
Choice of place for childbirth among pregnant women accessing antenatal care at Nnamdi Azikiwe University Teaching Hospital,Nnewi,Nigeria:a descriptive study
2022-02-15 04:54AnulikaAfonnePaulineEzendukaLindaOdikpoClementinaNwankwoEstherSilas
Nursing Communications 2022年13期
Anulika Afonne,Pauline Ezenduka,Linda Odikpo,Clementina Nwankwo,Esther Silas
1Department of Nursing Science,Faculty of Health Sciences&Technology,Nnamdi Azikiwe University,Nnewi Campus,Nnewi PMB 5001,Nigeria.
Abstract Objective: This study determined choice of place of delivery among women accessing antenatal care clinics in Nnamdi Azikiwe University Teaching Hospital (NAUTH) Nnewi in Anambra state. Methods: A descriptive survey was conducted with three hundred and twenty‐two pregnant women who registered for antenatal care at Nnamdi Azikiwe University Teaching Hospital, Nnewi. Data were collected using a self‐structured questionnaire and analyzed with a Chi‐square test of association and Fisher’s exact test were used to test the hypothesis at 5% level of significance. Results: Findings from the study showed that 39.75% of the pregnant women chose private hospitals as their place of delivery, 37.27% chose NAUTH, 6.52% and 7.14% chose other government hospitals and home delivery, respectively. There was a significant difference between education level and occupation of the participants in the choice of place of childbirth.Privacy, finance, distance and approach of health workers were significant predictors of choice of delivery place among the women. Conclusion: Health planners need to recognize the determinant choice of delivery place as more efforts should be given to educate women and empower them.However, utilization of tertiary health facilities for childbirth may increase if the privacy of pregnant women is maintained,health workers relate well with clients and the cost of health care services is reduced.
Keywords:antenatal care; health care facility; maternal mortality; skilled birth attendant
Introduction
Maternal mortality remains unacceptably high as about 295,000 women died during and following pregnancy and childbirth in 2017.The vast majority of these deaths (94%) occurred in low resource settings and most could have been prevented [1]. Nigeria records nearly 20% of all global maternal deaths, and it is estimated that a Nigerian woman has 1 in 22 lifetime risk of dying during pregnancy or childbirth or postpartum [2]. Therefore, increasing in the number of women who deliver in a health facility can be an important means in reducing maternal mortality of low‐income settings like Nigeria.
Choice of delivery location is the selection (made by a pregnant woman) of an appropriate place to be delivered her baby. Basically,the delivery places in Nigeria can either be at home or health facilities.A woman can deliver her baby at home, with or without the presence of a birth attendant,who may be trained or untrained.Home delivery is usually the cheapest but is associated with attendant risks of infection and lack of available equipment should complications occur. It has been noted that a significant number of pregnant women in developing countries still deliver at home unattended to by skilled birth attendants [3].
Institutional deliveries can occur at private or public facilities.Public facilities like Nnamdi Azikiwe University Teaching Hospital(NAUTH), Nnewi are owned and financed by the government, while private facilities are the most expensive and are often perceived as having the best amenities and offering the best standard of care in Nigeria. Most maternal deaths occur as a result of complications during labor,delivery,or within the first 24 hours after birth.Most are preventable or treatable such as hemorrhage, infections and preeclampsia/eclampsia [4]. Birth is an event of great importance in family life, and the quality of birth outcome can be enhanced through proper antenatal care(ANC) coupled with making an informed choice of place of delivery as recommended by health professionals [5].Furthermore, the majority of the maternal deaths that occur are avoidable or preventable if deliveries are managed by skilled attendants[1].
According to the 2013 Nigeria Demographic and Health Survey(NDHS), only 36% of births occurred in a health facility and skilled health workers delivered only 38% of all births in the country [6]. A qualitative study conducted by Chol et al [7] in Asmara village,Eritrea, recognized two factors as facilitators of women’s access and utilization of maternal health services [7]. These factors were health education and women’s empowerment. Also, in a descriptive cross‐sectional study carried out in a primary health facility in Southern Nigeria by Johnson et al, choice of place of delivery was influenced by distance, cost, skills of health care provider, supply of drugs and attitude of health care workers [8]. Finally, according to a cross‐sectional survey conducted in Nigeria by Egharevba et al [9] in South‐East Nigeria, events around labor, number of children and availability of relatives affect the choice of place of delivery. All these studies mentioned above were carried out in rural areas and primary and secondary health care institutions, hence the need to study a tertiary health institution in an urban area. This study, therefore, was designed to elucidate the choice of place for childbirth among pregnant women assessing antenatal care at NAUTH, Nnewi, Nigeria.
Methods
Descriptive survey design was adopted for the study to assess choice of delivery place among pregnant women attending ante‐natal clinic at Nnamdi Azikiwe University Teaching Hospital, Nnewi. Nnewi is a town in Anambra State, South‐East Nigeria. The study population consists of 1,650 pregnant women who attended antenatal clinics at NAUTH, Nnewi from September, 2018 to February,2019. The sample size of 322 pregnant women was obtained using the Yaro Yamane formula.Purposive sampling technique was used by the researchers in selection of the participants. The inclusion criteria are pregnant women attending antenatal care in NAUTH who willingly accepted to participate and filled the questionnaire forms.The instrument for data collection was self‐structured questionnaire which experts in the field of study. To ensure reliability of the instrument, a pilot study of the instrument was conducted using thirty‐two women attending Antenatal clinic at Chukwuemeka Odimegwu Ojukwu Teaching Hospital (COOUTH), Awka, from which a reliability test was carried out using a Spearman Brown coefficient correlation and it was found to be 0.79.A total of 360 copies of the questionnaire were distributed,only 322 however, were retrieved, making the response rate 89%.Data were analyzed using Graph Pad Prism version 5.0. Simple frequencies and proportions were used to present the sociodemographic characteristics, and Chi‐square and Fisher’s exact test were used to assess the relationship between choice of place of delivery and independent variables. Ethical clearance was obtained from NAUTH Health Research Ethics Committee, Nnewi (Ref. No:NAUTH/CS/66/VOL.3/86).
Results
The sociodemographic characteristics of the participants are presented in Table 1. The age range of the women was from 15 to 45 years.Majority of the respondents (29.5%) were from the age group 20‐24 years, while the least (7.45%) were from the age group 15‐19 years.The highest percentage of respondents were married (91.93%), those who were single were 5.28%, while the divorced were 0.93%. The educational status of the participants showed that 37.58%had tertiary and secondary education, respectively, 16.46% had primary education, while only 8.39% had no formal education. Among the respondents, 41.61% were private workers, 34.78% were public servants, and 13.98% were students. The parity of the respondents showed that 29.81% were nulliparous, 45.96% had given birth to one or two children, 17.70% had three to four children, while 6.52% had five children and above (Table 1).
Of all the respondents, 92.86% chose to deliver in a health facility,while 7.14% chose home delivery (Figure 1). Of those who chose to deliver in a health facility, 39.75% chose private hospitals as their delivery place, followed by NAUTH (37.27%) and mission hospitals(9.32%).It is also evident from the result that the least choice of place for child delivery recorded were other government hospitals and home delivery, 6.52% and 7.14%, respectively. The figure also showed that 47.83%of the respondents assessed NAUTH as the best place for child delivery, followed by private hospitals irrespective of their choices.
Table 2 shows the reasons for the participants’ choice of NAUTH as a place of child delivery. Of the 97 respondents that delivered at NAUTH, 25.77% chose it for safe and clean delivery, 24.74% for skilled professionals available, 22.68% for better service, 6.19% for fear of complications, while 1.03% chose it as a result of proximity.218 respondents had never delivered at NAUTH. Of these, 22.94%could not give any reason for not choosing NAUTH. However, 23.85%gave their reason as too much protocol at NAUTH, while 24.31%stated other reasons outside the options on the questionnaire (such as too many investigations, fear of being operated on, prolonged stay after delivery etc). Some others stated that students use patients to learn (14.22%), while 5.05% stated that it takes time and 4.13%gave reasons of unpleasant approach of some workers. Some of the respondents who chose NAUTH, but may not have given reasons for choosing it may have given reasons for not choosing it since they may have not accessed the facility yet.
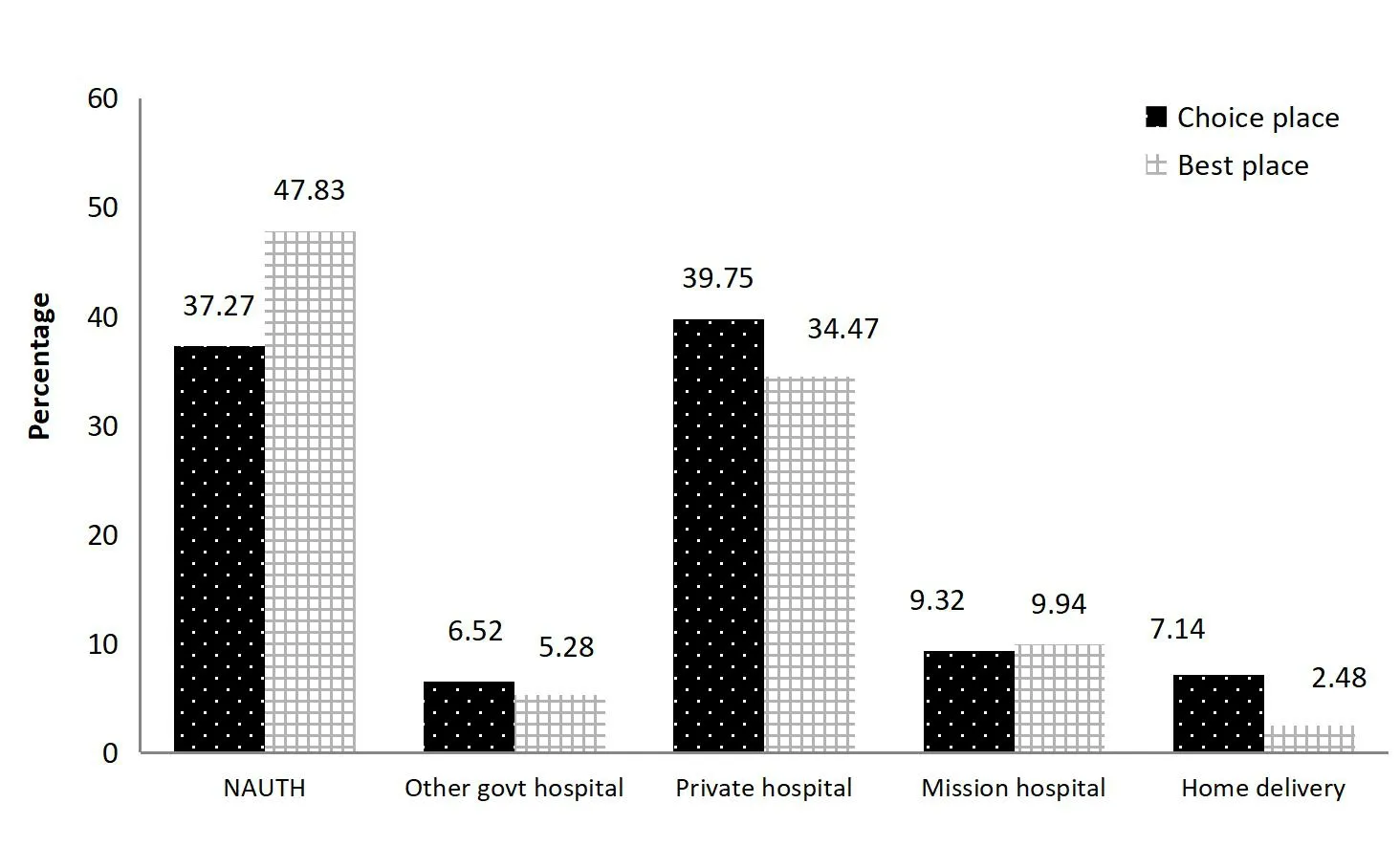
Figure 1 Participants’ choice of place of child delivery and best place of delivery
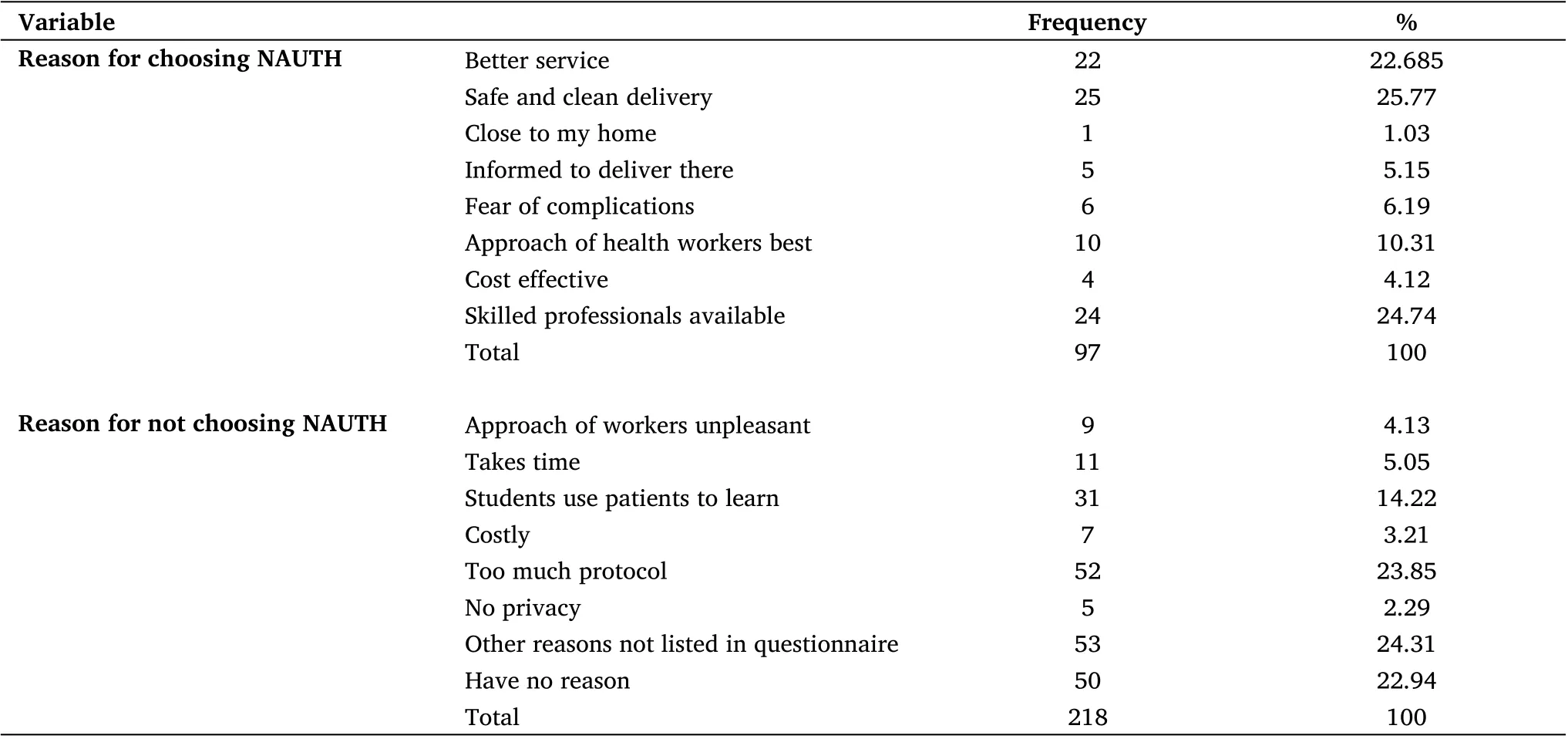
Table 2 Reason for choosing or not choosing NAUTH as place of child delivery for participants who had delivered before
Of the 322 participants, 21 chose other government hospitals as a place of child delivery (Table 3). Among these, 23.81% chose other government hospitals due to the far distance to NAUTH, 14.29% for trust in doctor and less time spent, while 4.76% as a result of bad experience they had at NAUTH. The most frequent reasons given for choosing private hospitals were trusted in doctor (37.50%), spending less time(19.53%) and no means of transport (1.50%). Also, from the table,it could be seen that of the 30 participants who selected mission hospitals, 36.67% gave their reasons as trust in doctor (36.67%),distance to other hospitals is far (23.33%) and owned by a church(16.67%). It is evident from the table that reasons for home delivery were privacy (26.09%), followed by not expensive (21.74%) while only 13.04% chose no need for transport as a reason.
There was a significant difference between educational level and occupation of the participants in choice of place of childbirth whereas there is no significant difference between age and choice of place of childbirth(Table 4).
Regarding educational status, the participants with secondary education showed that there is one in four likelihood that a woman will choose NAUTH rather than other facilities (other government hospitals, private hospital, mission owned hospitals and home) as delivery place compared to participants who no had formal education[OR (95% CI) 0.27 (0.10‐0.76)] (Table 5). Furthermore, the association between formal education and no formal education showed that participants with formal education had one in three chances of choosing NAUTH as against other facilities as choice of place of delivery compared to participants with no formal education[OR (95% CI) 0.36 (0.13‐0.97)]. Occupational status of the participants showed participants that public servants had one in four chances of choosing NAUTH over other facilities as place of delivery compared to participants who were housewives [OR (95% CI) 0.26(0.10‐0.68)]. Also, the association between those working (public service and private work)and housewives shows that participants who are working had one in three chances of choosing NAUTH as against other health facilities as place of delivery when compared to participants who are housewives[OR (95% CI) 0.36 (0.14‐0.90)].
From Figure 2, both husband and wife made a decision where to deliver (53.73%), followed by the women alone (24.22%) and husband (15.53%). Figure 3 shows that, of the 97 participants who had delivered in NAUTH before, 34% rate their child delivery service to be good.
Discussion
Result of the study on choice of place of childbirth among pregnant women assessing ante natalcare in Nnamdi Azikiwe University Teaching Hospital, was presented. According to the findings, majority chose private hospitals as their delivery place, followed by NAUTH,mission hospitals and other government hospitals.Home delivery was the least in the women’s choice of delivery place.It was obvious in the study that majority chooses to have their baby in the hospital and there is a preference from one hospital to the other. The result agrees with Gebregziabher et al [5] and Nwankwo et al [10], who saw high level of the respondents choosing hospital as their preferred place of delivery. The result, however, is inconsistent with another study carried by Idris, Gwarzo and Shehu [11] where majority (70.2%) of the respondents chose home delivery as against hospital. The difference and the similarity may be due to different‐socio demographic and socio‐cultural characteristics of the study participants. In a similar study, Envuladu et al [12] discovered the least in her study population chose home delivery. However,Andersen’s model posits that need is the most proximate determinant of health services utilization. The need can be conceptualized as perceived (by the individual woman) or evaluated (by an expert, such as a physician). One’s construction of need is more evaluative than perceived [13].
Results also showed that participants who have delivered in NAUTH chose it mostly for the safe and clean delivery, skilled professional who takes the delivery, better services rendered,fear of complications and close distance. This implies that one’s past experience is likely to influence choice of place of childbirth and also having information could influence women’s knowledge about delivery risks and availability of services. This finding is in agreement with Gebregziabher et al [5] and Envuladu et al [12], who discovered that women who had complications during their last pregnancy are more likely to choose a tertiary hospital as their place of delivery.Similarly,Yahya and Pumpaibool[14] also saw hospital delivery especially very important to women who had previous pregnancy complications in addition to having had their previous delivery in the hospital.Contradicting this finding was a report from Shambe et al [15] who saw the safety of pregnant mothers as the major consideration that influenced the place of delivery among women of reproductive age in this population hence hospital delivery was the most favoured place of delivery and made some women to prefer one hospital to the other.

Table 3 Participants’reasons for choosing other health facilities as place of child delivery
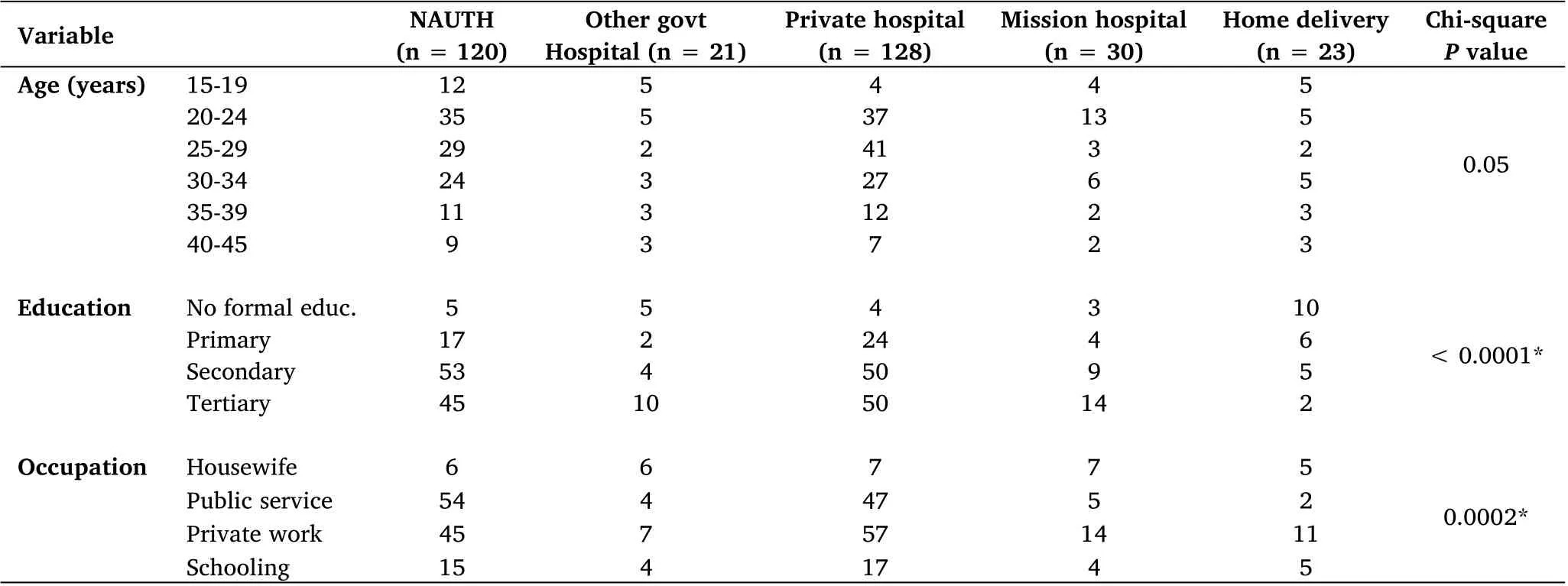
Table 4 Selected socio-demographic correlates for participants’choice of place of child delivery
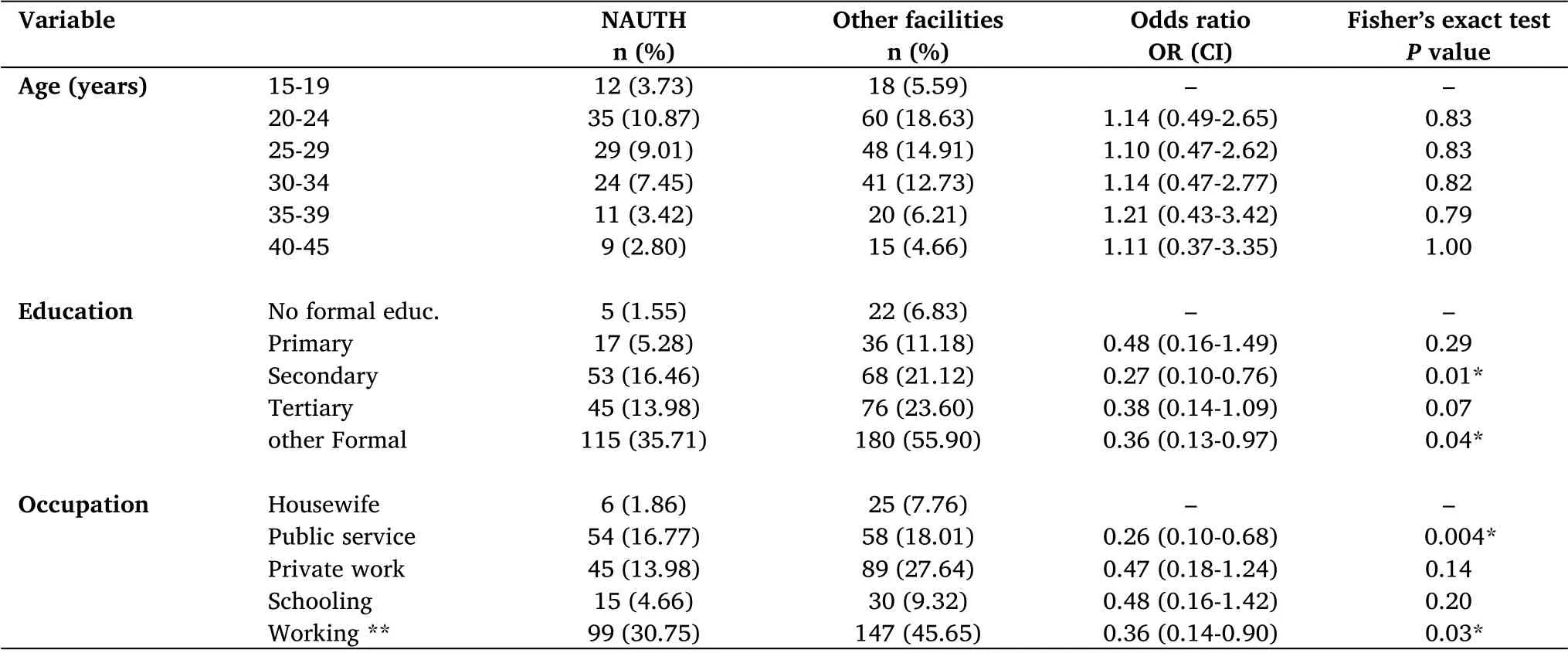
Table 5 Test for association of selected socio-demographic variables with women’s choice of place of delivery (n =322)
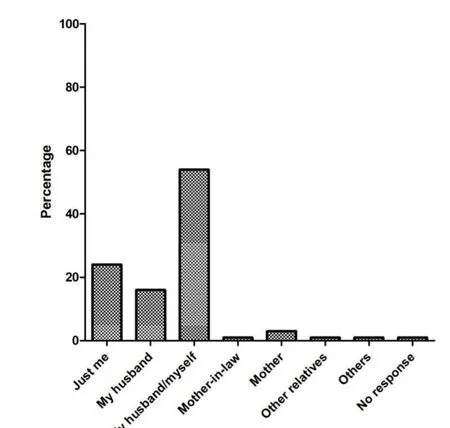
Figure 2 Who decides where you deliver?
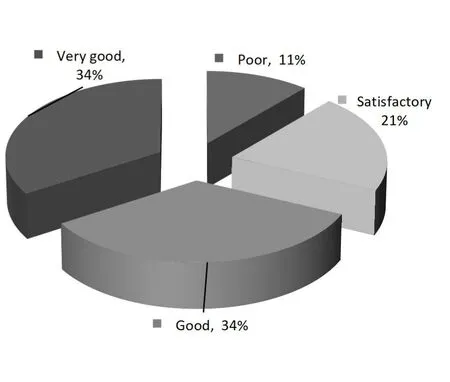
Figure 3 Rating of child delivery service at NAUTH by respondents
Furthermore,the reason for choosing other government hospitals as against NAUTH, a tertiary hospital according to this study, were mostly due to far distance to NAUTH, trust on some doctors in other hospitals, and lesser time spent in receiving care and previous bad experience had at NAUTH. This implies that physical distance from their houses imposes another cost to the pregnant women:opportunity cost time spent to obtain these services in terms of distance is very important in the use of reproductive health services. This finding is consistent with Envuladu [12] and Johnson et al [8] who discovered distance and unfriendly attitude of health care workers which is similar to previous bad experience the women had as a reason for choice of delivery place. In addition, the cost of hospital bill,unexpected labor, and failure to book for ANC was other reasons identified by Egharevba et al [9] and Envuladu [12], contrary to the findings from this study. Result on who makes decision on choice of delivery place. Findings from the study shows majority of the women reported joint decision followed by self and husband deciding alone.This finding agrees with Seljeskog, Sundby and Chimango [16] who saw cultural aspects such as influence from decision‐makers like husbands, perceptions of danger signs and traditional views on pregnancy and delivery were important.A similar report was given by Nwankwo et al [10] that decision‐makers in the family affect place or choice of delivery. This spans through decisions to spend the money earned by the women.Many cases were taken by their husbands while decisions were taken jointly with their husbands with “others” as decision‐makers totaling. Similarly, decisions to utilize health care services were taken by the husbands of the respondents alone.Some of decisions were taken jointly with their husbands which were similar to the report by Yahya and Pumpaibool [14].
From socio‐demographic variables, age was found to have no association with the choice of delivery place in this study. The similarity may be due to similar socio‐cultural characteristics of the study participant. The possible explanation for this finding could be choice of the hospital as a delivery place among majority of women in all the age group implies that the participants have a better understanding about the advantages of hospital deliveries.Contrary to this finding, Yahya and Pumpaibool [14], in their report discovered age had an association with the selection of delivery place as older women are more likely to make a decision independently or together with their partner concerning their delivery place, unlike the younger ones who might not be bold enough to decide on delivery place or even contribute to the decision.
Educational status of the women was found as one of significant predictors for choice of delivery place. Participants with formal education had one in three chances of choosing Nnamdi Azikiwe University Teaching Hospital, Nnewi over other facilities (other government hospitals, private hospitals, mission hospitals and home delivery) as a choice of place of delivery compared to participants with no formal education. Other studies have shown comparable results with this finding, including study by Johnson et al [8] and Mukhtar et al[17]who stated that Female education should empower them to make better choices about their health services options especially delivery. Another study conducted with Syrian women by Bashouur and Abudulsalam [18], indicated that the demographic variables like woman’s education were statistically related to preference of delivery place. Participants with formal education are expected to be aware and have knowledge on choosing where to deliver based on their health condition. They are more likely to seek modern health care than those who are not. Education is likely to improve the general status of women and help them to build up confidence to make decisions about their own health. Educated women could have better access to information through reading and following media about maternal health care and they could have better knowledge about the advantages of maternal health care and pregnancy‐related complications corroborated by Yahya and Pumpaibool[14],and Gebregziabher et al[5] in their report.
However, the findings showed a significant difference between occupation of the participants and their choice of place of childbirth.Association between those working and housewives showed that participants are working had one in three chances of choosing NAUTH as against other health facilities as a place of delivery compared to participants who are housewives. The possible reason for this finding could be the working class may appear to have the wherewithal to pay for the price of NAUTH and given the perception of better quality at NAUTH,it is no surprise that they utilize them. In agreement with this finding, Yahya and Pumpaibool [14], and Gebregziabher et al [5] in their own report saw paid work in essence as one of the influencers to the choice of delivery place.
Conclusion
Choice of delivery place is a necessary tool for curbing maternal and fetal mortality and morbidity in Anambra and Nigeria. It is necessary for health workers attending to pregnant women during ANC to educate, organize community‐based campaigns on choice of place of child delivery. This will increase the knowledge on the need to make inform choices toward place of child delivery. Also, utilization of tertiary health facilities for childbirth may increase, if privacy of pregnant women is maintained, health workers relate well with clients, cost of health care services is reduced and less time spend. In addition, decision‐makers in the families especially husbands should be encouraged to support their wives to get the appropriate care required during pregnancy and child delivery. Families should develop plans to empower the female child holistically, as this will have a positive effect on their choice of place of delivery.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia