering the EPM test,Newman-Keuls’spost hoctest showed that the open arms’ time increased in PPX (1 mg/kg,p.o.) compared to reserpine group (Figure 5B). Also,entries in closed arms did not show percentage differences (Figure 5C). OFT results proved that after reserpine administration,PPX did not induce locomotion pattern in any of the doses used (Figure 5DandE).
Effects of repeated administration with dopaminergic D3/D2 receptor agonist on the reserpine model
The effect of PPX in reserpine-related nociception was investigated as a preventive treatment. Notably,the daily administration of PPX (1 mg/kg) during 4 days markedly inhibited mechanical hyperalgesia induced by reserpine (Figure 6A),with inhibition of 53% (F(3,16)= 49.54,P< 0.001;Figure 6B). Data fromFigure 6also show that pregabalin (30 mg/kg,p.o.) showed a significant difference in analgesia data even as PPX (1 mg/kg,i.p.),with inhibition of 79%. Furthermore,PPX treatment (1 mg/kg,i.p.) did not affect the thermal nociception induced by reserpine (Figure 6C). Significantly,reserpine or PPX treatment did not change the animals’ weight in our experiments (Figure 6D),and these administrations did not induce irritability,salivation or tremors,or change hair appearance (data not shown).
Effect of repeated treatment with PPX in the central neurotransmitter contents after reserpine administration
Aiming to assay the possible mechanisms in which PPX could induce analgesic actions,after we assessed if the levels of biogenic amines could be restored through the preventive treatment with PPX,especially dopamine,in the frontal cortex and spinal cord tissues. Reserpine administration induced downregulation of dopamine in all evaluated structures,including the frontal cortex (Figure 7A) and spinal cord (Figure 7B),compared to vehicle-treated control mice. Interestingly,frontal cortex (one-way ANOVA treatment effect:F(3,18)= 10.17,P< 0.001;Figure 7A) and spinal cord (one-way ANOVA treatment effect:F(3,19)= 7.794,P< 0.001;Figure 7B) exhibited levels of dopamine restored after PPX treatment (1 mg/kg). The loss of dopamine was prevented by pregabalin only in the spinal cord. These results indicate that the PPX ability to restore the dopamine levels in central and spinal structures is directly associated with antinociceptive action after reserpine administration.
Effect of repeated treatment with PPX in the oxidative damage and antioxidant activity after reserpine administration
An increase in ROS production in mononuclear cells and reduce GSH activity could be observed in FM patients (Shibrya et al.,2017). As shown inFigure 8A,the reserpine group showed higher DCF levels than the vehicle group. Relevantly,differently than reserpine group,PPX treatment reduced the DCF levels (one-way ANOVA treatment effect:F(2,14)= 6.843,P< 0.001;Figure 8A). Reserpine administration induced marked increase NO concentration (one-way ANOVA treatment effect:F(2,15)= 5.751,P< 0.01;Figure 8B),which was mitigated by PPX treatment. Moreover,as shown inFigure 8C,the reserpine group increased oxidative marker levels compared to the vehicle group. Interestingly,PPX treatment markedly inhibited carbonyl groups in the central nervous system (CNS) after reserpine induction (one-way ANOVA treatment effect:F(2,15)= 13.29,P< 0.001;Figure 8C),although it failed to restore the decrease of sulfhydryl content in the spinal cord (P> 0.05;Figure 8D). Next,we assessed the effects of PPX on SOD concentration in the CNS after reserpine administration. As shown inFigure 8E,PPX treatment significantly upregulated SOD activity when compared to reserpine control group (one-way ANOVA treatment effect:F(2,15)= 6.493,P< 0.01).

Figure 1|Experimental design.
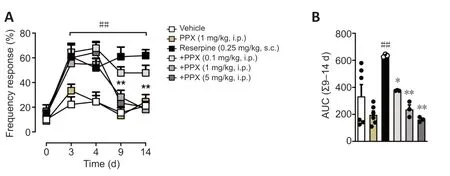
Figure 2|Anti-hyperalgesic effects of PPX during reserpine model.
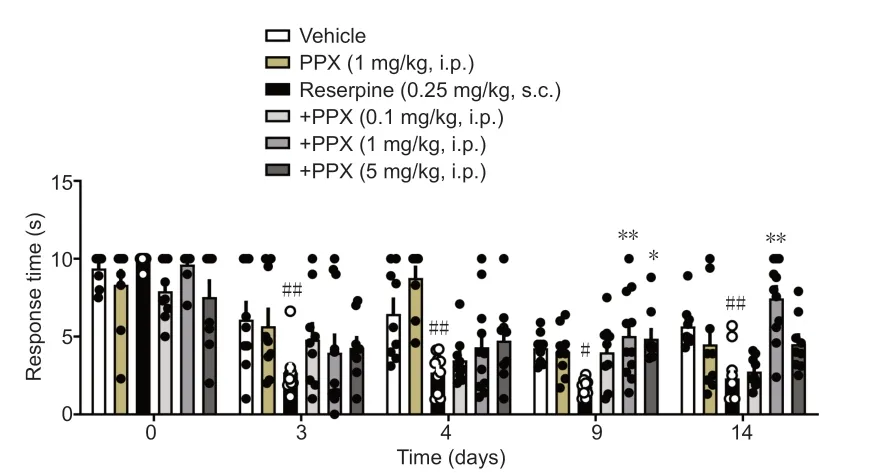
Figure 3|Antinociceptive effects of PPX in reserpinized mice.

Figure 4|Effect of therapeutic PPX treatment (0.1; 1 and 5 mg/kg,intraperitoneally) in the tail suspension test [TST: A] and splash test [ST: latency to grooming (B),grooming time (C) and the number of grooming (C)].
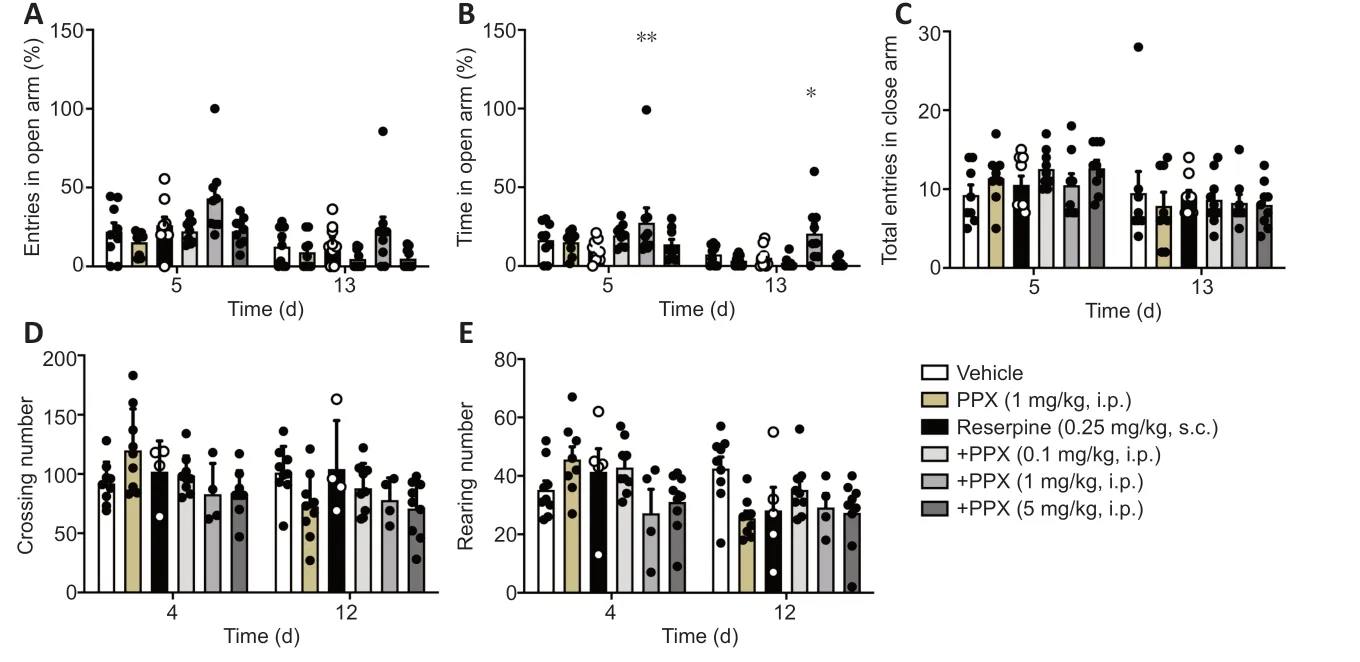
Figure 5|PPX treatment (0.1; 1 and 5 mg/kg,intraperitoneally) in the elevated plus-maze [EPM: open arms entries (A),time spent in open arms % (B) and the number of entries in closed arms (C)],and open field test [OFT: D and E].

Figure 6|Effects of preventive PPX treatment in reserpinized mice.
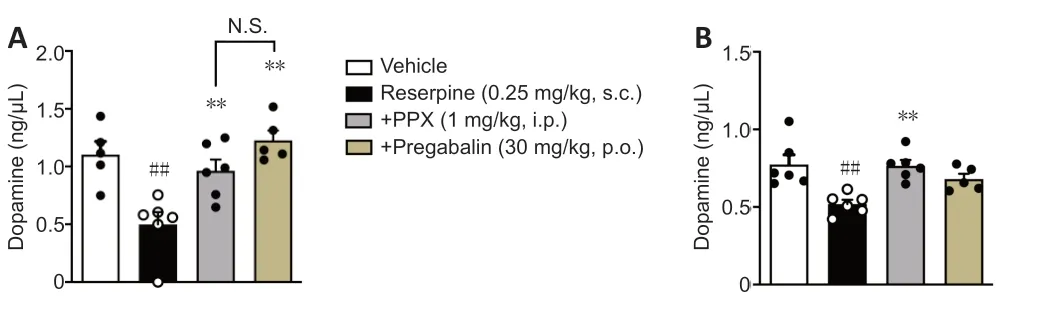
Figure 7| Effect of the PPX in the dopamine level on the frontal cortex (A) and spinal cord (B) after reserpine administration (0.25 mg/kg,subcutaneously).

Figure 8|PPX inhibited oxidative damage and restored antioxidant enzymes after reserpine model. DCFH (A),nitrite (B),carbonyl groups (C),sulfhydryl groups (D) levels,and activity of superoxide dismutase (SOD) (E) were measured on the spinal cord.
Discussion
FM is characterized by non-inflammatory chronic widespread pain associated to persistent fatigue,sleep disturbances,mood disorders,joint pain,and irritable bowel syndrome (Sluka and Clauw,2016; Nagakura et al.,2018; Fischer et al.,2020). Although of their epidemiologic impact,FM’s physiopathology is not fully understood,which represents the importance of the search for new therapeutical strategies. Currently,available therapies for FM treatment are based on symptomatology control,such as prescription of analgesics and 5-HT/NA reuptake inhibitors for pain and mood disorders,but not treating the pathology justifying looking for new immunomodulatory and analgesic therapies. Accumulating evidence has shown that biogenic amines,such as DA,NA,and 5-HT,play a central role in maintaining physiology homeostasis,such as cognition,mood and sleep regulation,memory consolidation,and pain modulation (Staud and Rodriguez,2006; Sluka and Clauw,2016). Evidence suggests that NE and 5-HT are primary neurotransmitters of the descending pain inhibiter system,and curiously,analysis of cerebrospinal fluid of patients diagnoses with FM presents show a decrease in biogenic monoamines (Shibrya et al.,2017). Emerging evidence investigated the function of the mesolimbic dopaminergic system in the modulation of pain and mood disorders (Mitsi and Zachariou,2016; Serafini et al.,2020),whereas dysfunctions in their actions are associated with exacerbating perception of nociceptive information (Russo and Nestler,2013; Mitsi and Zachariou,2016).
Interestingly,patients diagnosed with FM show reduced activity of neurons in the dopaminergic mesolimbic system,such as in the ventral tegmental area,during anticipation of pain and reduced binding of the dopaminergic D3/D2 receptor (Mitsi and Zachariou,2016; Serafini et al.,2020). Furthermore,the ventral tegmental area also is associate with processes involving mood,reward,addiction,reinforcement,and learning (Settell et al.,2017),evidencing the impact of neuronal alterations induced by chronic pain. DA’s role in pain modulation and chronicity is tightly consolidated through several studies (Dennis and Melzack,1983). Furthermore,it has been reported that treatment with dopaminergic agonists inhibited allodynia and hyperalgesia in experimental models (Yao et al.,2020). Recent data show that the activation of D1-type receptors in A11,a crucial area relates to pain modulations (located in the posterior portion of the hypothalamus),is related to the maintenance and chronicity of pain (Li et al.,2019; Liu et al.,2019),whereas the D2-type receptors are related antinociceptive role-play of DA in neuro system (Liu et al.,2019). This study significantly extended these previous findings by demonstrating that PPX - a dopaminergic D3/D2 receptor agonist - attenuates the mice’s FM-like model. The mechanisms underlying the antinociceptive,antidepressant,and anxiolytic effects of PPX was related to: i) its ability to restore dopamine level in the CNS,ii) reduce oxidative damage,and iii) up-regulation of the genomic antioxidant defense. Albrecht and collaborators (2015) highlighted that,in addition to the possible role in nociception,DA is also essential for cognitive function. The authors used positron emission tomography to assess DA pathways’ changes and evaluated the associations between D3/D2 receptors with experimental pain. Therefore,DA can mediate cognitive impairment frequently reported by patients with chronic pain (Albrecht et al.,2016). The study by Arnold et al. confirmed these findings by reporting that,during painful stimuli,changes in activities were observed in the main nociceptive areas (for example,the brainstem - the origin of the descending analgesic pathway),as well as the same authors correlated these regions as dysfunctional pain inhibition in FM (Arnold et al.,2019). As already mentioned,patients with FM demonstrate alterations in endogenous pain inhibitory signals,suggesting an imbalance between the nociceptive and antinociceptive systems (Sarzi-Puttini et al.,2020).
Previous data demonstrated the antidepressant effect of D3/D2 receptors in the experimental model of lipopolysaccharideinduced depression (LPS) (inflammatory model of depression) (Lieberknecht et al.,2017a). Lieberknecht and collaborators identified the neuroprotective and immunomodulatory properties of the dopaminergic D3/D2 agonist (Lieberknecht et al.,2017a). Moreover,the authors described that this dopaminergic agonist might induce an effect similar to the traditional antidepressants used in the clinic (duloxetine/fluoxetine) since treatment with PPX inhibited the typedepressive behavior in the tail suspension test (TSC),as well as the anecdotal behavior in the spray test of sucrose solution (splash test) (Lieberknecht et al.,2017a). Accordingly,it has been reported in the literature that catecolamines reuptake inhibitors are useful for treatment of depression and pain during FM,suggesting that 5-HT depletion could be a plausible explanation responsible for the episodes of depression in the temporal course of the disease (Singh et al.,2019). Therefore,this study’s results regarding the alteration of type-depressive behavior and those related to pain induced by reserpine may be associated with D3/D2 receptors’ modulation. In this study,it was also possible to observe that the dopaminergic D3/D2 agonist inhibited the depressive-like behavior induced by reserpine in the forced swim test and splash test,reinforcing that PPX blocks anecdotal behavior in animals. In humans,anecdotal behavior is closely associated with depression,which is also present in FM. Previous data suggest that chronic pain and depression show similar neuroplasticity changes since monoaminergic neurotransmitters are decreased in individuals with chronic pain and depression (Yao et al.,2020). Likewise,regions of the brain involved in pain signalings,such as the amygdala,hippocampus,prefrontal cortex,and anterior cingulate cortex,also are involved in pain transmission and mood disorders. Emotional disorders,such as anxiety,anhedonia,and cognitive deficits,could be associated with the chronic pain condition (Yao et al.,2020).
Dopaminergic signaling in the same areas involved in pain processing (from the midbrain to the hippocampus,extended amygdala,prefrontal cortex,and anterior cingulate cortex,among other brain regions) has been implicated in anxietylike behavior (DeGroot et al.,2020). Previou reported demonstrated that amygdala,the hippocampus,and the prefrontal cortex,as well as mesolimbic,mesocortical,and nigrostriatal dopaminergic circuitry,are the main brain regions involved with the control of anxiety (Zarrindast and Khakpai,2015). In this context,EPM used to assess anxiogenic behavior in animals,treatment with PPX increased time in the open arm,suggesting that this dopaminergic agonist (D3/D2) controls anxiogenic behavior during the development of FM through dopaminergic circuitry. Although research consistently shows reduced levels of central 5-HT in patients with FM and animal models,emerging evidence suggests that DA could be another crucial factor involved in pain,anxiety,and depression,both associated with FM (Hernandez-Leon et al.,2019).
Previous data have already publicized that during FM have low DA,5-HT,and NA levels (Rus et al.,2018). Therefore,FM symptoms may be the result of impairment of these neurotransmitters,which reflects data described by Sarzi-Puttini et al. (2020). This study described that to maintain the hypoactivity of the descending analgesic pathways during FM,catecolamines neurotransmitters in the biological fluid of patients with FM are downregulated when compared to healthy individuals,and brain dopaminergic activity during painful stimulation decreased (Sarzi-Puttini et al.,2020). Here,biochemical analyzes have significantly demonstrated that reserpine considerably decreased the levels of DA in the spinal cord and frontal cortex of mice,and treatment with PPX restored the levels of DA in the CNS. In this perspective,Bravo et al. showed that the upregulation of NA and 5-HT contributes to control and reduction of persistent pain. Neuropathies are commonly treated with tricyclic antidepressants,selective 5-HT reuptake inhibitors,and gabapentinoids when antidepressants are contraindicated (Bravo et al.,2019). The monoaminergic system is directly associated with chronic pain and demonstrated that depression and anxiety are also correlated with this system,turning this relation a promising pharmacological target in treating sensory and emotional changes evidenced in chronic pain (Bravo et al.,2019). Therefore,our experimental findings reaffirm the neuromodulator,antidepressant,immunomodulator,and antinociceptive effect of dopaminergic agonists,particularly D3/D2 receptors.
Besides altering neurotransmitters and signaling pathways,mitochondrial dysfunction and highest ROS production are commonly evident in patients diagnosed with FM. Further,in these individuals is verify a decrease in coenzyme Q10 (CoQ10),is that the supplementation with CoQ10 reduced the symptoms of FM in patients and experimental model of FM induced by reserpine (Cordero et al.,2012; Alcocer-Gomez et al.,2017; Brum et al.,2020). Additionally,Shibrya and colleagues reported antioxidant dysfunctions in patients diagnosed with FM,including higher ROS levels in mononuclear cells and reduced GSH activity,an essential agent in cellular protection against free radicals. They showed that the low-dose of irradiation (LDI) effectively inhibited the depletion of 5-HT,DA,and NE induced by reserpine injection (Shibrya et al.,2017). Furthermore,Yldirim and Alp (2017) observed a reduction in catalase and peroxidase glutathione,important antioxidants agents,levels in patients diagnosed with FM.
Additionally,current reports indicate that the family of transients receptor potential (TRP) - Ca2+permeable channels - is an essential series of receptors associated whit several physiological functions,including the transmission of painful stimuli (Uslusoy et al.,2017; Yuksel et al.,2017),and that may be related to physiopathology of FM mainly through of the overload Ca2+entry in intramitochondrial space on dorsal root ganglion neurons induced by exacerbating levels of free radicals (Yuksel et al.,2017; Brum et al.,2020). Mainly,transients receptor potential vanilloid 1 and transients receptor potential melastatin 2 can be activated by different stimuli,including ROS and low pH (Yuksel et al.,2017). These receptors are vastly expressed in dorsal root ganglion neurons - an essential pathway for the transduction of nociceptive stimuli from the peripheral - and sciatic nerve. Therefore,Yüksel and collaborates showed that the treatment with selenium (Se) - acts as a cofactor of GSH - decreased the hyperalgesia and ROS levels in rats with FM (Yuksel et al.,2017). Corroborating with these data,Brum and collaborates also identify elevated ROS and mitochondrial dysfunction levels in the FM experimental model induced by reserpine,which was reverted by supplementation whit CoQ10 (Brum et al.,2020). Herein,animals treated with PPX showed a reduction in ROS and NO levels and decreased the damage into lipids of the CNS. Lastly,PPX restored the reduction of SOD activity in the CNS after reserpine induction. Altogether,these results suggest that PPX inhibited oxidative damage in the central tissues associated to inhibition of hyperalgesia and mood behavior induced by reserpine. However,more studies will need to be done to investigate the effect of PPX in distinct signaling pathways related to ROS/RNS damage during the FM-like model in mice.
The limitation of our study was the lack of measure other neurotransmitters involved in central sensitization. Nonetheless,it was not possible to measure the levels of 5-HT and NA in the frontal cortex and spinal cord,justifying further experiments.
In summary,the data presented corroborate with our study results (Lieberknecht et al.,2017a,b) and demonstrated that PPX - a dopaminergic D3/D2 receptor agonist - inhibited pain and mood dysfunction in a fibromyalgia-like model in mice. PPX antinociceptive and antidepressive-like properties were able to restore dopamine levels and antioxidant responses in the CNS after reserpine administration. Altogether,our data suggest that dopaminergic D3/D2 receptor might constitute an innovative and unusual target,and open-up new perspective for developing new analgesic and neuromodulator drugs to treat persistent pain,including fibromyalgia-related symptoms,especially in cases of poor clinical outcomes. Nonetheless,additional reports will need to assess the effect of PPX in wellconducted clinical trials performed in FM patients.
Author contributions:Study design and concept,and manuscript writing: CPM,RSP,RCD; experiment implementation and manuscript drafting: CPM,RSP,GMB,RAMA,PCLS,RCD; figure production: RSP,RCD; data analysis: CPM,RSP,GMB,RS,RPZ,RCD; experiment support: CPM,RSP,GMB,EGF,RS,RPZ,RAMA,PCLS,RCD. All authors read and approved the final manuscript.
Conflicts of interest:The authors declare that they have no conflicts of interest.
Financial support:This project was supported by grants from Programa de Pós-graduação em Neurociências (PGN),Programa INCT-INOVAMED (grant No. 465430/2014-7),Fundação de Apoio à Pesquisa e Inovação do Estado de Santa Catarina (FAPESC),Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES),and Conselho Nacional deDesenvolvimento Científico e Tecnológico (CNPq),all from Brazil. CPM was recipient of a master fellowship from CAPES-Brazil; RSP and GMB were undergraduate students in Physiotherapy receiving grants fromCNPq; EGF and RS were recipient of a PhD fellowship from CAPES-Brazil; RAMA,PCLS and RCD are recipients of a research productivity fellowship from the CNPq.
Institutional review board statement:The study was approved by the Universidade Federal de Santa Catarina (UFSC) Ethics Committee (approval No. 2572210218) on May 10,2018.
Copyright license agreement:The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement:Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check:Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
- 中国神经再生研究(英文版)的其它文章
- A Drosophila perspective on retina functions and dysfunctions
- Celeboxib-mediated neuroprotection in focal cerebral ischemia: an interplay between unfolded protein response and inflammation
- Effects of delayed repair of peripheral nerve injury on the spatial distribution of motor endplates in target muscle
- Neurorehabilitation using a voluntary driven exoskeletal robot improves trunk function in patients with chronic spinal cord injury: a single-arm study
- Gene and protein expression profiles of olfactory ensheathing cells from olfactory bulb versus olfactory mucosa
- Inhibition of microRNA-29b suppresses oxidative stress and reduces apoptosis in ischemic stroke