
Unicentric Castleman disease was misdiagnosed as pancreatic mass:A case report
2022-03-15 07:12:08HongYanZhaiXinYuanZhuGuiMingZhouLiZhuDanDanGuoHaoZhang
World Journal of Clinical Cases 2022年4期
INTRODUCTION
Castleman’s disease (CD) is a lymphoproliferative disorder of unknown cause and is rarely seen clinically.The pathological features are obvious proliferation of lymph follicles,blood vessels and plasma cells.CD is divided into two main types:Unicentric CD (UCD) and multicentric CD (MCD).UCD occurs as a solitary enlarged mass and mediastinal lymph nodes are the most commonly affected.Surgical excision has proven to be curative for UCD.MCD appears as a systemic disease with peripheral lymphadenopathy.MCD has a poor response to surgery and monoclonal antibodies with rituximab have become a research hotspot.Here,we present a 40-year-old woman with characteristic clinical,radiological and histological findings of UCD,demonstrating an incidental retroperitoneal mass misdiagnosed as pancreatic tumor.
CASE PRESENTATION
Chief complaints
A 40-year-old woman presented to the ultrasound department of our hospital complaining of a pancreatic mass found by physical examination.She came to our hospital to clarify the diagnosis.She had no obvious conscious symptoms,such as fever,abdominal pain,abdominal distension,or jaundice.
But as all his courtiers were watching him he did not like to make any more objections19, and ordered the floor to be taken up, as the young man desired
History of present illness
The patient had no obvious conscious symptoms,such as fever,abdominal pain,abdominal distension,or jaundice.
History of past illness
The patient had no previous medical history.
Personal and family history
CD is a lymphoproliferative disorder of unknown cause and is rarely seen clinically.The pathological features are obvious proliferation of lymph follicles,blood vessels and plasma cells.Clinically,it is characterized by significant enlargement of deep or superficial lymph nodes.Since its first recognition in 1956[1],understanding of CD has improved after segregation of UCD and MCD,showing distinctive prognosis and treatment approaches.
We had been to many University of Louisville basketball games and even a few University of Kentucky games in this hallowed hall, but the anticipation2 of seeing Michael Jordan and the Chicago Bulls against the Washington Bullets (with ex-University of Louisville star Felton Spencer) made our pace across the massive parking lot seem like a quick one, with lots of speculation3 about how the game was going to go
Physical examination
The patient’s temperature was 36.6 °C,heart rate 73 bpm,respiratory rate 16 breaths/min,blood pressure 120/70 mmHg and oxygen saturation in room air 98%.Clinical abdominal examination did not reveal any positive signs.Our clinical considerations were benign or malignant tumor of the pancreas.
Laboratory examinations
Blood analysis showed normal prothrombin and partial thromboplastin times and Ddimer level.Urinalysis was normal for a-fetoprotein,ferritin,carcinoembryonic antigen,carbohydrate antigen-199,sugar chain antigen as well as human epididymal epithelial secretory protein.
Didn t she know me? the little soldier asked himself, or was she angry because I missed our meetings? and he followed the crowd till he got to the palace
Imaging examinations
As soon as the Wolf had uttered these words, he beat his paw against the damp ground and instantly he took the shape of the Tsar s beautiful daughter: so like to her that no one in the world could have told that he was not the Tsarevna herself. Then, bidding Helen the Beautiful wait for him outside the walls, Tsarevitch Ivan led the Gray Wolf into the Palace to Tsar Afron.
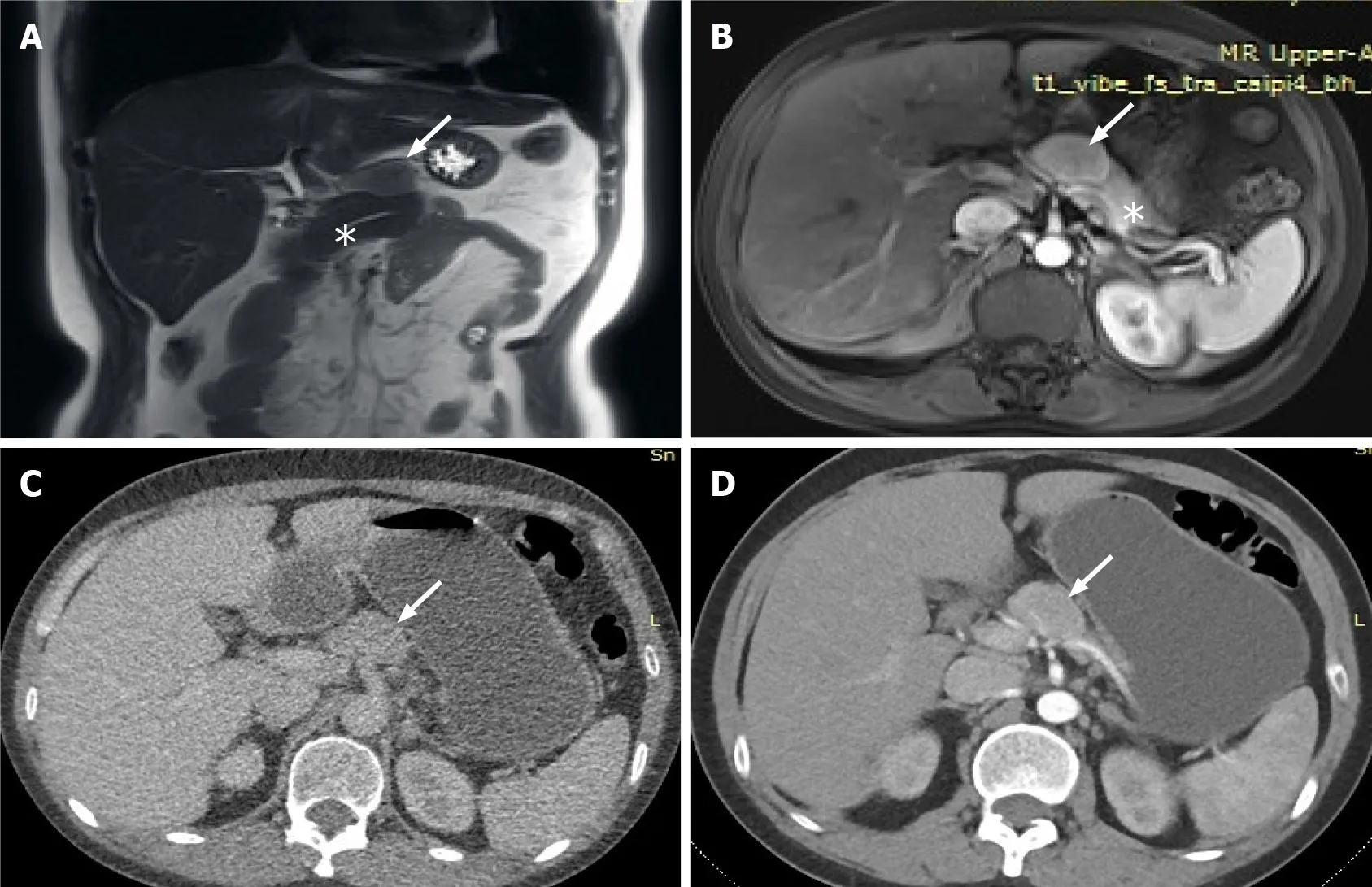
The lesion was further evaluated by computed tomography (CT) and magnetic resonance imaging (MRI).CT revealed a mixed density nodule located above the pancreatic body that was convex and shallowly lobulated,showing uneven progressive enhancement,and the degree of enhancement in each stage was lower than that of pancreatic parenchyma (Figure 2).MRI revealed an isointense lesion located above the pancreatic body that was clearly separated from the normal pancreas.The edge was enhanced in the arterial phase,and the degree of internal enhancement in each phase was lower than that of the pancreatic parenchyma.As most pancreatic adenocarcinomas have poor blood supply,they usually display low enhancement on arterial phase of enhanced images.However,the lesion in this case showed rich blood supply on CEUS,enhanced MRI,and enhanced CT,so pancreatic adenocarcinoma was ruled out.Therefore,we believed that the abnormal enhancement of the upper part of the pancreatic body was a solid pseudopapillary tumor or a neuroendocrine tumor.
Further diagnostic work-up
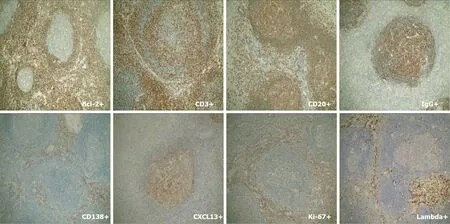
Mass resection was performed and histological examination revealed lymphoid tissue proliferation,with lymphoid follicular hyperplasia,mantle hyperplasia,interfollicular plasma cell hyperplasia,and local vascular hyperplasia (Figure 3).Plasma cells showed strong immunostaining for CD138 and IgG.IgG4 was occasionally positive and the expression rate was<40%.No restrictive expression of kappa and lambda was observed.B and T cells were positive for CD20 and CD30.CD21 and CD23 showed the follicular dendritic cell network.Germinal center cells were positive for Bcl-2,and weakly positive for CD10 and Bcl-6.Cxc113 and cyclin D11 were positive in a few scattered cells.Ki-67 was highly expressed in germinal centers (Figure 4).These results gave the most likely diagnosis as CD.
The incidence and prevalence of CD has become difficult to evaluate due to its rare occurrence in the general population,and it affects both sexes equally[2].UCD is usually found to have a peak incidence in the second to fourth decades of life[3].In most cases,UCD occurs as an isolated mediastinal lymph node enlargement.Patients present with a single lymph node with painless enlargement and slow growth,ranging from several centimeters to approximately 20 cm in diameter.Mediastinal lymph nodes are the most commonly affected,followed by cervical,axillary and abdominal lymph nodes.Occasionally,they are found in external tissues such as larynx,vulva,pericardium,subcutaneous muscle,lung,and orbit,as well as intracranially.Most patients have no systemic symptoms and a few complain of cough,dyspnea or other constitutional symptoms.Patients can survive for a long time after tumor resection,which is a benign course of disease.
FINAL DIAGNOSIS
All the examinations failed to give a definitive diagnosis;therefore,the patient underwent surgery.During the surgery,we observed a 3 cm × 2 cm mass above the pancreatic body,with a clear boundary and tough texture,located anterior to the bifurcation of the splenic artery and the common hepatic artery,pushing the upper edge of the pancreas interior to it.Careful separation of the adhesion between the tumor and the surrounding tissues along the surface of the tumor ensured that the tumor was well demarcated from the pancreas.

TREATMENT
The patient had an uneventful postoperative clinical course.Two months after surgical removal of the mass,the patient was asymptomatic,and a new MRI scan showed complete removal of the tumor.
OUTCOME AND FOLLOW-UP
The patient underwent surgery to remove the mass located above the pancreatic body.
DISCUSSION
The patient had no personal or family medical history.
I advise you to do what you think will turn out to yourhappiness, said the girl. Be kind and good to her, but rememberthis; from the hour we part we shall never see each other again. Years passed; then one day she met the old friend and sweetheartin the street; he looked ill and miserable15, and she could not helpasking him, How are you?
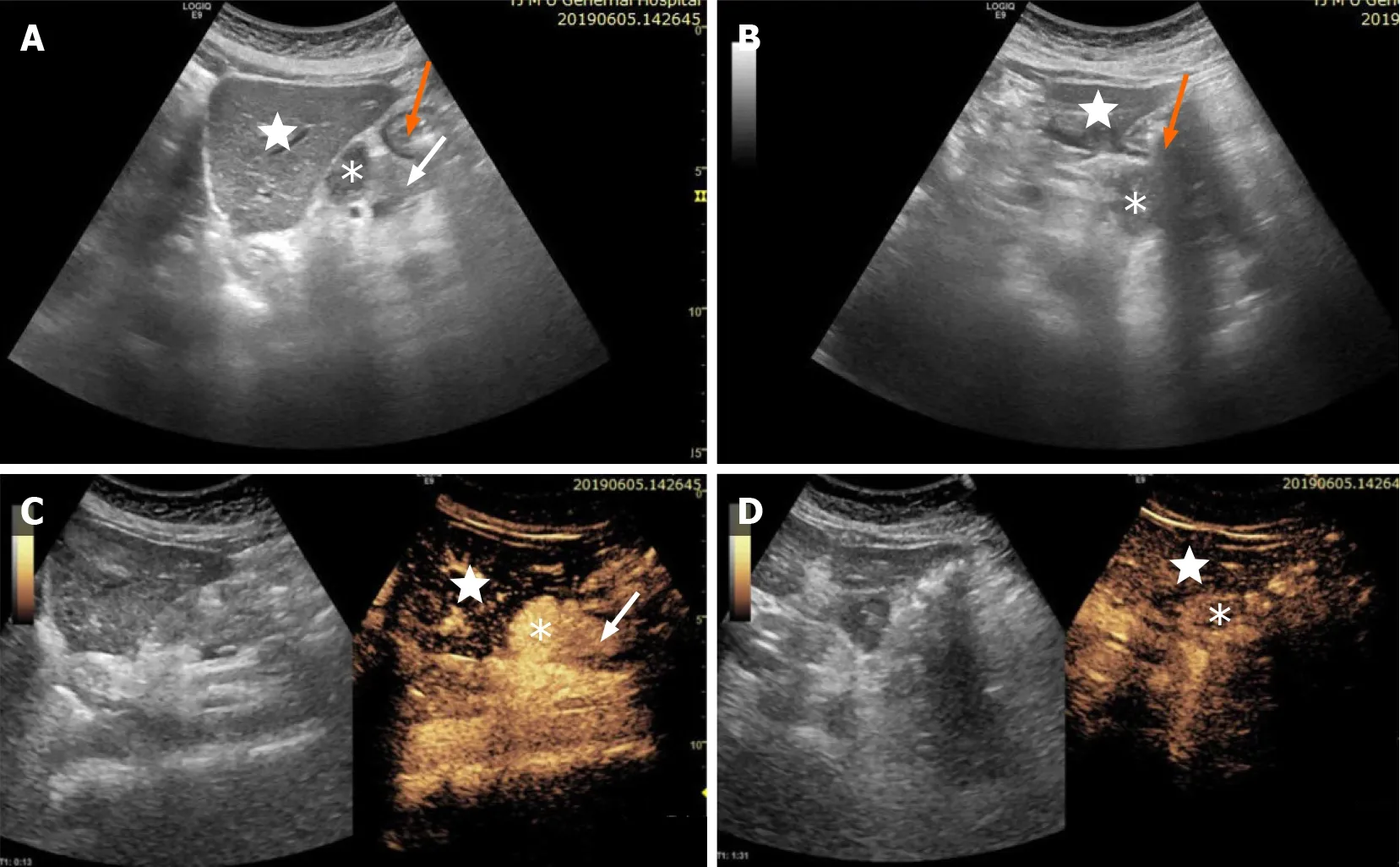
Initial imaging with conventional ultrasound (US) examination,revealed a 3.2 cm × 2.5 cm hypoechoic mass between the body of the pancreas,left lobe of the liver and stomach,with clear boundaries,irregular shape,uneven echoes,and no obvious blood flow signals.In order to make a diagnosis,the patient underwent contrast-enhanced US (CEUS) examination.CEUS showed hyperenhancement of the lesion in the arterial phase,and slightly high enhancement in the venous phase.CEUS suggested differential diagnosis of benign pancreatic tumor,neuroendocrine tumor or solid pseudopapillary tumor,but the possibility of tumor in other organs could not entirely be excluded (Figure 1).
MCD is rarer than UCD and tends to present later in the sixth and seventh decades.MCD has a constellation of systemic symptoms with peripheral lymphadenopathy involving multiple compartments throughout the neck,chest,abdomen and pelvis.It also has an association with human immunodeficiency virus and human herpesvirus-8 infections[4,5].In a few patients,multiple neuropathy,organ enlargement (liver and spleen),endocrine disease,serum immunoglobulin and skin disease were found simultaneously.MCD often presents with an invasive venereal course that is accompanied with infection.
Frizzera[6] proposed the diagnostic criteria of CD (Table 1).It should be pointed out that it may be difficult to make a definite and accurate clinical pathological diagnosis based on histopathology or clinical manifestations alone,and the two must be combined,especially for MCD.

The differential diagnosis of CD includes lymphoma and any other causes of lymphadenopathy.Initial investigations encompasses a CT scan that reveals the location,extent and number of lymph nodes involved,which are then visualized with homogeneously intense contrast enhancement[7].MRI and positron emission tomography/CT[8] can be used to clarify the involvement of any soft tissues.Due to the diversity of the clinical and pathological manifestations of CD,sometimes it is difficult to distinguish from scrofula,malignant lymphoma,mediastinal neurogenic tumor (ectopic paraganglioma),ectopic gland tumor,connective tissue disease,blood vessels and immune cell lymphadenopathy[9,10].When patients present with lymph node enlargement,we should think of CD,and excisional biopsy is usually required to establish the final diagnosis.Combining medical history,physical examination,laboratory examination and pathological examination,it is important to initially rule out diseases of known cause.
In the present case,the patient was initially misdiagnosed with a pancreatic tumor by enhanced CT,enhanced MRI and CEUS.Based on CEUS,we highly suspected that the mass might be derived from the pancreas,and/or it might be a tumor from other parts of the body.We initially differentiated the diagnosis between benign and malignant lesions.The pancreatic adenocarcinoma usually present hypoenhancement on arterial phase of CEUS.Patients with focal pancreatitis have symptoms of upper abdominal pain and digestive systems,and the enhancement of focal pancreatitis was similar to normal pancreatic parenchymas,and most of them were overall isoenhancement of synchronization.Patients with functional pancreatic neuroendocrine tumors have corresponding symptoms,even non-functional pancreatic neuroendocrine tumors have abundant blood vessels.Pancreatic adenocarcinoma is characterized by high enhancement in the arterial phase of CEUS,which occurs earlier than in normal pancreatic parenchyma,with high enhancement or equal enhancement in the venous phase[11].Solid pseudopapilloma has different proportions of cystic and solid components.Those with the dominant solidity may show significantly high enhancement in the arterial phase of CEUS,but subsided enhancement in the venous phase.Based on the above performance,the contrast enhancement mode of the mass in the present case was most consistent with a pancreatic neuroendocrine tumor and a solid pseudopapilloma.However,the enhancement pattern of this case was not exactly consistent with pancreatic tumors.The patient had no symptoms,and the boundary of the tumor was clear,which led us to confirm whether it was not a tumor of the pancreas.Therefore,MRI was recommended for further diagnosis.Because MRI has high accuracy in diagnosing pancreatic tumors[12],patients with an early diagnosis of non-functioning well-differentiated neuroendocrine carcinomas of the head of the pancreas using MRI have a good outcome.
Surgical excision has proven to be curative for UCD.Just like the patient in our manuscript,in some reports[13-15],no recurrence was found either clinically or radiologically that underwent surgical excision.Moreover,surgical excision was seen to decrease the mortality rates (17.6% to 3.8%) in UCD in a systematic review of 404 published cases[2,16].In contrast,MCD had a poor response to surgery and worse prognosis when compared to UCD.MCD does not have a proven treatment regimen.Multicentric type is ineffective after surgery,the prognosis is poor,and the median survival time is about 14-30 mo;Severe infections,multiple organ failure,and transformation to malignant tumors are the main causes of death in such patients.However,monoclonal antibodies,anti-IL-6 receptor monoclonal antibodies or chemotherapy with rituximab has have become a research hotspot[17-19].
Trint felt sorry for the boy. He looked like he was around eight years old, and no kid should have to spend Christmas Eve in a truck stop. The parents were loading up on coffee and Trint guessed they d been driving somewhere to spend the holidays with relatives, and the snow forced them to hole up here. They were drinking coffee hoping to stay awake so they could finish their trip if the weather cleared up.
CONCLUSION
CD is a lymphoproliferative disorder and is rarely seen clinically.The pathological features are obvious proliferation of lymph follicles,blood vessels and plasma cells.CD divided into unicentric and multicentric types.UCD occurs as a solitary enlarged mass and shows a benign disease course.Surgical excision has proven to be curative.MCD presents as a systemic disease with peripheral lymphadenopathy and has a poor response to surgery.When patients with lymph node enlargement are encountered clinically,we should consider CD,and excisional biopsy is usually required.It is particularly important to first rule out diseases that are known causes of lymphadenopathy.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report