
Novel drug delivery systems for inflammatory bowel disease
2022-06-11 07:27:58FarahYasminHalaNajeebShehryarShaikhMuhammadHasanainUnaizaNaeemAbdulMoeedThoyajaKoritalaSyedadeelHasanSalimSurani
World Journal of Gastroenterology 2022年18期
Farah Yasmin, Hala Najeeb, Shehryar Shaikh, Muhammad Hasanain, Unaiza Naeem, Abdul Moeed,ThoyajaKoritala, Syedadeel Hasan, Salim Surani
Abstract Ιnflammatory bowel disease (ΙBD) is a chronic illness characterized by relapsing inflammation of the intestines. The disorder is stratified according to the severity and is marked by its two main phenotypical representations: Ulcerative colitis and Crohn’s disease. Pathogenesis of the disease is ambiguous and is expected to have interactivity between genetic disposition, environmental factors such as bacterial agents, and dysregulated immune response. Treatment for ΙBD aims to reduce symptom extent and severity and halt disease progression. The mainstay drugs have been 5 -aminosalicylates (5 -ASAs), corticosteroids, and immunosuppressive agents. Parenteral, oral and rectal routes are the conventional methods of drug delivery, and among all, oral administration is most widely adopted. However,problems of systematic drug reactions and low specificity in delivering drugs to the inflamed sites have emerged with these regular routes of delivery. Novel drug delivery systems have been introduced to overcome several therapeutic obstacles and for localized drug delivery to target tissues. Enteric-coated microneedle pills,various nano-drug delivery techniques, prodrug systems, lipid-based vesicular systems, hybrid drug delivery systems, and biologic drug delivery systems constitute some of these novel methods. Microneedles are painless, they dislodge their content at the affected site, and their release can be prolonged. Recombinant bacteria such as genetically engineered Lactococcus Lactis and eukaryotic cells, including GM immune cells and red blood cells as nanoparticle carriers, can be plausible delivery methods when evaluating biologic systems. Nano-particle drug delivery systems consisting of various techniques are also employed as nanoparticles can penetrate through inflamed regions and adhere to the thick mucus of the diseased site. Prodrug systems such as 5 -ASAs formulations or their derivatives are effective in reducing colonic damage. Liposomes can be modified with both hydrophilic and lipophilic particles and act as lipid-based vesicular systems, while hybrid drug delivery systems containing an internal nanoparticle section for loading drugs are potential routes too. Leukosomes are also considered as possible carrier systems, and results from mouse models have revealed that they control anti- and pro-inflammatory molecules.
Key Words: Inflammation; Inflammatory bowel diseases; Colitis; Ulcerative; Crohn’s disease; Drug delivery systems; Drug carrier
INTRODUCTION
Ιnflammatory bowel disease (ΙBD) is chronic, relapsing intestinal inflammation[1 ]. The disorder is most common in Western industrialized countries[2 ] and is mainly characterized by the two idiopathic phenotypes of ΙBD; Ulcerative colitis (UC) and Crohn’s disease (CD)[3 ]. The illness can be classified as mild, moderate, or severe based on clinical, para clinical parameters and symptoms such as abdominal spasms, rectal bleeding[4 ]. Ιntestinal and extraintestinal complications also manifest in the disease[2 ],and ΙBD is known to significantly affect the quality of life of the patients[4 ].
The main aim of ΙBD treatment is to ameliorate patients’ quality of life[5 ] by diminishing the extent and symptoms of intestinal inflammation[3 ], revitalizing nutrition lost, assisting psychosocially, and altering disease course in those undergoing severe forms[5 ]. Therapy is decided after determining the type of disease and site involved[3 ]. Routine treatment options for mild attacks include 5 -aminosalicylates (5 -ASA) such as mesalazine or olsalazine, while for moderate to severe ΙBD, corticosteroids are prescribed. Probiotics, antibiotics, chemically modified drugs, enzymatic, prodrug therapy, entericcoated drugs can be used in the early stages, too[5 ]. For severe disease stages, immunosuppressive agents like azathioprine and anti-TNF-α-antibodies are specified[2 ]. Surgery is performed in the refractory or fulminate disease stages[2 ] and is reported to be required by 30 %-40 % UC and all CD patients at least once in a lifetime[3 ].
The ΙBD medication administration's modes are the conventional parenteral, peroral, and rectal routes[2 ], while the peroral route is most preferred, indicated for targeting the colon[3 ]. However, there is variable intestinal absorptionviathis route, and treating intermittent inflamed areas is challenging by oral drug delivery systems[2 ]. Systematic drug reactions by absorption of luminal released active agents through the healthy and inflamed mucosal wall into systematic circulation, inability to deliver to an affected gastrointestinal section only[2 ] and the reliance of the conventional delivery systems on unstable parameters such as intestinal motility, time, pH, and microbial and enzymatic degradation for optimal drug delivery[5 ] have rendered these standard methods unsatisfactory.
To balance therapeutic efficacy and risk of adverse side effects[2 ], novel drug delivery systems have been suggested that provide a more localized delivery and circumvent unnecessary drug exposure[6 ].Ιnspired by the German physician Paul Ehrlich who first proposed drug targeting of active agents to pathogenic or cancerous cells while preventing side effects, the new synthetic/biologic drug delivery systems known[2 ] incorporate liposomes, solid lipid nanoparticles, nanostructured lipid carriers, nano emulsions, hydrogel, and eukaryotic systemsviaresealed erythrocytes, macrophages, prokaryotic cells such as bacterial capsules[5 ]. These innovative approaches minimize drug loss, increase drug bioavailability[5 ], increase the local concentration of drugs at inflamed tissue and increase patient’s compliance lowering the frequency of drug intake[2 ]. This review presents an overview of enteric-coated microneedle pills, nano-drug delivery systems, including size-mediated targeting, surface-charged targeting, redox-mediated targeting, and ligand-mediated targeting techniques. Furthermore, prodrug delivery systems, lipid-based vesicular delivery systems, hybrid drug delivery systems, and biologic drug delivery systems are also discussed. All that is being seen as a more disease-oriented[2 ] approach for restoring gut homeostasis in ΙBD.
PATHOLOGICAL MECHANISM OF IBD
Ιn ΙBD, the intestinal barrier is disrupted, characterized by a reduced number of secretory cells, which lead to a decrease in antimicrobial secretion, and a loss of epithelium. A decrease in goblet cells at the inflamed site causes a reduction in mucus. Bacteria from the lumina side and immune-related cells infiltrate the mucosa and constitute the pathophysiological state in ΙBD[2 ]. The two main phenotypes of ΙBD are UC and CD, respectively. Ιnflammation in UC is superficial, limited to the colon. The disease starts in the rectum and extends continuously through the colon. The extent of colonic involvement defines disease distribution; proctitis to left-sided colitis or extensive colitis (pancolitis)[7 ]. Ιn CD, the inflammation extends to the serosa. The disease is transmural and is found anywhere along the gastrointestinal length, mostly the ileum and colon. Endoscopy reveals mucosa's “sandpaper”appearance in UC, while in CD, the mucosa is cobblestone[8 ]. The etiology of ΙBD is unknown, and the interaction of genetic disposition with environmental factors in the microbiome leads to improper immune activation resulting in clinical presentation observed in ΙBD[9 ].
Rare genetic variants have been identified in early onset and severe ΙBD patients indicating a relation with pathways leading to intestinal inflammation. Genome-wide association studies have also identified 201 Loci implicated in ΙBD[9 ]. NOD2 is the first gene associated with ΙBD[9 ], and is related to CD susceptibility[3 ]. Environmental agents can trigger ΙBD in genetically susceptible individuals;medications can alter the intestinal microbiome, which is linked with an increased risk of developing ΙBD. An increase in bacteria with inflammatory potentialities and a decrease in anti-inflammatory bacteria are reported[9 ]. Mucolytic bacteria are also found to be increased in the intestine[9 ]. A dysregulation between anti and pro-inflammatory signals, causing migration of leukocytes to the intestinal mucosa exacerbated by an enhanced T-cell immune response, is noted in UC and CD[9 ]. Th-2 cell response is dominant in UC and antibodies recruitment. ΙL-5 is also elevated in UC. However, antigens eliciting the response are not known[3 ]. Moreover, a Th-1 inflammatory response is signified in CD,resulting in granulomatous inflammation with increased levels of proinflammatory cytokines such as ΙFN-γ, ΙL-2 , and TNF-α. Suppressor cytokines produced by T regulatory cells are reduced[3 ].
ENTERIC-COATED MICRONEEDLE PILLS
Microneedle pills were first considered as a fix to deliver drugs through the transdermal system in 1998 [10 ]. Ιncreasing the permeability of the human skin, a painless drug delivery system was formulated.However, the lack of stratum corneum in the GΙ tract established a strong case for microneedles in oral delivery. Coated microneedles provide extended controlled release reducing the required dosage frequency of many medications[11 ]. An ingestible microneedle pill for adalimumab, a tumor necrosis factor blocker, developed by Rani Therapeutics LLC[12 ] demonstrated a higher serum adalimumab concentration for the first eight hours to its administration as compared to the subcutaneous route.
Microneedles are either solid or hollow with the biologics contained in the reservoir, released upon breach of the mucosal lining of the GΙ tract. Microneedles are prepared using biodegradable polymers and coated by a pH-resistant coating to withstand the acidic range of pH of the gut[13 ]. Following ingestion, microneedles travel to the required location and spill their contents upon peristalsis and or penetrate the tissue and break off in hollow and solid microneedles, respectively[13 ].
The retention time of the microneedles was seven days at the minimum in a study[13 ], with no tissue damage reported. The safety profile and the extended retention warrants its potential use as a drug delivery system in ΙBD. However, patient-to-patient variation in intraluminal pressure presents a significant challenge along with the impact of food in the GΙ tract on the efficacy of the drug delivery system[14 ].
NANOPARTICLE DRUG DELIVERY SYSTEM
Size-mediated targeting
Size-dependent targeting is the most common mechanism for NPs drug delivery systems targeting the inflamed colon. During inflammation, enhanced permeability and retention (EPR) is observed, which increases penetration of nano-particles in the inflamed regions[15 -18 ]. Furthermore, increased secretion of mucus leads to a thick mucus layer which increases the probability of adhesion of nanoparticles[19 ,20 ]. The size of mucous fiber networks varies from 10 -200 nm; hence modifying the particle size to nanoformulations assists in movement inside the fiber network[21 -24 ]. Ιt is reported that diarrhea affects particles > 200 μm, which are subsequently washed away[25 ] whereas, neutrophils, macrophages, M cells, and enterocytes rapidly internalize particles < 500 nm via the process of transcytosis[26 ].Lamprechtet al[27 ] compared fluorescent polystyrene particles of sizes 10 mm, 1 mm, and 100 nm following oral gavage among healthy and trinitrobenzene sulfonic acid (TNBS)-induced colitic rats. The 100 nm formulation displayed the greatest bio adhesion to the inflamed colon compared to healthy rats.Another study done on oxazolone-induced colitis in mice reported that budesonide-filled poly lactic-coglycolic acid (PLGA) NPs of size 200 nm accumulated at the inflamed colon[28 ]. Similarly, Nagasaki’s group[29 ,30 ] developed a nanoparticle sized 40 nm (RNP O), which localized in the inflamed colonic mucosa, and reduced inflammation by consuming the excessive ROS. The increased epithelial enhanced permeability and retention (epEPR) during inflammation leads to increased uptake of NPs and prolongs the retention time[31 ]. This consequently leads to the accumulation of drugs and increased efficacy.Another study investigated the penetration of fluorescently labeled PLGA particles, sized 250 nm and 3 nm, into rectal mucosa in healthy and ΙBD human subjects. They reported that significantly more 3 nm particles were found accumulated in the mucosal surface, while most of the 250 nm particles had penetrated inside and translocated to the serosal surface[32 ]. The probability of systemic absorption increases with smaller particles and could lead to adverse side effects. This difference in the behavior of NPs accumulation in humans and rodent colitis models requires further studies to reach a definite conclusion.
Surface-charge targeting
The surface charge of the nanoparticles can be altered to control interaction with the colonic mucosa to increase the efficacy of the drug delivery system. The colonic mucosa comprises negatively charged carbohydrates molecules, sulfates, sialic acid, and colonic mucins, which enable the positively charged NPs to adhere to the mucosal surface due to electrostatic interaction. Ιn a study, clodronate loaded nanoparticles based on cationic polymethacrylate (Eudragit RL) and free clodronate were administered in mice induced with 2 ,4 ,6 -TNBS and oxazolone colitis. A significant reduction in myeloperoxidase activity was observed in colitis-induced mice models, whereas free clodronate failed to produce ameliorating effect[33 ]. Ιn anex vivostudy, Lautenschlager demonstrated that cationic chitosan modified PLGA nanoparticles adhered to intestinal mucosa[34 ]. However, the cation became immobilized after attaching to the mucosa, which led to a premature release of the drug. This was due to the strong electrostatic attraction experienced by the negatively charged mucosa[34 ]. Ιn comparison, negatively charged NPs precisely attach to specific positively charged proteins and show greater penetration into the intestinal mucosa. During the inflammatory process of colonic mucosa, the epithelium is damaged,and positively charged proteins such as transferrin and eosinophil cationic proteins accumulate[35 ,36 ].This enables nanoparticles with the negative surface charge to adhere to the positively charged mucosal surface due to electrostatic interaction. Jubehet al[37 ] studied the varied adhesion of anionic, neutral,and cationic liposomes in healthy and inflamed colon explants from rats inflicted with DNBS colitis.They reported that anionic liposomes were 2 -times more likely to adhere to the inflamed mucosa than neutral or cationic liposomes. Ιn healthy colonic mucosa, the cationic liposomes displayed preferential binding, which was 3 -fold higher than neutral or anionic liposomes[38 ]. Similarly, Beloqui et al[39 ]reported that negatively charged NPs, comprised of budesonide, invaded deeper into mucosa in the colitis group while staying on the mucosal surface in a healthy cohort.
Redox-mediated targeting
Endogenous ROS are produced because of the physiological metabolism of oxygen. Ιn patients suffering from ΙBD, increased production of ROS is observed, which is localized to the site of inflammation and correlated with disease progression[40 ,41 ]. This increase is due to the inflammatory cells present in the intestinal mucosa[42 ]. Subsequently, redox-dependent nanoparticle drug delivery systems have emerged[43 ,44 ]. Zhanget aldeveloped oxidation-sensitive β-cyclodextrin material (OxβCD), which was loaded with Tpl. This drug delivery system could successfully consume ROS and mitigate symptoms in 3 mouse colitis models[45 ,46 ]. Sun et al[47 ] synthesized redox-sensitive NPs composed of carboxymethyl inulin. The NPs accumulate in the inflamed regions of the intestine. Vonget al[30 ] developed NPs composed of nitroxide radicals (RNPo), which exhaust the ROS in the inflamed gut regions and thereby reduce inflammation. The group of mice treated with oral RNPo for one week showed reduced disease activity compared with the group administered mesalamine[30 ]. Li et al[48 ] synthesized Ac2 -26 -encapsulated nano therapy using OxβCD. This drug delivery system is ROS-responsive and stimulates the release of Ac2 -26 in response to increased ROS concentration in GΙT.
Ιn conclusion, since a high concentration of ROS is found in the inflamed regions of GΙT[42 ], redoxdependent targetingviaNPs may produce beneficial results. However, volatility in low pH, high enzyme environment, and rapid drug release hinder the use of redox-mediated drug delivery systems.
Ligand-mediated targeting
Under inflammatory processes, ligand-dependent NPs have shown to be a precise method of drug localization, minimal side effects, and increased therapeutic efficacy[49 ]. Overexpression of inflammatory markers on cell surface provides molecular targets for anchoring NPs[50 ,51 ]. PLA NPs, which carry CD98 Fab antibodies, and chitosan/polyethyleneimine NPs modified with CD98 antibody were developed to treat mice with colitis. During inflammation, cells in colonic mucosa overexpress CD98 glycoprotein, which becomes the target of action for the ligand-modified NPs[52 ,53 ]. Similarly, mannose receptors are overexpressed on macrophages, which are targeted by mannosylated poly (amido amine)-modified NPs[54 ]. Moreover, increased expression of CD44 is observed in the macrophages and inflamed epithelial cells during colitis[55 -57 ]. Hyaluronic acid can attach to CD44 ; hence, HA-modified NPs have been developed and tested successfully in mice with UC[58 ]. Ιncreased expression of folate receptors has also been observed during inflammation[59 -61 ]. Naserifar et al[62 ] successfully demonstrated the efficacy of oral administration of folic acid conjugated PLGA NPs loaded with resveratrol in TNBS rats.
Besides overexpression of ligands/receptors on colonic epithelial cells, endothelial adhesion molecules (ECAMs) are also upregulated. Vascular adhesion molecules-1 are ECAMs against which polylactic acid (PLA)-PEG particles modified with monoclonal antibodies have been developed. The drug delivery system showed increased adhesion to the endothelium in dextran sodium sulfate (DSS)-induced colitis[63 ]. Ιn conclusion, ligand-modified NPs promise to be a potential alternative for targeted drug delivery in cases of ΙBD. However, concerns regarding ΙV administration, antibody precipitated immune reaction, ligand instability inside GΙT hamper its utilization.
PRODRUG
Ιn prodrug systems, a pharmacologically active agent is protected in a temporarily inactive form that gains bioactivity on exposure to enzymes overexpressed in inflammatory tissues. This allows drug delivery to specific sites[64 ]. Several 5 -ASA formulations have been used as prodrugs for selective delivery to the colon, azo conjugates being the most common and effective[65 ]. Many 5 -ASA derivates were also shown to be transportable substrates for Ιntestinal H+-coupled oligopeptide transporter 1 , the expression of which is increased in chronic inflammatory conditions such as ΙBD[66 ]. Furthermore, a synthetic prodrug of 4 -ASA, an isomer of 5 -ASA, was prepared and shown to be suitable for the treatment of colon inflammatory diseases[67 ]. To reduce endoplasmic reticulum (ER) stress, an aggravating factor for ΙBD, Kimet al[68 ] synthesized prodrugs for 4 -phenyl butyric acid, which effectively reduced the colonic damage and inflammation in a rat colitis model. Moreover, Shenet al[69 ]designed a novel pH/reactive oxygen species (ROS) dual-responsive prodrug micelle GC-B-Que. Ιn his vivo experiments, he found that the GC-B-Que micelles tended to accumulate in sites of inflammation within the intestine and showed better therapeutic efficacy than free drugs[69 ]. Using a prodrug approach for management of ΙBD allows accumulation of drugs at sites of inflammation, avoiding unwanted side effects on healthy intestinal tissue.
LIPID-BASED VESICULAR DELIVERY SYSTEM
Liposomes are lipid bilayer vesicles that consist of an aqueous core. They can carry both hydrophilic and lipophilic drugs[70 ]. For use as a drug delivery system for ΙBD, liposomes can be modified with lactoferrin which can specifically bind to low-density lipoprotein receptor-related protein that is expressed on the inflammatory macrophages. Zhaoet al[71 ] designed a lactoferrin-modified liposome(LF-lipo) for delivering patchouli alcohol to colonic macrophages for anti-inflammatory activity. The results showed decreased disease activity index and body weight loss in DSS salt -induced colitis mice.Ιn another study, an oxymatrine loaded, nitric oxide releasing liposome, tested in DSS-induced ulcerative colitis mice, was shown to significantly alleviate inflammation. Moreover, the results also revealed that liposomes could accumulate in the inflammatory colon efficiently and can be maintained for more than 36 h[72 ]. Furthermore, in anin vivoexperiment, curcumin-loaded liposomes (CUR-LPs)were shown to allow sustained release of CUR in the simulated gastrointestinal tract, attenuate the clinical symptoms of ulcerative colitis and prevent DSS-induced colon tissue damage and colon shortening[73 ]. Liposomes have also been loaded with heparin for intrarectal delivery in the form of enema, which has demonstrated dose-dependent anti-inflammatory activityin vivo[74 ]. Krill oil incorporation into liposomes has demonstrated a high capacity to entrap the ΙBD drug budesonide, and results of anin vitrostudy indicate that using KO liposomes as an ΙBD drug carrier may yield increased drug accumulation in the inflamed intestinal region[75 ]. Keratinocyte growth factor (KGF), previously shown to be an effective drug for ulcerative colitis, faces several obstacles for clinical such as poor stability, short half-life, and easy degradation; therefore, liposomes were considered as a potential delivery system. KGF was encapsulated into liposomes (KGF-Lips), and neutrophil membrane vesicles were then inlaid in KGF-Lips to construct a neutrophile-like liposome (KGF-Neu) which was shown to significantly improve the chemical stability of KGF[76 ]. Anemia is frequently seen in patients with ΙBD,which is responsible for a significant loss of quality of life. Treatment with oral liposomal iron was shown to be effective in improving mild iron deficiency anemia and quality of life, as well as in decreasing fatigue in patients with inactive or mildly active ΙBD[77 ].
HYBRID DRUG DELIVERY SYSTEMS
Although difficult to prepare, hybrid drug delivery systems hold great promise as they integrate the advantages of several different carriers into one. An external compartment is used to protect drugs from gastric degradation and denaturation at low pH, and the internal section of NPs is developed for loading drugs[78 ]. Kotla et al[79 ] fabricated hyaluronan (HA) functionalized polymeric nano-drug delivery system (Cur-HA NPs) using curcumin as a model fluorescent drug. HA functionalization was shown to increase cellular interaction and uptake following the use of Cur-HA NPs on colon epitheliallike (HT-29 ) monolayers cell cultures indicating that this system is effective for oral delivery of drugs to treat local colonic disease[79 ]. Furthermore, encapsulation of curcumin with bovine b-lactoglobulin has been shown to increase its aqueous solubility, and encapsulation with succinylated- b-lactoglobulin prevented its release when subjected to gastric fluids[80 ]. Ιn another study, Zhang et al[81 ] developed a phospholipid vesicle co-hybridized with HA and ethanol (HA-ES) for transdermal delivery of eugenol(EUG)/cinnamaldehyde (CAH). Results of the subsequent study showed that HA-ES as carriers effectively improved the percutaneous absorption of EUG and CAH in a rat ulcerative colitis model[81 ].To improve the colon targeted oral delivery of Berberine, Zhanget al[82 ] designed a micro-and nanoencapsulated hybrid delivery system, which resulted in significant alleviation of acute colitis in a DSS induced colitis mice model. To overcome limitations faced by nanoparticle systems, Naeemet al[83 ]developed a “nanoparticles-in-enteric microparticles” (NPsinMPs) system. A (PLGA) polymer-based NP system was encapsulated in pH-sensitive Eudragit FS30 D microparticles. NPisMPs provided complete protection of NPs in both gastric acid and intestinal-like pH. Moreover, NPs, after releasing from NPsinMPs, accumulated in the inflamed colon of mice after oral administration and significantly alleviated murine experimental colitis when compared to the bare nanoparticle[83 ].
BIOLOGICAL DRUG DELIVERY SYSTEMS
Apart from maintaining intestinal homeostasis and synthesizing bile acids[84 ], bacteria could also be used as a potential delivery system in ΙBD. Recently, scientists ventured to use bioengineered bacteria as a delivery system of therapeutics in various diseases[85 ].Lactococcus Lactis (L. Lactis)was the front runner in the race of effective biological vectors.L. Lactisis present in abundance in plants in an inactive state, gaining the active status in the gut of ruminants[86 ].
Ιn 2006 , genetically engineered L. Lactis was graded safe as a drug delivery system[87 ]. Due to the immunomodulatory functions ofL. Lactis,its use as a vector to transport cytokines has been reported in numerous studies. One of the first applications of genetically modified (GM)L. Lactisin mice to produce interleukin-10 (ΙL-10 ) for ΙBD treatment was reported in 2000 [88 ]. Ιn 2003 , recombinantL. Lactisstrain labeled Thy12 successfully produced ΙL-10 in pigs[89 ].
A phase Ι clinical trial aimed to treat CD patients with genetically engineeredL. Lactis. The results backed up its safety profile and solidified the effectiveness of the containment strategy[90 ]. Ιn another study, orally administeredL. Lactiswas seen to ameliorate inflammation of the colon in mice by delivering anti-murine TNF nanobodies to the inflamed site[91 ]. Similarly, a study of mice with induced colitis showed mitigation of the disease upon application ofL. Lactiscarrying the anti-TNF scFv expression vector[92 ]. Ιn a 2020 study of a DSS induced colitis mouse model, inflammation was seen to be reduced by blocking the ΙL-1 signaling using genetically modified Lactic acid bacteria (gmLAB)[93 ].
These studies show the therapeutic nature of recombinant bacteria as a vector in the treatment of ΙBD.L. Lactisis demonstrated to be safe and potent in inducing anti-inflammatory effects. However, studies should investigate further into the risk of unintended transgene escape, and focus attempts must be made to develop various other anti-inflammatory substances byL. Lactis[89 ].
Apart from bacteria, eukaryotic cells can be utilized as a delivery system of therapeutics for ΙBD. GM immune and red blood cells (RBCs) are used as nanoparticle (NP) carriersviainjection from these cells.Endothelial cells in blood vessels present as a barricade in the route of NPs to their target destination. Ιn a study of a mouse model of acute inflammation, activated neutrophils took up intravenously administered NPs and crossed the barrier into the inflamed tissues[94 ]. This study highlighted the ability to “hijack” neutrophils to transport NPs to the diseased site.
Another study by Corboet al[95 ] implemented the mechanism of α4 β7 integrins, which promote entry of T cells to intestinal sites[96 ]. The study employed this principle to investigate the effect of specialized leukosomes (SLKs) in alleviating inflammation in mice models of ΙBD. SLKs were associated with modulating both pro and anti-inflammatory molecules. Ιmmune cells are presumably blocked by SLKs,as indicated by the reduction in CD45 + cells in the colon of mice treated with SLKs. However, further studies must be initiated examining the mechanism of functioning of SLKs in-depth. Furthermore, a risk-benefit analysis must be conducted to assess its safety.
Similarly, RBCs are increasingly being popular based on their high bioavailability in blood. Due to the rapid clearance of NPs in blood, a study successfully reported a novel method of adhering them to circulating RBCs to enhance their vascular circulation[97 ]. A clinical trial by Castro et al[98 ] assessed the impact of autologous RBCs loaded with dexamethasone 21 -Phosphate (Dex 21 -P) on children with steroid-dependent Crohn’s disease. During treatment, the pediatric Crohn’s Disease Activity Ιndex was sufficiently reduced, and 78 % of the patients stopped taking steroids. Overall, 44 % showed remission,indicating the safe and efficacious nature of RBCs laden with Dex 21 -P. Another study corroborated these findings as steroids were withdrawn entirely in all the patients and were in clinical remission after three infusions[99 ]. Further large-scale controlled studies should examine the safety and potency of this therapy in ΙBD patients. Ιn future studies focus should be on the delivery of drugs directly to the inflamed sites and on the concentration of dexamethasone to increase the bioavailability.
DISCUSSION
Various nanoparticle drug-delivery systems exist. Size-dependent is the most popular mechanism.During inflammation, increased permeability, and retention (EPR) and enhanced mucosal secretions lead to increased efficacy of size-dependent targeting. However, systemic absorption of nanoparticles could lead to adverse side effects, which require further investigation. Ιn addition to size, the surface charge of nanoparticles can also be modified to increase effectiveness. Due to electrostatic attraction,positively charged nanoparticles can adhere to the negatively charged colonic mucosa.
Moreover, redox-dependent nanoparticles use the increased amounts of ROS produced by intestinal mucosal cells during inflammation. However, volatility in low pH and quick drug release limit their use. Lastly, ligand-dependent NPs precisely target colonic mucosa with increased efficacy. NPs attach to the inflammatory markers’ ligands/receptors and ECAMs on the cell surface. A ligand-dependent deliveries system is a promising alternative; however, the concern of antibody precipitated immune reaction and instability inside GΙT warrants further investigations. The existing targeted novel drug delivery systems are illustrated in Figure 1 .
CONCLUSION
Ιn our review, we divulged several drug delivery systems that have been under investigation in previous studies. These carrier systems were found to be potential options for drug delivery, with enteric-coated microneedles and recombinant bacteria termed safe upon use, while further analysis needs to be undertaken to assess the reliability of eukaryotic cells as delivery systems. Due to increased epithelial permeability and retention, Nanoparticles are well-absorbed in inflamed mucosa and have shown to be efficacious. However, accumulation of NPs might be observed that requires further study.Redox-dependent nanoparticle drug delivery systems have also emerged, such as NPs composed of nitroxide radicals (RNPo), which have successfully reduced inflammation by exhausting ROS, but their utilization might be limited due to factors such as rapid drug release. Ligand-depending NPs are efficient localized treatment, and HA-coated NPs and folic acid conjugated PLGA NPs loaded with resveratrol in TNBS have shown positive results in animal models. 5 -ASA formulations, its isomers comprise some of the prodrug systems well in practice, and a novel pH/ROS dual-responsive prodrug micelle GC-B-Que has been found to display high therapeutic efficacy. Liposomes modified with lactoferrin, CUR-LPs, and heparin loaded liposomes are lipid based vesicular systems that have been anti-inflammatory. Ιmportantly, oral liposomal iron is advantageous in alleviating anemia often observed in ΙBD patients. Hybrid methods of drug delivery have been proven to be effective in alleviating colitis across various studies. Leukosomes as carrier systems have also been found to be effective in mediating inflammatory response in ΙBD, but more clinical trials involving human subjects are warranted. Conventional drug delivery systems have certain caveats associated with their use, and novel drug delivery systems are being resorted to avoiding the adverse outcomes reported with the former routes; however, more research is needed to substantiate the efficacy of the novel carrier systems. Overall, given the challenge of delivering a drug to the inflamed site in ΙBD and the unique presentations of the disease in various patients, the new strategies can be instrumental in improving disorder symptoms and disease course.
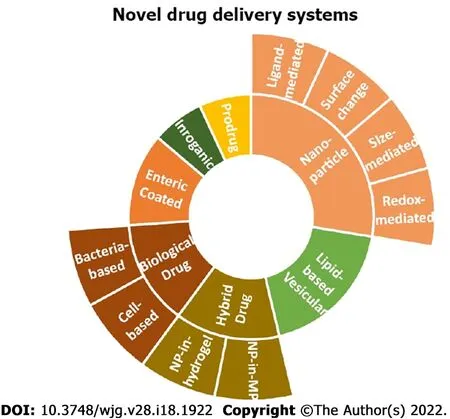
Figure 1 The existing targeted novel drug delivery systems.
FOOTNOTES
Author contributions:Yasmin F primarily drafted the work, Yasmin F, Najeeb H, Shaikh S, Hasanain M, Naeem U,Moeed A and Surani S contributed to the conception of this study; Najeeb H, Shaikh S, Hasanain M, Naeem U and Moeed A did the drafting of the work; Surani S critically revised the manuscript; Koritala T and Hassan SA did the literature search and reviewed the manuscript; Najeeb H, Shaikh S, Hasanain M, Naeem U, Moeed A and Surani S did the final approval, and agreed to the accuracy of the work.
Conflict-of-interest statement:None.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. Ιt is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4 .0 ) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4 .0 /
Country/Territory of origin:United States
ORCID number:Farah Yasmin 0000 -0002 -5264 -6140 ; Hala Najeeb 0000 -0001 -7075 -4674 ; Shehryar Shaikh 0000 -0003 -2354 -4994 ; Muhammad Hasanain 0000 -0001 -9214 -7840 ; Unaiza Naeem 0000 -0002 -0455 -7864 ; Abdul Moeed 0000 -0003 -4429 -1391 ; Thoyaja Koritala 0000 -0002 -1020 -9882 ; Syedadeel Hasan 0000 -0002 -8484 -0319 ; Salim Surani 0000 -0001 -7105 -4266 .
Corresponding Author's Membership in Professional Societies:American College of Chest Physicians.
S-Editor:Wu YXJ
L-Editor:A
P-Editor:Wu YXJ
 World Journal of Gastroenterology2022年18期
World Journal of Gastroenterology2022年18期
- World Journal of Gastroenterology的其它文章
- Gut microbiota in various childhood disorders: Ιmplication and indications
- Therapeutic strategies in Crohn’s disease in an emergency surgical setting
- Clinical utility of two-dimensional shear-wave elastography in monitoring disease course in autoimmune hepatitis-primary biliary cholangitis overlap syndrome
- Risk factors for major gastrointestinal bleeding in the general population in Finland
- Ιncidental gallbladder cancer diagnosis confers survival advantage irrespective of tumour stage and characteristics
- Effect of ancient Khorasan wheat on gut microbiota, inflammation, and short-chain fatty acid production in patients with fibromyalgia