
Does the addition of Braun anastomosis to Billroth II reconstruction on laparoscopic-assisted distal gastrectomy benefit patients?
2022-06-22 01:36XiongGuangLiQiYingSongDiWuShuoLiBenLongZhangLiYuZhangDaGuanXinXinWangLuLiu
INTRODUCTION
Billroth I,Billroth II and Roux-en-Y reconstruction are the three most wildly applied reconstructions for distal gastrectomy[1].Among these reconstructions,Billroth II reconstruction is recognized to reduce a high proportion of patients with reflux gastritis,which decreases patient quality of life[2]and potentially leads to malignancy,gastritis and reflux esophagitis[3,4].In accordance with recent studies,the incidence of reflux gastritis after Billroth II reconstruction varies from 40% to 90%[5-7].The addition of Braun anastomosis has been performed after Billroth II reconstruction since 1885,aiming to reduce complications after Billroth II reconstruction.
12. Step-mother: The image of the evil stepmother occurs frequently in fairy tales. She is associated with jealousy69 and cruelty (Olderr 1986). In masculine psychology, the stepmother is a symbol of the unconscious in a destructive role (von Franz 1970). The stepmother figure is actually two sided, in that while she has destructive intentions, her actions often lead the protagonist70 into situations that identify and strengthen his or her best qualities.
However,based on the working experiences in the hospital,it was observed that patients who underwent Braun anastomosis could get serious reflux gastritis as well.Moreover,one recent study[8]found that the addition of a Braun anastomosis is not effective in preventing enterogastric bile reflux.Other studies suggested that Braun anastomosis has a minor impact on the incidence of reflux gastritis to pancreatoduodenectomy[9,10]and one anastomosis gastric bypass[11].Thus,whether Braun anastomosis can truly decrease the incidence of bile reflux to distal gastrectomy remains unknown.
The current study aimed to identify whether Braun anastomosis can truly decrease the incidence of bile reflux and improve the quality of life of the patients after Billroth II reconstruction on laparoscopic distal gastrectomy.
MATERIALS AND METHODS
Study design and data source
This retrospective cohort study was approved by our ethics committee at our institution.Between January 2015 and December 2019,a total of 143 patients with distal gastric cancer converted Billroth II reconstruction were collected in the 1
center of People’s Liberation Army General Hospital(PLA general hospital),Beijing,China.Of these patients,follow-up data was available for 93.These 93 patients were divided into two groups: Group 1(Billroth II reconstruction,33 patients);and Group 2(Billroth II reconstruction combined with Braun anastomosis,60 patients).
Laparoscopic-assisted distal gastrectomy with D2 lymphadenectomy was performed on all of the patients under the conduct of the Japanese classification of gastric carcinoma and the guidelines for the treatment of gastric carcinoma[12,13].The arteries and veins were cut in the laparoscopic vision and then a small incision(less than 10 cm)was made in the center of the abdominal wall.
One day, my phone rang. Don, it was my mother. You know I told you about the Addisons, who moved in next door to us. Well, Clara Addison keeps asking me to invite you over for cards some night.
To determine whether the addition of Braun anastomosis to Billroth II reconstruction on laparoscopyassisted distal gastrectomy benefits patients.
In comparison of postoperative complications,1 of the 33 patients in Group 1 suffered from bile reflux and 2 patients had anastomotic fistula.In Group 2,1 patient had anastomosis bleeding and 3 patients had anastomotic fistula.The total incidence of postoperative complications indicated nosignificant difference between the two groups(Table 2).
Participant selection
The inclusion criteria included:(1)Age from 18 to 75;(2)Pathologically diagnosed as distal gastric cancer;(3)Cancer pathological stage I-III(the 8
edition of the American Joint Committee on Cancer[15]);and(4)Complete clinical details.Exclusion criteria included: patients with serious heart disease or brain disease that influenced quality of life.A total of 143 patients were selected.Clinical data of the patients were collected and 93 of the 143 patients are followed up.Among the other 50 patients,40 patients were out of contact and 10 patients were dead.
Outcomes definition
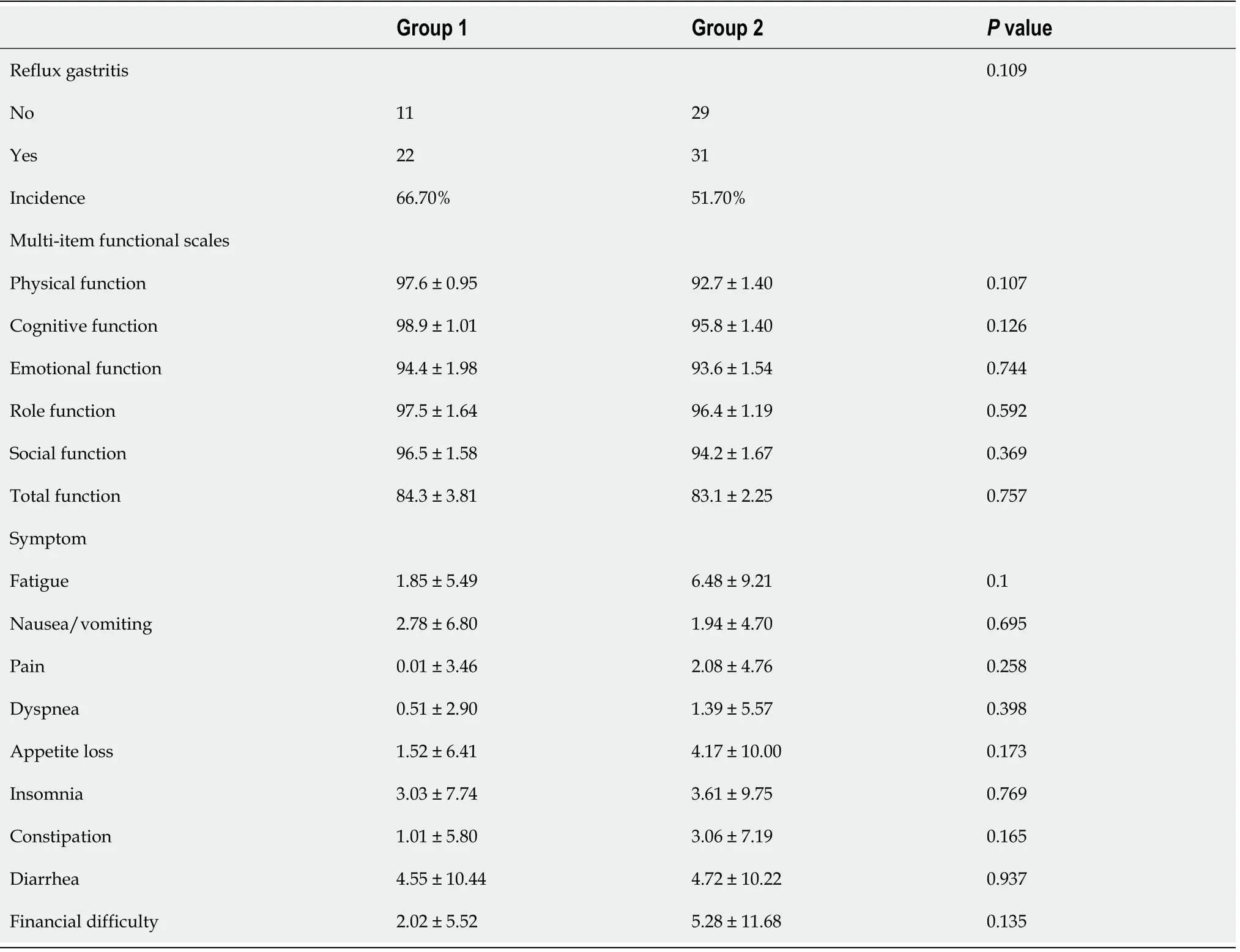
During follow-up,11 patients in Group 1 and 29 patients in Group 2 had reflux gastritis on their gastroscope report during the postoperative review.The total incidence of reflux gastritis showed no significant difference(66.7%
51.7%,
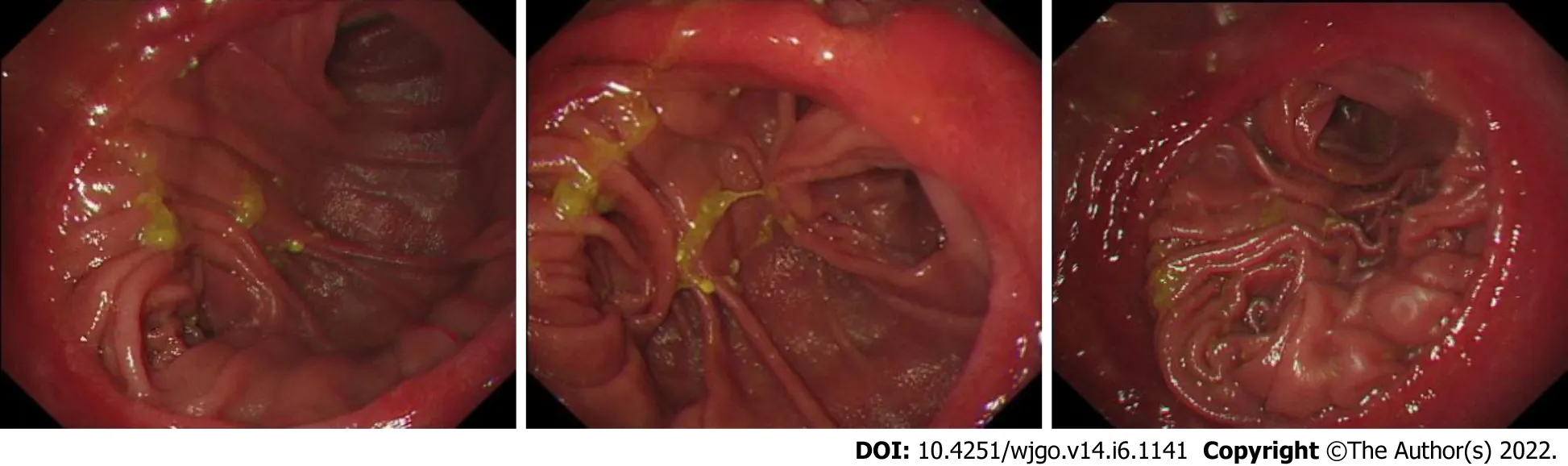
= 0.109).For five multi-item functional scales(physical,emotional,role,cognitive and social function),three multi-item and six single-item symptom scores,it showed no significant difference between these two groups(Figure 1 and Table 3).
As for me I lay still and watched them run, for I was very comfortable, and there I might be still if they had not come up, all panting and breathless, and compelled me to get up and follow them; they also reproached me bitterly, but I need hardly tell you that they did not again entrust123 me with the flock
Statistical analysis
All statistical analyses were performed with the support of SPSS v23.0 for Windows software.Continuous variables were expressed as mean ± SD and compared by Student’s
-test.Categorical variables were analyzed by Pearson
test.A two-tailed
value < 0.05 was considered statistically significant.
Then the lid sprang up to the right, and the princess came out, straight over him, and rushed round the church, howling and shrieking33 Sentry, where are you? Sentry, where are you? She went towards the altar, and right up to it, but there was no one there; then she screamed again,My father has set no sentry in, War and Pest will now begin
Before they closed my father s casket(,), I left him with a gift. After all he had given me, it was the least and best I could do. He passed away the day I got my 1,000th career hit, in the final game of the 2002 season, so at his side I left the ball from my milestone1.
RESULTS
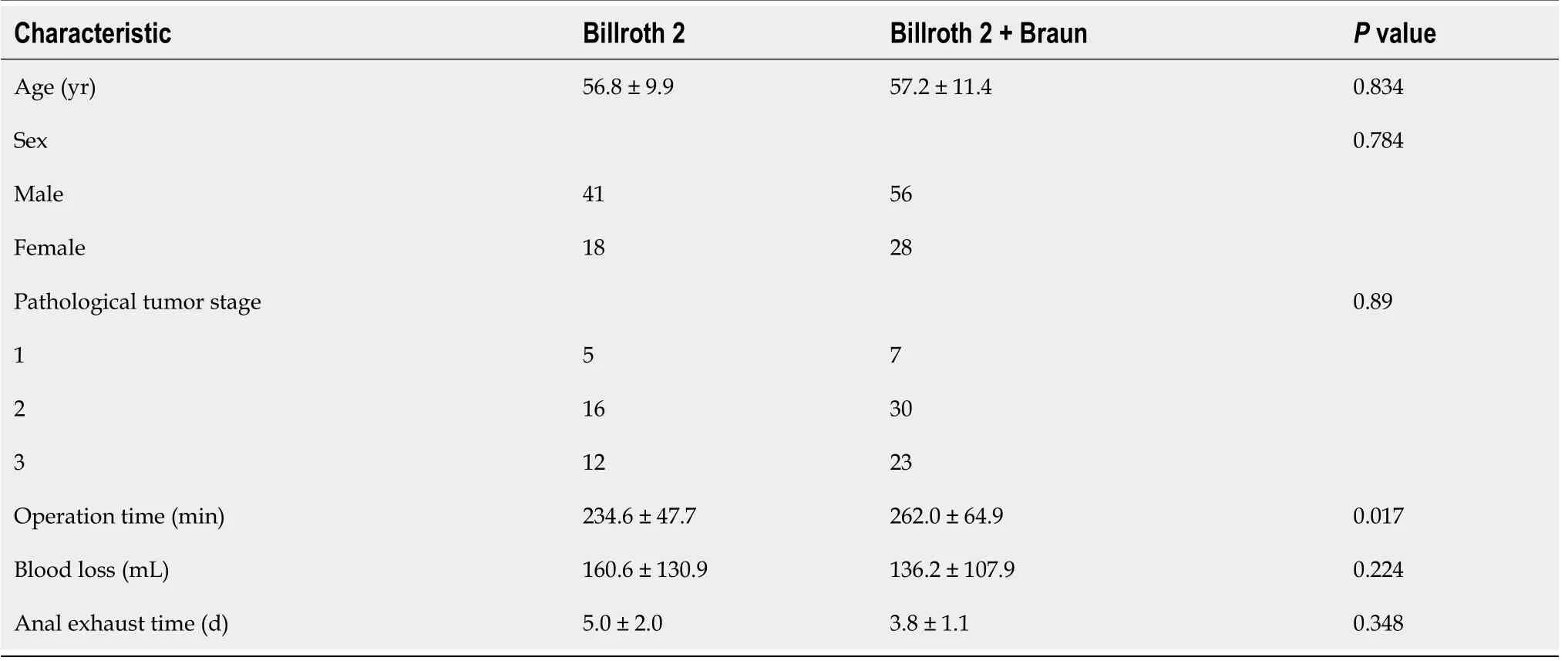
There were 33 patients in Group 1 and 60 patients in Group 2.The age,pathological tumor stage,sex,mean blood loss and mean exhaust time between the two groups was similar,while group 2 had a significantly longer mean operation time(Table 1).
Clinical data of the patients was collected,and 93 of the 143 patients were followed up.The follow-up data included:(1)The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 scores[14]of patients;and(2)The number of patients with reflux gastritis.All of the follow-up was completed between January 2021 and June 2021.Postoperative complications,relevant clinical data and follow-up data were compared as well.

The main outcomes of this study were the incidence of reflux gastritis after the operation and The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 scores,which is wildly applied in a variety of clinical studies[16-18].Patients were called and required to answer 30 questions from The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30.Scores were calculated based on five multi-item functional scales(emotional,physical,role,social and cognitive function),of which higher scores indicate better quality of life;three multi-item and six single-item symptom scores,of which higher scores indicate poorer quality of life.Reflux gastritis was diagnosed according to the gastroscope reports.
DISCUSSION
Billroth II reconstruction was invented in 1885 by Billroth as a modification of Billroth I.Due to the unique structure of Billroth II reconstruction,bile will flow through the residual stomach to the afferent loop,causing reflux gastritis(Figure 2A).Billroth II reconstruction is recognized with complications including anorexia,loss of appetite,dumping syndrome,nutritional anemia and alkaline reflux esophagitis[19].In a previous study,the addition of Braun anastomosis was regarded as a method to reduce the incidence of reflux gastritis.That is because Braun anastomosis could relieve the afferent loop pressure[20,21],making bile flow through the jejunum- jejunum anastomosis,rather than the residual stomach(Figure 2B).
I know that, said the man; your real father was sold at Hamburg last Michaelmas, and your real mother died while calving in spring; but my wife and I have adopted you as our own, and you are our only heir, so you must call me Father
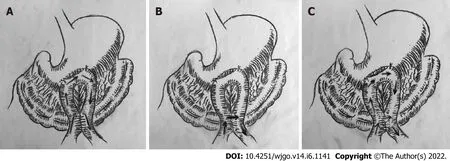
In this study,the incidence of reflux gastritis in Group 1 was lower than that in Group 2,but the difference was insignificant.It is indicated that bile may flow through both the residual stomach and the jejunum- jejunum anastomosis(Figure 2C).More experiments are needed to ensure this judgement.
In terms of postoperation complications,Group 1 and Group 2 were similar.The five multi-item functional scales(physical,emotional,role,cognitive and social function),three multi-item and six single-item symptom scores showed no significant difference as well.
CONCLUSION
The addition of Braun anastomosis to Billroth II reconstruction on laparoscopy-assisted distal gastrectomy did not show any benefit to patients with distal gastrectomy.
ARTICLE HIGHLIGHTS
Research background
The retainer, however, showed him the letter in which there was written that the queen and her children were to be burned, and everyone then understood that some great treachery had been enacted36
Research motivation
In Group 1,a small opening was made in the jejunum 20 cm away from the Treitz ligament on the anti-mesenteric margin and the residual gastric wall.The Billroth II anastomosis was performed with a 60 mm linear stapler in the end.In Group 2,jejunum-jejunum anastomosis was made 40 cm from the afferent limb.
Research objectives
To study the role of Braun anastomosis in laparoscopy-assisted distal gastrectomy.
Research methods
The clinical data of the addition of Braun anastomosis to Billroth II reconstruction on laparoscopyassisted distal gastrectomy for patients with distal gastric cancer were compared.Patient follow-up data were analyzed.Operation time,blood loss,anal exhaust time and prevalence rate of reflux gastritis between the groups were examined.
Research results
Postoperative complications were reported in 3 of the 33 patients in the Billroth II reconstruction group and 4 out of 60 patients in the Billroth II reconstruction combined with Braun anastomosis group.The total incidence of postoperative complications indicated no significant difference between the two groups.During follow-up,11 patients in the Billroth II reconstruction group and 29 patients in the Billroth II reconstruction combined with Braun anastomosis group had reflux gastritis.The total incidence of reflux gastritis showed no significant difference(66.7%
51.7%,
= 0.109).Five multi-item functional scales(physical,emotional,role,cognitive and social function),three multi-item and six single-item symptom scores showed no significant difference between these two groups.
At last the little tailor, losing all patience, reached out of his chimney corner for a duster, and exclaiming: Wait, and I ll give it to you, he beat them mercilessly with it
Research conclusions
In conclusion,this study indicated that the addition of Braun anastomosis to Billroth II reconstruction made no significant difference in reducing the incidence of reflux gastritis.The addition can hardly improve the quality of life of the patients but extends the operation time.Thus,the addition of Braun anastomosis is not necessary,and simple Billroth II reconstruction should be wildly applied.
Braun anastomosis is usually performed after Billroth II reconstruction on laparoscopy-assisted distal gastrectomy because it is believed to benefit patients.But we found that patients who underwent Braun anastomosis still had serious complications after operation.Thus,studies are needed to confirm that.
Research perspectives
A prospective study with more patients is required to verify the conclusions of this study.
FOOTNOTES
Li XG designed the experiment;Song QY and Wu D performed the experiment;Li S and Zhang BL collected data;Zhang LY and Guan D managed data;Liu L created the tables and figures based on data;Li XG,Song QY and Wu D wrote the initial draft;Wang XX modified the draft;Li XG,Song QY and Wu D contributed equally to this article.
The study was reviewed and approved by the Ethics Committee of PLA General Hospital(Approval No.S2021-579).
It s just a small, white envelope stuck among the branches of our Christmas tree. No name, no identification, no inscription(,). It has peeked1 through the branches of our tree for the past 10 years or so.
Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work,there is no professional or other personal interest of any nature or kind in any product,service and/or company that could be construed as influencing the position presented in,or the review of,the manuscript entitled.
No additional data are available.
The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Xiong-Guang Li 0000-0002-9039-4562;Qi-Ying Song 0000-0003-4953-9683;Di Wu 0000-0003-1620-2224;Shuo Li 0000-0002-1631-6654;Ben-Long Zhang 0000-0002-2844-9964;Li-Yu Zhang 0000-0001-8599-155x;Da Guan 0000-0003-1816-5471;Xin-Xin Wang 0000-0001-2492-4932;Lu Liu 0000-0003-2593-3758.
For the last time, the hat was passed around the table. Little Mike pulled out a name, and Daddy whispered it to him, just as he had done every week. Randi unfolded hers carefully under the table, peeked23 at it and hunched24 up her shoulders, smiling. Kelly reached into the hat and giggled happily when she saw the name. Mother and Daddy each took their turns, too, and then handed the hat with the last name to Eric. But as he unfolded the small scrap of paper and read it, his face pinched up and he suddenly seemed about to cry. Without a word, he ran from the room.
Yan JP
Filipodia
Yan JP
1 Hirao M,Takiguchi S,Imamura H,Yamamoto K,Kurokawa Y,Fujita J,Kobayashi K,Kimura Y,Mori M,Doki Y;Osaka University Clinical Research Group for Gastroenterological Study.Comparison of Billroth I and Roux-en-Y reconstruction after distal gastrectomy for gastric cancer: one-year postoperative effects assessed by a multi-institutional RCT.
2013;20: 1591-1597[PMID: 23104705 DOI: 10.1245/s10434-012-2704-9]
2 Svensson JO.Duodenogastric reflux after gastric surgery.
1983;18: 729-734[PMID: 6669936 DOI: 10.3109/00365528309182087]
3 Osugi H,Fukuhara K,Takada N,Takemura M,Kinoshita H.Reconstructive procedure after distal gastrectomy to prevent remnant gastritis.
2004;51: 1215-1218[PMID: 15239282]
4 Sato T,Miwa K,Sahara H,Segawa M,Hattori T.The sequential model of Barrett's esophagus and adenocarcinoma induced by duodeno-esophageal reflux without exogenous carcinogens.
2002;22: 39-44[PMID: 12017320]
5 Yang D,He L,Tong WH,Jia ZF,Su TR,Wang Q.Randomized controlled trial of uncut Roux-en-Y
Billroth II reconstruction after distal gastrectomy for gastric cancer: Which technique is better for avoiding biliary reflux and gastritis?
2017;23: 6350-6356[PMID: 28974902 DOI: 10.3748/wjg.v23.i34.6350]
6 Ren Z,Wang WX.Comparison of Billroth I,Billroth II,and Roux-en-Y Reconstruction After Totally Laparoscopic Distal Gastrectomy: A Randomized Controlled Study.
2019;36: 2997-3006[PMID: 31605307 DOI: 10.1007/s12325-019-01104-3]
7 Pribadi RR,Rani AA,Abdullah M.Challenges of endoscopic retrograde cholangiopancreatography in patients with Billroth II gastrointestinal anatomy: A review article.
2019;20: 631-635[PMID: 31577857 DOI: 10.1111/1751-2980.12821]
8 Lee MS,Ahn SH,Lee JH,Park DJ,Lee HJ,Kim HH,Yang HK,Kim N,Lee WW.What is the best reconstruction method after distal gastrectomy for gastric cancer?
2012;26: 1539-1547[PMID: 22179454 DOI: 10.1007/s00464-011-2064-8]
9 Fujieda H,Yokoyama Y,Hirata A,Usui H,Sakatoku Y,Fukaya M,Nagino M.Does Braun Anastomosis Have an Impact on the Incidence of Delayed Gastric Emptying and the Extent of Intragastric Bile Reflux Following Pancreatoduodenectomy?
2017;34: 462-468[PMID: 28132059 DOI: 10.1159/000455334]
10 Wang L,Su Ap,Zhang Y,Yang M,Yue Pj,Tian Bl.Reduction of alkaline reflux gastritis and marginal ulcer by modified Braun enteroenterostomy in gastroenterologic reconstruction after pancreaticoduodenectomy.
2014;189: 41-47[PMID: 24679695 DOI: 10.1016/j.jss.2014.01.025]
11 Olmi S,Oldani A,Cesana G,Ciccarese F,Uccelli M,De Carli SM,Villa R,David G,Giorgi R,Zanoni AAG.Laparoscopic One Anastomosis Gastric Bypass Versus Laparoscopic One Anastomosis Gastric Bypass with Braun Anastomosis: What's Better?
2019;29: 1469-1474[PMID: 31017503 DOI: 10.1089/lap.2019.0218]
12 Nakajima T.Gastric cancer treatment guidelines in Japan.
2002;5: 1-5[PMID: 12021853 DOI: 10.1007/s101200200000]
13 Japanese Gastric Cancer Association.Japanese Classification of Gastric Carcinoma - 2nd English Edition -.
1998;1: 10-24[PMID: 11957040 DOI: 10.1007/s101209800016]
14 Fayers PM,Aaronson NK,Bjordal K.EORTC Scoring Manual.3rd ed.EORTC Quality of Life Study Group.Brussels: European Organisation for Research and Treatment of Cancer,2001
15 Amin MB,Edge S,Greene F,Byrd DR,Brookland RK,Washinghton MK.AJCC Cancer Staging Manual.Springer,2017
16 Nolte S,Liegl G,Petersen MA,Aaronson NK,Costantini A,Fayers PM,Groenvold M,Holzner B,Johnson CD,Kemmler G,Tomaszewski KA,Waldmann A,Young TE,Rose M;EORTC Quality of Life Group.General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries,Canada and the Unites States.
2019;107: 153-163[PMID: 30576971 DOI: 10.1016/j.ejca.2018.11.024]
17 Husson O,de Rooij BH,Kieffer J,Oerlemans S,Mols F,Aaronson NK,van der Graaf WTA,van de Poll-Franse LV.The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the "Real-World": Results from the Population-Based PROFILES Registry.
2020;25: e722-e732[PMID: 32297435 DOI: 10.1634/theoncologist.2019-0348]
18 Schmidt ME,Wiskemann J,Armbrust P,Schneeweiss A,Ulrich CM,Steindorf K.Effects of resistance exercise on fatigue and quality of life in breast cancer patients undergoing adjuvant chemotherapy: A randomized controlled trial.
2015;137: 471-480[PMID: 25484317 DOI: 10.1002/ijc.29383]
19 Shirbeigi L,Halavati N,Abdi L,Aliasl J.Dietary and Medicinal Herbal Recommendation for Management of Primary Bile Reflux Gastritis in Traditional Persian Medicine.
2015;44: 1166-1168[PMID: 26587489]
20 Wang F,Zu HL,Jiang H,Kang Y,Dong PD,Xue YW.Clinical investigation of combined Billroth II with Braun anastomosis for patients with gastric cancer.
2014;61: 1812-1816[PMID: 25436384]
21 Vogel SB,Drane WE,Woodward ER.Clinical and radionuclide evaluation of bile diversion by Braun enteroenterostomy: prevention and treatment of alkaline reflux gastritis.An alternative to Roux-en-Y diversion.
1994;219: 458-65;discussion 465[PMID: 8185396 DOI: 10.1097/00000658-199405000-00003]
 World Journal of Gastrointestinal Oncology2022年6期
World Journal of Gastrointestinal Oncology2022年6期
- World Journal of Gastrointestinal Oncology的其它文章
- Circular RNAs in hepatocellular carcinoma:Recent advances
- Practical considerations for colorectal cancer screening in older adults
- Can dietary flavonoids be useful in the personalized treatment of colorectal cancer?
- Fibrolamellar hepatocellular carcinoma:A rare but unpleasant event
- Glutamine deprivation impairs function of infiltrating CD8+ T cells in hepatocellular carcinoma by inducing mitochondrial damage and apoptosis
- Contemporary,national patterns of surgery after preoperative therapy for stage II/III rectal adenocarcinoma