
iStent inject® and cataract surgery for mild-to-moderate primary open angle glaucoma in Japan: a cost-utility analysis
2022-06-22 03:12:34AtaruIgarashiKyokoIshidaNobuyukiShojiAliceChuHeatherFalveyRuHanMakiUeyamaYoshieOnishi
INTRODUCTION
Glaucoma is a chronic, progressive disease resulting in a degeneration of the optic nerve. It is a leading cause of irreversible blindness in Japan
. In 2015, a nationwide survey of welfare offices in Japan ranked glaucoma as the first causative disease (29%) among newly certified visually impaired individuals ≥18y
. Primary open angle glaucoma(POAG) is the most common type of glaucoma
. It is characterized by a progressive vision loss due to the loss of retinal ganglion cells and optic nerve damage and by optic neuropathy combined with ocular hypertension (OHT)
.Population-based studies from the early 2000s estimated the prevalence of POAG in Japan to be 4% among adults aged ≥40y
. Due to the asymptomatic nature of mild-tomoderate POAG, 93% of patients with POAG in Japan remains undiagnosed and not treated
. The epidemiological study conducted between 2000 and 2002 found a high rate of newly diagnosed cases of glaucoma (89%)
despite the emphasis of the Japanese Glaucoma Society Guideline
on the importance of an early diagnosis and treatment for avoiding permanent vision loss.
Scenario analysis considering the full caregiver burden from a societal perspective was conducted to test the robustness of results.
In this cost-utility analysis, the iStent
inject
with cataract surgery strategy was found to be cost-effective
cataract surgery alone in patients with mild-to-moderate POAG needing cataract surgery. At the WTP threshold of ¥5 000 000/QALY, the iStent
inject
with cataract surgery strategy was found to have at least a 90% probability of being cost-effective.The results are considered robust based on one-way sensitivity analyses. Considering the loss of productivity of family caregivers and caregiver burden, the iStent
inject
with cataract surgery strategy was found to dominate cataract surgery alone and save costs associated with loss of productivity of working family caregivers and caregiver burden in patients needing cataract surgery. When the cost of iStent
inject
with cataract surgery increased from the original input of ¥279 900 to¥516 300, the ICUR reached the WTP threshold ¥5 000 000/QALY gained.This is the first cost-utility analysis comparing the iStent
inject
with cataract surgery
cataract surgery alone in the Japanese patients with mild-to-moderate POAG. The model inputs were obtained from the Japanese and global data with validation by Japanese clinical experts to represent the local Japanese setting.The results from this model are consistent with previously published studies that used the same model adapted to different settings, including France
, Canada
and Spain
. A similar cost-utility analysis to the present analysis assessed combined MIGS of one or two trabecular micro-bypass stents with cataract surgery in German patients with POAG
. However,the analysis was conducted separately in two subgroups of patients with moderate and advanced POAG. The study found that in the moderate stage, the implementation of two stents during cataract surgery produced the highest effectiveness and the lowest ICUR among cataract surgery combined with three alternative MIGS methods: 1) one trabecular micro-bypass stent, 2) two stents, and 3) intracanalicular scaffold, compared with cataract surgery alone. These findings reinforce the benefit of using iStent
inject
on early stages of POAG.
SUBJECTS AND METHODS
A Canadian health state-transition Markov model
was adapted to estimate the cost-utility of iStent
inject
combined with cataract surgery compared with cataract surgery alone in one eye in patients with mild-to-moderate POAG over lifetime horizon with monthly cycle length from the perspective of Japanese public payer. Health outcomes included quality-adjusted life-year (QALY) as the primary outcome and life years and number of blind eyes as the secondary outcomes. Cost outcomes included a total cost as the primary outcomes, while secondary outcomes were surgery(cataract surgery with or without iStent
inject
, trabeculotomy,trabeculectomy), medication, progression-related medical service (physician consultation, test), and AEs (hyphema,hyperaemia, stent obstruction, medication for AEs). The full caregiver burden was evaluated in the scenario analysis and considered productivity loss of working family caregivers and caregiver burden proxied by long-term care insurance level 1.Costs and health outcomes were discounted at a 2.0% annual rate based on the Japanese guideline
.
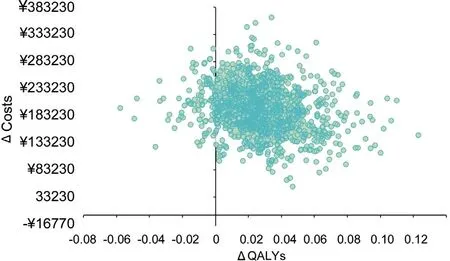
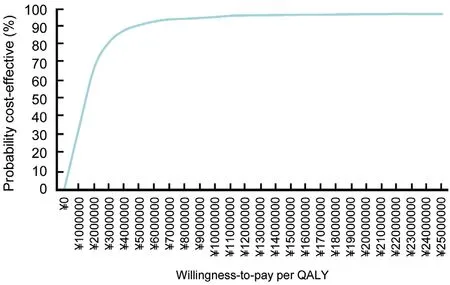
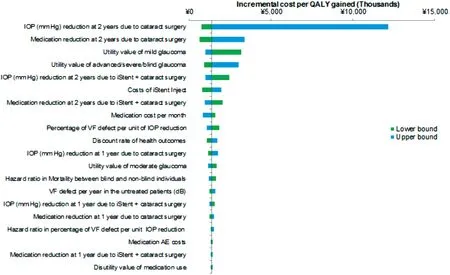
Both deterministic and probabilistic sensitivity analyses were conducted to evaluate the impact of assumptions used in the model and the variability surrounding model inputs. The deterministic one-way sensitivity analysis(OWSA) was conducted for the deterministic base case to determine the significant drivers of cost-utility. The 95%confidence interval was used as lower and upper bounds of the one-way sensitivity analysis. When not available, a ±25%variation of the deterministic base value was applied for the low and high values. Probabilistic base case analysis was conducted using 1000 iterations from random draws of the underlying parameter uncertainty. A beta distribution was used for proportion and utility values; a gamma distribution was considered for costs; a lognormal distribution was used for healthcare resource uses; and a normal distribution was considered for clinical data. The probabilistic base case analysis was expressed as ICUR scatterplot and costeffectiveness acceptability curve (CEAC). The willingness-topay (WTP) threshold of ¥5 000 000/QALY in Japan, set by the Central Social Insurance Medical Council (Chuikyo), was used as a marker to judge the cost-utility
.
窗外明媚的秋光从窗帘缝隙里钻进来,空中悬浮着灰尘。这世界满是尘埃,漂浮在空气中或停留在某一处,看似不存在,其实随处可见。
The model structure has previously been published
and was validated by Japanese clinical experts to reflect current clinical practice in Japan (Figure 1). Patients with mild-to-moderate POAG treated with background ocular hypotensive medications entered the model initiating cataract surgery with or without iStent
inject
. Patients could progress from baseline severity levels to next severity levels, defined according to the visual field (VF) defect (decibels, dB)
as mild glaucoma (0 to 6 dB), moderate glaucoma (6.01 to 12 dB),advanced glaucoma (12.01 to 20 dB), and severe glaucoma or blindness (<20 dB). Patients could discontinue background medication due to non-adherence, contraindications and intolerable AEs and receive subsequent surgeries in the case of disease progression such as trabeculotomy, followed by trabeculectomy as the last surgery. AEs of background medication, such as dryness, redness, and blurred vision and AEs of cataract surgery and iStent
inject
combined with cataract surgery, including stent obstruction, hyperaemia, and hyphema, were considered.

Inputs of the model, including patients’characteristics, clinical data, utility, and costs, were drawn from clinical trials, the literature and official Japanese sources.The Japanese data were used whenever available. Japanese clinical experts validated all assumptions and data used in the model.
改革开放前的相当长一段时期,我国新闻出版业重生产轻市场、重出版轻发行的倾向十分明显。不仅出书品种少,书报刊的流通销售渠道更是不畅,新华书店作为唯一的合法发行力量,远远无法满足群众日益旺盛的购书需求。1982年文化部发布《关于图书发行体制改革工作的通知》,提出我国图书发行体制改革的总目标:在全国组成一个以国有新华书店为主体,多种经济成分、多条流通渠道、多种购销形式、少流转环节的图书发行体系,即“一主三多一少”。这项改革打破了新华书店对图书发行权尤其是批发权的长期垄断,极大地刺激了民营书商的发展。据统计,到1987年年底,非国有书店从无到有,发展到1万多家,数量是国有书店的1.18倍。[2]
To reflect the Japanese real-world setting, the model was populated with clinical characteristics collected from the Japanese cross-sectional study
. Patients needing cataract surgery entered the model at a mean age of 64.5y, 60.5% in mild and 39.5% in moderate health state.In the absence of other glaucoma epidemiology in Japan,data were obtained from the Early Manifest Glaucoma Trial(EMGT) conducted in the US
. The relative risk of mortality was obtained from an Australian cohort
.
Three types of clinical data were included in the model: treatment pattern, efficacy, and safety. As no Japanese data were identified, global data from the original model were used. In the absence of treatment pattern for glaucoma in Japan, the VF defect at entry (-3.0 dB for mild patients and -6.0 dB for moderate patients) and during progression (-0.05 dB natural decline rate per month in untreated patients), mean time to receive subsequent surgeries and hazard ratio of receiving subsequent surgeries per unit of IOP reduction compared with no IOP change (0.83) were obtained from the EMGT
and expert opinions. The time to background medication discontinuation (59.53mo) was based on expert opinions. The IOP reduction, utilisation of background medication, and probabilities of AEs caused by cataract surgery and subsequent surgeries were based on an RCT comparing iStent
inject
combined with cataract surgery with cataract surgery alone
. Probabilities of AEs caused by background medication was obtained from a cost-utility analysis investigating the long-term health and economic outcomes of direct pressure-lowering medication for OHT
.
In the absence of Japanese data, global data from the original model were used
. Utility values of patients in different severity levels and disutility values due to subsequent surgeries and background medication for AEs were obtained from a Dutch cross-sectional survey assessing the impact of VF defect on POAG patient utility values
. Health preference was measured by the Health Utilities Index 3 (HUI-3) using tariffs for the Canadian population. In the absence of disutility value for trabeculotomy, the same disutility value for trabeculectomy was assumed for trabeculotomy with confirmation from the clinical experts.
The ICUR scatterplot in probabilistic base case analysis is shown in Figure 2. iStent
inject
with cataract surgery strategy was found to produce higher QALYs in 97.8% of the iterations. All the probabilistic simulations suggest iStent
inject
is associated with an increase in costs.Figure 3 presents the results of CEAC. At the WTP threshold of ¥5 000 000 per QALY gained, the iStent
inject
with cataract strategy was found to have a 90% probability of being cost-effective. Figure 4 presents the results of OWSA.The top key drivers of ICUR were an IOP reduction at 2y due to cataract surgery alone, medication reduction at 2y due to cataract surgery alone and utility value of mild glaucoma.
For background medication, the cost element consisted of actual medication costs and medication service costs, including fees of prescription, basic dispensing, dispensing, and drug management instruction. According to the Japanese Glaucoma Society guidelines
, Japanese published study
and clinical expert opinions, four categories of drugs are currently used as standard medications in Japan: prostaglandin (PG) as the 1
line, beta-blocker (BB) and combination of PG and BB as the 2
line, and more than 2 combinations of carbonic anhydrase inhibitors (CAI)/BB+PG medication as the 3
line.Market shares of medications were obtained from Inoue
and expert opinion. Unit costs of medications were obtained from the MHLW
. Unit cost of medication service per bottle were obtained from the MHLW
. Based on the expert input, medical wastage was not considered. To treat AEs caused by background medication, patients need to consult an ophthalmologist (1 time/mo) and have some tests run,
slitlamp microscopy (1 time/mo) and Goldmann applanation(2 times/mo). The healthcare resource use and frequency of treatment of AEs caused by surgeries are presented in Table 1.
网络密度指网络中各节点之间联系的紧密程度,节点之间联系越多,网络密度就越大[12]。经计算分析,三峡旅游流的网络密度为0.248 3,表明大三峡旅游地区景区存在一定的网络联系,但部分节点联系不紧密。从节点中心性来看,三峡旅游流主要向解放碑、白帝城、小三峡、神女峰、三峡大坝、三峡人家、恩施大峡谷几个景区聚集,以传统三峡旅游游线景区为主,与三峡腹地景区联系较少,与三峡周边极富吸引力的旅游目的地如九寨-黄龙联系较少,与其他景区节点的旅游联系也较弱,区域旅游整体发展出少数景区集聚现象,

In the scenario analysis from a societal perspective, full caregiver burden consisting of productivity loss of working family caregiver and formal caregiver burden were only applied to severely affected patients. An average wage of working family caregiver (¥307 700/mo) was collected from the MHLW
. It was assumed that 20% of severely affected patients would have family caregiving with a frequency of once a month. Formal caregiver burden was proxied by longterm care insurance level 1 (¥112 400/mo) as defined by the MHLW
under the assumption that all severely affected patients require the same level of care as patients receiving level 1 nursing care. A health economics expert verified the assumptions.
观察组的肠鸣音恢复时间、肛门自主排气时间均明显少于对照组,其护理满意度大于对照组(P<0.05),具体见表1。
Given the progressive nature of the disease, the main objectives of all glaucoma treatments are to safely reduce and maintain intraocular pressure (IOP) to a target level that will preserve the remaining vision
and to minimize the resulting negative effect on the patient’s quality of life (QoL)
. Since nonadherence to therapy can have a negative impact on clinical outcomes, treatment should be selected carefully with consideration of the patient’s QoL, lifestyle and comorbidities as well as medication-associated adverse events (AEs), costs and life expectancy
.
RESULTS
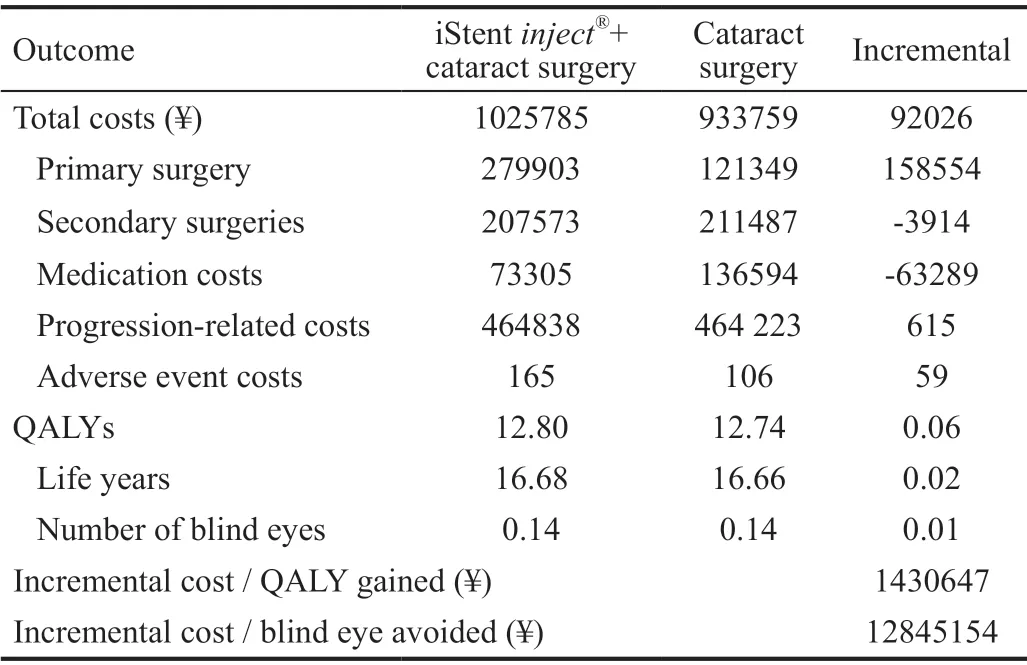
The iStent
inject
with cataract surgery strategy was found to be cost-effective compared with cataract surgery alone over a lifetime horizon in the probabilistic base case analysis. The incremental cost-utility ratio (ICUR) was estimated to be ¥1 430 647/QALY gained and the incremental costeffectiveness ratio (ICER) was estimated to be ¥12 845 154/blind eye avoided. The iStent
inject
with cataract strategy was found to increase cost compared to cataract surgery alone (¥1 025 785
¥933 759, respectively) but was more effective in increasing QALYs (12.80
12.74) and avoiding blinded eyes (0.133
0.141) than cataract surgery alone.The differences in costs were mainly driven by the cost of primary surgery (¥279 903
¥121 349). The iStent
inject
with cataract surgery vs cataract surgery strategy was found to be cost-saving in two cost components: cost of secondary surgery (¥207 573
¥211 487, respectively) and cost of medication (¥73 305
¥136 594). Small differences were found between iStent
inject
with cataract surgery strategy and cataract surgery strategy alone in progression-related medical cost (¥464 838
¥464 223, respectively) and AE costs (¥165
¥106). The base case results are depicted in Table 2.
牛皮糖站在一块预制板上,俨然一位乐队指挥正在指挥一场协奏曲。挥舞着手臂,指挥着他的队伍,淋漓酣畅地开始了前所未有的伟大工程。看到镇长前来,他连忙放下手头工作,匆匆赶到镇长和村长站着的那堆红砖面前。
Five types of cost data were included in the model:surgery procedure costs, progression-related medical service costs, background medication costs, AE-related treatment costs,and societal costs. All costs were as of April 2021. Procedure fees for iStent
inject
, cataract surgery, trabeculotomy, and trabeculectomy were obtained from the Japanese Ministry of Health, Labour and Welfare (MHLW)
. Progressionrelated medical service costs were calculated as the product of frequencies and unit costs of healthcare resource use, including physician consultation, VF defect test, optic disc imaging,examination of the ocular fundus, IOP measurement, eyesight test, slit-lamp microscopy, and gonioscopy. Frequency data were obtained from clinical experts. Unit costs were obtained from the MHLW
.
The Markov model used in this analysis ensured a robust approach to evaluate the impact of iStent
inject
compared with iStent
inject
combined with cataract surgery in terms of effectiveness as measured by QALY, the number of blind eyes,and costs. It is particularly suited to model chronic diseases such as POAG. The Markov model allows the synthesis of data from various sources and extrapolation from primary data sources over time. Sources of the model were credible as they were based on published literature and were completed and/or validated by experts.
我们这些学生的学习水准都很差劲儿,一问三不知是我们的家常便饭。如果市政府不组建这所学校,让这些少年散放到社会上——毫无疑问,我们当中得有很多人会成为少年犯。市政府正是基于这样的担心才成立了这所非驴非马的学校,把这些天性难驯的顽劣学生圈在这儿读书,让他们学习将来到社会上生存的手艺,成为自食其力的、无害的人。总之,这家学校不是培养国家的栋梁和大用之材的地方。
(6)应用与指导性。不同利益方出于各种应用的目的,以及了解在油田开发的不同阶段的储量资产状况,都要求进行油气储量评估。利益方有油气开发与经营者、投资者、权益拥有者、买卖方、政府管理机构、金融机构及监管机构等。但各利益方因所属业务范围不同,在应用及指导方面的着重点不尽相同。
DISCUSSION
According to the Japanese Glaucoma Society Guideline
, the current treatment of POAG in Japan usually begins with topical anti-glaucoma medications followed by laser treatments in case of failure. Incisional surgeries are typically reserved as last resort therapies. To date, no specific treatment pattern has been recommended based on the severity while new therapeutic options have been developed. Their introduction to clinical practice have addressed and diminished burden associated with traditional glaucoma treatments which include non-adherence,low persistence
, contraindications and intolerable AEs following anti-glaucoma medications; unsustainability of IOP reduction following laser treatment; and higher risks of lifelong complications and failures following incisional surgery in patients with mild-to-moderate POAG. iStent trabecular micro-bypass stent system introduced surgeons to the first micro-invasive glaucoma surgery (MIGS) offering a safe and effective, tissue-sparing, minimally traumatic approach to treat mild-to-moderate open angle glaucoma (OAG) without compromising vision acuity. iStent
inject
is the 2
generation MIGS device marketed by Glaukos in 2018. It is based on the same fluidic method of action as the 1
iStent
but preloaded with 2 stents where aqueous humour outflow is improved,thereby lowering IOP and possibly decreasing the dependence on pressure-lowering topical medications
. The iStent
inject
is indicated for patients undergoing treatment with IOP-lowering drugs for mild-to-moderate POAG, including those with normal-tension glaucoma, and used in conjunction with cataract surgery
. In the 2-year iStent
inject
pivotal randomised controlled trial (RCT) in patients with mild-tomoderate POAG undergoing cataract surgery
, the stents were found to be effective in lowering IOP. Furthermore, mean medication use was statistically significantly lower in the iStent
inject
with cataract surgery cohort
the cataract surgery only cohort. As the cost-utility of iStent
inject
has not previously been evaluated in Japan, we aimed to conduct a cost-utility analysis based on Japanese data. The objective of this analysis was to evaluate the cost-utility of iStent
inject
in combination with cataract surgery
cataract surgery alone in patients with mild-to-moderate POAG in the Japanese setting, from a public payer’s perspective.
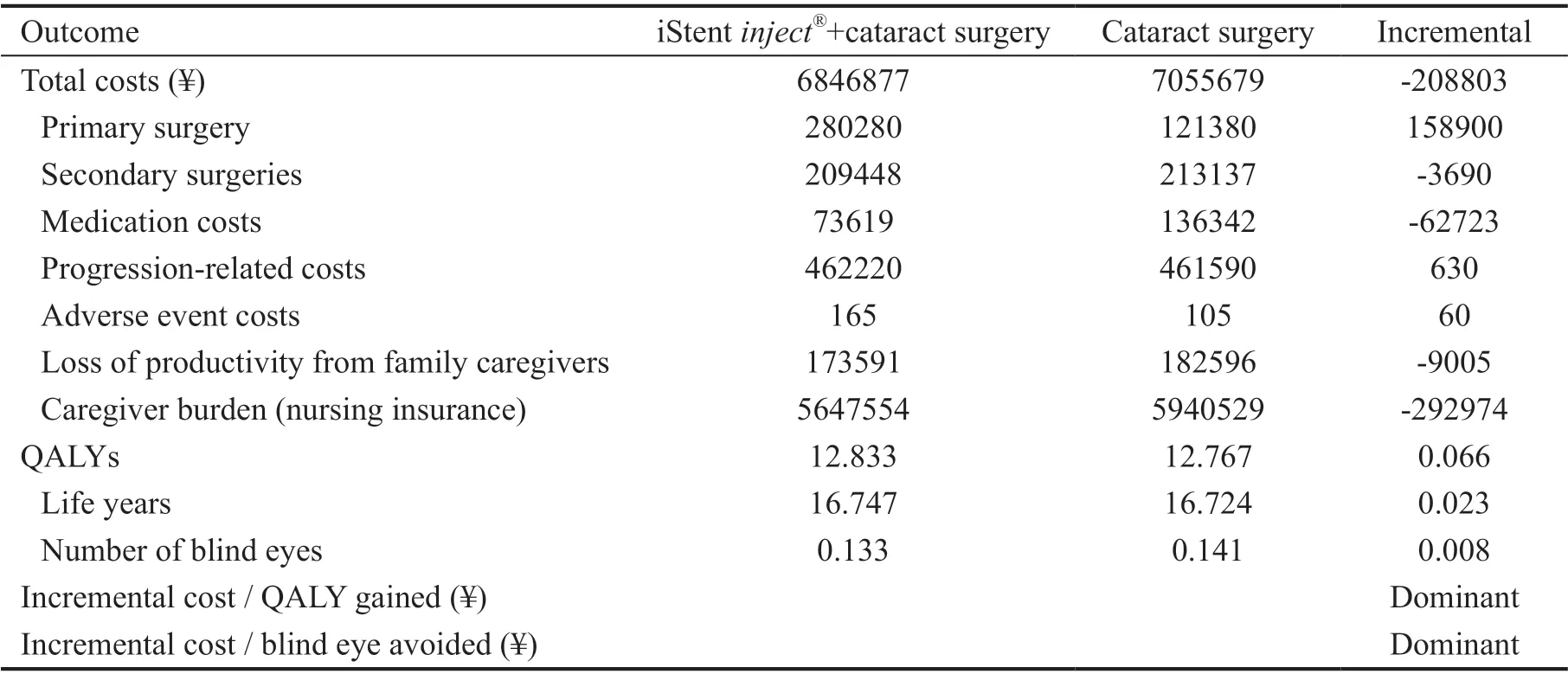
Based on scenario analysis from the societal perspective, iStent
inject
with cataract surgery strategy was found to dominate cataract surgery alone strategy,with a cost saving of -¥208 803, increased number of QALY gained of 0.066, and 0.008 blind eyes avoided. The results of scenario analyses are presented in Table 3.
The interpretation of study results should consider the following limitations. First, due to limited data available for the progression of glaucoma severity and the impact of trabecular micro-bypass surgery (TBS) device, we simulated the disease progression indirectly through the IOP level and the IOP reduction by the medical device. Future models should incorporate long-term evidence on the effect of these medical devices on slowing the progression of glaucoma. Second,the relationship between IOP level and glaucoma severity progression was derived from an international study, as there are no Japanese data available. However, the data were validated by Japanese clinical experts, who confirmed that it could represent the case in Japan. Third, a constant rate of a natural decline in VF for all patients, regardless of glaucoma severity, was applied. This was a conservative assumption as an application of higher rates of the natural decline in VF for patients with moderate and advanced glaucoma would improve the cost-utility of TBS devices. And finally, assumptions were made for long-term IOP reductions by treatments because long-term IOP reduction data were not available in the literature at the time of this study. There were 2-year data available for TBS devices: a 1.2% decline in IOP reduction in the 2
year (8.3) compared with the previous year (8.4)
. Yet,in the present analysis, conservative assumptions were applied:5% decline in the efficacy on IOP reduction compared with the previous year and no efficacy after 10y.
Long-term follow-up of patients who underwent an iStent
inject
implantation is needed to measure the change in VF loss, IOP reduction, and medication reduction. Existing modelling methods depend on assumptions for extrapolation as well as mapping of an IOP reduction to the progression of glaucoma severity. No evidence on healthcare resource utilisation by glaucoma health states is available for Japanese patients. The estimates of resource use were collected from expert opinions. Changes may have occurred in treatment practice due to the introduction of other treatment options.Updated resource use estimates related to the extent of VF loss or glaucoma severity are of need for future economic modelling purposes. The impact of medication nonadherence in patients who underwent iStent
inject
implantation has not been examined in the literature either. A real-world observational study may provide valuable insights into the change in risk of glaucoma progression due to nonadherence in patients who underwent iStent
inject
implantation.
In conclusion, the iStent
inject
with cataract surgery is a costeffective strategy over cataract surgery alone from the payer’s perspective and cost-saving from the societal perspective in patients with mild-to-moderate POAG in Japan.
The authors thank Glaukos Corporation for funding the study.The authors also thank Małgorzata Biernikiewicz of Creativ-Ceutical, Krakόw, Poland for providing medical writing support in accordance with Good Publication Practice (GPP3)guidelines (http://www.ismpp.org/gpp3).
Igarashi A, Ishida K, Shoji N, Chu A, and Falvey H conceived the research and designed the analyses; Han R, Ueyama M and Onishi Y acquired the data and Han R, and Ueyama M performed the analyses; all authors participated in the interpretation of the data; All authors wrote the manuscript, participated in its revisions, read and approved the final manuscript.
手足部位是人体负重、劳动的重要器官,常因烧伤、意外事故、手术等造成皮肤软组织缺损,且发生率高[1-2],由于其功能重要,对修复要求高。全厚皮片移植术是一种最常用的修复方法,相比于韧厚或中厚皮片修复,耐磨且不易增生瘢痕,相比于皮瓣移植修复,难度小,无臃肿影响外观情况。由于全厚皮较厚,创基血运各不相同,常常导致皮片成活不理想,影响预后。为达到手术后皮片存活的最佳效果,2012年9月至2016年8月,笔者在全厚皮移植后常规治疗的基础上采用高压氧综合治疗。现报道如下。
and
received consultant fees for their roles in study design,interpretation of results and review of the manuscript;
also reports grants and other from Gilead Sciences KK.,grants from Intuitive Surgical GK., grants from Boston Scientific Japan Inc., grants and personal fees from Pfizer Japan Inc., grants from Beckton Dickinson and Company, grants from Milliman Inc., personal fees and other from Terumo corporation, personal fees from Chugai Pharmaceuticals Inc.,personal fees from Astellas Pharma Inc., other from Fuji film Inc., other from CSL Behring Japan Inc., personal fees from Sanofi Japan Inc., personal fees and other from Takeda Pharmaceutical Inc., personal fees from Nippon Boeringer Ingelheim Inc., personal fees from Ono pharmaceutical Inc.,personal fees from Taiho pharmaceutical Co. Ltd., personal fees from Eisai Inc., personal fees from Abbvie GK, personal fees from Sumitomo Dainippon Pharma Inc., personal fees from Ayumi Pharmaceutical Inc., personal fees from Medilead Inc., personal fees from Novo Nordisk Japan Inc., personal fees from Novartis Pharma Inc., personal fees from GSK Inc.,outside the submitted work.
also received consulting fees from Seikagaku Corporation;
and
are employees of Glaukos and stockholders of Glaukos;
,
and
are employees of Creativ-Ceutical.
1 Yamada M, Hiratsuka Y, Roberts CB, Pezzullo ML, Yates K, Takano S, Miyake K, Taylor HR. Prevalence of visual impairment in the adult Japanese population by cause and severity and future projections.
2010;17(1):50-57.
2 Morizane Y, Morimoto N, Fujiwara A, Kawasaki R, Yamashita H, Ogura Y, Shiraga F. Incidence and causes of visual impairment in Japan:the first nation-wide complete enumeration survey of newly certified visually impaired individuals.
2019;63(1):26-33.
3 Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, Kuwayama Y, Mishima HK, Shimizu H, Tomita G, Inoue Y, Kitazawa Y, Tajimi Study Group JGS. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study.
2004;111(9):1641-1648.
4 Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis.
2014;121(11):2081-2090.
5 Yamamoto T, Iwase A, Araie M, Suzuki Y, Abe H, Shirato S, Kuwayama Y, Mishima HK, Shimizu H, Tomita G, Inoue Y, Kitazawa Y, Tajimi Study Group JGS. The Tajimi Study report 2: prevalence of primary angle closure and secondary glaucoma in a Japanese population.
2005;112(10):1661-1669.
6 Quigley HA. Glaucoma.
2011;377(9774):1367-1377.
7 SPECIAL ISSUE : The Japan Glaucoma Society Guidelines for Glaucoma (4th Edition).
2018;122(1):5-53.
8 Chang CP, Hodapp EA. Risk Factors in glaucomatous progression,2015. https://glaucomatoday.com/articles/2015-sept-oct/risk-factors-inglaucomatous-progression
9 Canadian Ophthalmological Society Glaucoma Clinical Practice Guideline Expert Committee, Canadian Ophthalmological Society.Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of glaucoma in the adult eye.
2009;44(Suppl 1):S7-S93.
10 Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M, Group EMGT. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial.
2002;120(10):1268-1279.
11 Vizzeri G, Weinreb RN. Cataract surgery and glaucoma.
2010;21(1):20-24.
12 Nelson P, Aspinall P, Papasouliotis O, Worton B, O’Brien C. Quality of life in glaucoma and its relationship with visual function.
2003;12(2):139-150.
13 Kashiwagi K, Furuya T. Persistence with topical glaucoma therapy among newly diagnosed Japanese patients.
2014;58(1):68-74.
14 Kashiwagi K, Chono E, Koesters S, Yap PS. Persistence and treatment patterns of fixed combination drugs for glaucoma: a retrospective claims database study in Japan.
2020;20(1):223.
15 Corporation G. Glaukos Corporation 2017 Investor Day. 2017.
16 Intraocular Drainage for Cataract Surgery Conference. Requirements for the Use of Intraocular Drains in Cataract Surgery (2nd Edition).
2016;120(7):494-497.
17 Samuelson TW, Sarkisian SR Jr, Lubeck DM, Stiles MC, Duh YJ,Romo EA, Giamporcaro JE, Hornbeak DM, Katz LJ. Prospective,randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract:two-year results.
2019;126(6):811-821.
18 Patel V, Ahmed I, Podbielski D, Falvey H, Murray J, Goeree R. Costeffectiveness analysis of standalone trabecular micro-bypass stents in patients with mild-to-moderate open-angle glaucoma in Canada.
2019;22(4):390-401.
19 Shiroiwa T, Fukuda T, Ikeda S, Takura T, Moriwaki K. Development of an official guideline for the economic evaluation of drugs/medical devices in Japan.
2017;20(3):372-378.
20 Ahmed IIK, Podbielski DW, Patel V, Falvey H, Murray J, Botteman M,Goeree R. A Canadian cost-utility analysis of 2 trabecular microbypass stents at time of cataract surgery in patients with mild to moderate open-angle glaucoma.
2020;3(2):103-113.
21 Mills RP, Budenz DL, Lee PP, Noecker RJ, Walt JG, Siegartel LR,Evans SJ, Doyle JJ. Categorizing the stage of glaucoma from prediagnosis to end-stage disease.
2006;141(1):24-30.
22 Ono T, Yuki K, Asaoka R, Kouyama K, Abe T, Tanabe S, Fukagawa K, Uchino M, Shimoyama M, Ozawa Y, Ozeki N, Shiba D, Tsubota K.Glaucomatous visual field defect severity and the prevalence of motor vehicle collisions in Japanese: a hospital/clinic-based cross-sectional study.
2015;2015:497067.
23 Leske MC, Heijl A, Hussein M,
. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial.
2003;121(1):48-56.
24 Wang JJ, Mitchell P, Simpson JM, Cumming RG, Smith W. Visual impairment, age-related cataract, and mortality.
2001;119(8):1186-1190.
25 van Gestel A, Schouten JSAG, Beckers HJM, Severens JL, Hendrikse F, Webers CAB. The long term effectiveness and cost-effectiveness of initiating treatment for ocular hypertension.
2014;92(6):513-523.
26 Nieland K, Labbé A, Schweitzer C, Gicquel G, Kleintjens J, Ostawal A, Treur M, Falvey H. A cost-effectiveness analysis of iStent inject combined with phacoemulsification cataract surgery in patients with mild-to-moderate open-angle glaucoma in France.
2021;16(6):e0252130.
27 van Gestel A, Webers CA, Severens JL, Beckers HJ, Jansonius NM, Hendrikse F, Schouten JS. The long-term outcomes of four alternative treatment strategies for primary open-angle glaucoma.
2012;90(1):20-31.
28 Ministry of Health, Labour and Welfare. Various information on medical fees, April 2020. https://shinryohoshu.mhlw.go.jp/shinryohoshu/kaitei/doKaiteiR02;jsessionid=5C49509B945B58423A7 9A5DAD7640FBB
29 Inoue K. Characteristics and segregation of each glaucoma combination ophthalmic drug.
2018;60(12):1491-1495.
30 Ministry of Health, Labour and Welfare. Drug Master Search, April 2021. https://www.mhlw.go.jp/topics/2021/04/tp20210401-01.html
31 Ministry of Health, Labour and Welfare. Labor statistics, 2019. https://www.mhlw.go.jp/toukei/itiran/roudou/chingin/kouzou/z2019/dl/01.pdf
32 Ministry of Health, Labour and Welfare. Long-term care insurance statistics. Survey of Long-term Care Benefit Expenditures, May 2020.
33 Hasegawa M, Komoto S, Shiroiwa T, Fukuda T. Formal implementation of cost-effectiveness evaluations in Japan: a unique health technology assessment system.
2020;23(1):43-51.
34 Teus MA, Belda JI, Lavín C, Garcà a-Feijoà J, Falvey H, Buseghin G, Soler M, Appierto M. Cost-effectiveness analysis of iStent
inject
implantation during cataract surgery compared to cataract surgery alone for mild to moderate open-angle glaucoma patients in Spain.
2021:1-10.
35 Bartelt-Hofer J, Flessa S. Comparative efficacy and cost-utility of combined cataract and minimally invasive glaucoma surgery in primary open-angle glaucoma.
2020;40(6):1469-1479.
猜你喜欢
工会博览(2022年33期)2023-01-12 08:53:02
实用手外科杂志(2022年2期)2022-08-31 09:48:08
出版人(2022年2期)2022-02-26 08:13:42
——栽培注意事项
新农村(浙江)(2021年10期)2021-10-18 02:53:44
新农村(浙江)(2021年10期)2021-10-18 02:53:42
Zoological Research(2019年6期)2019-10-31 10:51:06
青年歌声(2019年4期)2019-04-11 08:35:02
现代装饰(2017年9期)2017-05-25 02:00:08
中亚信息(2016年3期)2016-12-01 06:08:24
食品工业科技(2014年11期)2014-03-11 18:16:28
 International Journal of Ophthalmology2022年6期
International Journal of Ophthalmology2022年6期
- International Journal of Ophthalmology的其它文章
- Intraocular lens removal or not during vitrectomy for acute infectious endophthalmitis after cataract surgery
- Vitreous function and intervention of it with vitrectomy and other modalities
- Short-term outcomes of mitomycin C-augmented excisional bleb revision with capsulectomy for failed Ahmed glaucoma valve
- Evaluation of nintedanib as a new postoperative antiscarring agent in experimental extraocular muscle surgery
- Multimodal imaging of experimental choroidal neovascularization
- A novel Nance-Horan syndrome mutation identified by next-generation sequencing in a Chinese family