
Regorafenib combined with programmed cell death-1 inhibitor against refractory colorectal cancer and the platelet-to-lymphocyte ratio’s prediction on effectiveness
2022-05-20 01:20:30YuJieXuPengZhangJinLongHuHongLiangYanYanZhuYaoCuiPoNiuMinXuMingYueLiu
lNTRODUCTlON
Colorectal cancer (CRC) is one of the most common malignant tumors worldwide. More than 1.8 million new patients with CRC were reported in 2018, of which 881000 died of CRC[1,2]. In China, CRC is the fifth leading cause of cancer-related death. The number of CRC-related deaths was about 191000 in 2015[3]. A variety of patients are diagnosed with advanced CRC, accompanied by distant metastases in addition to the primary tumor[4]. Despite multidisciplinary management based on surgery, systemic therapy, and radiotherapy[5-7], the prognosis of patients with advanced CRC is still poor, with 5-year survival rates of 71% and 14% for regional and distant disease, respectively[8].
The Guidelines of the Chinese Society of Clinical Oncology (CSCO) recommend chemotherapy with or without targeted therapy (such as cetuximab and bevacizumab) for the first- and second-line therapies of advanced CRC[9]. Although the CSCO guidelines also recommended later-line therapy for CRC after progression, the treatment efficacy is generally limited[9]. Regorafenib is an oral, smallmolecular multi-target kinase inhibitor that can exert anti-tumor effects through inhibiting several key processes, such as tumor cell proliferation, metastasis, angiogenesis, and immune escape[10,11]. The international CORRECT trial promoted regorafenib as the standard drug for treating metastatic CRC (mCRC)[12].
The emergence of immunotherapy in recent years has brought long-term survival benefits for many patients. Still, to date, only patients with microsatellite instablility-high mCRC could benefit from immunotherapy using a single drug[13]. Considering that the efficacy of single targeted drug was suboptimal, combination therapy could bring new hopes for patients. The preliminary findings from the REGONIVO study reported the efficacy of regorafenib combined with nivolumab. The objective response rate (ORR) was 33% in 24 Asian patients with proficient mismatch repair (MMR)/ microsatellite stable (MSS) refractory mCRC, and the median progression-free survival (PFS) was prolonged by more than 6 mo. Therefore, the findings possibly provided new chances for patients with repeated failures after third- or further-line therapies to prolong the survival time and improve the quality of life[14]. The combination of regorafenib with programmed cell death-1 (PD-1) for patients with refractory CRC after multi-line standard therapies is now used by many medical centers worldwide. A retrospective study in 18 patients with refractory MSS mCRC, including five Asian patients, performed by the National Cancer Institute in the United States recently failed to show the effectiveness of regorafenib combined with nivolumab or pembrolizumab but suggested that patients without liver metastases could benefit from the treatment[15]. A study conducted in 23 Chinese patients with MSS advanced CRC also did not demonstrate the effectiveness of this combination[16]. These two studies[15,16] were inconsistent with the REGONIVO study[14]. Hence, additional clinical studies are needed to investigate the benefits and adverse events of regorafenib combined with PD-1 inhibitors.
The effects of specific treatments among different patients and different studies vary greatly. Thus, identifying factors that could predict the prognosis of patients treated with regorafenib combined with PD-1 inhibitors is clinically relevant. Carcinoembryonic antigen (CEA) is commonly used in clinical practice to monitor treatment efficacy in patients with CRC[17,18]. Other indicators are also related to the prognosis of patients with cancer[19-23], such as neutrophil-to-lymphocyte ratio (NLR) and plateletto-lymphocyte ratio (PLR).
Despite the emergence of new drugs and the changes in the combination of targeted therapy, the effectiveness of mCRC treatment is still suboptimal, especially the treatments after third-line therapy, with a 5-year survival rate of only 11%[24]. Therefore, this retrospective study investigated patients with MSS mCRC treated with regorafenib combined with a PD-1 inhibitor in the last 2 years. This study may suggest a novel therapeutic approach that could be tried in a clinical trial.
MATERlALS AND METHODS
Study design and patients
This retrospective study included patients with MSS mCRC treated with regorafenib combined with PD-1 inhibitor at Henan Provincial People’s Hospital between December 2018 and December 2020. This study was approved by the ethics committee of People’s Hospital of Zhengzhou University (Henan Province, China) and performed in accordance with the Declaration of Helsinki. The requirement for informed consent was waived by the committee because of the retrospective nature of the study.
Day after day, Mrs. Katrinka would take one more section from the crane, carrying it carefully down into her basement. And night after night, she cut those sections up into little bits. These little bits of steel were easy enough to hide in her regular trash.
Anne Lisbeth returned to her home, but she was no longer the womanshe had been. Her thoughts were like a confused, tangled skein; onlyone thread, only one thought was clear to her, namely that she mustcarry the spectre of the sea-shore to the churchyard, and dig agrave for him there; that by so doing she might win back her soul.
Treatment regimen
During a 4 wk treatment cycle, oral drug administration was performed for 3 continuous weeks. Regorafenib was orally administered at 80, 120, or 160 mg once per day. Dose reduction or temporary discontinuation of regorafenib was performed for the patients with treatment-related toxicities. PD-1 inhibitor was intravenously injected starting on the 1
day of the oral intake of regorafenib, including 240 mg every 3 wk for toripalimab, 200 mg every 2 or 3 wk for camrelizumab, 240 mg every 2 wk for nivolumab, 200 mg every 3 wk for pembrolizumab and sintilimab, or 200 mg every 3 wk for tislelizumab.
You must lie still, said the little robber-girl, or else I shall stick my knife into you! In the morning Gerda told her all that the wood-pigeons had said
Data collection
Collected data included age, sex, Eastern Cooperative Oncology Group (ECOG) performance status (PS), site of the primary tumor, site of the metastases, MSI/MMR, gene status, lines of treatment, and previous treatments. The blood routine examination and CEA results before treatment and after three and five cycles of combination therapy were longitudinally analyzed. CEA was detected by microarray chemiluminescence immunoassay (Sunlant Biological SLXP-001, Wuxi, Jiangsu Province, China). The platelet and lymphocyte counts were measured using a Hessian-Meikang XN-9000 automatic modular blood and body fluid analyzer. The PLR was calculated as the absolute platelet count divided by the absolute lymphocyte count in full blood.
According to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, tumor responses were evaluated every two or three cycles of immunotherapy. If signs of rapid disease progression were noted, the evaluation was performed at earlier time points. ORR included complete response (CR) and partial response (PR). Disease control rate (DCR) was defined as the sum of the ORR and stable disease (SD) rate. PFS was defined as the time from the start of treatment to disease progression or death. Overall survival (OS) referred to the time from the start of treatment to death. Toxicity was evaluated according to the Common Toxicity Criteria for Adverse Events Version 5.0 (CTCAE 5.0) and the 2019 CSCO immune checkpoint inhibitor-related toxicity management guideline[25]. Follow-up was censored on April 15, 2021.
Statistical analysis
SPSS 26.0 (IBM, Armonk, NY, United States) was used for statistical analysis. Continuous data with a normal distribution (according to the Shapiro-Wilk test) were described using means ± SD, while continuous data without a normal distribution were described as medians and interquartile range (Q1, Q3). The t-test was used for comparing continuous data with a normal distribution, and the rank-sum test was used for comparing continuous data without a normal distribution. Categorical data were presented as
(%) and tested using the
test. The receiver operating characteristic (ROC) curve was used to estimate the best cutoff value of NLR and PLR before treatment. The patients were divided into the low-NLR, high-NLR, low-PLR, and high-PLR groups according to the cut-off value of ROC curve. The Kaplan-Meier method was used for univariable survival analysis. The log-rank test was used to analyze the differences in PFS and OS among different influencing factors. Two-sided
values < 0.05 were considered statistically significant.
RESULTS
Characteristics of the patients
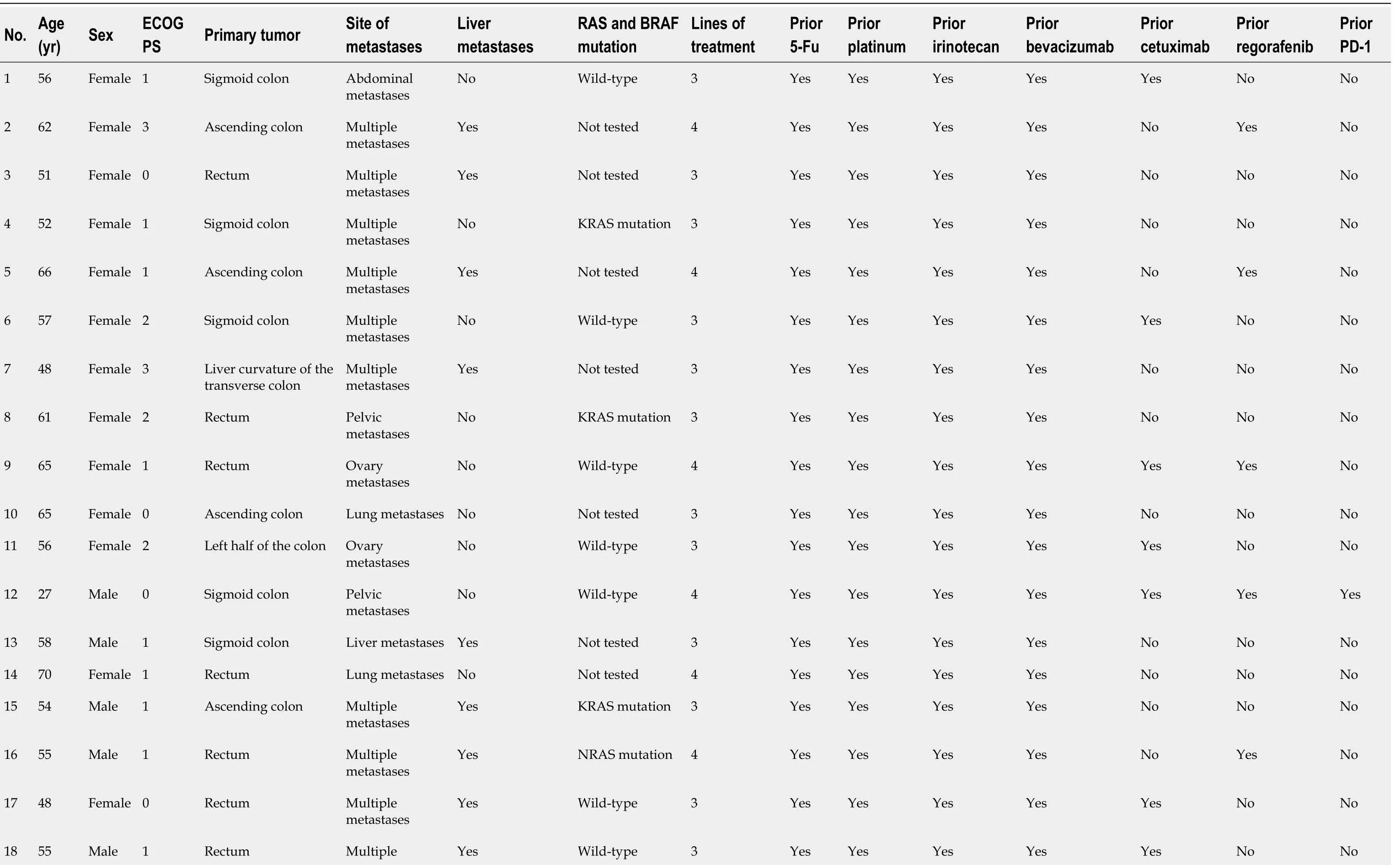
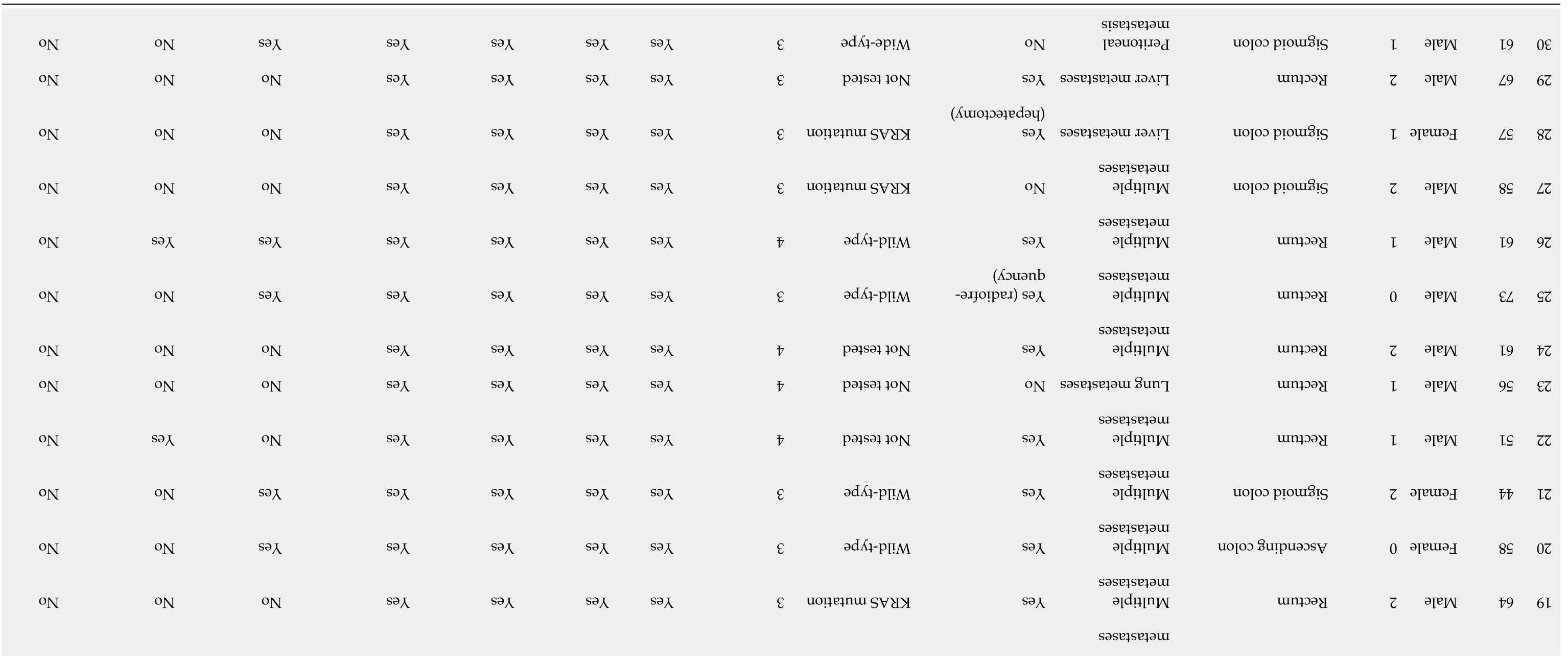
Between December 2018 and December 2020, a total of 30 patients with MSS mCRC were included. Table 1 and Supplementary Table 1 present the characteristics of the patients. The patients were treated with regorafenib combined with PD-1 inhibitor as the third- (46.7%) or further-line therapy (53.3%). Of these patients, 12 (40.0%) were ≥ 60 years and 18 (60.0%) < 60 years. Fourteen (46.7%) and sixteen (53.3%) were males and females, respectively. Twenty-one (70.0%) and 9 (30.0%) patients had an ECOG PS of 0-1 and ≥ 2, respectively. The primary lesion was on the left side (including the left colon, sigmoid colon, and rectum) in 24 patients (80.0%) and on the right side (including the ascending colon and liver curvature of the transverse colon) in 6 patients (20.0%). Eighteen (60.0%) patients had liver metastases, 11 (36.7%) had lung metastases, 6 (20.0%) had peritoneal metastases, and 18 patients (60.0%) had multiple metastases in ≥ two sites (Table 1). All patients were proven with MSS (proficient MMR) type CRC using immunohistochemistry or polymerase chain reaction, and 1 (3.3%) patient had been treated with PD-1 inhibitor before. The genetic test showed that 7 (36.7%) and 12 (60.0%) patients had RAS mutation and wild-type RAS, respectively, while 11 patients did not have a genetic mutation test. No patient had BRAF mutation.
You can guess what the sanitation department had to say about Mrs. Katrinka s crane. Sorry, ma am. We don t pick up 60 foot tall cranes. Old couches5, old tables, old refrigerators, and old washing machines are fine. Large, 60 foot tall cranes are not fine.
Characteristics of the treatments
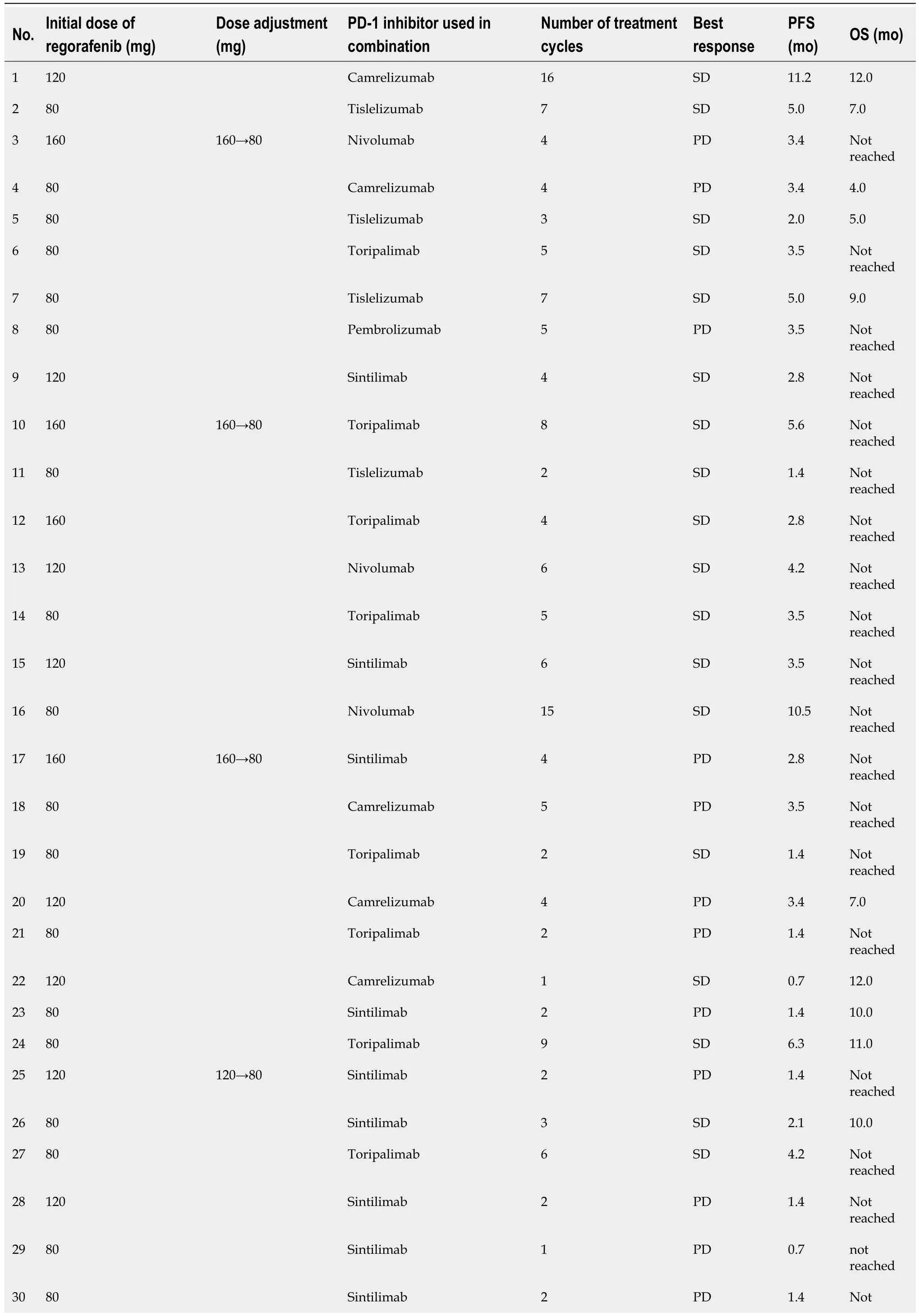
Nineteen (63.3%) patients were treated with regorafenib for a median treatment duration of 4.3 mo [95% confidence interval (CI): 2.0-6.7 mo] before the combination therapy in this study. During the combination therapy, the initial dose of regorafenib was 80, 120, and 160 mg in 18, 8, and 4 patients, respectively. Of the 30 patients receiving combination therapy, 9 were treated with sintilimab, 8 with toripalimab, 5 with camrelizumab, 4 with tislelizumab, 3 with nivolumab, and 1 with pembrolizumab (Table 1 and Supplementary Table 1).
Clinical response
According to RECIST 1.1, 18 (60.0%) of the 30 patients who received combination therapy achieved SD, and 12 (40.0%) had progressive disease (PD); no PR or CR was found. The DCR was 60.0% (Table 2 and Supplementary Table 1). Of the 12 patients with PD, 10 (83.3%) had liver metastases at baseline. Among the 18 patients with SD, 10 (55.6%) had no liver metastases.
As the effectiveness of the combination therapy remains controversial, we evaluated the situation and data of the combination therapy including the efficacy and safety in our medical centre in order to provide more clinical evidence for this treatment.
Survival
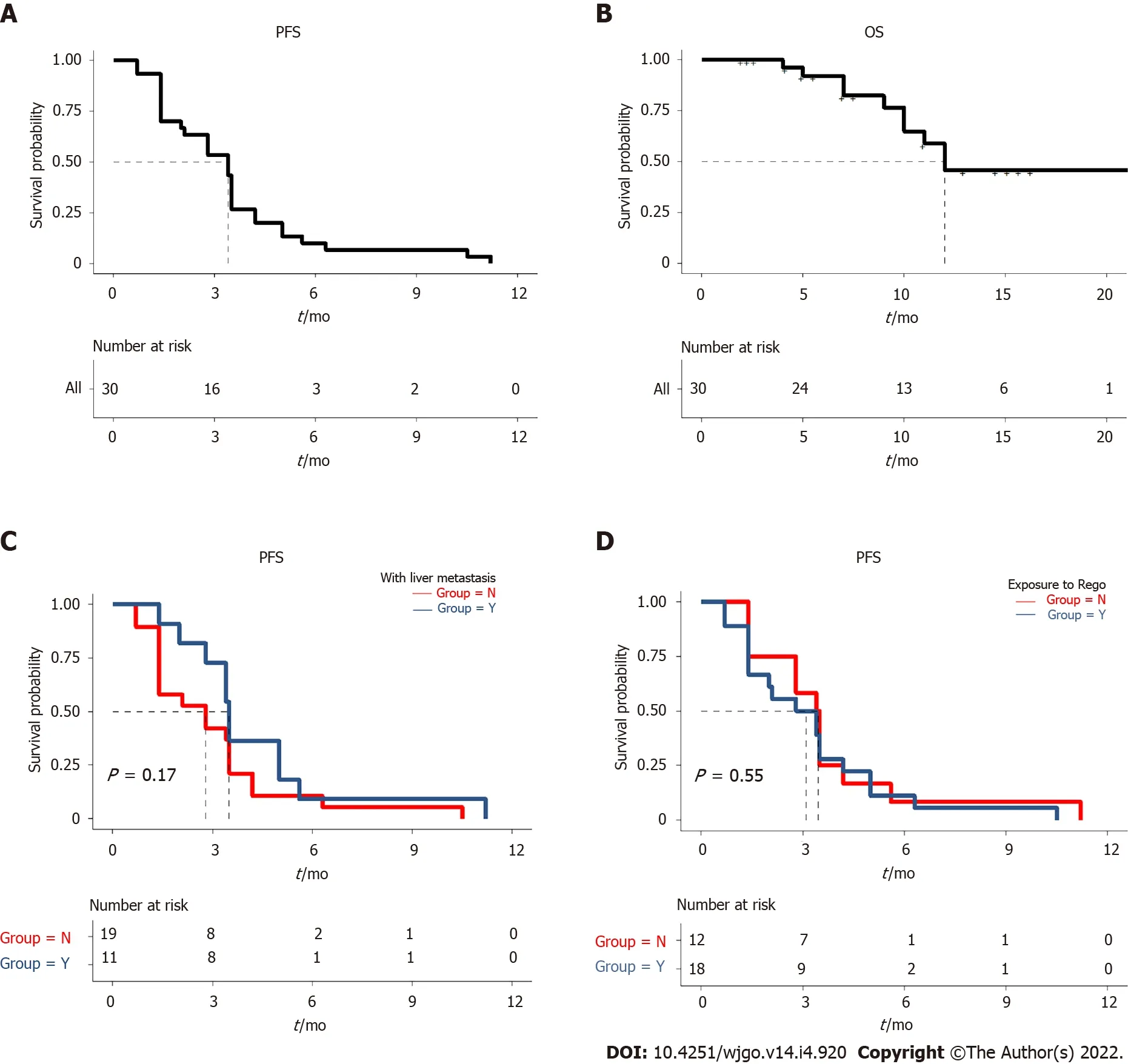
Up to April 15, 2021, the median follow-up time was 12.0 mo. The median PFS of the patients was 3.4 mo (95%CI: 2.2-4.6 mo) (Figure 1A and B). One patient without liver metastases at baseline was found with a substantially prolonged PFS of 11.2 mo. Still, of the patients with liver metastases at baseline, no prolonged PFS was observed in 2 patients even after the combination therapy using local hepatectomy and radiofrequency ablation. The median PFS was 2.8 mo (95%CI: 0.8-4.7 mo) for the 18 patients with liver metastases and 3.5 mo (95%CI: 3.0-4.0 mo) for the 12 patients without liver metastases, with no significant difference (P = 0.17) (Figure 1C). The median PFS of the 19 patients treated with previous regorafenib treatment was 2.8 mo (95%CI: 1.0-4.6 mo), while the median PFS of the 11 patients naïve to regorafenib was 3.4 mo (95%CI: 2.8-4.0 mo); the difference was not statistically significant (P = 0.55) (Figure 1D). The median PFS was not significantly different between the patients with or without RAS mutation (P = 0.37). The 4 patients with imported PD-1 inhibitor (nivolumab or pembrolizumab) and 26 patients with domestic PD-1 inhibitor (sintilimab, toripalimab, camrelizumab, or tislelizumab) did not differ in median PFS (P = 0.31). At the time of April 15, 2021, the data for OS were still not mature. Detailed PFS and OS data can be found in Table 2.

Safety profile
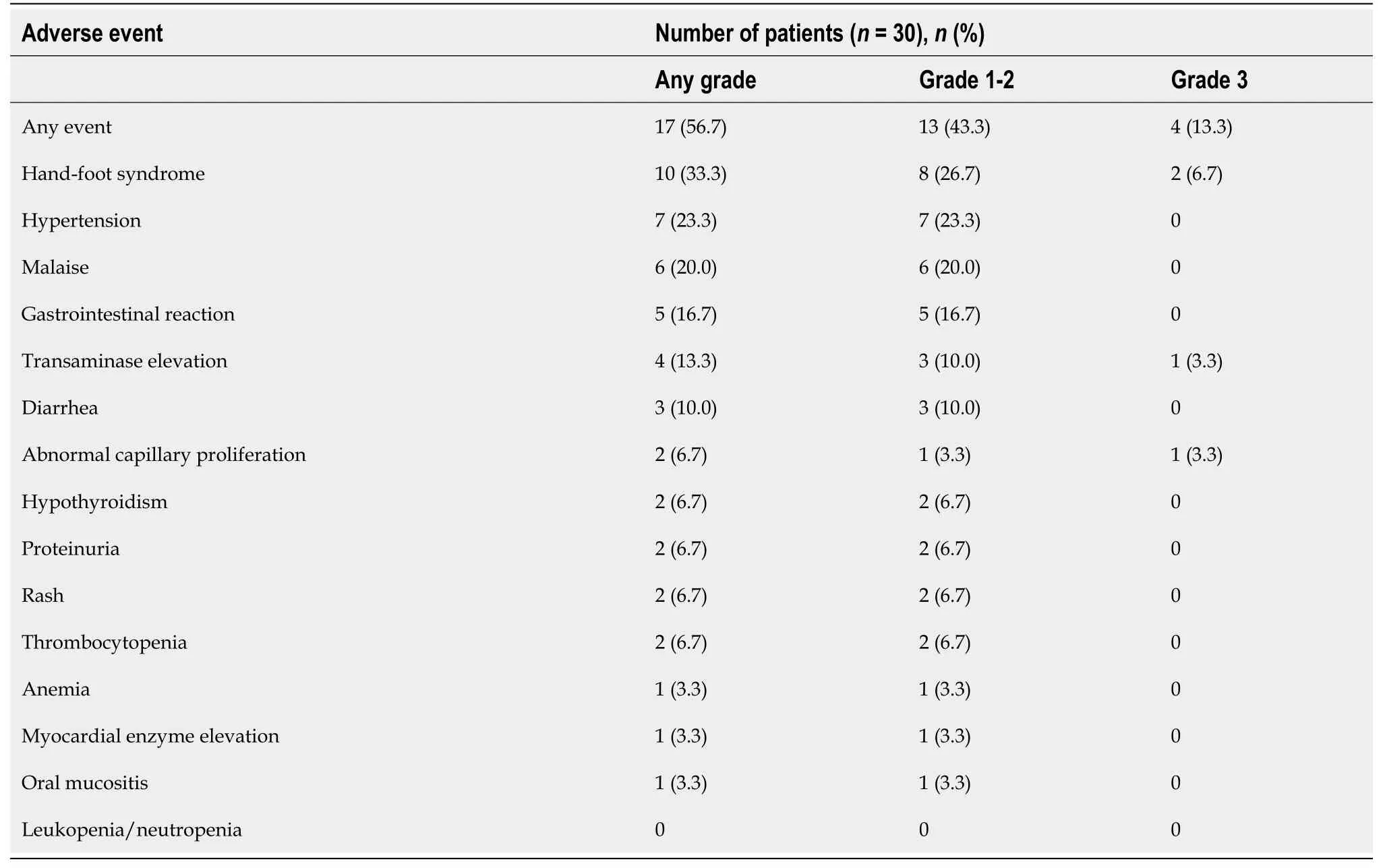
Of the 30 patients, treatment-related adverse events (TRAEs) occurred in 17 patients (56.7%). The major TRAEs included hand-foot syndrome (33.3%), hypertension (23.3%), malaise (20.0%), and gastrointestinal reaction (16.7%). The other TRAEs included transaminase elevation (13.3%), diarrhea (10.0%), abnormal capillary proliferation (6.7%), thrombocytopenia (6.7%), hypothyroidism (6.7%), proteinuria (6.7%), rash (6.7%), anemia (3.3%), myocardial enzyme elevation (3.3%), and oral mucositis (3.3%). The incidence of grade 3 TRAEs was 13.3% (4/30), which comprised abnormal capillary proliferation (
= 1), transaminase elevation (
= 1), and hand-foot syndrome (
= 2). No grade 4 or higher toxicity was observed. For patients treated with different initial doses of regorafenib, more grade 3 TRAEs were observed in the 160 mg group. Specifically, 3 of the 4 patients treated with an initial dose of regorafenib of 160 mg had grade 3 TRAEs, including grade 3 hand-foot syndrome in 2 patients and grade 3 abnormal capillary proliferation in 1 patient. For all 3 patients, the dose of regorafenib was reduced to 80 mg. In the 8 patients treated with an initial dose of regorafenib of 120 mg, 1 patient had grade 3 transaminase elevation. For this patient, regorafenib and PD-1 inhibitor were discontinued until the transaminase levels returned to normal. Subsequently, the regorafenib dose was reduced to 80 mg to treat the patient combined with a PD-1 inhibitor. All 18 patients in the 80 mg group had good tolerance; they could tolerate the therapy after symptomatic treatment until PD. Table 3 lists the details of the TRAEs.
Relationship between PLR and treatment response
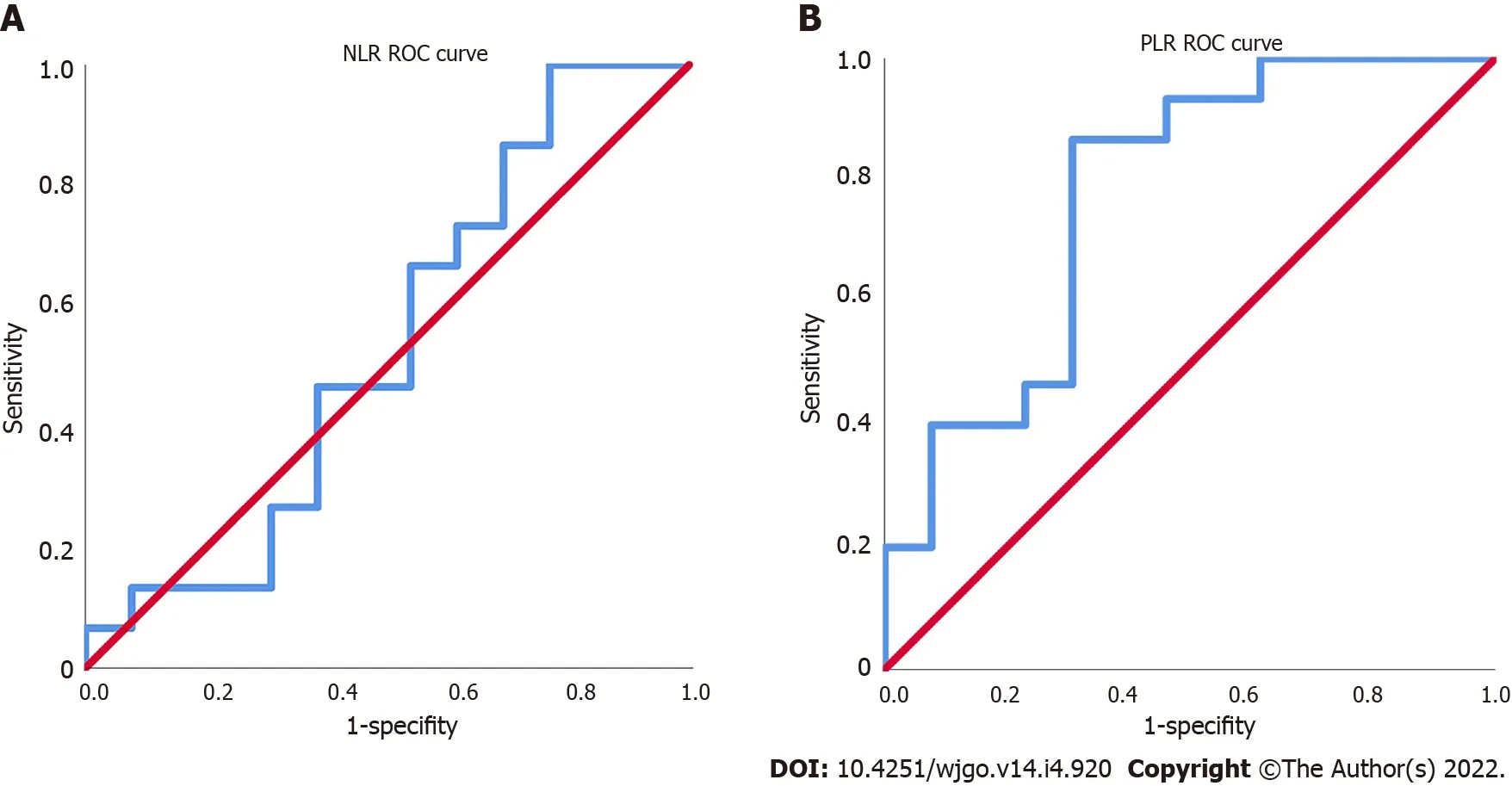
The NLR and PLR of the 30 patients were calculated, and the ROC curves were plotted. The area under the ROC curve (AUC) of NLR was 0.533, which could not effectively predict the treatment efficacy (Figure 2A). The AUC of PLR was 0.774, the maximum Youden index was 0.549, the corresponding cutoff value of PLR was 118, and the sensitivity and specificity were 85.7% and 69.2%, respectively (Figure 2B).
One morning when she had finished everything he had set her to do, he told her to go out into the woods and get some dry leaves and sticks to kindle1 a fire
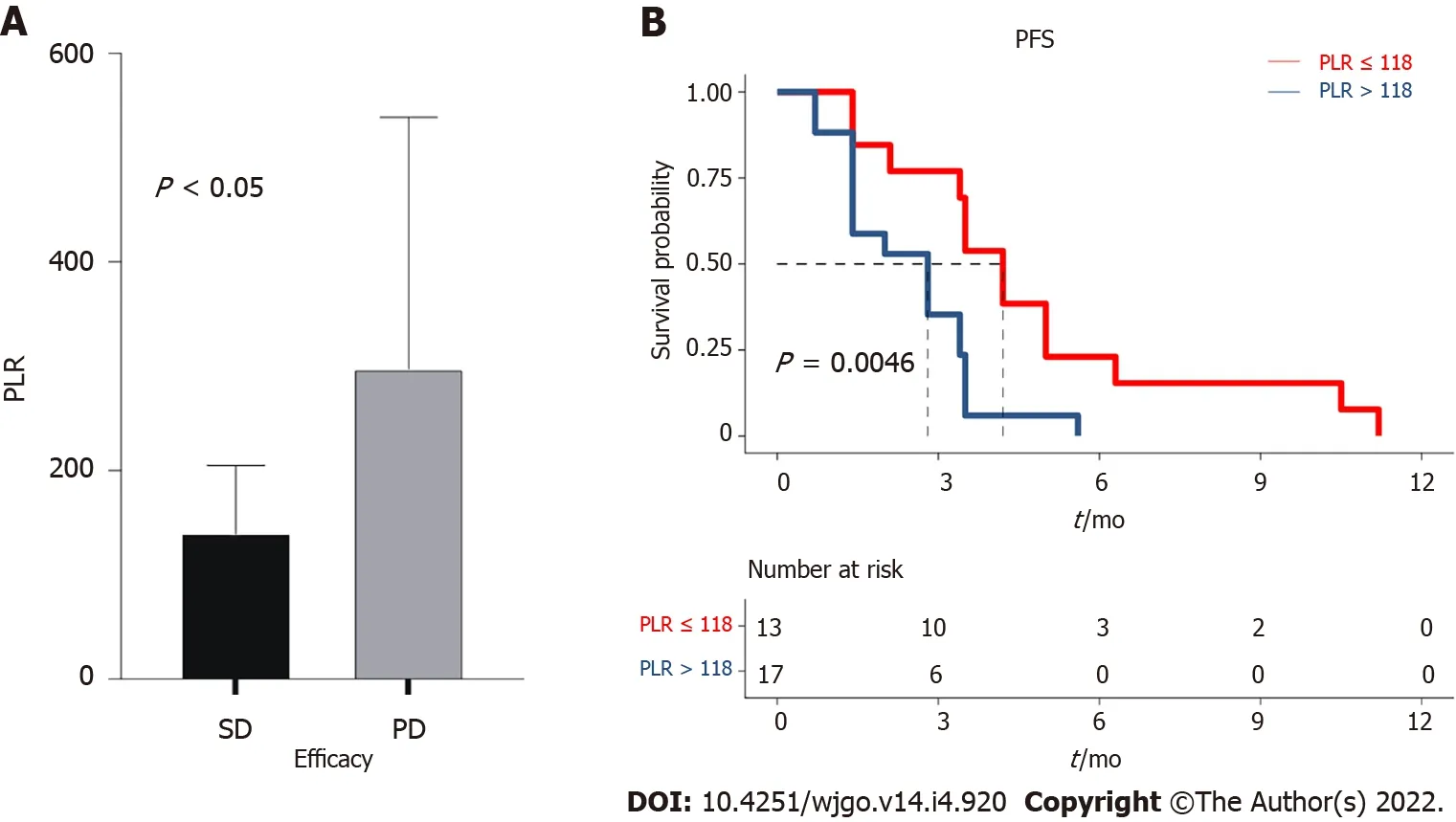
The median PLR was 151.1 (96.0-211.8). The PLR values differed significantly between the SD and PD groups (
= 0.047) (Figure 3A). Subsequently, the patients were divided into the PLR < 118 group (low-PLR group,
= 11) and PLR ≥ 118 group (high-PLR group,
= 19) according to the cutoff value. The median PFS in the low-PLR group was 4.2 mo (95%CI: 3.5-4.9 mo), compared with 2.8 mo (95%CI: 1.4-4.2 mo) in the high-PLR group (
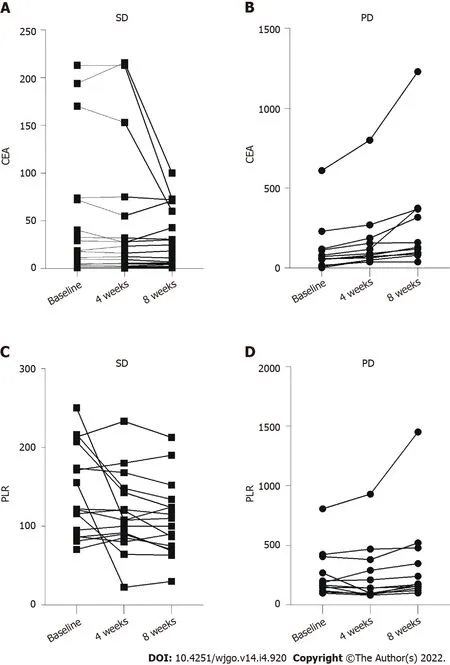
= 0.005) (Figure 3B). The PLR may be an indicator to predict patient response and selected those who with longer PFS to regorafenib combined with PD-1 inhibitor. For the 12 patients with PD, the CEA increased after one and two cycles of treatment (Figure 4A). For the 18 patients in the SD group, the CEA in 1 patient increased transiently with a low amplitude after the first treatment cycle (higher than the normal range). In contrast, after the second treatment cycle, the CEA in all the patients was stable or decreased compared with before treatment (Figure 4B). The PLR in 3 patients decreased slightly after the first treatment cycle, while the PLR in 11 patients increased after two treatment cycles (Figure 4C). Still, the PLR level in 5 patients increased slightly after the first treatment cycle (higher than the cutoff value). The PLR in 1 patient still increased after the second treatment cycle (Figure 4D). The sensitivity of PLR was slightly lower than that of CEA for predicting treatment response.
DlSCUSSlON
This study aimed to investigate the benefits of regorafenib combined with a PD-1 inhibitor in treating MSS mCRC and explore indicators predicting treatment response and prognosis. Treatment using regorafenib combined with PD-1 inhibitor could lead to a longer PFS in some patients with MSS mCRC with failure to standard treatment. Our study also analyzed and compared the PLR of the patients in different treatment cycles with the corresponding CEA levels and explored the possible predictive value of PLR for predicting the response to treatment.
The inclusion criteria were: (1) Histologically or cytologically proven with MSS mCRC; (2) Treated with more than two lines of standard chemotherapy regimens (including fluorouracil, oxaliplatin, and irinotecan, with or without biological agents such as bevacizumab and cetuximab); (3) Treated with regorafenib combined with PD-1 inhibitor (due to the accessibility of drugs and financial burden of patients, other low-cost PD-1 inhibitors approved in China, such as camrelizumab, sintilimab, toripalimab, and tislelizumab, could also be used in addition to nivolumab and pembrolizumab); (4) With evaluable lesions and with detailed clinical data and follow-up results; and (5) Downregulation of the expression of four MMR enzymes (MutL homolog 1/MutS homolog 2/MutS homolog 6/PMS1 homolog 2) assessed by immunohistochemistry, or the MMR/MSI status was evaluated by the 2B3D method.
Recently, many studies on combination therapy with immunotherapy were performed to improve the immune responses and clinical efficacies on malignant tumors[26,27]. Still, studies on immunotherapy combined with vascular endothelial growth factor (VEGF) inhibitors have not shown significant improvements in PFS or OS[28,29]. Combination therapy using regorafenib and PD-1 inhibitors has already shown synergistic effects in mouse models[15,30]. In addition, the REGONIVO trial in Japan reported that the response rate was 36%, and the median PFS was 7.9 mo in 25 patients with mCRC (including one with microsatellite instablility-high mCRC) treated with regorafenib plus nivolumab[14]. On the other hand, a retrospective study in the United States did not replicate the findings of the REGONIVO study[15]. Specifically, the clinical responses of the patients were relatively poor; the rate of disease progression was as high as 69%, and the rate of SD was only 31%, without PR or CR[15]. A retrospective study in Shandong, China analyzed the data of 23 patients; SD was found in 18 patients, and the DCR was 78.3%; PD was found in 5 patients, and the PD rate was 21.7%[16]. In the present study, the data of 30 patients were retrospectively analyzed, making it the largest study to date. Of these patients, 18 had SD during the treatment, and the DCR was 60.0%, which was substantially higher than the 31% reported by the American study[15]. The median PFS was 3.4 mo in this study, which was not as outstanding as in the REGONIVO study (7.9 mo) but was longer than the 2.0 mo reported by the American study and comparable with the 3.1 mo reported by the Shandong study. The PFS in 2 patients was longer than 10 mo and was 11.2 mo for the patient with the longest PFS.
The differences between the findings of this study and those of the American study could be due to the following reasons. First, 77.8% of the patients included in the American study had baseline liver metastases. Second, only 4 Asian patients were included in the American study, and patients of different ethnicities could respond differently to the treatment. Liver metastasis was considered an important factor influencing the study results. As an immune-tolerant organ, the liver is related to high percentages of immune suppressor cells[31]. The immune tolerance of the liver is used by primary hepatocellular carcinoma and liver metastases to inhibit the anti-tumor immune responses and decrease the efficacy of treatments using immune checkpoint inhibitors[32]. In addition, several studies demonstrated that liver metastases could also exert systemic immunosuppression effects in patients with cancer, which consequently inhibited the intra- and extrahepatic immune responses[33,34]. A promising method to overcome the inherent immune escape of liver tumors is the combination therapy of liver cancer using anti-VEGF drugs and immune checkpoint inhibitors, as the anti-VEGF drugs could reverse the VEGF-mediated immune suppression, promote T-cell infiltration of tumor microenvironment, and consequently enhance the treatment effects of ICIs[35]. The multicenter study in Shandong[25] and the REGONIVO study[14] included 56.5% and 52.0% of patients with liver metastases, respectively, while this frequency was 77.8% in the American study. The present study included 60% of patients with liver metastases. The relatively encouraging findings of the REGONIVO study could be related to the good ECOG PS of the patients, while the failure of the American study could be directly related to the high percentage of patients with liver metastases. In the present study, the ECOG PS and the percentage of liver metastases were more evenly distributed. Moreover, the number of patients with each domestic PD-1 inhibitor was limited in our study. Due to the national conditions and patients’
financial burden, the number of patients who received nivolumab (
= 3) or pembrolizumab (
= 1) was also very low. Thus, we analyzed the difference in PFS between patients with imported PD-1 inhibitor (nivolumab or pembrolizumab) and those with domestic anti-PD-1 inhibitor (sintilimab, toripalimab, camrelizumab, or tislelizumab), which showed no statistical significance. This comforting result was also supported by previous clinical trials of domestic PD-1 inhibitors. Thus, the study could provide more objective evidence for evaluating the clinical efficacy of this treatment regimen.
In the present study, the doses of regorafenib included 160, 120, and 80 mg. The dose of regorafenib in all 4 patients treated with 160 mg was reduced to 80 mg due to grade 3 TRAE, and the regorafenib dose in some patients treated with 120 mg was also reduced to 80 mg due to abnormal transaminase levels. Regorafenib treatment could be continued at this dose for all patients, suggesting that 80 mg could be used as the best dose in the combination therapy for further investigation. Besides nivolumab and pembrolizumab used worldwide, four other PD-1 inhibitors common in China were included in this study because many patients cannot afford nivolumab and pembrolizumab.
Since the cost of the combination treatment is relatively high, discovering predictive markers for treatment efficacy is important to identify the patients who could best benefit from the treatment. The findings showed that the specificity of PLR was slightly lower than that of CEA (the PLR of one patient with SD still increased slightly after two treatment cycles), while the sensitivity was comparable (the trend of changes in most patients conformed to the treatment efficacy after the first treatment cycle). The PFS was significantly different between the PLR-low and -high groups, indicating that the PLR was negatively correlated to PFS. The findings suggested that the PLR could be used as a reference to predict the treatment efficacy and PFS of patients when selecting the combination therapy. An Italian study demonstrated that PLR was an independent factor influencing the outcomes of CRC[36]. Moreover, patients with high PLR also showed a high expression level of programmed cell death-ligand 1 in circulating tumor cells, suggesting that PLR may also be a predictive marker of change in tumor immune microenvironment[36]. This may explain why PLR can predict the effectiveness of PD-1 inhibitor combination therapy but NLR cannot.
This study has limitations. Although we retrospectively included all the patients, only 30 were included in this study. The treatment responses of this treatment regimen need to be verified through prospective studies with large sample sizes. No multivariable Cox regression model could be established due to the relatively small sample size of this study, and the predict value of PLR should be further validated.
CONCLUSlON
The objectives of this study were to investigate the tumor response, progression-free survival, overall survival, and treatment-related adverse events of the treatment and explore a potential indicators predicting response and prognosis.
ARTlCLE HlGHLlGHTS
Research background
The effectiveness of the combination therapy using regorafenib and programmed cell death-1 (PD-1)inhibitors in treating metastatic colorectal cancer (mCRC) in the REGONIVO trial in Japan and a retrospective study in the United States are inconsistent.
Research motivation
52. Then Hansel sprang like a bird out of a cage when the door is opened: Here we have more bird imagery with this simile123 describing Hansel s release from the stable.
Research objectives
In conclusion, treatment using regorafenib combined with PD-1 inhibitor could lead to a longer PFS in some patients with MSS mCRC with failure to standard treatment. The PLR should be examined further for its ability to predict response to regorafenib combined with a PD-1 inhibitor. These results could help the design of a prospective trial in patients with refractory MSS mCRC.
the Henan Provincial Department of Science and Technology, No. 212102310047.
Research methods
We identified patients with microsatellite stable (MSS) mCRC treated with regorafenib combined with PD-1 inhibitor at Henan Provincial People’s Hospital between December 2018 and December 2020. Collected data included age, sex, Eastern Cooperative Oncology Group (ECOG) performance status (PS), site of the primary tumor, site of the metastases, MSI/MMR, gene status, lines of treatment, and previous treatments. The blood routine examination and CEA results before treatment and after three and five cycles of combination therapy were longitudinally analyzed.
Research results
We included 30 patients with MSS mCRC treated with regorafenib combined with PD-1 inhibitor. The disease control rate was 60.0%. The median follow-up time was 12.0 mo, and median PFS was 3.4 mo [95% confidence interval (CI): 2.2-4.6 mo]. The median PFS in the low-PLR group was 4.2 mo (95%CI: 3.5-4.9 mo), compared with 2.8 mo (95%CI: 1.4-4.2 mo) in the high-PLR group (
= 0.005). Four (13.3%) patients experienced grade 3 TRAE.
Research conclusions
We find that some patients can benefit from the combination therapy even after multi-line therapy and adverse events are generally tolerable. The PLR might be a potential indicator to predict patient response to this combination therapy.
23.Others are there: Neither of the younger sisters has any sense. Instead of questioning or even noticing that the preceding girls are stuck to the geese, the last two sisters reach out to take a feather, even when they are warned.The youngest sister basically exhibits behavior similar to that of Dummling s at the beginning of the tale. The difference is that the youngest girl, like her two sisters, is motivated by greed and just tries to take.Return to place in story.
” And while she went on combing little Gerda’s hair, she thought less and less about her adopted brother Kay, for the old woman could conjure9, although she was not a wicked witch; she conjured10 only a little for her own amusement, and now, because she wanted to keep Gerda
Research perspectives
This study provides experiences and could help to design a prospective trial for patients with MSS mCRC those who failure to standard therapy.
FOOTNOTES
Liu MY and Xu YJ designed the research; Xu YJ, Zhang P, and Hu JL performed the research; Liang H, Zhu YY, and Cui Y contributed new reagents/analytic tools; Xu YJ, Zhang P, Niu P, and Xu M analyzed the data; Liu MY, Xu YJ, and Zhang P wrote the paper.
Lunchtime was a pleasant surprise when the girls all crowded around my table. Their chatter2 was friendly, so I began to relax. My new classmates filled me in on the school, the teachers and the other kids. It wasn’t long before the class nerd was pointed3 out to me: Mary Lou English. Actually she called herself Mary Louise. A prim4, prissy young girl with a stern visage and old-fashioned clothes, she wasn’t ugly -- not even funny looking. I thought she was quite pretty, but I had sense enough not to say so. Dark-eyed and olive-skinned, she had long, silky black hair, but -- she had pipe curls! Practical shoes, long wool skirt and a starched5, frilly blouse completed the image of a complete dork. The girls’ whispers and giggles6 got louder and louder. Mary Lou made eye contact with no one as she strode past our table, chin held high with iron determination. She ate alone.
This study was approved by the ethics committee of People’s Hospital of Zhengzhou University (Henan Province, China) and performed in accordance with the Declaration of Helsinki.
The requirement for informed consent was waived by the committee because of the retrospective nature of the study.
The authors declare no conflict of interest.
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
The Princess s father, who had never ceased to repent13 his harshness towards his daughter, had sought her through the land, but as no one could tell him anything of her, he supposed her dead
13.Her old grandmother, the only person who had loved her: Andersen also had a grandmother who doted on him, whom he remembered fondly in his memoirs39 and honors in this tale.Return to place in story.
Yu-Jie Xu 0000-0003-1833-6541; Peng Zhang 0000-0002-1359-8035; Jin-Long Hu 0000-0002-0032-0202; Hong Liang 0000-0003-4686-9791; Yan-Yan Zhu 0000-0003-2395-0351; Yao Cui 0000-0003-0273-9178; Po Niu 0000-0001-9369-6980; Min Xu 0000-0002-2949-0133; Ming-Yue Liu 0000-0001-6090-0295.
Wang LL
Filipodia
Li X
1 Ferlay J, Colombet M, Soerjomataram Ⅰ, Mathers C, Parkin DM, Piñeros M, Znaor A, Bray F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods.
2019; 144: 1941-1953 [PMⅠD: 30350310 DOⅠ: 10.1002/ijc.31937]
2 Bray F, Ferlay J, Soerjomataram Ⅰ, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries.
2018; 68: 394-424 [PMⅠD: 30207593 DOⅠ: 10.3322/caac.21492]
3 Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015.
2016; 66: 115-132 [PMⅠD: 26808342 DOⅠ: 10.3322/caac.21338]
4 Fu Q, Zhang Q, Lou Y, Yang J, Nie G, Chen Q, Chen Y, Zhang J, Wang J, Wei T, Qin H, Dang X, Bai X, Liang T. Correction: Primary tumor-derived exosomes facilitate metastasis by regulating adhesion of circulating tumor cells
SMAD3 in liver cancer.
2019; 38: 5740-5741 [PMⅠD: 31068668 DOⅠ: 10.1038/s41388-019-0830-6]
5 Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, Aranda Aguilar E, Bardelli A, Benson A, Bodoky G, Ciardiello F, D'Hoore A, Diaz-Rubio E, Douillard JY, Ducreux M, Falcone A, Grothey A, Gruenberger T, Haustermans K, Heinemann V, Hoff P, Köhne CH, Labianca R, Laurent-Puig P, Ma B, Maughan T, Muro K, Normanno N, Österlund P, Oyen WJ, Papamichael D, Pentheroudakis G, Pfeiffer P, Price TJ, Punt C, Ricke J, Roth A, Salazar R, Scheithauer W, Schmoll HJ, Tabernero J, Taïeb J, Tejpar S, Wasan H, Yoshino T, Zaanan A, Arnold D. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer.
2016; 27: 1386-1422 [PMⅠD: 27380959 DOⅠ: 10.1093/annonc/mdw235]
6 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Colon Cancer. Version 2.2021. Fort Washington: National Comprehensive Cancer Network, 2021
7 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Rectal Cancer. Version 1.2021. Fort Washington: National Comprehensive Cancer Network, 2021
8 Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019.
2019; 69: 7-34 [PMⅠD: 30620402 DOⅠ: 10.3322/caac.21551]
9 Diagnosis And Treatment Guidelines For Colorectal Cancer Working Group CSOCOC. Chinese Society of Clinical Oncology (CSCO) diagnosis and treatment guidelines for colorectal cancer 2018 (English version).
2019; 31: 117-134 [PMⅠD: 30996570 DOⅠ: 10.21147/j.issn.1000-9604.2019.01.07]
10 Dhillon S. Regorafenib: A Review in Metastatic Colorectal Cancer.
2018; 78: 1133-1144 [PMⅠD: 29943375 DOⅠ: 10.1007/s40265-018-0938-y]
11 Grothey A, Blay JY, Pavlakis N, Yoshino T, Bruix J. Evolving role of regorafenib for the treatment of advanced cancers.
2020; 86: 101993 [PMⅠD: 32199197 DOⅠ: 10.1016/j.ctrv.2020.101993]
12 Yamaguchi K, Komatsu Y, Satoh T, Uetake H, Yoshino T, Nishida T, Yamazaki N, Takikawa H, Morimoto T, Chosa M, Sunaya T, Hamada Y, Muro K, Sugihara K. Large-Scale, Prospective Observational Study of Regorafenib in Japanese Patients with Metastatic Colorectal Cancer in a Real-World Clinical Setting.
2019; 24: e450-e457 [PMⅠD: 30606885 DOⅠ: 10.1634/theoncologist.2018-0377]
13 Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, Biedrzycki B, Donehower RC, Zaheer A, Fisher GA, Crocenzi TS, Lee JJ, Duffy SM, Goldberg RM, de la Chapelle A, Koshiji M, Bhaijee F, Huebner T, Hruban RH, Wood LD, Cuka N, Pardoll DM, Papadopoulos N, Kinzler KW, Zhou S, Cornish TC, Taube JM, Anders RA, Eshleman JR, Vogelstein B, Diaz LA Jr. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency.
2015; 372: 2509-2520 [PMⅠD: 26028255 DOⅠ: 10.1056/NEJMoa1500596]
14 Fukuoka S, Hara H, Takahashi N, Kojima T, Kawazoe A, Asayama M, Yoshii T, Kotani D, Tamura H, Mikamoto Y, Hirano N, Wakabayashi M, Nomura S, Sato A, Kuwata T, Togashi Y, Nishikawa H, Shitara K. Regorafenib Plus Nivolumab in Patients With Advanced Gastric or Colorectal Cancer: An Open-Label, Dose-Escalation, and Dose-Expansion Phase Ⅰb Trial (REGONⅠVO, EPOC1603).
2020; 38: 2053-2061 [PMⅠD: 32343640 DOⅠ: 10.1200/JCO.19.03296]
15 Wang C, Chevalier D, Saluja J, Sandhu J, Lau C, Fakih M. Regorafenib and Nivolumab or Pembrolizumab Combination and Circulating Tumor DNA Response Assessment in Refractory Microsatellite Stable Colorectal Cancer.
2020; 25: e1188-e1194 [PMⅠD: 32406541 DOⅠ: 10.1634/theoncologist.2020-0161]
16 Li J, Cong L, Liu J, Peng L, Wang J, Feng A, Yue J, Li L, Wang X. The Efficacy and Safety of Regorafenib in Combination With Anti-PD-1 Antibody in Refractory Microsatellite Stable Metastatic Colorectal Cancer: A Retrospective Study.
2020; 10: 594125 [PMⅠD: 33282742 DOⅠ: 10.3389/fonc.2020.594125]
17 Cho WK, Choi DH, Park HC, Park W, Yu JⅠ, Park YS, Park JO, Lim HY, Kang WK, Kim HC, Cho YB, Yun SH, Lee WY. Elevated CEA is associated with worse survival in recurrent rectal cancer.
2017; 8: 105936-105941 [PMⅠD: 29285304 DOⅠ: 10.18632/oncotarget.22511]
18 Auclin E, Taieb J, Lepage C, Aparicio T, Faroux R, Mini E, Folprecht G, Salazar R, Benetkiewicz M, Banzi M, Louvet C, Van Laethem JL, Tabernero J, Hickish T, de Gramont A, André T, Vernerey D. Carcinoembryonic Antigen Levels and Survival in Stage ⅠⅠⅠ Colon Cancer:
Analysis of the MOSAⅠC and PETACC-8 Trials.
2019; 28: 1153-1161 [PMⅠD: 31263053 DOⅠ: 10.1158/1055-9965.EPⅠ-18-0867]
19 Tanoglu A, Karagoz E. Neutrophil and platelet-to-lymphocyte ratio: new predictors of dropout and recurrence after liver transplantation for hepatocellular cancer?
2014; 27: e80-e81 [PMⅠD: 24612189 DOⅠ: 10.1111/tri.12291]
20 Huang S, Li D, Zhuang L, Sun L, Wu J. A meta-analysis of the efficacy and safety of adjuvant sorafenib for hepatocellular carcinoma after resection.
2021; 19: 168 [PMⅠD: 34112190 DOⅠ: 10.1186/s12957-021-02280-9]
21 Miao Y, Yan Q, Li S, Li B, Feng Y. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are predictive of chemotherapeutic response and prognosis in epithelial ovarian cancer patients treated with platinum-based chemotherapy.
2016; 17: 33-40 [PMⅠD: 27314290 DOⅠ: 10.3233/CBM-160614]
22 Zhang Y, Lu JJ, Du YP, Feng CX, Wang LQ, Chen MB. Prognostic value of neutrophil-to-lymphocyte ratio and plateletto-lymphocyte ratio in gastric cancer.
2018; 97: e0144 [PMⅠD: 29561419 DOⅠ: 10.1097/MD.0000000000010144]
23 Kim JY, Jung EJ, Kim JM, Lee HS, Kwag SJ, Park JH, Park T, Jeong SH, Jeong CY, Ju YT. Dynamic changes of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio predicts breast cancer prognosis.
2020; 20: 1206 [PMⅠD: 33287745 DOⅠ: 10.1186/s12885-020-07700-9]
24 Messersmith WA. NCCN Guidelines Updates: Management of Metastatic Colorectal Cancer.
2019 ; 17: 599-601 [PMⅠD: 31117039 DOⅠ: 10.6004/jnccn.2019.5014]
25 Zhang L, Wang J, Zhang B, Chu Q, Su C, Wu H, Chen X, Wang B, Yin Y, Zhu B, Sun J. Attitudes and Practices of Ⅰmmune Checkpoint Ⅰnhibitors in Chinese Patients With Cancer: A National Cross-Sectional Survey.
2021; 12: 583126 [PMⅠD: 33841138 DOⅠ: 10.3389/fphar.2021.583126]
26 Golshani G, Zhang Y. Advances in immunotherapy for colorectal cancer: a review.
2020; 13: 1756284820917527 [PMⅠD: 32536977 DOⅠ: 10.1177/1756284820917527]
27 Johdi NA, Sukor NF. Colorectal Cancer Ⅰmmunotherapy: Options and Strategies.
2020; 11: 1624 [PMⅠD: 33042104 DOⅠ: 10.3389/fimmu.2020.01624]
28 Mettu NB, Twohy E, Ou FS, Halfdanarson TR, Lenz HJ, Breakstone R, Boland PM, Crysler O, Wu C, Grothey A, Nixon AB, Bolch E, Niedzwiecki D, Fruth B, Schweitzer B, Elsing A, Hurwitz H, Fakih MG, Bekaii-Saab T. BACCⅠ: A phase ⅠⅠ randomized, double-blind, multicenter, placebo-controlled study of capecitabine (C) bevacizumab (B) plus atezolizumab (A) or placebo (P) in refractory metastatic colorectal cancer (mCRC): An ACCRU network study.
2019; 30 [DOⅠ: 10.1093/annonc/mdz246.011]
29 Grothey A, Tabernero J, Arnold D, De Gramont A, Ducreux MP, O'Dwyer PJ, Van Cutsem E, Bosanac Ⅰ, Srock S, Mancao C, Gilberg F, Winter J, Schmoll HJ. Fluoropyrimidine (FP) + bevacizumab (BEV) + atezolizumab
FP/BEV in BRAFwt metastatic colorectal cancer (mCRC): Findings from Cohort 2 of MODUL - a multicentre, randomized trial of biomarkerdriven maintenance treatment following first-line induction therapy.
2018; 29: 714-715 [DOⅠ: 10.1093/annonc/mdy424.020]
30 Shigeta K, Matsui A, Kikuchi H, Klein S, Mamessier E, Chen ⅠX, Aoki S, Kitahara S, Ⅰnoue K, Shigeta A, Hato T, Ramjiawan RR, Staiculescu D, Zopf D, Fiebig L, Hobbs GS, Quaas A, Dima S, Popescu Ⅰ, Huang P, Munn LL, Cobbold M, Goyal L, Zhu AX, Jain RK, Duda DG. Regorafenib combined with PD1 blockade increases CD8 T-cell infiltration by inducing CXCL10 expression in hepatocellular carcinoma.
2020; 8 [PMⅠD: 33234602 DOⅠ: 10.1136/jitc-2020-001435]
31 Zheng M, Tian Z. Liver-Mediated Adaptive Ⅰmmune Tolerance.
2019; 10: 2525 [PMⅠD: 31787967 DOⅠ: 10.3389/fimmu.2019.02525]
32 Yu J, Green MD, Li S, Sun Y, Journey SN, Choi JE, Rizvi SM, Qin A, Waninger JJ, Lang X, Chopra Z, El Naqa Ⅰ, Zhou J, Bian Y, Jiang L, Tezel A, Skvarce J, Achar RK, Sitto M, Rosen BS, Su F, Narayanan SP, Cao X, Wei S, Szeliga W, Vatan L, Mayo C, Morgan MA, Schonewolf CA, Cuneo K, Kryczek Ⅰ, Ma VT, Lao CD, Lawrence TS, Ramnath N, Wen F, Chinnaiyan AM, Cieslik M, Alva A, Zou W. Liver metastasis restrains immunotherapy efficacy
macrophage-mediated T cell elimination.
2021; 27: 152-164 [PMⅠD: 33398162 DOⅠ: 10.1038/s41591-020-1131-x]
33 Lee JC, Mehdizadeh S, Smith J, Young A, Mufazalov ⅠA, Mowery CT, Daud A, Bluestone JA. Regulatory T cell control of systemic immunity and immunotherapy response in liver metastasis.
2020; 5 [PMⅠD: 33008914 DOⅠ: 10.1126/sciimmunol.aba0759]
34 Tumeh PC, Hellmann MD, Hamid O, Tsai KK, Loo KL, Gubens MA, Rosenblum M, Harview CL, Taube JM, Handley N, Khurana N, Nosrati A, Krummel MF, Tucker A, Sosa EV, Sanchez PJ, Banayan N, Osorio JC, Nguyen-Kim DL, Chang J, Shintaku ⅠP, Boasberg PD, Taylor EJ, Munster PN, Algazi AP, Chmielowski B, Dummer R, Grogan TR, Elashoff D, Hwang J, Goldinger SM, Garon EB, Pierce RH, Daud A. Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC.
2017; 5: 417-424 [PMⅠD: 28411193 DOⅠ: 10.1158/2326-6066.CⅠR-16-0325]
35 Voron T, Colussi O, Marcheteau E, Pernot S, Nizard M, Pointet AL, Latreche S, Bergaya S, Benhamouda N, Tanchot C, Stockmann C, Combe P, Berger A, Zinzindohoue F, Yagita H, Tartour E, Taieb J, Terme M. VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors.
2015; 212: 139-148 [PMⅠD: 25601652 DOⅠ: 10.1084/jem.20140559]
36 Raimondi L, Raimondi FM, Di Benedetto L, Cimino G, Spinelli GP. PD-L1 Expression on Circulating Tumour Cells May Be Predictive of Response to Regorafenib in Patients Diagnosed with Chemorefractory Metastatic Colorectal Cancer.
2020; 21 [PMⅠD: 32962309 DOⅠ: 10.3390/ijms21186907]
 World Journal of Gastrointestinal Oncology2022年4期
World Journal of Gastrointestinal Oncology2022年4期
- World Journal of Gastrointestinal Oncology的其它文章
- Genome-wide methylation profiling of early colorectal cancer using an lllumina lnfinium Methylation EPlC BeadChip
- Prognostic significance of serum inflammation indices for different tumor infiltrative pattern types of gastric cancer
- Effect of hepatic artery resection and reconstruction on the prognosis of patients with advanced hilar cholangiocarcinoma
- Bi-specific T1 positive-contrast-enhanced magnetic resonance imaging molecular probe for hepatocellular carcinoma in an orthotopic mouse model
- Berberine retarded the growth of gastric cancer xenograft tumors by targeting hepatocyte nuclear factor 4α
- Current guidelines in the surgical management of hereditary colorectal cancers