
Second-order problem solving:Nurses’ perspectives on learning from near misses
2021-12-11 13:55:52YiYngHupingLiuGwenSherwood
Yi Yng ,Huping Liu ,* ,Gwen D.Sherwood
a Peking Union Medical College,School of Nursing,China
b The University of North Carolina at Chapel Hill,School of Nursing,NC,USA
Keywords:Near misses Nurses Nurse’s role Patient safety Problem solving Tertiary care centers 4I framework of organizational learning
ABSTRACT Objectives:Near misses happen more frequently than actual errors,and highlight system vulnerabilities without causing any harm,thus provide a safe space for organizational learning.Second-order problem solving behavior offers a new perspective to better understand how nurses promote learning from near misses to improve organizational outcomes.This study aimed to explore frontline nurses’ perspectives on using second-order problem solving behavior in learning from near misses to improve patient safety.Methods:A qualitative exploratory study design was employed.This study was conducted in three tertiary hospitals in east China from June to November 2015.Purposive sampling was used to recruit 19 frontline nurses.Semi-structured interviews and a qualitative directed content analysis was undertaken using Crossan’s 4I Framework of Organizational Learning as a coding framework.Results:Second-order problem solving behavior,based on the 4I Framework of Organizational Learning,was referred to as being a leader in exposing near misses,pushing forward the cause analysis within limited capacity,balancing the active and passive role during improvement project,and promoting the continuous improvement with passion while feeling low-powered.Conclusions:4I Framework of Organizational Learning can be an underlying guide to enrich frontline nurses’ role in promoting organizations to learn from near misses.In this study,nurses displayed their pivotal role in organizational learning from near misses by using second-order problem solving.However,additional knowledge,skills,and support are needed to maximize the application of second-order problem solving behavior when near misses are recognized.
What is known?
· Near misses present learning opportunities to improve safety,but organizational efforts to learn from near misses often fail.
· Second-order problem solving behavior (SOPSB) offers a new perspective to understand how individuals promote organizational learning from errors,yet there is limited evidence exploring SOPSB in learning from near misses.
What is new?
· SOPSB was recognized as actions to prevent the recurrence of near misses,including exposing the occurrence of near misses,pushing forward the cause analysis,trying out improvement projects,and promoting continuous improvement.Inherent in the four actions,nurses were feeling equal parts passionate and low-powered.
· By using SOPSB,on the one hand,frontline nurses demonstrated their active and pivotal role in learning from near misses.On the other hand,nurses usually felt low-powered when conducting SOPSB due to the characteristics of near misses,scarcities of safety management knowledge and unsupportive working environment.
1.Introduction
Despite decades of focus,patient safety remains a primary health care concern due to the high rate of errors[1].Beyond the negative aspect of patient harm,errors can serve as valuable learning resources for organizations by examining why they occur and how they should be prevented.Learning more about errors can help organizations work towards adjustments of strategies and behavior to restructure the system and increase safety [2].Although adverse events have long been regarded as an important key to learning,near misses have attracted considerable attention recently.A near miss is defined as an incident which did not reach the patient by chance or timely intervention [3].Near misses have garnered attention because they occur more frequently than adverse events–as much as 7 to 100 times more frequently [4],allowing for a greater quantitative analysis and learning process.More importantly,near misses have remarkably similar causes with adverse events[5]and can shed light on system vulnerabilities and suggest preventative strategies without causing harm [6,7],showing great value in optimizing the cost/benefit ratio for investment in patient safety.
Organizational efforts to learn from errors often fail because the role of employees’ behavior in learning has not been fully appreciated [8].Few organizations train their employees in effective problem solving behavior as a part of the organization’s approach to learning from critical safety events.Research showed that when faced with problems,“fixing and forgetting” was the predominant problem solving choice made by healthcare workers;those who took actions to solve problems for system-wide learning and solutions were less than 10% [8].
Based on the concept of organizational learning,Tucker [8]developed the second-order problem solving behavior (SOPSB)model to exhibit employees’ effort to promote learning from failures.According to Tucker,first-order problem solving behavior manifested as temporarily correcting or only“patching”a problem without any further actions.By contrast,SOPSB emphasized the individuals’ response to problems by investigating the underlying causes and searching for preventative countermeasures.SOPSB has been accepted as an effective approach to successful organizational learning and highlights the important role of the grass-roots employees in safety and quality management as well[9-11].For near misses,SOPSB appears particularly practical because the distinctive features of near misses– less visibility and harmlessness means that organizational learning relies on the problem solving behavior of frontline employees,who hold first-hand information of near misses.However,SOPSB in learning from near misses has received only marginal attention in the literature.Limited knowledge mostly comes from comments of managers or studies that have used quantitative [12,13] and qualitative [14] approaches to explore near-miss reporting.Although reporting is critical to organizational learning for lasting improvements,it is not enough to get a full sense of the learning efforts just like the SOPSB does.Jeffs indicated that only by reporting problems was to no avail for learning because the problems would go into a black hole without seeking further investigations [15].
In recent years,China has emphasized the importance of learning from errors,including near misses,by issuing the National Provisions on Medical Quality and Safety and establishing the nationwide adverse events reporting system,which makes the exploration of SOPSB in learning from near misses more necessary.As the last line of defense in preventing patients from being harmed,frontline nurses are in a position to experience more near misses [16].They are a primary force of quality and safety management [17],which makes them an indispensable part in conducting SOPSB to promote organizational learning from near misses.Thus,it is important to understand the nurses’perceptions and experiences of applying SOPSB to increase organizational knowledge about near misses based on a qualitative approach in pursuit of a naturalistic paradigm.Given this,the findings of this study are meaningful as basic data to develop a comprehensive educational and managerial program.Therefore,the aim of this study was to explore frontline nurses’ perspectives on using second-order problem solving behavior in learning from near misses to improve patient safety.
2.Theoretical framework
Theoretically,we drew on the 4I Framework of Organizational Learning proposed by Crossan [18].The framework emphasizes four key steps (intuiting,interpreting,integrating,institutionalizing) and relations in determining how organizational learning happens in the multi-level dynamic process.It shows a range of activities that explain how knowledge produce,transfer and utilize from the individual level to the organizational level.For example,individuals recognize information-based triggers (intuiting),develop models for understanding,bring out the meaning in groups (interpreting),and eventually realize the organizational learning by translating a shared understanding into coordinated action (integrating) and embedded it into work routines (institutionalizing).We chose this particular framework to theoretically underpin the study because it has been well proved and empirically grounded in research of organizational learning [19-21].More importantly,it emphasizes the dynamic process of learning and knowledge construction from the individual to the organizational level [18],which aligns with the aims of this study.
3.Methods
3.1.Study design
A qualitative exploratory design with semi-structured interviews and directed content analysis was employed.
3.2.Participants
Participants were recruited from 19 nursing units in three general tertiary hospitals in east China.Hospitals ranged in size from 1,300 beds to 2,500 beds.A purposive sampling of Registered Nurses was recruited using maximum variation sampling for working experience,educational level and unit.The inclusion criteria were for nurses with at least five-year work experience and have had the experience of near misses during their work.We deliberately recruited senior nurses because of their experience with near misses,relatively higher safety awareness and exposure to SOPSB.Head nurses and managers were not recruited because they do not work in direct care,where most near misses occur and their views on SOPSB may differ from those of frontline nurses.Potential participants were identified in discussion with the corresponding nursing department of the participating hospital.Letters explaining the purpose of the study were then sent to the target nurses who met our inclusion criteria.We obtained written consent from those who were keen to participate.We accepted the suggestion by Sandelowski that the sample size is a matter of quality rather than quantity,and decided the size by the saturation of data [22].In this study,saturation was reached after 15 interviews,and a further four interviews were carried out to validate the saturation.Table 1 provides the detail of participants.
3.3.Data collection
Data were collected between June and November 2015 through audio-recorded,face-to-face,and semi-structured individual interviews.Interviews were carried out by the first author,who was a Ph.D.candidate and had been fully trained of qualitative study.Each interview lasted between 45 and 96 min.The interviewer adopted a conversational and emphatic approach.The foci of the interviews began with a general question about near misses that nurses had experienced,followed by a series of questions related to the behavior he/she perceived as SOPSB.Probing questions were added to gain more detailed information,such as ‘please describe what you mean by reward on near-miss reporting’.Table 2 provides examples of frequently asked questions.Considering the participants’unfamiliarity with the term ‘SOPSB’ might account for a bias,the interviewer first gave a brief introduction of SOPSB,namely,the behaviors that promote learning from working problems or failures.Towards the end of each interview,the participant was asked to state the role of frontline nurses related to the management of near misses,which gave them an opportunity to reflect on their efforts to assure patient safety and enhance their participation in SOPSB.During and immediately after each interview,the interviewer made field notes of the session.
3.4.Data analysis
This study used the qualitative directed content analysis to analyze data,which is a methodology that explores a phenomenon of interest using a theory as a guide[23].In this study,Crossan’s 4I Framework of Organizational Learning was employed as a guide to describing the frontline nurses’ perceptions of SOPSB.All digital audio-recording of the interviews were transcribed verbatim (in Mandarin) within 48 h after each interview.After comparing transcripts with audiotapes for accuracy,relevant information such as emotional content was noted from the field notes.All interview transcripts were then analyzed following the suggestions provided by Assarroudi et al.[23].The initial coding categories were based on the 4I Framework.The main steps of the directed content analysis included:reading transcripts as a whole to have a feel of the essence of participants’ descriptions of SOPSB;using the 4I Framework as the initial coding categories;selecting participants’quotes supporting the particular code;reflecting on the central ideas extracted and synthesizing participants’ perceptions;converting participants’ perceptions of SOPSB into a written form.
3.5.Trustworthiness
In this study,method triangulation involving comparing data from transcripts and field notes was used.Throughout the process,two researchers analyzed the data to ensure the investigator triangulation,and any discrepancies were resolved through group discussion.To achieve peer debriefing,researchers discussed the analysis with experts in qualitative research and patient safety,and also applied the results to a group of nurses(including two quality managers and four frontline nurses) in January 2016.Moreover,three randomly selected nurses from the interviews were asked to review the data to reconfirm the accuracy of the results.To further achieve transferability,researchers provided raw quotations from the transcribed text for each category.
3.6.Ethical considerations
The study was approved by the Ph.D.research review board in the relevant Chinese university.Permission to perform the interviews was obtained from the managers of the selected hospitals.Nurses who agreed to participate signed an informed consent form and were informed that they were free to choose the location for the interview and had the right to withdraw at any time.Confidentiality and anonymity were stressed,and any identifying data of persons mentioned in the interviews were deleted from the transcriptions of the audiotapes.The interviewer and participants were mutual strangers before the interview.
4.Findings
In this study,23 registered nurses were initially invited to participate,19 agreed to be interviewed.More participants were female (18/19).The nurses’ age ranged between 29 and 40 years old;work experience ranged from six to 21 years.
Categorized according to the 4I Framework,each SOPSB is explained based on the framework and described from the nurses’perspective (Table 3).
4.1.Intuiting:being a leader in exposing near misses
Participants related that exposing near misses to the responsible persons or departments is an essential part of SOPSB.According to them,only by disclosing the invisible near misses could further action possibly be taken at the organizational level.
“If you do not expose the near misses that happened,others will never be aware of the problem,let alone take actions to prevent their recurrence.” (N1,quality supervisor)
Different strategies were employed to expose near misses,which helped focus the managers’ attention on those issues that should be urgently addressed,as well as protected the nurses from being punished.For example,nurses tended to use formal ways like structural reports to disclose near misses of high risk or had other teams involved.Informal chats were commonly used to share near misses with low risk or share those that might cause punishment.
“The bugs in electronic ordering system may result in serious medication error,so we report it through the official reporting system.” (N3,RN)
“If I am the person responsible for a near miss,the most I would do is to tell my colleagues I know well in private.” (N4,RN)
However,since near misses were hard to gain attention in clinical work,several participants stated that they had taken extra effort to optimize the exposure effect,for example,by calculating the frequency of occurrence before reporting.
“Near miss did not cause any harm,the managers will not take them seriously without any data about the potential consequence.”(N1,quality supervisor)
4.2.Interpreting:pushing forward the cause analysis within limited capacity
Participants stated that for both near misses and adverse events,searching for an in-depth explanation of why it happened should be the very core of SOPSB.Only by recognizing the causes could the organization make purposeful and effective changes,especially when the causes come to the system level.
“The SOPSB refers to my responses to the causes;when I experience a near miss,I look for the causes and then come out with measures.” (N6,quality supervisor)
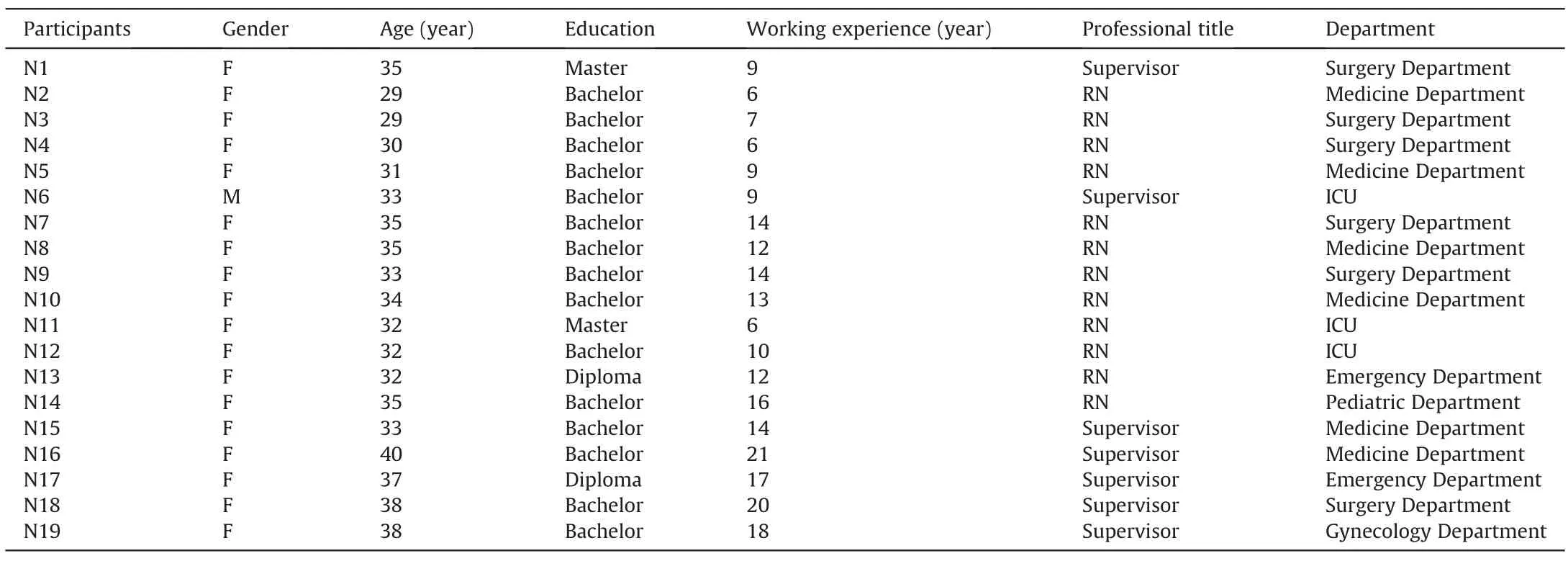
Table 1 Characteristics of participants.
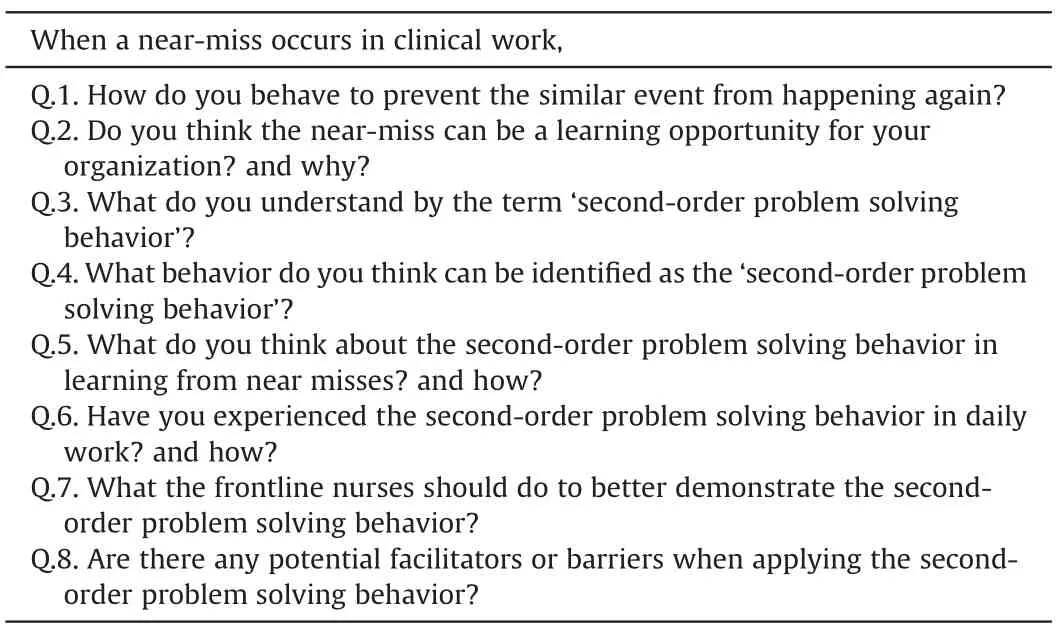
Table 2 Interview guide.
For near misses,the cause analysis was often perceived as part of the responsibility of frontline nurses.Self-reflection was reported to be the dominant way.
“I was the only person who cares about this near miss;I have to think about by myself why this event happened to me rather than others.” (N2,RN)
To further exploit the due role of cause analysis,several participants mentioned that sharing causes with others,especially the stakeholders,was important.In clinical practice,‘win-win communication’ is a good way to make the patients as well as nurses much safer.
“We use the WeChat(a favorite instant-communication tool)to let everyone in the unit know why the near miss happened.It would be meaningless if the analysis goes into the black hole.”(N15,quality supervisor)
However,it was difficult to complete a deep search for the underlying causes.Participants reported that while individual nurses lacked knowledge about causes analysis,near misses also rarely gained collective attention and got few chances to be discussed systematically.In fact,nurses tended to impute the causes of near misses to individuals rather than the flawed system.“I think most of the medication near misses are the results of individual carelessness,there is no reason to attribute them to similar look or medicine distribution system.” (N14,RN)
To compensate for their deficiency in analyzing causes,some nurses were willing to ask for assistance,especially when the investigations of causes would not have detrimental effects on themselves.
“Although the head nurse sometimes is unaware the near misses happened,I will seek help from her.After all,the cause is a time bomb.” (N8,RN)
Furthermore,participants stated that the value of near misses has not been fully realized and causes analysis was more typically regarded as the managers’business.They are concerned about how colleagues and managers treated them during the analysis.
“Only when the working atmosphere emphasizes the learning from near misses will I do cause analysis,or else others may say you are trying to shift responsibility.” (N12,RN)
4.3.Integrating:balancing the active and passive role during the improvement project
Suggesting and trying out countermeasures based on causes was reported as the best reflection of SOPSB.Participants expressed that no matter how detailed the analysis was,improving the current work process was the best sign of actually using what was learned from near misses at the organizational level.
“I think the most critical aspect of SOPSB is changing.Only when the new measures are implemented could indicate our department indeed to learn something from near misses.” (N1,quality supervisor)
Participants mentioned that due to the no-harm feature of near misses,nurses sometimes had to exert more effort for their ideas to be accepted.In general,the ideas presented with sound current evidence or surveys were more likely to be approved.
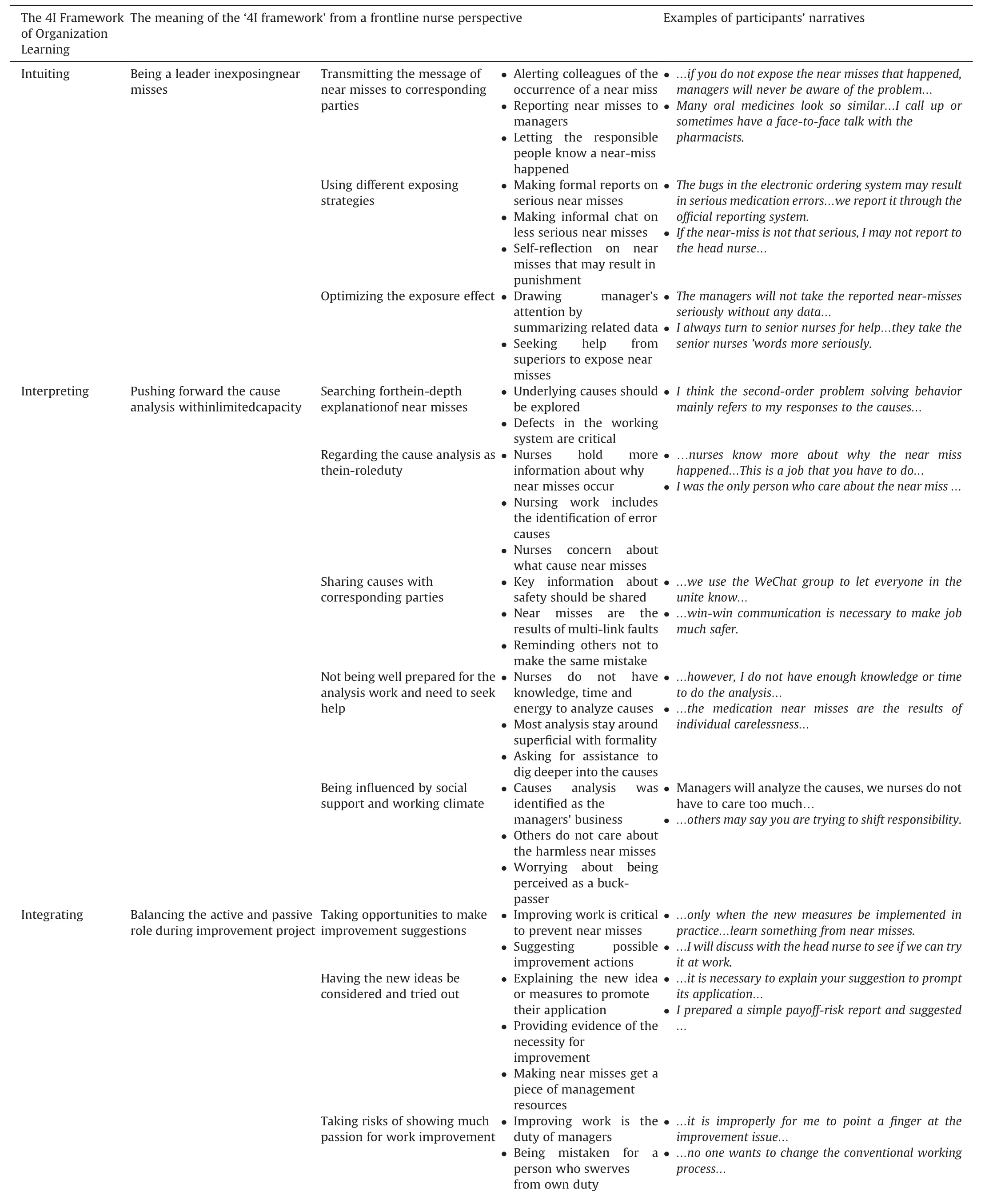
Table 3 Example of the analysis process regarding the nurses’ perception of SOPSB in learning from near misses.
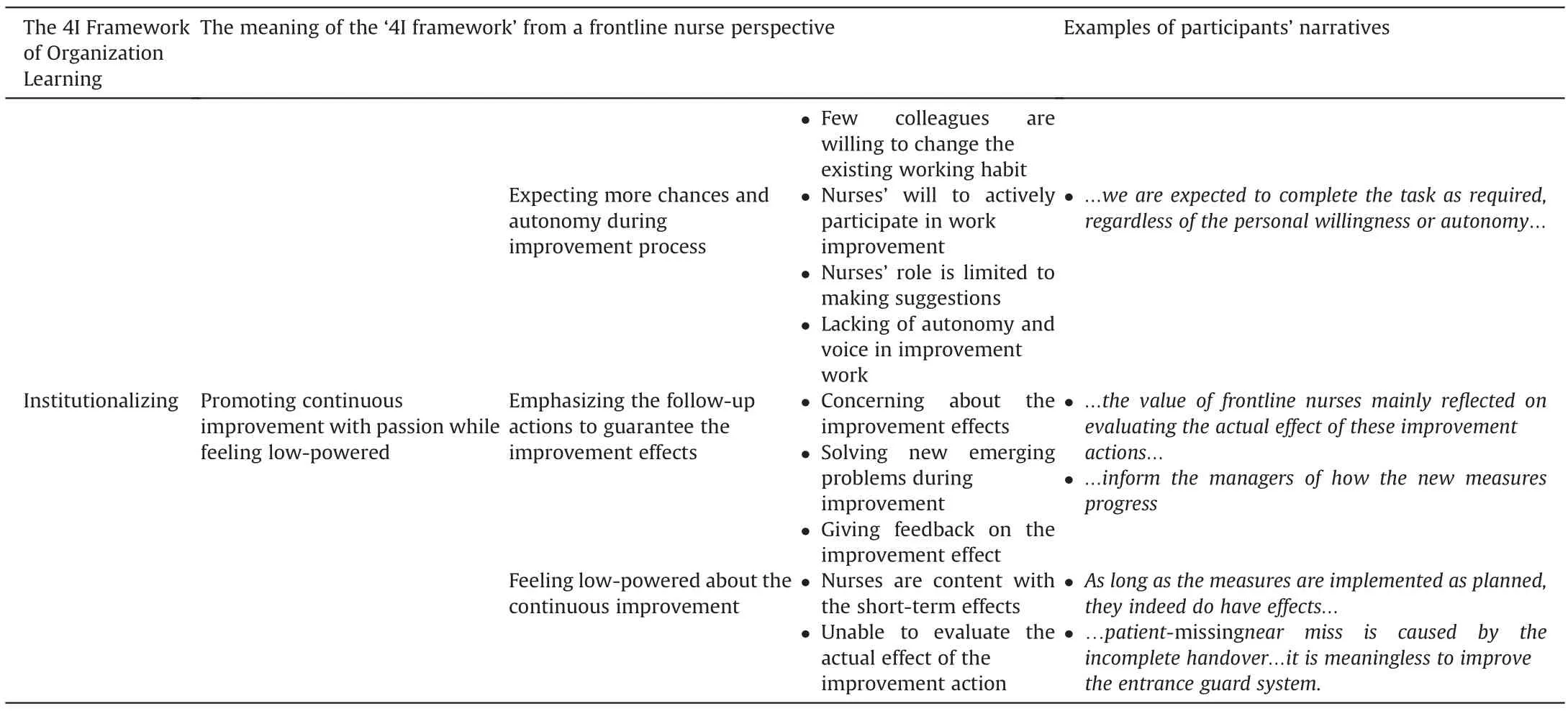
Table 3 (continued)
“I prepared a simple payoff-risk report and suggested that the improvement project should focus on the near misses regarding patient identification.” (N6,quality supervisor)
Although the majority of participants appreciated the chance to participate in the improvement activities,it was reported that showing an overly positive attitude was risky and nurses might be mistaken for those who swerved from the path of own duty.
“My job is to implement medical orders correctly,and it is improperly to point a finger at the safety and improvement issue,which is beyond the scope of my authority.” (N5,RN)
In fact,the frontline nurses’ improvement activities were usually limited to making suggestions.Participants mentioned that their autonomy and voice would inevitably be weakened once the countermeasures were applied.
“Once the suggested measures are accepted,we are expected to complete the task as required,regardless of the personal willingness or idea,our first duty is to get the work done.” (N3,RN)
4.4.Institutionalizing:promoting continuous improvement with passion while feeling low-powered
For clinical situations,it was unlikely to solve a problem fundamentally once and for all.According to the participants,taking follow-up actions such as giving feedback on the improvement effects was an indispensable part of SOPSB.Most nurses were willing to participate to completely prevent the events from happening again.
“The value of nurses mainly reflected on the evaluation of the actual effects of countermeasures,because we are those who benefit most from the successful prevention of near misses.” (N4,RN)
In practice,however,it was hard to evaluate accurately how well the improvement actions had been done.Participants emphasized that nurses were commonly satisfied with the instant effects of new measures;their enthusiasm for evaluating the long-term effects would fade away in busy work,especially for measures of preventing no-harm near misses.
“As long as the countermeasures are implemented as planned,they indeed have some effects,I think it is enough,and it is unnecessary to dwell too much on the long-term effect.” (N10,RN)
Besides,participants mentioned that defective improvement measures,such as those developed from inaccurate or ineffective cause analysis,also impede nurses’participation in the continuous improvement.
“The patient-missing near miss is caused by the incomplete handover procedure.It is meaningless to evaluate the effect of improving hospital entrance guard system.” (N16,quality supervisor)
5.Discussion
This study provides a better understanding of SOPSB by showing how nurse individuals act to promote the use of knowledge gained from near misses at the organizational level,including exposing the occurrence of near misses,pushing forward the cause analysis,trying out improvement projects,and promoting the continuous improvement.Inherent in the four actions,nurses were feeling equal parts passionate and low-powered.These findings are congruent with the core idea of the 4I Framework,which holds that individuals’ activities lay the foundation of a successful organizational learning by recognizing and interpreting improvement triggers,as well as transferring knowledge with the purpose of institutionalization [18].
5.1.Being a leader in exposing near misses to initiate learning
The National Health Service indicated that adequate access to safety data is the basis of learning[24].In this study,exposing near misses was recognized as the essential part of SOPSB and laid the foundation for the knowledge transferring to the organizational level,which has been described earlier[10,25].Paparella held that the learning value of system-based failures remained unreachable without reporting [11].Although most participants in this study lacked a deep understanding of the value of near misses and the improvement process,they commonly regarded the near misses as a deviation from normal and should be reported,which confirms the notion in 4I Framework that the individuals’ preconscious recognition of differences marks the beginning of organizational learning [18].
While it was generally reported that nurses held an inactive attitude towards error reporting [16,26,27],this study identified that frontline nurses have a leading role in exposing near misses,mainly reflected in their efforts to optimize the exposure effect.For example,nurses used different ways of exposing near misses based on the risk of near misses.This leading role can be explained by the nurses’ deeper understanding of the potential risks of near misses and the necessity of improvement since they are the last line of defense for safety.Another reason may be the less requirement of personal ability to expose near misses.However,as the international studies reported that the fear of punishment was a deterrent to nurses’participation of error reporting[16,27],our study showed that a non-learning working climate,particularly the punitive management style and a dearth of support could reduce nurses’willingness to take a leading role in exposing near misses,even for near misses with high risk.Cohen et al.[10]suggested that creating a work environment in which staff felt empowered,convenient and safe to report events was the key to promote SOPSB.
5.2.Pushing forward the cause analysis within limited capacity to validate learning
Cause analysis has been recognized as the critical step to generate knowledge from errors by identifying the potential risks and improvement opportunity [18].This study found that recognizing the underlying causes was the core aspect of SOPSB and laid the foundation of the following activities,which has been described earlier[8,11].Crossan et al.[18]indicated in the 4I Framework that developing explanations about learning opportunities is the sign of knowledge production and the real beginning of learning.Although the cause analysis was typically reported as the managers’ work,this study suggested that for near misses,cause analysis was sometimes recognized as an in-role duty of nurses.The main reason is that nursing work is more likely to be disrupted by near misses and nurses have first-hand access to the useful data regarding causes.Besides,as Sarvadikar et al.[28] reported,nurses had a higher expectation of being blamed than doctors when an error occurred,which may also inspire the nurses’ passion for cause analysis.The third reason might be that the selected hospitals in this study are well respected for their efforts in establishing patient safety culture;it has been reported that in organizations grounded in safety culture,the focus is on the how of errors rather than placing blame on who.Furthermore,the 4I Framework showed that a shared understanding of the interpretation of cause promotes learning at the organizational level.Likewise,this study demonstrated the nurses’ efforts in learning from near misses by communicating causes,such as discussing and transmitting the causes across the organization,which was consistent with earlier studies that sharing ideas about the causes of problems was the valuable part of SOPSB[8,9].Therefore,an open and smooth crossboundary communication channel is needed to facilitate organizational learning from near misses.
However,despite the nurses’ passion in cause analysis of near misses,there are still challenges,especially when it comes to system problems.The main barrier might be that since near misses do not cause actual harm,they rarely get chances to be discussed deeply within professional groups just like the adverse events,which makes the analysis mainly depends on individual ability rather than collective efforts.However,evidence suggests that most health employees including managers lack the necessary knowledge,skills and energy to search deeply and accurately into the underlying causes [29].Besides,a dearth of support and the organizations’ overemphasis on individual vigilance to ensure safety might be another reason.The Chinese traditional culture typically encourages self-criticism rather than examining the system process when an error occurs,which also helps explain why self-reflection became the primary way of analysis in this study.These findings can be considered as part of recommendations for providing comprehensive system-based safety education to increase the nurses’ effective participation in cause analysis.
5.3.Balancing the active and passive role during improvement project to explicit learning
This study found that the trial on working improvement was viewed as the best reflection of SOPSB.Participants reported thatonly when the countermeasures were identified and brought into effect could the nearmissesbepossibly prevented,which has been reported earlier [8,9].This finding demonstrates the notion in the 4I Framework that identifying and implementing a coordinated actionwas the symbol of learning at the organizational level [18].Although the nurses’efforts in improving work have not been well documented in Chinese hospitals,several participants in this study expressed a strong desire for trying out countermeasures to fundamentally solve near misses.This enthusiasm might come from nurses’being tired of the disruption of recurrent near misses and the fear of the potential consequences.But meanwhile,participants reported that nurses are mostly passive followers and have limited autonomy during improvement process,which may be a result of the traditional work pattern dominated by managers.The previous studies showed that nurses generally felt their role was unimportant in quality improvement projects and few were involved in any safety initiative[29,30].Furthermore,this study showed that nurses were sometimes criticized for their high enthusiasm in improvement activities,especially by those with a more passive view.This has been rarely reported becausetheideaoffullyparticipatinginqualitymanagementhaslong been advocated.This finding is understandable in China since nurses are commonly viewed as the passive performers of physicians’order,and the traditional culture advocates that people should know their distance or place,with low tolerance for employees who are perceived as horning in on management work.These findings raise the question of whether the failure of learning from near misses lies with the employees’poor activities or the lack of management support,and a culture change may be needed.
5.4.Promoting continuous improvement with passion while feeling low-powered to achieve a successful learning
Results of this study showed that in complex clinical work,key elements of SOPSB are the continuous evaluation and improvement of measures.Other studies likewise confirm that promoting longterm change should be an important part of SOPSB [9,25].Phimister et al.[31] indicated that only through continuous evaluation and feedback could practice be pushed to a higher level and fundamentally solve near misses.From a theoretical standpoint,the 4I Framework supports that embedding coordinated action into work systems acts as the symbol that learning really happened at the organizational level[18].
Due to the high risk of being involved in accidents caused by invalid countermeasures,many participants in this study appreciated the continuous improvement and voiced concern about how their suggested actions were integrated into work routines.However,the work of continuous improvement sometimes got bogged down in clinical work and did not realize the intended effect.Considering the characteristics of near misses and the current working environment,the ‘instant gratification’ and‘discounted countermeasures’ might be the main reasons.On the one hand,the no-harm feature of near misses diminishes the overall concern about the necessity of continuously improving work.Additionally,the busy clinical work and limited authority perceived by nurses also make them feel content with the instant effect of countermeasures in the short run.White et al.[32] reported that nurses generally found it difficult to find time for improvement without additional resources.On the other hand,due to a lack of knowledge,skills,or resources,the planned improvement measures are sometimes inaccurately implemented or discounted,making it difficult to evaluate the real preventative effects and improve the work further.These findings emphasize the importance of setting up an effective evaluation and feedback mechanism,thus ensure the measures take place as expected and increase the nurses’ awareness of continuous improvement.
5.5.Limitations and future research
Participants in this study may have been excessively positive in their perceptions because no one else had previously asked them what they thought about near misses and SOPSB,and they seemed to expect some routes for their concerns to be taken seriously.Besides,to compensate for the nurses’inaccurate understanding of near misses and SOPSB,this study selected participants in highquality tertiary hospitals who had more chances to access the relevant content in staff training.However,on the other hand,the purposive sampling might influence the findings’ automatic extrapolation to the lower-level healthcare settings.Moreover,it is difficult to comment on our findings in relation to the previous literature as the absence of comparable studies.
Despite these limitations,the insights gained from this study still generated robust evidence for practice and provided a good foundation on which to build further studies.The findings provide evidence that validates the link between nurses’ practice of learning from near misses and the 4I Framework,which can be used as a foundation to further develop educational materials and management programs to implement the 4I Framework in clinical work,thus,to improve the learning effect from near misses.Besides,this study has pinpointed many particular items regarding the nurses’sense of SOPSB in learning from near misses,which can be amalgamated into an instrument and lay the foundation for the quantitative study.Moreover,this study incorporated nurses as a whole rather than distinguishing them between have and have not truly experienced near misses;future studies are suggested to explore different perspectives on these two nurse groups.
6.Conclusion
Learning from near misses is a critical but challenging aspect of patient safety.This study underpinned theoretically by the 4I Framework to demonstrate how the front-line nurses promote organizational learning from near misses through the lens of SOPSB.Since nurses expressed equal parts passionate and lowpowered regarding SOPSB in learning from near misses,this study highlighted the importance of developing a near-missesbased education and establishing learning,supportive working environment,thus improve the learning effect from near misses and promote patient safety.
Data availability statement
Authors declare the absence of shared data in the present study.
Funding
This work was supported by National Health Commission of the People's Republic of China,China [Number:201502017] and the Peking Union Medical College,School of Nursing,China [Grant Number 2015002017].
CRediT authorship contribution statement
Yi Yang:Conceptualization,Investigation,Data curation,Software,Formal analysis,Writing -original draft.Huaping Liu:Supervision,Methodology,Validation,Data curation,Writing -review &editing,Funding acquisition.Gwen D.Sherwood:Methodology,Writing -review &editing.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
The authors gratefully acknowledge all the participants in this study for their time to participate in the study and providing valuable information.The authors would also like to acknowledge Prof.Xinjuan Wu for her professional assistance in conducting this research.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2021.08.001.
 International Journal of Nursing Sciences2021年4期
International Journal of Nursing Sciences2021年4期
- International Journal of Nursing Sciences的其它文章
- Nursing students’ attitudes toward mobile learning:An integrative review
- Mobile health applications for the care of patients with breast cancer:A scoping review
- Nurses’ experiences in voluntary error reporting:An integrative literature review
- A study of the relationship between nurses’ experience,structural empowerment,and attitudes toward computer use
- Resilience of nurses at the epicenter of the COVID-19 pandemic in Lebanon
- Exploring the employment readiness and return to work status of breast cancer patients and related factors