
Timely vitrectomy without intraocular lens removal for acute endophthalmitis after cataract surgery
2022-06-22 03:14:00HaiXiaGuoRuoTianXieYunWangCaiYunYouYuanYuanLiuXiangDaMengJinGuoYuHuaYan
INTRODUCTION
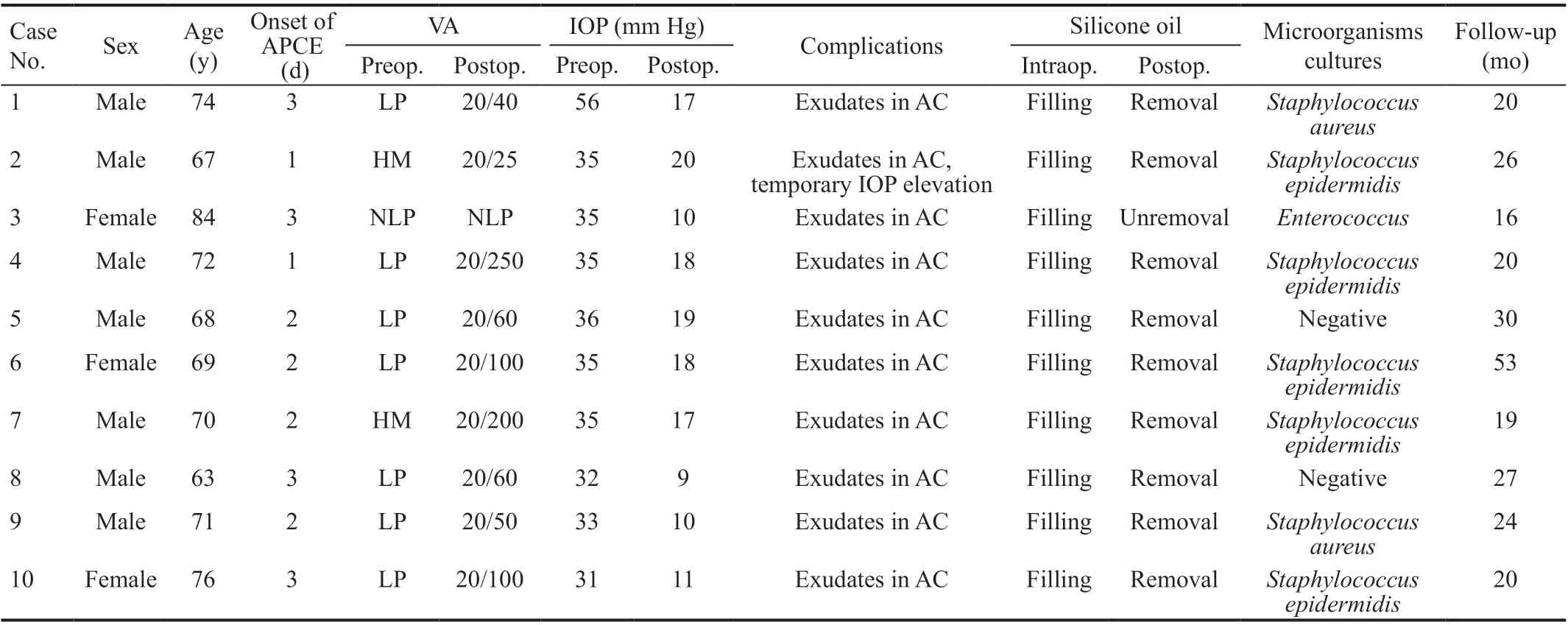
The mean age of all patients was 71.4y(range, 63-84y; Table 1). Five patients had a history of diabetic mellitus. All patients had symptoms of acute ocular pain and a sudden decrease of vision after cataract surgery. All patients had hypopyon, edema cornea, hyperemic and edema conjunctiva. The mean time between cataract surgery and the onset of endophthalmitis was 2d with a range from 1 to 3d.The mean follow-up period was 25.5mo with a range from 16 to 53mo.
Previous treatment methods included vitrectomy, IOL removal, and local and systemic use of antibiotics
; however,IOL removal decreases uncorrected visual acuity, leaving patients dissatisfied with the outcome, and likely leading to postoperative medical dissension. In most reports on the treatment of post-cataract endophthalmitis, the visual acuity of only half of the cases reached 20/40
. To date, there are few reports on the effect of vitrectomy on postoperative pseudophakic endophthalmitis without IOL removal.Therefore, the clinical features, causative organisms, and effects of vitrectomy and silicone oil tamponade without IOL removal in the treatment of APCE are reported here using a small case series.
SUBJECTS AND METHODS
从2004年开始,我国普通高校招收新疆高中班毕业生的工作实行“统一试卷、统一阅卷、单独划线、单独招生”的办法。2005年,国务院明确了高考录取过程中对少数民族考生优惠录取的政策。从2008年开始,对边疆、山区、牧区、少数民族聚居地区的少数民族考生,由省级招生委员会决定,可在高等学校调档分数线下适当降低分数要求投档,由学校审查决定是否录取。而教育部则表示少数民族高考加分政策不会改变。
This study involved a series of clinical characteristics and microbial factors in 10 eyes of 10 patients treated for APCE between January 2010 and December 2018 at Tianjin Medical University General Hospital. Post-cataract endophthalmitis is classified as APCE if it occurs within six weeks postoperatively, and chronic if it occurs after this period
. The diagnosis of APCE was the appearance of ocular pain, sudden vision decrease, conjunctival congestion and edema, corneal edema, hypopyon, and vitreous opacification after cataract surgery, regardless of whether the culture of intraocular fluid was ultimately positive
. Cases in which cataract surgery was combined with other eye surgeries were excluded. The posterior capsule had minor rupture during cataract surgery in 2 eyes, and was intact in 8 eyes. All patients received systemic antibiotics and vitrectomy combined with silicone oil tamponade, and the IOL was maintained in each eye.
The treatment indications for vitrectomy without IOL removal on APCE are as follows: 1) No abnormal changes in the implanted IOL, such as dissolution, reduced transparency, and deformation; 2) Patients with better corrected vision (>20/40)after cataract surgery before the occurrence of endophthalmitis;3) Absence of zonular dialysis or severe rupture of the posterior capsule (>1/4 quadrant) during cataract surgery; 4)Patients without severe systemic diseases.
神话故事最初来自民间,始于口头创造,经过一代又一代人的传承才得以流传至今。在神话故事中,神鬼和英雄传说为两大主体,其中蕴藏着人们对美好生活的向往,对理想的不懈追求和对英雄人物的推崇与尊敬,同时也是对现实压迫的一种反抗,因此神话故事中虽然多为不存在的事物,但其却是对现实世界最真实、最恰当的展现,以一种理想化的方式反映社会与人心,从中可以窥见人们的真实想法[1]。因此即便神话故事脱离现实,但后世的人们仍然能够了解当时的社会背景、人们所处的环境、生活方式、内心的状态和追求,极具层次性且具有深刻意义,是现实与想象的结合体。
例如,学生可以根据第二次笔记中记载的有关“蛋白质”专题的知识,进行蛋白质概念图的建构。学生在分析解决一定量的遗传题之后总结遗传题分析手段(方法)有两种: 通过遗传图解分析与通过系谱图分析等。
The Wilcoxon signed-rank test was used to assess the change in pre- and post-surgical IOP.
Routine topical cycloplegics (1.0% atropine sulfate) and topical corticosteroids(1.0% tobramycin dexamethasone) were administered 3 times per day for 7.0d after surgery. Systemic corticosteroids were administered orally with prednisolone at 30 mg once a day for 7.0d. Intravenous infusion of ofloxacin 100 mg twice a day for 7.0d and ofloxacin eye drops 3 times per day were then administered for 2.0wk. The routine follow-up was performed 1, 3, 5d, 1, 2, 4, 12wk, 6 and 12mo postoperatively.
All surgeries were performed under retrobulbar anesthesia (2.0% lidocaine) by the same surgeon(Yan H). An initial undiluted anterior chamber specimen was obtained for organism culture before irrigation/aspiration.The capsular bag was separated from the IOL with the use of viscoelastics. Then the anterior chamber and capsular bag were irrigated/aspirated completely and repeatedly. An initial undiluted vitreous specimen was also obtained for microbiological culture before vitrectomy. The posterior vitreous detachment from the optic disc was performed and infected vitreous was completely removed during vitrectomy.After vitrectomy, the anterior chamber and capsular bag were reirrigated/aspirated again if the anterior segment was not clear. Finally, the silicone oil was filled.
RESULTS
Although postoperative endophthalmitis is rare with an incidence of 0.02%-0.33%
, it is one of the most serious complications after cataract surgery
. If this condition is not treated in a timely manner, it may result in visual loss and even ocular atrophy. The incidence of endophthalmitis following phacoemulsification and intraocular lens (IOL)implantation is estimated to be between 0.012% and 1.3%since 2000
, and acute-onset post-cataract endophthalmitis(APCE) occurred in 0.04% cataract surgeries performed in the United States between 2013 and 2017
. Risk factors include anterior vitrectomy, cataract surgery combined with other ophthalmic surgery, younger age, intraoperative posterior capsule rupture, non-use of antibiotics, and non-use of behindthe-lens washout
.

据不完全统计,每年到林畲乡旅游参观的游客有5万余人次,其中包括前来研学旅行的学生,前来接受红色文化、廉政文化教育的群体和自驾游群体,以后还将有前来进行“医康养”项目的老年群体等,这意味着林畲乡的旅游产业将会逐渐壮大。
The mean pre-vitrectomy IOP was 36.3 mm Hg, with a range from 31 to 56 mm Hg. The mean post-vitrectomy IOP was 14.9 mm Hg with a range from 9.0 to 20 mm Hg (
<0.05).
The microorganisms of the aqueous humor and vitreous were
in 5 eyes (50%),
in 2 eyes (20%), and
in 1 eye (10%). Two eyes had negative cultures.
The pre-vitrectomy uncorrected visual acuity ranged from no light perception to hand motion and postvitrectomy from no light perception to 20/25 at the last followup (Table 1). After vitrectomy, the visual acuity increased in 9 eyes (90%), and unchanged in 1 eye (10%).
这是继5月英雄联盟季中冠军赛世界冠军、7月英雄联盟洲际系列赛亚洲对抗赛冠军、8月雅加达亚运会英雄联盟项目金牌之后,中国电竞战队再次斩获的重量级世界冠军。至此,在2018年的英雄联盟项目中,中国电竞战队创造历史最佳战绩,实现大满贯!
After vitrectomy, the symptoms of ocular pain progressively disappeared in all eyes. Corneal transparency was recovered,and hypopyon was not visible. The IOL was transparent in all eyes. Retinas remained completely attached in all eyes (10/10,100%) after vitrectomy. Silicone oil was removed in 9 eyes within 3.0-6.0mo postoperatively, and the retina remained attached in 9 eyes. The silicone oil was not removed in 1 eye that had no light perception because of serious retinal and vessel impairment. Figure 1 shows a case of APCE and final treatment result.
The examination and treatment of the patients were approved by the Ethics Committee of the Tianjin Medical University General Hospital and informed consent forms were obtained from all patients.
DISCUSSION
APCE is a serious complication
. It is different from anterior segment toxic reaction syndrome (TASS) in clinical and laboratory examinations
. If patients are not treated in a timely manner, the prognosis is poor
. Post-vitrectomy retinal detachment and management of IOL are still controversial in the treatment of APCE
. Vitrectomy for endophthalmitis has several advantages for patients, such as removing the infected organism, toxins and the infected vitreous that can cause subsequent retinal detachment
.Previous studies have shown that vitrectomy with silicone oil tamponade is preferable for post-surgery endophthalmitis
.Complete and early clearance of purulence and toxins is the most critical procedure for endophthalmitis, which will promptly halt and reverse potentially devastating damage to the eyes. Complete and early vitrectomy was the initial treatment of choice and recommended by recent studies compared with the tap-and-inject process in the Endophthalmitis Vitrectomy Study (EVS), with 79% of eyes achieving ≥20/40 visual acuity in a recent study compared to 53% in the EVS, especially for those whose initial visual acuity was light perception only
.Various factors have been described that influence the prognosis of APCE, such as microorganism virulence and treatment
. In our study, the APCE was diagnosed within 2.0d after cataract surgery and was immediately treated by vitrectomy. The higher culture-positive rate was obtained included
in 5 eyes,
in 2 eyes (20%), and
in 1 eye. The visual acuity increased in 9 eyes (90%) postoperatively, and one-half of the patients had a final vision of 20/60 or better. No retinal detachment or ocular atrophy was observed during the followup period. These results indicate that vitrectomy combined with silicone oil tamponade without IOL removal is effective and timely for APCE in our case series.
Previous methods of treating APCE include vitrectomy combined with IOL removal and irrigation/aspiration of the anterior chamber
. The purpose of these manipulations was to remove the bacteria easily and completely from the anterior chamber and capsular bag. Hayashi
reported that in some cases with delayed-onset post-cataract endophthalmitis,and IOL removal was required to eliminate the bacteria that adhered to the tip of the IOL haptic. Dave
concluded that IOL explantation could be necessary in the management of delayed-onset post-cataract endophthalmitis, while explantation of IOL is not a standard recommendation in the management of APCE. In our study, complete irrigation/aspiration of the anterior chamber and capsular bag was conducted intraoperatively, and there was no remaining inflammation in the anterior segment at the final follow-up. Therefore, we got the same effects though the IOL was not removed.
In addition, treating APCE with IOL removal may have some shortcomings, including a decrease of uncorrected visual acuity, retinal detachment and requirement of a secondary IOL implantation
. In the present study, vitrectomy without IOL removal can also successfully eradicate the endophthalmitis,increase uncorrected visual acuity with a low rate of postoperative complications and reoperation, and reduce unnecessary medical dissension.However, IOL removal or not in the treatment of APCE is still controversial, and we suggest that this management should be considered according to the different situations of different cases.
Supported by The Youth Incubation Foundation of Tianjin Medical University General Hospital (No.ZYYFY2018013).
None;
, None;
None;
None;
None;
None;
None;
None.
1 Simakurthy S, Tripathy K. Endophthalmitis. In:
Treasure Island (FL): StatPearls Publishing; 2022.
2 Patwardhan A, Rao GP, Saha K, Craig EA. Incidence and outcomes evaluation of endophthalmitis management after phacoemulsification and 3-piece silicone intraocular lens implantation over 6 years in a single eye unit.
2006;32(6):1018-1021.
3 Relhan N, Forster RK, Flynn HW Jr. Endophthalmitis: then and now.
2018;187:xx-xxvii.
4 Pershing S, Lum F, Hsu S, Kelly S, Chiang MF, Rich WL 3rd, Parke DW 2nd. Endophthalmitis after cataract surgery in the United States:a report from the intelligent research in sight registry, 2013-2017.
2020;127(2):151-158.
5 Bainbridge JW, Teimory M, Tabandeh H, Kirwan JF, Dalton R, Reid F,Rostron CK. Intraocular lens implants and risk of endophthalmitis.
1998;82(11):1312-1315.
6 Sun J, Guo Z, Li H, Yang B, Wu X. Acute infectious endophthalmitis after cataract surgery: epidemiological characteristics, risk factors and incidence trends, 2008-2019.
2021;14:1231-1238.
7 Das T, Dave VP, Dogra A, Joseph J, Sharma S; EMS working group.Endophthalmitis management study. Report #1. Protocol.
2021;69(7):1936-1941.
8 Kuhn F, Gini G. Ten years after… are findings of the Endophthalmitis Vitrectomy Study still relevant today?
2005;243(12):1197-1199.
9 Yannuzzi NA, Si N, Relhan N, Kuriyan AE, Albini TA, Berrocal AM, Davis JL, Smiddy WE, Townsend J, Miller D, Flynn HW Jr.Endophthalmitis after clear corneal cataract surgery: outcomes over two decades.
2017;174:155-159.
10 Cunha AM, Iglésias MM, Rocha-Sousa A, Falcão-Reis F, Falcão M.Endophthalmitis following intravitreal injection, cataract surgery,and vitrectomy: clinical features and visual outcomes.
2021;2021:9985821.
11 Kato JM, Tanaka T, de Oliveira LMS, de Oliveira MS, Rossi F,Goldbaum M, Pimentel SLG, de Almeida Junior JN, Yamamoto JH.Surveillance of post-cataract endophthalmitis at a tertiary referral center: a 10-year critical evaluation.
2021;7(1):14.
12 Ma X, Xie L, Huang Y. Intraoperative cefuroxime irrigation prophylaxis for acute-onset endophthalmitis after phacoemulsification surgery.
2020;13:1455-1463.
13 Sengillo JD, Chen Y, Perez Garcia D, Schwartz SG, Grzybowski A, Flynn HW Jr. Postoperative endophthalmitis and toxic anterior segment syndrome prophylaxis: 2020 update.
2020;8(22):1548.
14 Hernandez-Bogantes E, Navas A, Naranjo A, Amescua G, Graue-Hernandez EO, Flynn HW Jr, Ahmed I. Toxic anterior segment syndrome: a review.
2019;64(4):463-476.
15 Combey de Lambert A, Campolmi N, Cornut PL, Aptel F, Creuzot-Garcher C, Chiquet C; French Institutional Endophthalmitis Study Group. Baseline factors predictive of visual prognosis in acute postoperative bacterial endophthalmitis in patients undergoing cataract surgery.
2013;131(9):1159-1166.
16 Assil KK, Greenwood MD, Gibson A, Vantipalli S, Metzinger JL,Goldstein MH. Dropless cataract surgery: modernizing perioperative medical therapy to improve outcomes and patient satisfaction.
2021;32 Suppl 1:S1-S12.
17 Kannan NB, Sen S, Lalitha P, Mishra C, Rameshkumar G, Hariharan G,Siva Ganesa Karthikeyan R, Ramasamy K. Challenges in post-cataract surgery nocardia endophthalmitis: management strategies and clinical outcomes.
2020:1-6.
18 de Geus SJR, Hopman J, Brüggemann RJ, Klevering BJ, Crama N.Acute endophthalmitis after cataract surgery: clinical characteristics and the role of intracameral antibiotic prophylaxis.
2021;5(6):503-510.
19 Dib B, Morris RE, Oltmanns MH, Sapp MR, Glover JP, Kuhn F.Complete and early vitrectomy for endophthalmitis after cataract surgery:an alternative treatment paradigm.
2020;14:1945-1954.
20 Morris RE, Kuhn F. Complete and early vitrectomy for endophthalmitis.
2021;31(6):2794-2795.
21 Tabatabaei SA, Aminzade S, Ahmadraji A, Soleimani M, Sefidan BB, Kasaee A, Cheraqpour K. Early and complete vitrectomy versus tap and inject in acute post cataract surgery endophthalmitis presenting with hand motion vision; a quasi-experimental study.
2022;22(1):16.
22 Shirodkar AR, Pathengay A, Flynn HW Jr, Albini TA, Berrocal AM,Davis JL, Lalwani GA, Murray TG, Smiddy WE, Miller D. Delayedversus acute-onset endophthalmitis after cataract surgery.
2012;153(3):391-398.e2.
23 Patel SN, Storey PP, Levin H, Pancholy M, Obeid A, Wibbelsman TD,Kuley B, Ho AC, Hsu J, Garg SJ, Vander JF, Dunn JP. Endophthalmitis after cataract surgery: changes in management based on microbiologic cultures.
2021;5(1):16-22.
24 Hayashi Y, Eguchi H, Miyamoto T, Inoue M, Mitamura Y. A case of delayed-onset propionibacterium acnes endophthalmitis after cataract surgery with implantation of a preloaded intraocular lens.
2012;3(3):291-297.
25 Dave VP, Parmeshwarappa DC, Dogra A, Pappuru RR, Pathengay A,Joseph J, Das T. Clinical presentations and comparative outcomes of delayed-onset low-grade endophthalmitis managed with or without intraocular lens explantation.
2020;14:551-555.
猜你喜欢
红蜻蜓·低年级(2023年10期)2023-10-31 08:27:52
——王子今
作文小学高年级(2023年2期)2023-03-13 01:38:18
区域治理(2022年40期)2022-11-27 04:01:54
学生天地(2020年14期)2020-08-25 09:20:54
小哥白尼(趣味科学)(2019年7期)2019-11-16 09:04:20
动漫界·幼教365(小班)(2019年10期)2019-10-28 02:04:20
动漫界·幼教365(大班)(2019年10期)2019-10-28 01:54:09
动漫界·幼教365(中班)(2019年10期)2019-10-28 01:53:17
大众电视(蓝天下)(2018年8期)2018-10-26 01:00:16
下一代英才(酷炫少年)(2018年6期)2018-07-09 03:17:44
 International Journal of Ophthalmology2022年6期
International Journal of Ophthalmology2022年6期
- International Journal of Ophthalmology的其它文章
- Intraocular lens removal or not during vitrectomy for acute infectious endophthalmitis after cataract surgery
- Vitreous function and intervention of it with vitrectomy and other modalities
- Short-term outcomes of mitomycin C-augmented excisional bleb revision with capsulectomy for failed Ahmed glaucoma valve
- Evaluation of nintedanib as a new postoperative antiscarring agent in experimental extraocular muscle surgery
- Multimodal imaging of experimental choroidal neovascularization
- A novel Nance-Horan syndrome mutation identified by next-generation sequencing in a Chinese family