
Doctor-led intensive diet education on health-related quality of life in patients with chronic renal failure and hyperphosphatemia
2022-03-15 07:11:56XianDongFengXueXieRuiHeFangLiGuiZhongTang
World Journal of Clinical Cases 2022年4期
INTRODUCTION
Chronic renal failure is the final stage of kidney disease wherein renal function in patients is almost lost.Therefore,maintenance hemodialysis is needed for renal replacement therapy.Hyperphosphatemia,which is related to renal dysfunction and endocrine changes,is a common complication during treatment[1-4].The lack of knowledge about hyperphosphatemia in patients with chronic renal failure on hemodialysis affects their rational diet and medication according to doctor 's advice,which directly causes the continuous increase of blood phosphorus levels.Therefore,health education during treatment is necessary[5].At present,the nursing staff is mostly responsible for the health education of patients.Communication and interaction between doctors and patients is limited,and the content of health education may be poorly remembered.Doctor-led health education can improve the interactions between doctors,nurses,and patients and has a good intervention effect on multiple lifestyle-related diseases[6].This study observed the effect of doctor-led intensive diet education on health-related quality of life in patients with chronic renal failure and hyperphosphatemia.
MATERIALS AND METHODS
Baseline data
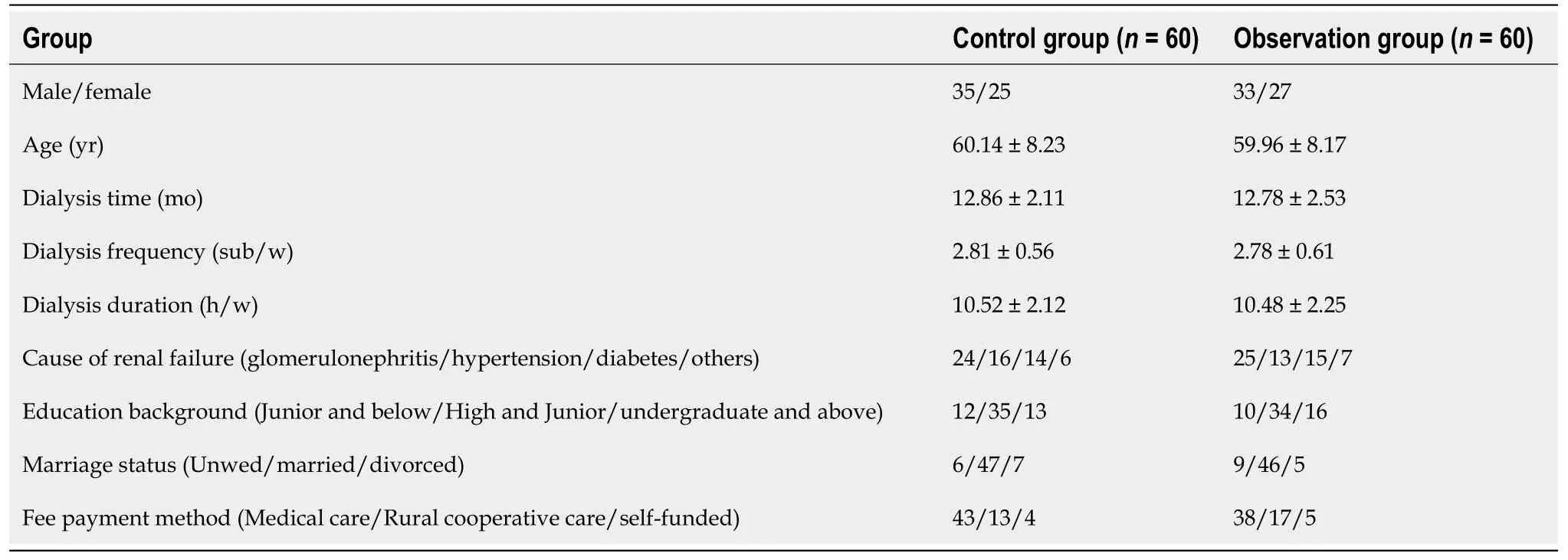
A total of 120 patients with chronic renal failure and hyperphosphatemia on hemodialysis who were admitted to our hospital between July 2018 and March 2020 were selected as the research subjects.There were 67 male and 53 female patients;their ages ranged from 42 to 70 years,with an average age of 60.25 ± 7.85 years.According to the treatment method,patients were divided into two groups with 60 patients each.As shown in Table 1,no significant difference (>0.05) was reported for the general data comparison.
Inclusion and exclusion criteria
Inclusion criteria for our study were defined as follows.(1) In line with the standard of chronic renal failure[7];(2) Blood phosphorus was≥1.78 mmol/L while phosphate binders were taken;(3) Age was≥18 years but ≤ 70 years;(4) Expected survival period was>6 mo,the disease was relatively stable,and patient’s understanding ability was good (,the ability to cooperate with the treatment and curative effect evaluation);(5) Hemodialysis treatment was for≥6 mo;and (6) Complete clinical data was available.
Patients were excluded if they had:(1) Chronic renal failure combined with heart failure,severe infection,malignant tumor,or other serious complications;(2) Central nervous system diseases,infectious diseases,or severe depression and anxiety;or (3) A history of diseases that could affect calcium (Ca),phosphorus (P),and parathyroid hormone (iPTH) metabolism.
Methods
The control group was given routine health guidance and publicity materials,such as the Handbook of Health Education for Dialysis Patients.The educational topics reviewed with patients included the causes of hyperphosphatemia in patients on hemodialysis,its clinical manifestations,hazards,treatment drugs,medication precautions,common phosphorus-rich foods,methods to reduce phosphorus intake in the diet,and common food phosphorus/protein ratios.Nursing staff carried out oral education during hemodialysis.
The observation group was given doctor-led intensive diet education on the basis of the control group,and the intensive health instructors included bed doctors and responsible nurses.Doctors gave lectures regularly and organized patients to carry out centralized education,consistent with the Handbook of Health Education for Dialysis Patients.Doctors used common pictures of high phosphorus foods in the form of slides and oral lectures to enhance the understanding and memory of patients and their families.Doctors described ways to reduce phosphorus intake in patients’ daily diets and guidelines for cooking.Types of common phosphate binders,methods of intake,and associated precautions were also introduced.According to the patients’ conditions,examination results,complications,,personalized diet guidance was given to encourage patients to ask questions and to answer patients’ questions in detail.A Diet Diary was issued,and patients were asked to record the type and quantity of food consumed for 3 consecutive days.In accordance with their entries,the problems existing in patients’ diets were understood and corrected.
“Is it possible?” said the lord-in-waiting, “I never imagined it would be a little, plain, simple thing like that. She has certainly changed color at seeing so many grand people around her.”
Indices
The changes in EQ-5D-3L scores,disease-related knowledge,and compliance scores before intervention and 3 and 6 mo after intervention in the two groups were recorded.The levels of serum iPTH,Ca,P,calcium-phosphorus product (Ca × P),serum creatinine (Scr),and blood urea nitrogen (BUN) before intervention and 3 and 6 mo after intervention in the two groups were detected,and the satisfaction of the two groups was statistically analyzed.
Hyperphosphatemia is a common metabolic comorbidity in patients on hemodialysis that can stimulate iPTH secretion,aggravate mineral metabolism disorders,cause renal bone disease and skin itching (pruritus),and increase the risk of cardiovascular disease[9].At present,the clinical treatment of hyperphosphatemia in patients with chronic renal failure mainly proceeds from hemodialysis,the use of intestinal phosphorus binders,and restriction of dietary phosphorus intake[10].
Detection method
The venous blood of patients under a fasting state and before dialysis was collected before intervention and 3 and 6 mo after intervention.The blood was centrifuged at 3500 r/min for 10 min.Serum was used to detect iPTH with a chemiluminescence immunoassay analyzer (Roche,E601).The blood Ca,P,Scr,and BUN levels were detected using the 7600 automatic biochemical analyzer and its supporting reagents from Hitachi,Japan.Serum Ca × P levels were subsequently calculated.
Evaluation standard
In this study,the blood iPTH,Ca,P,and Ca×P levels of those who received doctorled intensive diet education interventions for 3 and 6 mo were lower than those of patients who received conventional nursing interventions;patient satisfaction of the former group was also higher.However,the levels of Scr and BUN in the two groups were similar.This result suggests that doctor-led intensive diet education can ameliorate the state of Ca and P metabolism disorders in patients with chronic renal failure and hyperphosphatemia and boost patient satisfaction.However,doctor-led intensive diet education does not affect renal function.This result is essentially consistent with the conclusions of the extant research[15-18] and can be explained by the notions that patients often have better compliance with doctors' requirements,and doctors provide patients with more comprehensive knowledge of dietary phosphorus limits,through more intuitive and specific education models.
Patients’ compliance scores were assigned based on a self-administered questionnaire and evaluated on a 100-point scale.The higher the score,the better the patient’s compliance.
Similarly,patient satisfaction was determined using the self-administered questionnaire and evaluated on a 100-point scale.A total score 90 was indicative of a rating of “very satisfactory”.The total score was 70-90.A total score<70 indicated a patient rating of “not satisfactory”.
Statistical analysis
SPSS Statistics 19.0 software was used to process the data.Measurement indicators were described by mean ± SD.Independent sample-test was used to compare data between groups,paired-test was used to compare data within groups,and thetest was used to compare count data.Avalue of less than 0.05 was statistically significant.
RESULTS
Comparison of blood iPTH,Ca,P,and Ca × P levels between the two groups
Although increasing the frequency and duration of dialysis and taking intestinal phosphorus binders can reduce the amount of phosphorous in the blood to a certain extent,such activities still may not work to maintain blood phosphorus within the normal range.Correct diet control is of great importance to reduce blood phosphorus levels[11].However,most patients lack the knowledge of diet control and cannot achieve satisfactory self-management results.Under conventional intervention methods,the nursing staff is mostly responsible for health education,and measures such as the distribution of publicity materials and oral education between diagnosis and treatment are adopted.However,because of the differences in patients’ understanding capability and educational level,the effect of health education is not ideal[12].
Comparison of renal function indices between the two groups
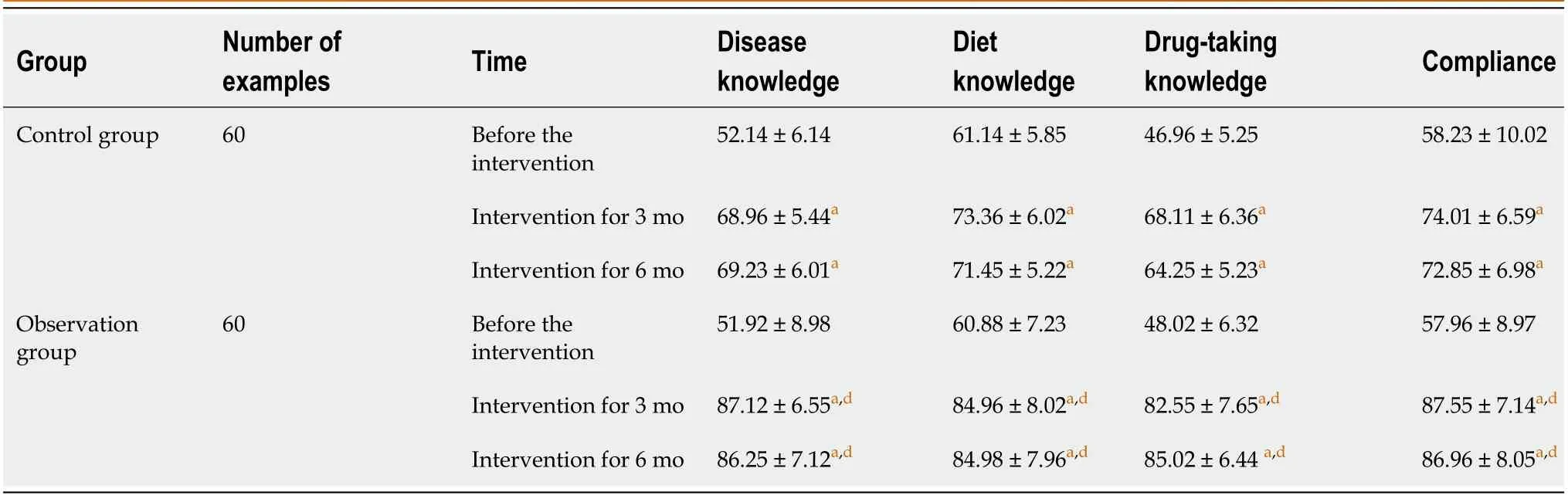
There was no significant difference in disease-related knowledge or compliance scores between the two groups before intervention (>0.05).After 3 and 6 mo of intervention,the scores of disease,diet,and medication knowledge and compliance in the two groups increased gradually (<0.05).Further comparison revealed that the scores of disease-related knowledge and compliance in the observation group were higher than those in the control group (<0.05) (Table 6).
Comparison of satisfaction between the two groups
Doctor-led intensive diet education is based on regular health education with doctor interventions,regular lectures,and face-to-face health education with patientsa combination of slides,oral lectures,and pictures to strengthen patients' disease-related knowledge.This approach can also offer personalized dietary guidance according to the specificities of patients’ situations.Patients can be instructed to make a Diet Diary,based on which problems can be found and corrected.Doctor-led intensive dietary education can enable patients to grasp disease-related knowledge and control their diets[13,14].

Comparison of EQ-5D-3L score between the two groups
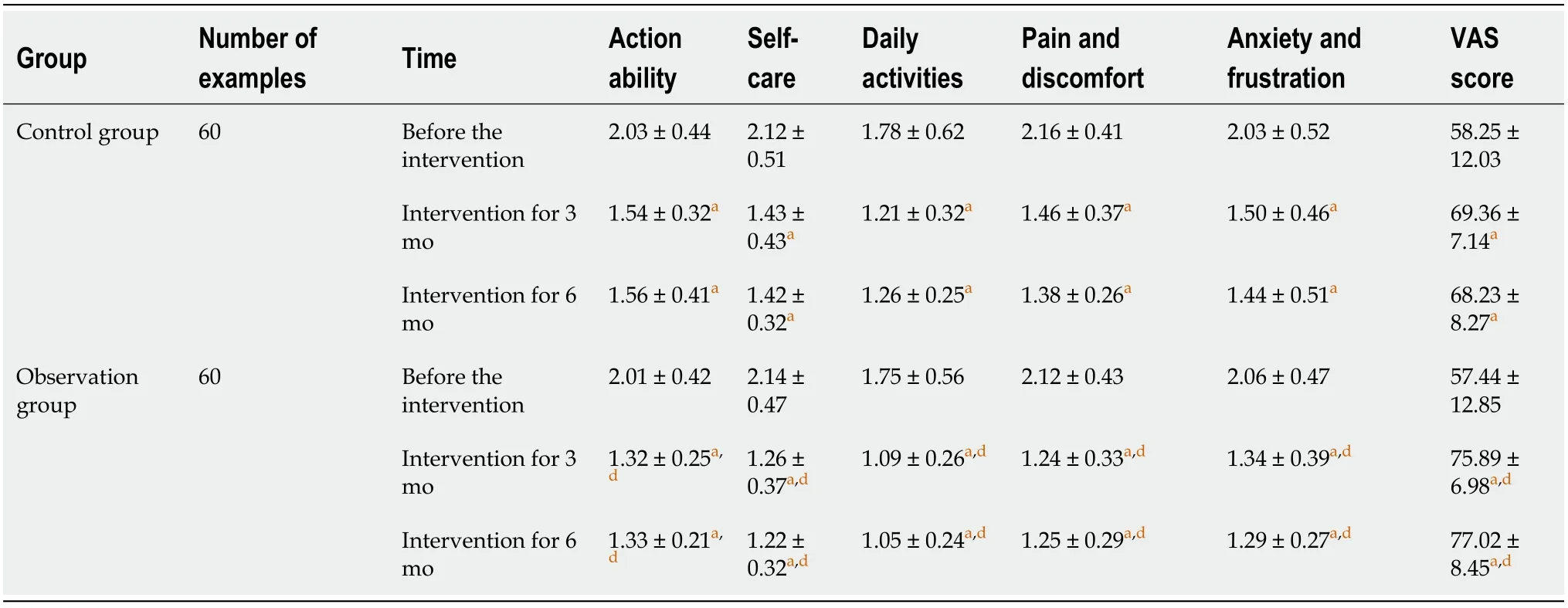
There was no significant difference in EQ-5D-3L scores between the two groups before intervention (>0.05).After 3 and 6 mo of intervention,the VAS scores of the two groups increased gradually (<0.05),and the scores of action ability,self-care,daily activities,pain and discomfort,and anxiety and depression decreased gradually (<0.05).Further comparison revealed that the overall EQ-5D-3L score of the observation group was better than that of the control group (<0.05) (Table 5).
When the three rogues25 saw the cooked meats, and the tart in the oven, and heard Nina s words, they were nearly beside themselves with amazement26, and began to consult at once how they were to get the goat into their own possession
Comparison of disease-related knowledge and compliance scores between two groups
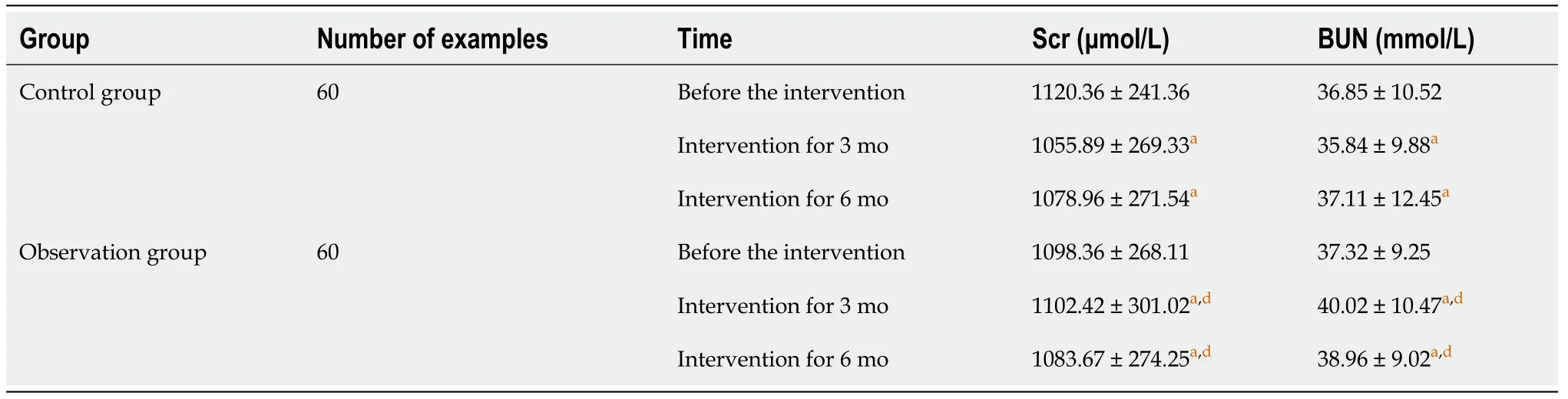
Before and 3 and 6 mo after intervention,there were no significant differences in Scr or BUN between the two groups (>0.05).Further comparison between the observation and control groups showed that there were still no significant differences in Scr and BUN (>0.05) (Table 3).
When cancer starts, for an unknown reason, a wall of calcium9 builds. Then the lump or cancer attaches itself to this wall. When Cocoa jumped on me, the force of the impact broke the lump away from the calcium wall. This made it possible for me to notice the lump. Before that, I couldn’t see it or feel it, so there was no way for me to know it was there.
The daughter had enough to do cracking nuts for him, and at the end of fourteen days she had only one tooth left in her mouth; she had broken all the rest with the nuts
DISCUSSION
Cognac s leash and put the basket in his mouth. He was off like a shot, racing15 toward Brad with his beautiful golden ears streaming behind him, as if he was hot on the trail of a speeding rabbit. There was a swell16 of laughter as our guests appreciated the dedication17 of our furry18 ring- bearer.
Blood phosphorus mainly comes from food and is absorbed through the small intestine.Patients on hemodialysis need a high-protein diet due to excessive protein consumption.The high phosphorus content of protein leads to an increase in phosphorus intake.In patients with chronic renal failure,glomerular filtration function decreases,as does the ability to excrete phosphorus.Thus,it is vital to instruct patients to follow a reasonable diet to achieve a balance between protein intake and phosphorus intake.
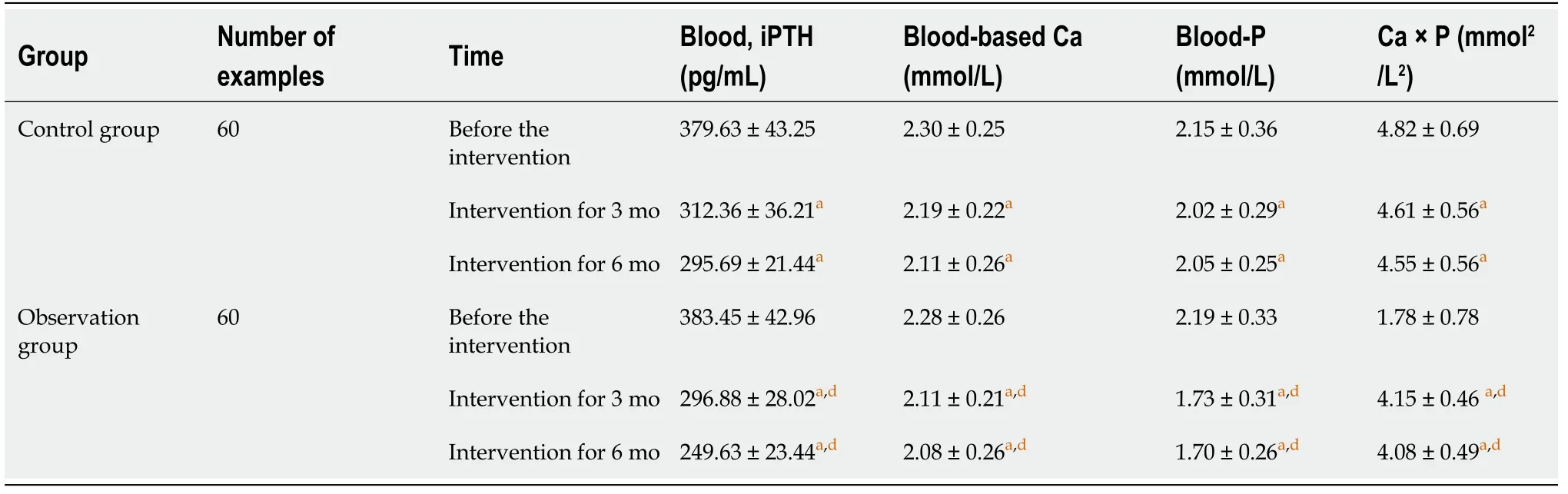
There was no significant difference in blood iPTH,Ca,P,or Ca × P levels between the two groups before intervention (>0.05).After 3 and 6 mo of intervention,the blood iPTH,Ca,P,and Ca × P levels in the two groups decreased gradually (<0.05).Further comparison showed that the blood iPTH,Ca,P,and Ca × P levels in the observation group were lower than those in the control group (<0.05) (Table 2).
But how do you suppose we can manage to live till summer comes round again? Do not be anxious about that, said the girl; if you will only marry me all will be well
The satisfaction rate in the observation group after 3 mo of intervention was 93.33% and after 6 mo,90.00%,which was high compared with the 80.00% and 71.67%,respectively,in the control group (<0.05) (Table 4).
EQ-5D-3L scores[8] included the health description system and visual analogue scale (VAS) scores.The health description system included five dimensions:action ability,self-care,daily activities,pain and discomfort,and anxiety and depression.The higher the score,the lower the quality of life in patients.The VAS score was assessed on a 100-point scale.The higher the score,the better the patient’s health status.Diseaserelated knowledge scores were determined using self-administered questionnaires that covered disease,diet,and medication knowledge of three methods.Each of these aspects was assessed on a 100-point scale.The higher the score,the richer the patient’s disease-related knowledge.
The EQ-5D-3L questionnaire is commonly used in clinical settings to evaluate the quality of life in patients with chronic renal failure with good reliability and efficacy[19,20].This study found that,compared with conventional nursing interventions,doctor-led intensive diet education interventions resulted in patients having VAS scores that were higher for mobility,self-care,and daily activities and lower for pain and discomfort and anxiety and depression,and in higher scores of disease-related knowledge and compliance.These results suggest that doctor-led intensive diet education can advance the quality of life in patients with chronic renal failure and hyperphosphatemia and strengthen disease-related knowledge and compliance.
Chronic renal failure with hyperphosphatemia is unfavorable to the prognosis of patients,and a reduction in blood phosphorus should be emphasized in clinical work.Restricting the intake of phosphorus in patients’ diets is an important way to reduce blood phosphorus.However,the status quo of patients’ knowledge of a reasonable diet with chronic renal failure and the effect of routine health education are not ideal.In this study,doctor-led intensive diet education was used in comparison with routine nursing education;the former can promote patients' mastery of and compliance with health knowledge and has certain advantages in regulating the balance of Ca and phosphorus in patients’ bodies and improving the quality of patients’ lives.Thus,doctor-led intensive diet education should be popularized and applied.
The clerk disappeared and came back a moment later with three robes in sturdy terry cloth. He chose blindly, hardly glancing down, taking the one on top. Three sizes, the clerk was saying, and a better selection of colors next month, but he was already in the aisle24, a coral-colored robe draped over his arm, his shoes squeaking28 on the tiles as he moved impatiently between the other shoppers to where she stood.
CONCLUSION
Doctor-led intensive diet education can improve the quality of life in patients with chronic renal failure and hyperphosphatemia,promote low-phosphorus diet behavior,and boost patient satisfaction.
ARTICLE HIGHLIGHTS
Research background
Secondary hyperparathyroidism,renal osteodystrophy,and cardiovascular adverse events can occur if long-term hyperphosphatemia is not corrected,leading to the adverse prognosis of patients with chronic renal failure.The clinical control measures for hyperphosphatemia in these patients include diet control.
Research motivation
Provide reference for the treatment of patients with chronic renal failure and hyperphosphatemia.
Research objectives
This study aimed to observe doctor-led intensive diet education effects on healthrelated quality of life,in patients with chronic renal failure and hyperphosphatemia.
The sight of a handful of gold pieces somewhat mollified her, however, and after making them both promise faithfully that on no consideration would they ask for the gold back again, she took the Princess into the house and grudgingly73 doled74 out to her just enough of her gay attire to make her presentable, while the rest she pretended to have lost
Research methods
We assessed 120 patients with chronic renal failure hemodialysis and hyperphosphatemia admitted to our hospital (July 2018–March 2020).The levels of serum parathyroid hormone (iPTH),calcium (Ca),phosphorus (P),calcium-phosphorus product (Ca × P),serum creatinine (Scr),and blood urea nitrogen (BUN) before intervention and 3 and 6 mo after intervention in the groups were assessed.
Research results
After 3 mo and 6 mo of intervention,the blood iPTH,Ca,P and Ca × P in the two groups decreased gradually,but there was no significant difference in Scr and BUN.The blood iPTH,Ca,P and Ca × P in the observation group were lower than those in the control group.The overall EQ-5D-3L score of the observation group was better than that of the control group.The scores of disease-related knowledge and compliance were higher in the observation group than in the control group.
Research conclusions
Doctor-led intensive diet education can improve the quality of life of patients with chronic renal failure and hyperphosphatemia,promote low-phosphorus diet behavior,and improve patient satisfaction.
The years passed, and I finished college and took a job in another town. Once, while visiting my parents, I used the phone in their bedroom, and noticed that the pickle jar was gone. It had served its purpose and had been removed. A lump rose in my throat as I stared at the spot beside the dresser where the jar had always stood. My dad was a man of few words, and never lectured me on the values of determination, perseverance12, and faith. The pickle jar had taught me all these virtues13 far more eloquently14 than the most flowery of words could have done.
Research perspectives
Exploring treatment approaches for patients with chronic renal failure and hyperphosphatemia can provide references for clinical work in the future.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report