
Multidimensional health literacy profiles and health-related behaviors in the elderly: A cross-sectional survey
2022-05-10 00:57:18YingXieWenhongAnChunyunZhengDiZhoHonghongWng
Ying Xie , Wenhong An , Chunyun Zheng , Di Zho , Honghong Wng ,*
a Xiangya School of Nursing, Central South University, Changsha, Hunan, China
b School of Health and Wellness, Panzhihua University, Panzhihua, Sichuan, China
Keywords:Aged China Community health centers Health behavior Health literacy Surveys and questionnaires
ABSTRACT Objectives: To investigate health literacy profiles using a multidimensional tool in the elderly,analyze the factors related to health literacy, and explore the relationships between health literacy and healthrelated behaviors.Methods: A cross-sectional survey including 440 participants was conducted at a community health center and a village health center in Changsha,Hunan Province,between June 2020 and August 2020.We used the Health Literacy Questionnaire (HLQ) to assess the elderly’s health literacy.Sociodemographic data and health-related behaviors of them were surveyed with a self-designed questionnaire.Latent profile analysis, Pearson’s chi-squared and ordinal logistic regression were used to analyze the data.Results: The median age of the 440 respondents was 68 years.The participants had the lowest scores in the “appraisal of health information” subscale (2.22 ± 0.52), followed by “navigating the healthcare system”subscale(2.89±0.81)of HLQ.Based on the analysis of three profiles,respondents who were 60-74 years(OR =2.06,95%CI:1.23-3.42, P =0.006),living in urban areas(OR =3.28,95%CI:2.17-4.94,P <0.001), with secondary education or above (OR =2.86, 95% CI: 1.92-4.27, P <0.001), and having health insurance (OR =1.89, 95% CI: 1.02-3.51, P =0.042) were significantly associated with health literacy.Statistically significant associations were found between health literacy level and health-related behaviors, including medical service-seeking behavior (χ2 =25.14, P <0.001), exercising regularly(χ2 =34.08,P <0.001),and taking a medical examination in the past 12 months(χ2 =24.76,P <0.001).Conclusion: The multidimensional health literacy survey has identified the low health literacy level among the elderly in community settings.It revealed the relationships of sociodemographic characteristics, including age, education level and residence, with health literacy.These findings emphasized the importance of health literacy in promoting health behaviors, guiding a profound understanding of the Chinese elderly’s health needs and health literacy to develop community-based health promotion interventions.
What is known?
· China has become one of the most aging countries globally;coping with the aging problem and achieving healthy aging has been an urgent problem to be solved.
· The elderly with low health literacy had a high risk of poor selfmanagement of health and underutilized health services,which burdened individual economies and national health systems.Improving the health literacy of older adults is a considerable determinant to achieve healthy aging.
· Most previous studies on the health literacy of the Chinese elderly focused on fundamental health literacy.However, the perception of health literacy has gradually extended to fundamental, interactive, and critical dimensions.
What is new?
· The older adults had a low level of health literacy in Changsha of China, especially in interactive and critical dimensions.
· Multidimensional health literacy of the older adults was categorized into three profiles(low health literacy,moderate health literacy,and high health literacy).Age,residence,and education level were still the most significant factors influencing health literacy profiles.
· Health literacy’s potential importance and mechanism in promoting health-related behaviors should be taken seriously,which could potentially optimize the health outcomes in the elderly in China.
1.Introduction
The population aged ≥60 years had reached 18.1%, and those aged ≥65 years had reached 12.6%in China by the end of 2019[1],which means China has become one of the most aging countries globally.Aging is a significant risk factor for chronic diseases,which aggravates the disease process of the elderly, reduces their quality of life, and increases the economic burden on families and society[2-4].In this context,formulating a method to cope with the aging problem and achieve healthy aging has become urgent.
Health literacy is a considerable determinant of the elderly to manage their health.To the elderly,empirical evidence consistently indicated that low health literacy caused a high risk of chronic diseases, infection, poor self-management of diseases, and underutilized health services [5-7], ultimately burdening individual economies and national health systems.However, a national health literacy survey of 2020 in China showed that health literacy was only 8.5% in the age group of 60-69 years, far from a target level of 20.0% set in the “Healthy China 2030” [8].Therefore, carrying out interventions to improve the health literacy of the elderly has long been a question of great interest in the public health of China.
Before developing appropriate and effective interventions for older adults, we must entirely understand their health literacy status and associated factors.As a multidimensional concept,health literacy was defined as “the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health”by the WHO[9].It highlights interactive and critical health literacy, except for fundamental health literacy of reading and writing because of the failed expectation on health literacy interventions implemented in fundamental health literacy surveys [10].Many studies in China have shown that the influencing factors for low health literacy include gender,age,education background, income, occupation, etc.[11-13].Some studies focused on the positive influence of health literacy on healthrelated behaviors [14].However, instruments used in most studies of China focused on fundamental health literacy and had limitations to reflect the elderly’s characteristics in critical and interactive dimensions.The Chinese Citizens’ Health Literacy Questionnaire is the most widely used instrument with 66 items,which tests residents’basic knowledge,healthy behavior and skills of foundational health literacy [15].There are too many items in this scale, and there is no questionnaire specifically for the elderly in China at present.
In addition, what is noteworthy is that most studies on health literacy are limited to considering the influence of participants’age and residence.They mainly focused on wide age groups instead of solely on the elderly, with regional limitations [5,16].Moreover,existing research focused on analyzing the relationship between disease-specific health literacy and health behaviors[17,18].
The Rapid Estimate of Adult Literacy in Medicine and the Test of Functional Health Literacy in Adults commonly used abroad only tests writing and reading ability [19,20].Professor Osborne et al.[10]developed a multidimensional measurement tool named the Health Literacy Questionnaire (HLQ) in 2013 covering the WHO’s definition of health literacy.The questionnaire contains nine independent subscales based on data from general residents, clinicians,and policymakers following a validity-driven approach.It has been used in different samples in multiple countries to evaluate a profile of an individual's health literacy needs and strengths from nine dimensions.In China, a confirmatory analysis of the Chinese version of the HLQ showed that the scale had strong reliability and validity[21],and a study used it to investigate the health literacy of medical students in Chongqing,China[22].To our knowledge,it has not yet been applied to the Chinese elderly.
We used the HLQ to conduct a cross-sectional survey among elderly aged 60 and above in Changsha,China.The purpose of this survey was to assess the elderly’ health literacy from a holistic perspective and use latent profile analysis to identify different health literacy profiles in the sample.We also explore the associated factors of health literacy profiles and investigate the relationship between health literacy profiles and health-related behaviors.It is expected to provide a basis to comprehensively understand the health literacy of the elderly and formulate health promotion measures.
2.Methods
2.1.Study setting and participants
From June to August 2020, a cross-sectional survey was conducted in a community health center and a township health center in Changsha,Hunan Province,China.Participants aged 60 and over were invited to participate in the survey when they came to the health centers for the health examination.
Totally 488 respondents participated in the survey; 440 questionnaires were valid, with an effective rate of 90.2%.The participants were screened from people aged ≥60 years old who had registered residence in Changsha or had lived in Changsha for at least six months.Only those participating in the study voluntarily were included.Elderly individuals who were unable to communicate effectively or cooperate with the survey, such as poor mental health, difficulty speaking due to illness, or other reasons, were excluded from this study.
2.2.Variables and measures
2.2.1.Sociodemographic characteristics and health-related behaviors
Age,sex,residence,education level,whether living alone,health insurance status, diagnosis of chronic diseases, history of hospitalization in the past 12 months, and admission to emergency department in the past 12 months were collected.
Health-related behaviors were also assessed,including exercise,medical examination in the past 12 months,and timing of medical service-seeking behavior.The variable “Timing of medical serviceseeking behavior” refers to the time of actively seeking medical service with three options: “immediately” means seeking medical service once symptoms onset; “recurrently” refers to seeking medical service constantly as symptoms have occurred many times; “unbearably” stands for seeking medical service when symptoms are intolerable.
2.2.2.Multidimensional health literacy
We used the HLQ developed by Professor Osborne to measure participants’ multidimensional health literacy [10].Permission to use the tool was obtained from Professor Osborne.It consists of 9 subscales and 44 items.Each HLQ subscale can be used independently and has an independent structure; hence, the total score for the whole questionnaire is not calculated.The HLQ is divided into two parts.The first part contains 23 items contributing to 5 subscales, namely “feeling understood and supported by healthcare providers,”“having sufficient information to manage my health,”“actively managing my health,”“social support for health,”“appraisal of health information”; each item was assessed by a 4-point Likert scale from 1 =strongly disagree to 4 =strongly agree.In the second part,there are 22 items,which form the other four subscales,including“ability to actively engage with healthcare providers,”“navigating the healthcare system,”“ability to find good health information,” and “understand health information well enough to know what to do.”In this part,each item was evaluated with a 5-point Likert scale,with 1 equating to“cannot do or always difficult” and 5 meaning “always easy.”
2.3.Data collection
We trained five data collectors on the questionnaire’s content and skills of conducting a face-to-face questionnaire survey.An investigator screened the participants when the community provided free medical examinations for older adults.After obtaining the informed consent of participants,questionnaires were collected during one-to-one,face-to-face contact by other investigators.The survey was anonymous and voluntary.The communication time for each participant was 15-20 min.After completing the questionnaire, each participant received a food gift package valued at 30 CNY as time compensation.
2.4.Ethical consideration
Before the investigation started, it was approved by the Ethics Review Committee of Xiangya School of Nursing,Central South University(Approval No.E201913).The participants were explained with the purpose,content,confidentiality,benefits,and voluntary participation principle.Considering their age and education level,we only obtained the verbal consent of each participant to ease their burden.The survey also got the consent and cooperation of each survey site.
2.5.Data analysis
Data were analyzed by using SPSS Version 26.0 [23].Latent Profile Analysis(LPA)was conducted to identify sample scores of 9 HLQ domains into different subgroups,which was implemented by Mplus software (Version 7.0) [24].The optimal number of sample profiles was determined according to multiple model fit indices calculated from the 2-profile model to the 5-profile model.Explanation of Fit Indices as follows [25]: The smaller the value of the Akaike information criterion (AIC) and the Bayesian information criterion (BIC), the better the model fit, Entropy was used to evaluate the accuracy of model classification, Lo-Mendell-Rubin likelihood ratio test(LMR)and bootstrapped likelihood ratio test(BLRT)were used to compare the differences between different profiles models.The differences in the optimal potential profiles of sociodemographic data were analyzed using the Mann-Whitney U test.We chose ordinal logistic regression analysis to estimate the influencing factors associated with health literacy profiles.
The relationship between the health literacy profiles and healthrelated behaviors was analyzed using Pearson’s chi-squared test.The difference in the health literacy profiles within the same health-related behaviors subgroup was judged by the adjusted standardized residuals (ASR) using post-hoc testing.When the absolute value of the standardized residual is greater than 3, we considered the difference of health literacy profiles in the healthrelated behaviors subgroup to be statistically significant.
3.Results
3.1.Sample characteristics
The median age of the 440 respondents was 68 years (IQR 64-72).Table 1 displays the sociodemographic characteristics and health-related behaviors of respondents in detail.The proportion of respondents living in rural areas was 58.9%(259/440).The majority of respondents are women(61.4%,270/440).Most respondents only completed a junior-high-school education or below.About 70% of the participants reported being diagnosed with chronic diseases(67.3%, 296/440).
3.2.Scores of the HLQ subscale
Table 2 reports the mean score and standard deviation of each HLQ subscale.In the first part, “social support for health” was the highest score subscale (2.87 ± 0.40), and the lowest score was observed for the “appraisal of health information” subscale(2.22 ± 0.52).For the other four subscales, the highest and lowest scoring subscales were “ability to actively engage with healthcare providers” (3.21 ± 0.82) and “navigating the healthcare system”(2.89 ±0.81).
3.3.Profile analysis of the HLQ
Table 3 summarizes the fitting statistics of models with the different number of profiles for the HLQ latent profile analysis.The AIC and BIC values were constantly decreased from the 2-profile model to the 5-profile model, along with the number of profiles.However,the LMR values of the 4-profile and 5-profile models were not statistically significant, and their entropy values were smaller than the 3-profile model, which indicated that these two models were not superior to the 3-profile model.Thus,the 3-profile model was confirmed as the optimal latent profile model for our sample’s health literacy.The differences across the three profiles of each HLQ subscale are listed in Table 4.Profile 1 was named low health literacy(LHL) because it included relatively low HLQ scores in all 9 HLQ domains (n =108, 24.6%).By analogy, Profile 2 and Profile 3 were denominated moderate health literacy (MHL; n =174, 39.5%) and high health literacy (HHL; n =158, 35.9%).Across the three HLQ latent variables, the differences in the HLQ domain scores were statistically significant.Pairwise comparison of the three profiles in each subscale showed that the score of the HHL group was significantly higher than that of the MHL group (P <0.001), and that of the MHL group was significantly higher than that of the LHL group(P <0.001).
3.4.Analysis of associated factors of health literacy profiles
Table 5 details the differences in health literacy level between subgroups based on the sociodemographic characteristics of respondents.We performed an ordinal polytomous logistic regression analysis taking sociodemographic variables with statistically significance as independent variables, and health literacy profiles as dependent variables.Table 6 reports the statistically significant results.This method was utilized because the results of the parallel line test were χ2=7.22,P =0.614,indicating that the proportional odds hypothesis existed.The table displays that the independent factors relating to the health literacy profiles of the sample were age, living in a rural area, completed secondary education, and having health insurance.Specifically, respondents aged 60-74 years had a higher health literacy level than those aged 75 years and above (OR =2.06, 95% CI: 1.23-3.42, P =0.006).The health literacy level of respondents living in urban areas was higher thanthose living in rural areas(OR =3.28,95%CI:2.17-4.94,P <0.001).The probability of having a better health literacy level was 2.86 times (95% CI: 1.92-4.27, P <0.001) higher in the group having completed secondary education than those who did not.Respondents with health insurance had a higher health literacy level than those without health insurance(OR =1.89,95%CI:1.02-3.51,P =0.042).
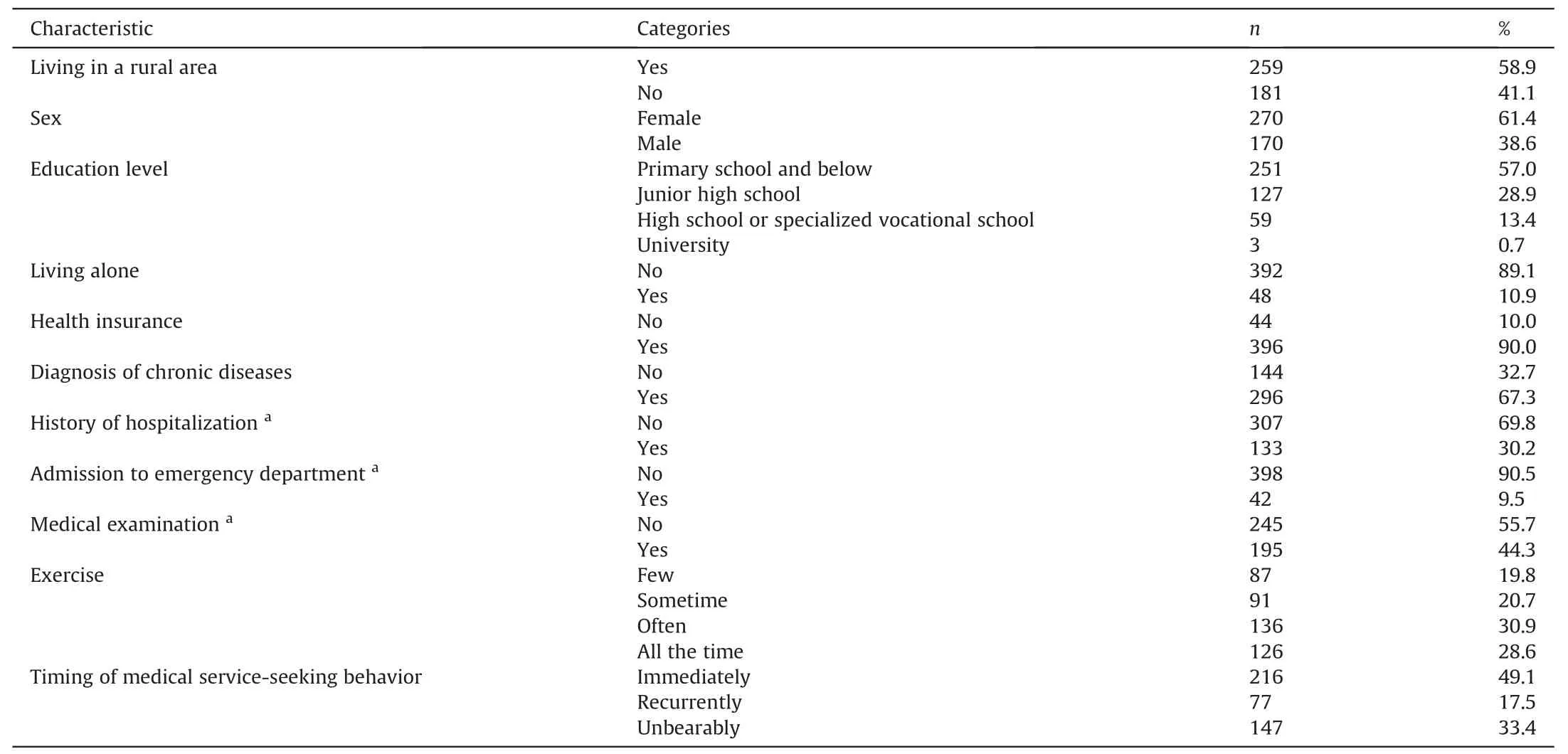
Table 1Sociodemographic characteristics and health-related behaviors of the sample (n =440).

Table 2The score for each HLQ subscale (n =440).

Table 3Fit statistics of Latent Profile Analysis of HLQ (n =440).
3.5.Association between health-related behaviors and health literacy profiles
Statistically significant associations were found between health literacy level and health-related behaviors, including timing of medical service-seeking behavior(χ2=25.14,P <0.001),exercising regularly(χ2=34.08,P <0.001),and taking a medical examination in the past 12 months (χ2=24.76, P <0.001) by Pearson’s chisquared test showed in Table 7.Table 7 also lists the results of the post-hoc test.For timing of medical service-seeking behavior, respondents choosing “recurrently” were more likely to be at a low health literacy level (ASR =4.4), were least likely to be at a high health literacy level (ASR =-3.0).Respondents in the “immediately”subgroup were less likely to be at a low health literacy level(ASR =-3.8).Moreover, associations between the choice of “unbearably”and the three health literacy profiles,between the choice of “immediately” and medium or high health literacy, were not statistically significant.In terms of the“exercise regularly”variable,the ASR was significant for exercising regularly and high health literacy level(ASR =5.0),and exercising irregularly and low healthliteracy level (ASR =4.8).For the option“take a medical examination in the past 12 months”,the ASR showed statistically significant associations between “not take a medical examination in the past 12 months”and“low health literacy”profile(ASR =4.0),and“take a medical examination in the past 12 months” and “high health literacy” profile (ASR =4.4).

Table 4Differences across profiles on the HLQ domains (n =440).

Table 5Sociodemographic characteristics of the three profiles and their differences (n =440).

Table 6Ordinal logistic regression analysis of sociodemographic data and three profiles (n =440).
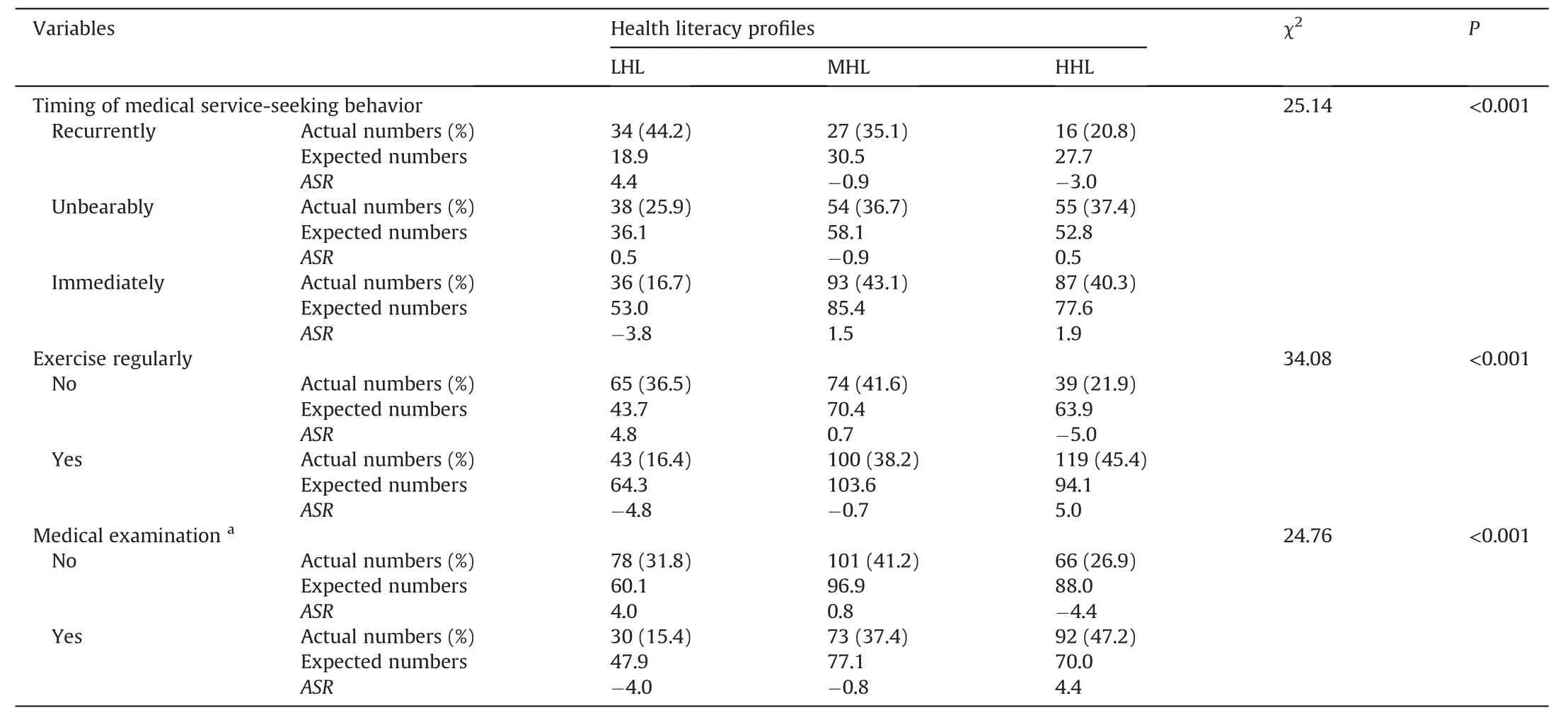
Table 7Associations between health-related behaviors and health literacy profiles (n =440).
4.Discussion
As far as we know,it might be the first study to catch the broad elements of health literacy’s definition to measure the health literacy status in China’s elderly using a multidimensional health literacy questionnaire.We used latent profile analysis to transform their health literacy into a 3-profile model.Based on the model,the survey showed that health literacy in the sample was associated with age, residence, and education level.Moreover, we observed differences in health literacy and health-related behaviors.
4.1.The distribution characteristics of health literacy
Although no critical value is used to determine poor health literacy using the HLQ, these results revealed some health literacy limitations among the elderly.The scores were not evenly distributed in each HLQ domain in our survey.On the first five subscales,the two subscales with the lowest scores were the “appraisal of health information”subscale and the“actively manage my health”subscale.It indicates an inability to understand health information and identify reliable information by themselves.Even they neglect their health status and take a passive attitude to decide their health[10].On the latter four subscales, the elderly scored lowest in“navigating the healthcare system,”reflecting that individuals have problems finding essential health services and information independently and actively and using the associated system [10].Collectively, low scores on those subscales identified the elderly have more interactive and critical health literacy limitations tohinder their access to vital health support for their health needs.However, few studies of older adults in China have noted the importance of interactive and critical health literacy.Therefore,with the extension of health literacy to more dimensions, further study on multidimensional health literacy is suggested.
By contrast, participants got a better score in the subscales of functional health literacy“ability to find good health information,”“having sufficient information to manage my health,” and “understanding health information well enough to know what to do.”[10]In other words,they are able to read or write health information to manage their health with others'help,which was the topical issue in most previous studies.However,the fundamental health literacy subscales scores among this sample were relatively low compared with scores of old Australian adults in Beauchamp’s study [26]using the same tool.Thus,the elderly in our survey are still at a low health literacy level,and they are not confident to have and utilize all the health-related information and services needed independently.
4.2.Associations among health literacy profiles and sociodemographic characteristics
After our study divided health literacy into three profiles (low health literacy, moderate health literacy, and high health literacy),further analysis found that age,residence,and education level were associated with health literacy profiles.Although using different instruments to measure health literacy, literature has proved a similar result that better sociodemographic status positively influenced health literacy in the elderly[18,27-29].Some potential mechanisms can explain the relationship.In terms of age, researchers have reported that health literacy changes dynamically with age;the cognition of health-related information of the elderly declines year by year [30].As for education level, it is mentioned that a person with higher education level is more capable of finding, understanding, and judging health-related information and interacting with health providers [31,32].Moreover,considerable differences in economy, education, and geography between urban and rural areas may be the barrier for the elderly to utilize health-related resources [33].Therefore, it is not surprising to identify that older adults living in rural areas have lower health literacy than those living in urban areas.
Given all these,sociodemographic status may contribute to low health literacy.Despite the rapid development of digital medicine and internet-based health information, traditional media such as TV are still the primary way to obtain and utilize health information for the elderly [34].They have little confidence in coping with complex electronic health information systems, especially distinguishing and utilizing digital health services, which may be partly responsible for the low health literacy of this group of older adults.Considering the immutable nature of the sociodemographic background and the growing popularity of digital medical technology, we must guarantee the feature of elderly orientation, both in operating technology and the presentation of health information content.Traditional medical services need to be appropriately maintained in rural areas while developing intelligent medicine,including face-to-face health education.
An interesting finding in our study was that having confirmed chronic diseases was not an independent risk factor for the health literacy of the elderly.It is different from the finding that people with four or more chronic diseases were more difficulties in good health literacy in Beauchamp’s study of adults using the same HLQ questionnaire [26].A study conducted in Hangzhou, China, can explain the difference.It concluded that the relationship between chronic disease-related conditions and health literacy was mixed,affected by the disease type,number of diseases,and age[33].Since our research is a local cross-sectional study, this result should be interpreted with caution.
4.3.Relationships among health literacy profiles and health-related behaviors
Our results indicated the reciprocal relationship between health literacy profiles and health-related behaviors.We found that respondents who regularly exercise and take medical examinations had a higher health literacy level.Similarly, respondents sought medical treatment immediately when symptoms onset was related to high health literacy levels.These results are in agreement with the findings fromthe elderlyin Xinjiang,China[35].However,the health literacy level had no associationwith the mediocre timingof medical help-seeking behavior.Evidence showed that it might be because the timing of medical service-seeking behavior is a complex behavioral habit affected by own attitudes and recognization of disease and accessibility of medical services [36].A systematic review of qualitative evidence revealed that interventions in the community improving health literacy might be able to promote health-related behaviors[37].Therefore,we should take the impact of health literacy on health-related behaviors seriously and improve the elderly’s health literacy through community-based health education interventions.We also suggest tech-back method should be used to promote the efficacy of interventions in the elderly[38].
4.4.Limitations
Our survey has several limitations.First,due to the early stage of COVID-19 containment and limited time for the survey, a nonrandom sample might lead to a selective basis.Additionally,those elderly excluded from this study due to unable to communicate effectively or cooperate with the survey might have lower health literacy.Second, a cross-sectional survey limited the causal inference of results.Third, the research site was only set in two health care centers in Changsha, so the results limited the generalization of the findings.
5.Conclusions
This survey revealed a low level of health literacy dimensions in older adults, especially dimensions about interactive and critical health literacy.It demonstrated the advantage of the multidimensional instrument for health literacy in understanding the weak domain and needs in the current health literacy of the elderly.This survey showed that the elderly’s health literacy profiles are associated with sociodemographic background because of the development of internet-based health information.Furthermore, the findings support the potentially important role of health literacy in promoting health-related behaviors,providing further guidance for community-based health interventions and policy development to improve health literacy to optimize the health outcomes in the elderly in China.
CRediT authorship contribution statement
Ying Xie:Conceptualization, Methodology, Formal analysis,Investigation, Writing-original draft, Writing - review & editing.Wenhong An:Data curation, Supervision, Writing-review & editing.Chunyuan Zheng:Investigation, Writing-review &editing.Di Zhao:Investigation, Writing-review & editing.Honghong Wang:Conceptualization, Methodology, Project administration, Writingreview &editing.
Funding
This study was funded with the Hunan Key Laboratory Platform for Nursing (2017TP1004).The funding provided assistance in the questionnaire collection process and the language editing service of the manuscript.
Declaration of competing interest
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
The authors appreciate all the health providers and participants in the two health centers for their participation and research group members' help in data collection.We also would like to thank Professor Osborne and his team for authorizing the use of the HLQ scale.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.02.007.
 International Journal of Nursing Sciences2022年2期
International Journal of Nursing Sciences2022年2期
- International Journal of Nursing Sciences的其它文章
- Brief Introduction on the Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity
- Subscription of International Journal of Nursing Sciences
- Development and evaluation of a teamwork improvement program
- Recognition of group activities for understanding intraoperative state of surgical team
- Association of operating room costs with head and neck surgical instrumentation optimization
- Editorial Board of International Journal of Nursing Sciences