
International examples of primary care COVID- 19 preparedness and response: a comparison of four countries
2022-07-26 06:02FelicityGoodyearSmithMichaelKiddTijaniIdrisAhmadOseniNagwaNashatRobertMashMehmetAkmanRobertPhillipsChrisvanWeel
Felicity Goodyear- Smith , Michael Kidd, Tijani Idris Ahmad Oseni, Nagwa Nashat, Robert Mash, Mehmet Akman, Robert L Phillips, Chris van Weel
ABSTRACT We report the learnings gleaned from a four- country panel (Australia, South Africa, Egypt and Nigeria) sharing their countries’ COVID- 19 primary healthcare approaches and implementation of policy at the World Organization of Family Doctor’s World virtual conference in November.The countries differ considerably with respect to size,national economies, average age, unemployment rates and proportion of people living rurally. South Africa has fared the worst with respect to waves of COVID- 19 cases and deaths. All countries introduced strategies such as border closure, COVID- 19 testing, physical distancing and face masks. Australia and Nigeria mobilised primary care, but the response was mostly public health and hospital- based in South Africa and Egypt. All countries rapidly adopted telehealth. All countries emphasised the critical importance of an integrated response between primary care and public health to conduct surveillance, diagnose cases through testing, provide community- based care unless hospitalisation is required and vaccinate the population to reduce infection spread.
The World Organization of Family Doctor’s(WONCA) Working Party on Research has a well- established process of running workshops at regional and world conferences,whereby a panel of experts present attributes of primary healthcare in their respective countries. A predeveloped template is used, and the comparative data plus ensuing discussion has formed the basis of a number of peer- reviewed publications.1Profiling and juxtaposing different countries’ primary healthcare approaches and their implementation of policy, as promoted by the WHO and WONCA, can reflect key lessons on how to implement primary healthcare and improve service delivery.
At the 2021 WONCA World virtual conference last November, the workshop focused on the contribution of primary healthcare to managing and preventing COVID- 19 in four selected countries: Australia, South Africa, Egypt and Nigeria. A call was made to members of the WONCA Working Party on Research planning to attend the conference to contribute to the panel, and countries selected for diversity of region and other characteristics. The aim of this paper is to analyse the findings of this interactive meeting and reflect on the lessons learnt from these comparisons.
The four countries vary considerably with respect to their national economies, the size of their populations, the life expectancy of their citizens, their unemployment rates and the proportion of the people who live in urban settings (table 1).
They have also had very different experiences of the COVID- 19 pandemic. South Africa has fared worst, with three severe waves(figure 1).2Egypt has had several smaller waves, while Australia successfully managed a suppression strategy until August this year,when a Delta outbreak became established.While Nigeria reports the lowest case rate,resource constraints on testing means considerable under- reporting and case rates are likely to be much higher than reported.
This pattern is also evident when looking at recorded deaths from COVID- 19 per million(figure 2).
National vaccination rates are shown in figure 3, which dramatically highlights the inequity in vaccination coverage.3In November 2021, high- income country Australia had 71% of its 26 million population fully vaccinated, whereas South Africa was at 23%, and the larger lower middle- income countries Egypt and Nigeria were at 13%and 1.6%, respectively. Vaccines were being provided free in Australia and Egypt to those over 12 years and in South Africa and Nigeria to those over 18 years. Primary healthcare has been involved in vaccination provision in all four countries. In South Africa, vaccination has been provided at pharmacies, clinics andcommunity venues, and in Nigeria, primary care (PC) and public health (PH) work together to conduct vaccination.Reasons for low vaccination rates in Egypt and Nigeria are likely to be complex, but as well as access issues with high rural populations, promulgation of anti- vaccination misinformation and religious beliefs may be contributing factors. Nigeria’s criteria for vaccination were 18 years and older, meaning that only half the population were eligible.
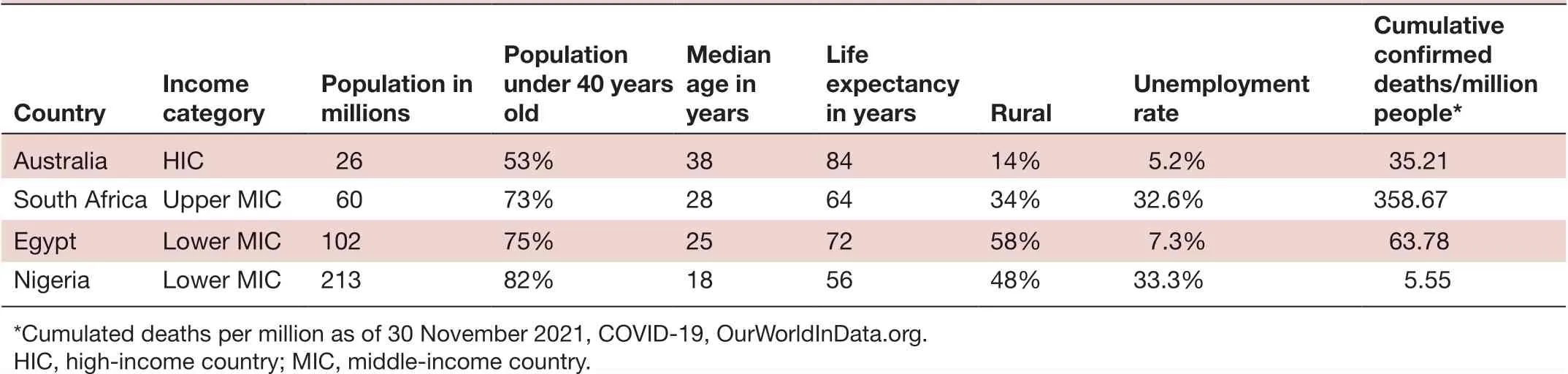
Table 1 Characteristics of the four countries
Australia’s low COVID- 19 infection rates are explicable,given it is a high- income country and managed to suppress outbreaks of infection for many months until vaccines were available. Despite lower vaccination rates, Egypt and Nigeria fare better than South Africa. Given the testing regimes, cases will be under- reported, but we expect this to be true in all three countries. For Nigeria, in particular,some COVID- 19 deaths may be unreported, but there is no corresponding increase in excess deaths to indicate that this is the explanation. Contributing factors may be early border closures and less international connectivity,a higher proportion of people living rurally with more outdoor living and the population being very young.Compared with South Africa, Nigeria has much lower rates of comorbidity with respect to diabetes (10.8% vs 3.6%)4and HIV (19.1% vs 1.3%).5There is also a theory about the possibility of ‘trained immunity’ to SARS- CoV- 2 from prior infections such as Lassa, malaria, tuberculosis and BCG vaccination, although this needs further research.6
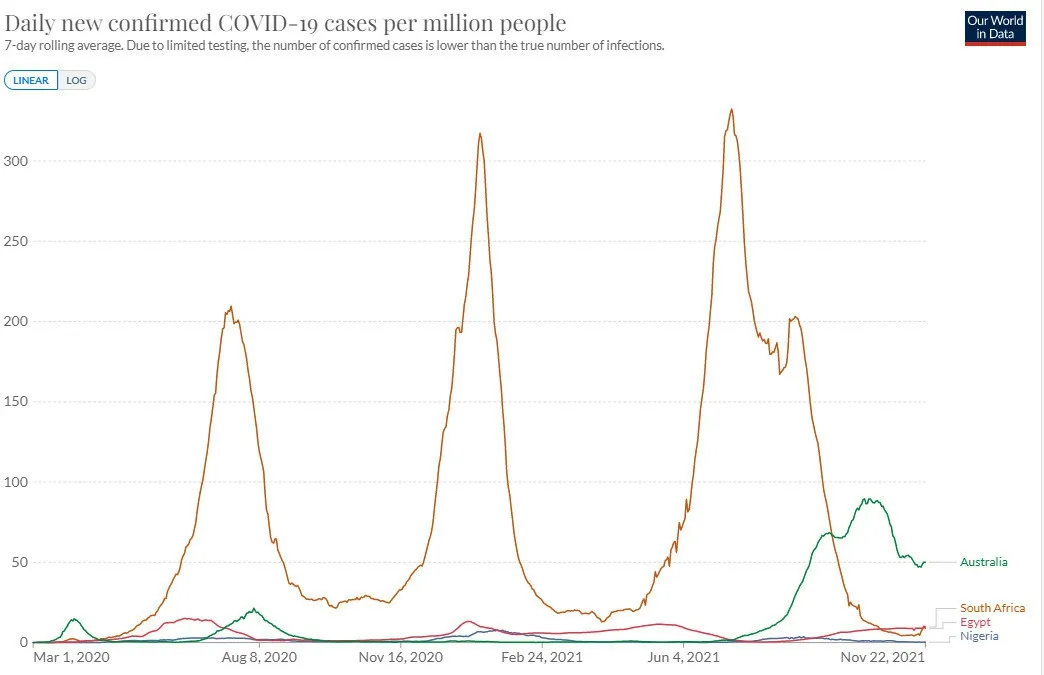
Figure 1 Daily new confirmed COVID- 19 cases per million people (7- day rolling average) as of 22 November 2021. Source:Johns Hopkins University CSSE COVID- 19 Data.
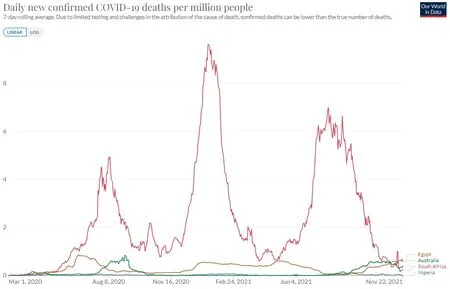
Figure 2 Daily new confirmed COVID- 19 deaths per million people (7- day rolling average) as of 22 November 2021.
Panellists were asked to identify factors or strategies that had reduced or slowed the spread of infection.The responses were remarkably similar. All countries identified early border control as a key at the start of the pandemic. Other factors identified were lockdowns during periods of community transmission as well as COVID- 19 testing. Contract tracing and surveillance were also cited in Australia and Egypt, although in Nigeria and South Africa resource constraints limited testing to high risk, suspected or exposed cases. All countries identified PH measures such as physical distancing, hand washing and face masks. In Australia, important strategies included protection of at- risk patients, the rapid move to telehealth for the whole population and the segregation of COVID- 19- related and usual care with the establishment of general practitioner respiratory clinics. In South Africa, PC facilities created separate streams for those with COVID- 19- related symptoms and those without.7In Nigeria, PC and PH worked together to conduct health education on testing and vaccination. National leadership has been important with regular communications about the actions the government was taking and the reasons for these.
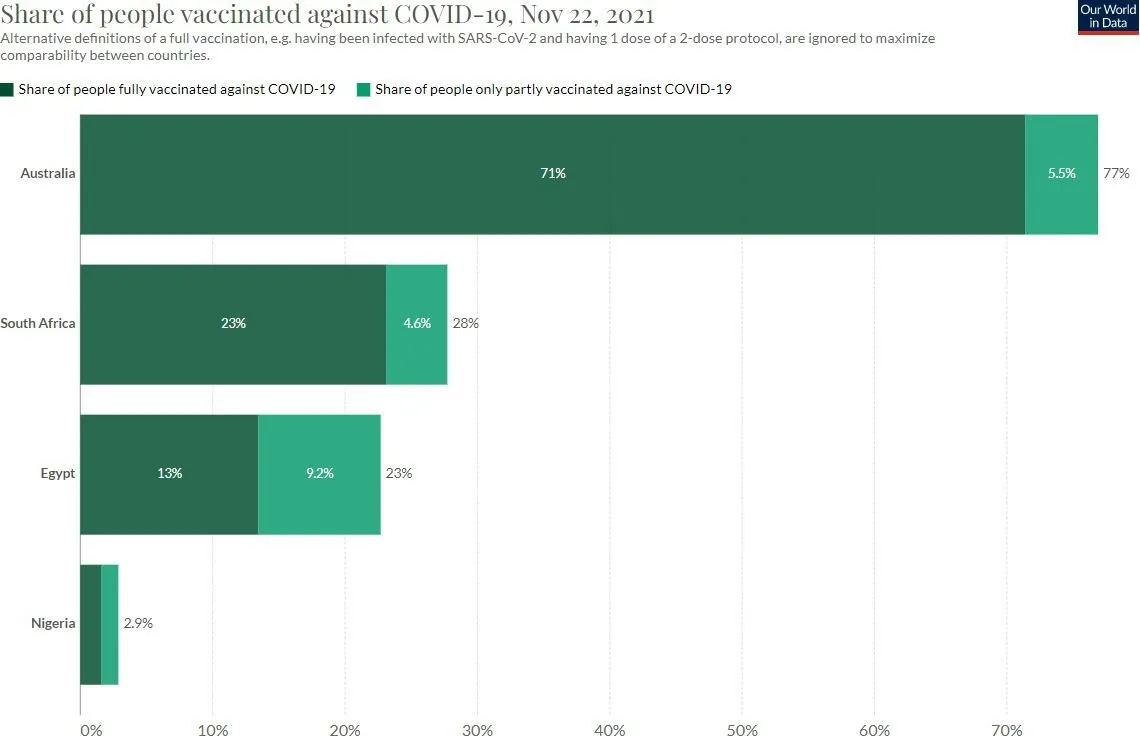
Figure 3 Share of people vaccinated against COVID- 19 as of 22 November 2021. Source: Official data collated by Our World in Data. This data is only available for countries which report the breakdown of dose administered by first and second doses in absolute numbers.
Policy- makers involved PC in the acute COVID- 19 phase to a greater or lesser degree. In Australia, a National COVID- 19 Primary Care Response was developed in consultation with stakeholders and ongoing engagement with the PC workforce, including a $1.1 billion initial funding package. This included provision of community- based mental health services. In Nigeria, policy- makers strengthened the role of and financial support for PC, but in South Africa national policy- makers mostly engaged with PH and infectious disease specialists with a focus on major hospitals and intensive care unit (ICU) beds. PC provided testing, treatment and support services to affected people, screening and testing took place in community settings in South Africa,8patients were triaged in PC in Nigeria and sent to PH centres for testing, while in Egypt there was limited coordination between PH and PC for triage and testing. In South Africa, family physicians also staffed and ran field hospitals for those only needing oxygen,recuperating, needing control of comorbidities or palliative care (not eligible for ICU).9
Technological innovations were apparent in all countries.Australia with more advanced technology and internet access,rapidly developed telehealth as an alternative to face- to- face consultations. In South Africa, PC facilities discovered the value of communicating with patients via alternative means(eg, WhatsApp) as most people have access to a mobile phone. In Egypt, a variety of technology innovations targeted specific high- risk groups such as telehealth for people with COVID- 19 and diabetes and a WhatsApp chatbot for supporting self- management in people with diabetes.10In Nigeria, PC used telehealth through phone calls and SMS messages via dedicated hospital lines alongside face- to- face consultations.
The challenges identified were remarkably similar for all four countries. For all, early availability of adequate supplies of personal protective equipment in PC was an issue. Problems associated with lack of coordination between PC and PH were outlined. Australia, a high- resource country, did not have issues with capacity for COVID- 19 testing, but testing ability was limited in Nigeria and Egypt and the long turn- around time for test results limited the effectiveness of contact tracing in South Africa. Faster vaccination was a major issue identified by Nigeria and Egypt as was initial vaccine supply and public concern about adverse effects in Australia and South Africa.
In South Africa, adaptation of PH messages to low socioeconomic contexts could have been done better with recognition of the inability to self- isolate for people living in shacks with shared toilets. Australia adopted a specific focus to equitable targeting of priority populations, including Aboriginal and Torres Strait Islander people, residents of aged care facilities, people from culturally and linguistically diverse backgrounds and those with disability.
CONCLUSlON: LESSONS FOR OTHER COUNTRlES
Table 2 outlines the strategies, experiences and limitations of each country’s response.
Each country summarised what had worked well, and what had not, from which other countries may learn. For Australia,having a National COVID- 19 Primary Care Response was key. Rapid introduction of telehealth for the whole population helped to reduce spread, protect the workforce and ensure continuity of care. General practitioners led ‘fever’clinics and vaccination offered through general practices and pharmacies across the country was catalysed by the public’s familiarity with PC settings, as well as through large,centralised hubs and in- reach programmes to support hardto- reach communities.
South Africa also identified that good communication and strong political leadership is key. What was needed was a clear command structure in the health system to coordinate all levels of care. Where community- orientated PC was implemented, this provided the ability to decongest facilities and provide more services in the community and household as well as to provide education and screening for COVID- 19 to the whole population at risk.7811However, community engagement and participation was insufficient in many areas to tailor PH messages to the local circumstances and ensureunderstanding and support for PH measures. Laboratory services proved to be a critical bottleneck.12
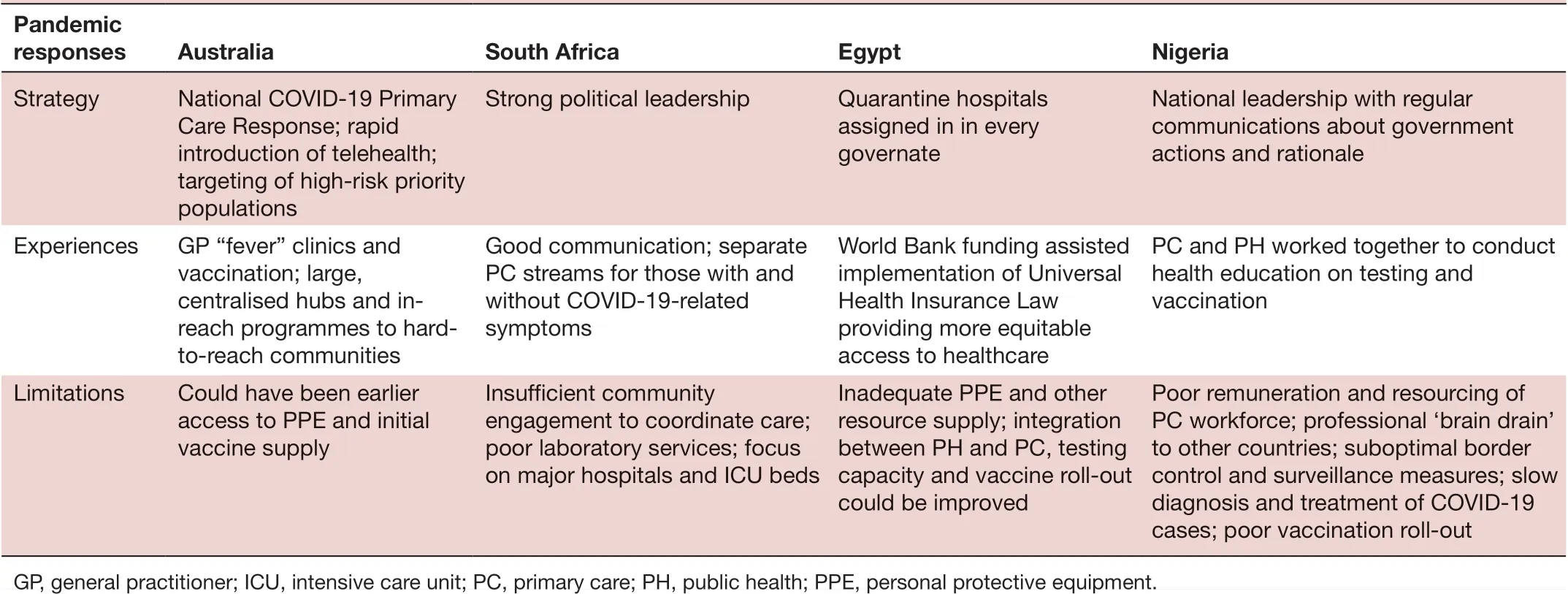
Table 2 Strategies, experiences and limitations of each country’s response
The Egyptian response included assigning quarantine hospitals in every governate, with medical teams composed of different specialties to take care of the inpatients in these hospitals. In June 2020, Egypt received US$400 million from the World Bank13to implement their 2018 Universal Health Insurance Law14and provide more equitable access to healthcare.
For Nigeria, the pandemic has highlighted the need for better remuneration and resourcing of the PC workforce to prevent or minimise the professional ‘brain drain’ to other countries. The response to the pandemic could have been improved by increased border control and surveillance measures, and the ability to promptly diagnose and treat COVID- 19 cases.
All four countries emphasised the critical importance of an integrated response between PC and PH services to protect the population, conduct surveillance, diagnose cases through testing, provide community- based care unless hospitalisation was required and vaccinate the population to reduce infection spread. The importance of collaboration, communication and integration between PC and PH in addressing epidemics has long been recognised.15Lack of involvement of PC and poor integration with PH in the COVID- 19 response has been identified in other countries.This was a key theme in a 2020 international study looking at the pandemic response in 111 countries,16–18and has also been recognised in a number of European studies.19–21PC frequently demonstrates agility and innovative capacity in the face of limited resources and a changing environment22contributing to the resilience required in the face of pandemics.
Author affiliations
1Department of General Practice and Primary Health Care, The University of Auckland, Auckland, New Zealand
2Department of Health, Australian Government, Canberra, Australian Capital Territory, Australia
3Department of Family Medicine, Ambrose Alli University, Ekpoma, Nigeria
4School of Medicine, Menoufia University, Shebin El- Kom, Egypt
5Department of Family and Emergency Medicine, Stellenbosch University,Stellenbosch, South Africa
6Department of Family Medicine, Marmara University, Istanbul, Turkey
7Center for Professionalism and Value in Health Care, American Board of Family Medicine, Lexington, Kentucky, USA
8Academic Unit of General Practice, Australian National University, Canberra,Australian Capital Territory, Australia
TwitterNagwa Nashat @nagwanashat
ContributorsAll authors contributed equally to this article and analysis, and read and approved the final version. FG- S organised the workshop and wrote the first draft of the paper. CvW chaired the workshop. MK, TIAO, NN and RM provided material from their respective countries. MA and RLP provided input into the analyses of the findings.
FundingThe authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interestsNone declared.
Patient consent for publicationNot applicable.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
ORClD iDsFelicity Goodyear- Smith http://orcid.org/0000-0002-6657-9401 Nagwa Nashat http://orcid.org/0000-0001-9470-5105 Chris van Weel http://orcid.org/0000-0003-3653-4701
 Family Medicine and Community Health2022年2期
Family Medicine and Community Health2022年2期
- Family Medicine and Community Health的其它文章
- Development and validation of the scale for measuring biopsychosocial approach of family physicians to their patients
- Acceptability of a task sharing and shifting model between family physicians and physiotherapists in French multidisciplinary primary healthcare centres: a cross- sectional survey
- Transitions in health service use among women with poor mental health: a 7- year follow- up
- Putting health workers at the centre of health system investments in COVID- 19 and beyond
- COVID- 19 vaccine hesitancy and related factors among primary healthcare workers in a district of Istanbul: a crosssectional study from Turkey
- Patient experience of residents with restricted primary care access during the COVID- 19 pandemic