
Experience of the patient’s success in facing post-stroke urinary incontinence:the patient’s perspective
2021-09-16 13:21HelttyHelttyRtnSitorusEviMrthNuryNusdwinuringtys
Frontiers of Nursing 2021年3期
Heltty Heltty, Rtn Sitorus Evi Mrth, Nury Nusdwinuringtys
aFaculty of Nursing, Medical Surgical, University of Indonesia, Depok, Jawa Barat 16424, Indonesia
bFaculty of Public Health, University of Indonesia, Depok, Jawa Barat 16424, Indonesia
cFaculty of Medicine, University of Indonesia, Depok, Jawa Barat 16424, Indonesia
Abstract:Objective: Post-stroke urinary incontinence (UI) is one of the sequelae of stroke.This situation affects all aspects of the patient’s life – physically, psychologically, socially, and spiritually.This study aimed to investigate the experience of patients’ success in facing a post-stroke UI.Methods: A qualitative study using the Rapid Assessment Procedure (RAP) approach was used in this study.Informants were selected using purposive sampling.In-depth interviews with as many as 8 patients who had recovered from post-stroke UI and living in the greater area of Southeast Sulawesi (Indonesia) were conducted.In-depth interviews were also conducted with 8 caregivers and 2 nurses.Data were analyzed using a thematic analysis approach and interpretation of data was based on Humanbecoming theory and Self-care deficit theory of nursing.Results: Five successful things the patients experienced during post-stroke UI were identified.The five successes were as follows:they provided information to get to know and understand post-stroke UI, followed the procedures to overcome post-stroke UI, conducted self-control exercises and stayed motivated, performed daily activities independently according to ability, and made use of family support and peers’ attention.Conclusions: These findings indicated that persistence, belief, independence, and social support (family and peer) made patients to successfully face their post-stroke UI and improved their quality of life.These findings also became the basis for developing a poststroke UI management model based on Humanbecoming theory and Self-care deficit theory of nursing.
Keywords: patient’s perspective • experience of patient’s success • post-stroke urinary incontinence
1.Introduction
Stroke is a chronic disease that causes several sequelae, one of which is urinary incontinence (UI).UI is characterized by an unconscious leakage of urine.This condition can occur immediately after a stroke or can occur later.1The prevalence of post-stroke UI is between 32% and 79%, of which around 25–28% experience UI after discharge from hospital, and about 15% experience UI 1 year after discharge from hospital.2
Post-stroke UI as a chronic disease requires holistic treatment.Many chronic health problems will respond well when handled from a holistic perspective.3The holistic health view focuses on the patient’s health care needs; these include not only needs related to the physical condition of his/her health, but also subjective aspects related to the social representation of his/her health condition.
The results of a systematic review that identified 10 studies reported that the use of incontinence pads and toileting programs were the most commonly used management approaches, and there were no studies that identify efforts to maintain patients’ continence care in homes.4Nurse-led strategies for continence care in hospitals tended to focus on product identification and containment of incontinence, rather than active treatment.5Observation at the hospital of Southeast Sulawesi also showed that the management of continence care tended to focus on the use of UI products, such as diapers.This research will be used as the basis for developing a poststroke UI management model for holistically and continuously caring for the patient at the patient’s home.Thus, development of a holistic post-stroke UI management model that facilitates continuous care at the patient’s home needs to be prioritized.
Although continence promotion had been carried out, a holistic care approach to the treatment of poststroke UI had not been undertaken.UI is still taboo in society.The results found that the embarrassment rate of UI patients reached 60%.6People with UI often chose not to leave home because they were afraid and ashamed of urine coming out in public places, feeling wet, and smelling of urine.7The symptoms of UI cause embarrassment, distress, low feelings of self-worth, and depression; in consequence, they influence people’s ability to take part in rehabilitation.8Around two-thirds of people with incontinence will never seek professional advice.9However, over time, they would develop expertise in facing their own condition.A person living with bladder dysfunction may try lots of different ways to cope with their situation.9For this reason, exploration of the patient’s experience during the post-stroke UI was required.
Exploration of patient experience during post-stroke UI is part of managing UI.Parse’s theory of Humanbecoming recommends that individual experiences can be a focus in public health nursing.10Developing nursing care based on concepts, principles, and values about care in Parse’s theory contributes to improving individual health.11Parse hypothesized that the theoretical view of nursing must focus on the quality of life from the perspective of the person.The paradigm in the theory of Humanbecoming emphasizes the importance of the type of specialized care that is needed by patients who choose and assume responsibility for their own health, and the purpose of such care is to facilitate nursing staff to observe and redress patients’ condition through their respective perspectives.Patients are health experts and nurses address their emotional, physical, spiritual, and psychological needs.12
In addition to Humanbecoming theory, this study also used the Orem theory.Orem believes that humans have natural abilities for self-care and nursing and must focus on these abilities.Orem also believes that self-care behavior requires knowledge and motivation because there is fatigue, hopelessness, and false beliefs that illnesses cannot be cured.Self-care can be considered as an individual’s capacity to carry out all activities necessary to live and survive both in terms of physical, psychological, and spiritual needs.This study aims to investigate the experience of patients’ success in the face of post-stroke UI they experienced.
2.Methods
2.1.Study design
The research design used was Rapid Assessment Procedure (RAP).RAP was used as a method for directly interacting, discussing, or listening to those experiences that the patient has undergone in dealing with poststroke UI.In-depth interviews were used by researchers to gain an insight into the daily experience of patients while undergoing post-stroke UI.The in-depth interview guide was developed based on Humanbecoming theory and self-care nursing deficit theory.
2.2.Study participants
Informants in this study were selected using purposive sampling.Data about the informants were taken from the medical records hospital of RSU Kota Kendari and RSU Dr.Ismoyo Kendari, and then researchers conducted a home visit to find informants who fit the established criteria.All informants were domiciled in Kota Kendari, Southeast Sulawesi (Indonesia).Informants were in compos mentis awareness, medically stable conditions, had successfully overcome post-stroke UI, had no swallowing disorders, no psychiatric disorders, no prostate hyperplasia, were able to read and write, and do not experience Dementia or Alzheimer’s.
2.3.Procedures
Data collection was carried out for 3 months during the 2019 period.Data was collected using in-depth interviews and informant observations.During data collection, the researcher was assisted by an assistant in charge of recording the nonverbal responses of informants.The length of in-depth interviews for each informant varies between 40 min and 60 min.Informants were explained that the purpose of this study was to explore the experience of patients’ success during the experience of post-stroke UI.This experience will provide input for developing a post-stroke UI management model.Informants signed the informed consent form to be an informant, were willing to share their experience, and expressed their consent to participate at any time.
The interview began with the main questions that were asked in this study:“How did you deal with a stroke that you experienced, and can you explain it?”.Then the informant was asked, “Can you tell us what were the opportunities and difficulties during overcoming post-stroke UI?”, “What beliefs did you have in facing post-stroke UI?”, “What were your strengths when faced with post-stroke UI?”, and “Can you tell us how you met the needs of daily activities during post-stroke UI?”
Information that had been collected from patient informants was verified for validity by conducting interviews with caregivers and nurses’ informants.This was done in an effort to triangulate data sources.13Further, this was done through in-depth interviews with eight caregivers and two nurses who treated informants, and each of these nurses had served at the RSU Kota Kendari and RSU Dr.Ismoyo Kendari hospitals for 10–15 years.Caregiver informants consist of four women and four men, aged between 30 years and 40 years; a caregiver was someone who had a family relationship with the informant (informant’s spouse, child, or relative of the informant).Some caregivers lived in the same house as the informant and some do not live together with the informant but in a location close to the informant’s house (but still in the same village/region).Caregivers were in a condition of compos mentis awareness, have not experienced psychiatric disorders, were able to read and write, and were willing to provide the information the researcher needed by signing informed consent to become an informant after receiving an explanation from the researcher that the information provided would be kept confidential.
Data that were declared valid through triangulation will give researchers confidence about the validity of the data; thus, there was no doubt in making conclusions about the research conducted.However, not all data were checked back to caregivers and nurses, but only data relating to patient behavior in dealing with post-stroke UI.In addition to triangulation of data sources, this research also used triangulation of data collection methods, namely in-depth interviews and observation.
2.4.Data analysis
Data analysis began by transcribing data.All interviews were recorded using a recording device, then transcribed into narrative form (verbatim),and later transferred to a computer for analysis.All pages were numbered and coded with informants’ contact numbers.Left and right margins were made wider.The left margin was used as a place for coding and notes, while the right margin will be used for commenting on content.The researcher notes were made in the left margin by using bold letters to separate from the interview text.The results of observations/field notes were also transcribed into narrative form to get a complete picture during the interview.
The verbatims were read repeatedly and were matched with the recording.The answers of the informants that have been transcribed were grouped according to the research questions.In each of the informants’ answer sheets, the researcher identified keywords that fit the purpose of the study.Then, the same keywords were grouped in one category, after which themes and sub-themes were determined.Ideas about themes were noted in analytical notes and discussed within the team.This led to the development of five key themes:“provided information to get to know and understand post-stroke UI,” “did the ways to overcome post-stroke UI,” “conducted self-control and stayed motivated,” “performed daily activities independently according to ability,” and “family support and peer’s attention.”
To ensure trustworthiness, we applied a thematic analysis approach.14Credibility was demonstrated by the way in which the researcher provided the transcript of the data for re-reading by the informant.If the informant revealed that the transcript was in accordance with his/her experience, then the transcript was considered to have fulfilled its credibility.The researcher would ask the informant to sign the transcript sheet if the data was appropriate and matched with the informant.For dependability, it could be achieved with an audit inquiry that involved reviewing data and documents that is supported wholly and in detail by the supervisors and experts who were involved in this research through a consultation process.They also played a role in helping to examine the themes found in this study.For confirmability, researchers confirmed the findings of this study in consultation with expert researchers and confirmed data/information in scientific circles, including senior nurses in the field of neurological nursing.For transferability, a detailed description of the methodology and context had been carried out and sampling was done purposively.
3.Results
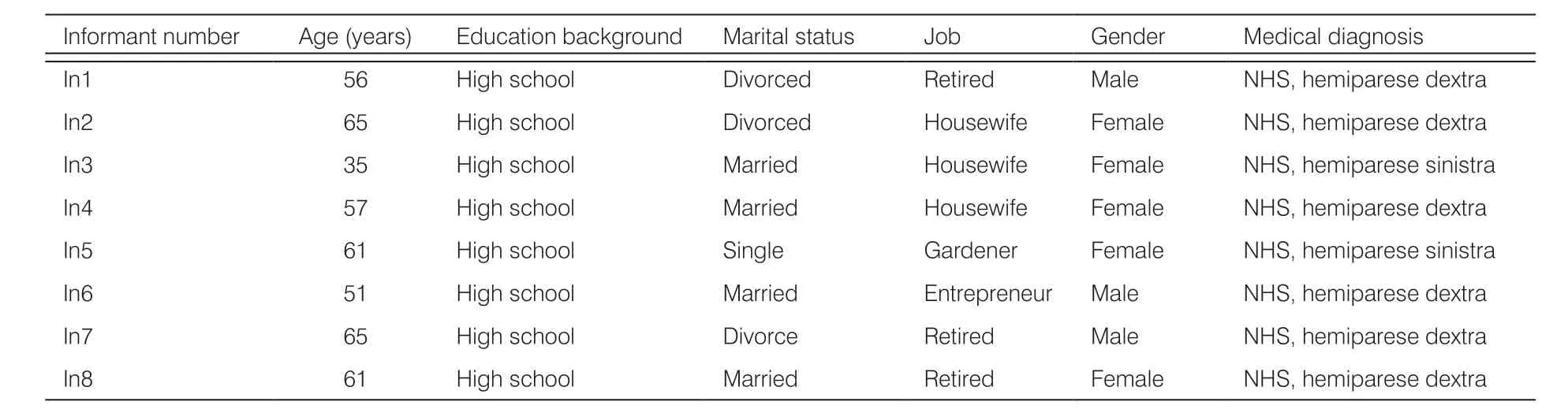
The characteristics of informant data were heterogeneous based on age, gender, marital status, and occupation.The age range of informants ranged from 35 to 65 years; in general the informant’s last education was high school, marital status was married partly, and the rest were widowed/widower and not married.Some informants were retired civil servants, the rest were entrepreneurs, housewives, and gardeners.All informants were Moslems.More than half of the informants are women and the rest are men.All informants were medically diagnosed with ischemic stroke (nonhemorrhagic stroke) with hemiparese dextra or sinistra.More than half of the informants had been treated at RSU Kota Kendari and some were treated at the RSU Dr.Ismoyo Kendari.(Table 1)
There were five themes and six sub-themes that had been identified (see Table 2).The five themes were:provided information to get to know and understand post-stroke UI, carried out the measures that are necessary to overcome post-stroke UI, conducted themselves with self-control and stayed motivated, performed daily activities independently according to ability, and availed of family support and peers’ attention.The themes found were also clarified with nurses as key informants who would provide their views, knowledge, and experience while treating post-stroke UI patients to increase researchers’ confidence in these results.Each theme will be explained and illustrated through a quote.

Table 2.Thematic analysis.
Theme 1:Provided information to get to know and understand post-stroke UI
This theme incorporated two sub-themes:information aboutinformant’s physicalandpsychosocial condition during experienceof post-stroke UI.
Subtheme 1.1.Information on physical condition during post-stroke UI
Some informants could not urinate in the bathroom as usual since a stroke, and so there were informants who urinate in their pants, gloves, mattresses, and bottles, especially at night.Informants urinate in pants, sarong, and on mattresses because informants could not resist urinating and had weakness in their hands and feet, thereby affecting the informants’ functional ability to reach the toilet and urinate in the toilet.There were informants who urinated in aqua bottles at night because they were reluctant to wake their wives who were sleeping.The following is the statement of an informant:“Since I had a stroke, I sometimes did not feel urinating...so I just came out (urinate)...I was also limited to move...my leg was weak...I could not go to the bathroom alone, sometimes my family helped me to the bathroom”.(In3, In5);“Sometimes I felt like urinating but I could not hold it anymore, so everything was wet, even the mattress was sometimes wet.” (In2)
Subtheme 1.2.Information on psychosocial conditions during post-stroke UI
The informants felt ashamed and inferior to interact with others.The informant expressed his/her reluctance to leave the house for fear that urine would come out and wet their clothes, so that others would see their clothes being wet and feel embarrassed with the smell of urine.This gave rise to unpleasant feelings (shame, feelings of anxiety, and insecurity) for the informant.The following is the statement of another informant:“I could not go anywhere at that time...I could not come to the neighbor’s celebration because it was uncomfortable when people saw that my clothes were wet and smelled of urine.” (In3)
Note: In1—In8, informant 1—8; NHS, non hemorrhagic stroke.

(Continued)
The informant felt that during illness the informant weighed on the family.The informant could no longer carry out his role at home and in the surrounding environment.Almost all informants revealed that during an illness in which UI was a predominant symptom, they could not do anything, could not work, could not help the family to make a living, and were no longer active in the surrounding social activities.The informant expressed this by shedding tears and was silent for a moment while staring blankly ahead.The following is the statement of yet another informant:“I could not do anything at that time...I bothered my children...I could not make and sell any more...just wanted to pee like a child who pees in his pants.I botheredmy family to clean my pee (speechless, looked down, took a deep breath).” (In2)
Theme 2:Took steps to overcome post-stroke UI
Informants preferred to try urinating in the bathroom.All informants revealed that they did not use pads or diapers because they were uncomfortable.Some informants had experienced irritation in the diaper use area, and for this reason they didn’t want to use pads anymore.All informants tried to walk to the bathroom to urinate.The informants tried to hold urination in various ways such as pausing in his/her walk for a moment if he/she was in a position to walk to the bathroom while pressing his/her thighs together.Initially, this method was not easy to do and the urine still came out to wet their clothes, but the informants continued to do this exercise because of their desire to recover and not wanting to burden the family.When the informants hold back urination, they also distracted his/her urinate sensation by reciting dhikr, praying, and imagining that he/she would do something pleasant if healed.As the informant states:“I hold urination until I arrived in the bathroom...I stopped walking for a while to urinate.Usually I pray, Allah (God)...please heal me from this disease (shed tears).” (In5).“I hold my urination...slowly...I pressed my thighs so that my urine did not come out.I tried to hold it in, at first, but my urine remained coming out and the floor became wet...but I kept trying.”(In8)
During the recovery of post-stroke UI, the informants also did not limit fluid intake.The results of the observation showed that all informants did not experience signs of dehydration, such as dry lips.The informant also checked his/her health at the neurology clinic and/or rehabilitation center.However, not all informants checked their health regularly due to differences in the informant’s control schedule and the availability of family time that would deliver, and also because of the geographical situation of the location of the house, as stated by the following informant:“Since I was discharged from the hospital (more than 8 months), I only twice took control of my health to the doctor and to physiotherapy...I was rather difficult...like this, my house on a hill...I was afraid of falling if I went down the hill (towards road), lots of rocks, even though I was held by my children but still I was afraid to fall”(In8)
Some informants overcame post-stroke UI by modifying the house, which was done by making a cubicle for informants to rest in during the day.Inside the cubicle, there was a hole for the informant to urinate.The cubicle was made by the informant’s husband by breaking down a few meters (about three meters) of the back wall of the house to make a small cubicle.The walls and floor of the cubicle were made of boards, measuring 3 4 meters, in which there was a hole to urinate for the informants.The hole was made by piercing the floor of the board and then covering it with a plastic mat.There was a bucket filled with water and a dipper for informants to clean up after urinating.The hole was closed again with a plastic mat after the informants urinated.Disposal was made directly into the garden and did not cause odor, but the family did not make a permanent and closed drainage, due to financial constraints.The cubicle looked clean, cool, and the air circulation was smooth because three windows were installed that were quite large.This simple toilet was very helpful for the informant to urinate, and the informant only takes five steps or moves his buttocks and legs in a sitting position to reach the hole.The family also felt that they were not too bothered to help the informant urinate with the existence of a simple toilet (hole).The following is the caregiver’s expression:“As long as there was no hole (toilet), I was pretty tired taking care of my wife (informant) back and forth to the bathroom, I lifted her into a wheelchair then I pushed her into the bathroom and I lower down her again to sit her on the toilet.It felt very heavy because my wife’s body weight was almost 80 kg...my waist felt like it was going to break...so I made a room from the board and the floor was also a board, I made a hole for my wife to urinate, the drain directly into the garden so it didn’t smell..circulation the air was also smooth...only at night we couldn’t sleep here because the air was very cold.”
The informant also urinated in the nearest bathroom, so that it was easier for the informant to reach the bathroom.
The servant, however, declined everything, and only begged for a horse and some money to enable him to travel, as he was anxious to see something of the world
Theme 3:Conducted themselves with self-control and stayed motivated
This theme incorporated four sub-themes:positive thoughts, drawing closer to God, holding back emotions, andbeliefs.
Subtheme 3.1.Positive thoughts
Positive thoughts expressed by informants through some of their statements included the following, namely that:all must be dealt with, there were still many stroke patients whose conditions were worse, must be enthusiastic in dealing with this disease, should take advantage of the time and opportunity that were given, must try to fight this disease, must be able to walk so that it was possible to urinate in the bathroom.As the informant put it:“I thought this all must be dealt with, there were still many people with strokes whose condition was worse than mine, filling life must be enthusiasm...illness must be dealt with.It was a shame if you didn’t take advantage of the available time and opportunity.Especially in terms of age, still given a long life...this was what I thought should be utilized.”(In1, In5)
Subtheme 3.2.Drawing closer to God
Drawing closer to God is identified from the expressions of informants who often pray for healing to God, read the holy book (Al-Qur’an) as a way to get closer to God, surrender, and pray.More than half of the informants said that all this was left to God.
Subtheme 3.3.Holding back emotions
Informants also control emotions by always being grateful, being patient, and holding back emotions without being easily offended and not easily getting angry.
The informants believed that they could recover from the post-stroke UI, informants were optimistic about it, and they were confident that everything could be better.The statement of the informant follows:“sure, God willing (Insha Allah), get well, hope in the Almighty...while we tried our best.”(In2, In3, In7)
Theme 4:Performed daily activities independently according to ability
Informants tried to keep doing their daily activities independently, such as eating and dressing without the help of a caregiver.The informant also tried to go to the bathroom by walking with a cane and holding on to the wall.Some informants have started shopping at shops near the house to buy their needs because they have been able to resist the urge to urinate and were able to count some money, but remain under the supervision of a caregiver.
Theme 5:Family support and peers attention
Informants revealed that they could face this all because of family assistance.Families helped care for them, took the informants to the hospital to check their health, provided walking aids, and made simple toilets.The family also always encouraged the informant, so that the informant was increasingly diligent to do the exercises.All family members (spouse, children, grandchildren, and nephews) helped in taking care of the informant.There were informants whose children took turns coming to care for them, cook, and help bathe.Some informants were cared for by their nephews and brother because they were not married; on the other hand, some informants were cared for by their children, son-in-law, and grandchildren due to loss of spouse (died and/or divorced).The informant felt happy with the help and attention from the family.One informant said:“My children took turns coming to took care of me every day, for cooking, helped me take a shower, helped me urinate.Almost every night I woke my husband because I wanted to pee and my feet were hurt.Children also joined the venture and bought me a cane and wheelchair (smile).” (In4) “During my illness I was assisted by my relatives and nieces.Since I was not married, my niece always came to take care of me.” (In5) “The family of my wife also always helps in taking care of me.In-laws, parents, and siblings also gave attention and motivation.” (In6)
The informants felt that the assistance provided by the family was more than enough, and although the caregivers felt tired while caring for the informants, they still took care of them.The members of the family as caregivers also revealed that their sleep was often disturbed, that their weight dropped during caring for the informant, and that they felt tired, but the family still extended care for the informant.The family expressed a sense of concern, could not bear, and was not ready if the informant left them (died) in this sick condition.This was expressed by the family with tears.The following is the caregiver’s statement:“I was “half-dead” while taking care of my wife, sometimes people met me asking if I was sick.My wife was sick but I looked sick...my mind as a husband when my wife was sick like I was also dying...I could not bear it if my wife left me at an age like now, I still want to be together.It feels unbelievably sad...I felt bad about eating.But we always tried to give the best for my wife’s recovery.” ( caregiver In4)
Besides support from caregivers, informants also received support and attention from friends who came to visit the informants.They shared experiences and information related to actions taken during overcoming post-stroke UI.This made the informant feel happy and not alone in dealing with his illness, so that the informant became more eager to recover.
4.Discussion
4.1.Theme 1:Provided information to get to know and understand post-stroke UI
Information was essential for the nurse to be able to care for the patient, information was necessary to know the patient’s conditions.15Information delivered by patients is related to their physical and psychosocial condition, and reflects the patient’s knowledge of their conditions that can assist nurses in determining appropriate interventions.Nurses have the potential to identify people with incontinence, establish appropriate interventions, and provide valuable health education to empower patients.5Considering several etiologies and related factors with the occurrence of UI following a stroke, a thorough assessment is needed to describe the type and severity of incontinence, so that treatment can be tailored to meet the individual’s needs.16Several studies concluded that the lack of nursing staff’s knowledge about continence is an indication of poor continence care.5Thus, nurses’ knowledge in the care of post-stroke UI patients needs to be improved, including in providing a comprehensive assessment.In holistic nursing, all aspects of patients and effects of such nursing on the treatment process are considered, and these aspects include the patients’ thoughts, emotions, cultures, opinions, and attitudes that are factorscontributing to recovery, happiness, and satisfaction.17
4.2.Theme 2:Participated in measures to overcome post-stroke UI
Taking steps to overcome post-stroke UI illustrates the patient’s ability and skills to achieve healing.In the theory of Humanbecoming, healing is seen as a personal force that arises from an individual’s good relationship with his environment.Health is a personal/individual commitment in which a person participates in creating his health with others and the environment.18The ability of informants to carry out ways to overcome the occurrence of post-stroke UI that they experienced reflects the personal values they hold and the uniqueness of the individual in improving his quality of life.The theory of Humanbecoming also mentioned that humans choose to adjust or not adjust to others, and choose a few things when they pursue their hopes and dreams with something familiar or foreign.
Based on the results of this study, some ways in which the informant overcame his post-stroke UI showed the ability of informants to know, understood, and decide what should be done to overcome the disease.This was based on the knowledge and desire of the patient to recover, and for this reason the informant carried out a process of shifting (transforming) his/her health pattern by prudently exercising the choice to change attitudes in leading everyday life.In the theory of Humanbecoming, it is stated that transformation in health patterns can occur when individuals find insights about themselves that were previously unclear, and when they find ways to change toward the hopes and dreams that they value.19,20Besides, the informants’ desire to recover made them always fulfill the necessary measures to overcome post-stroke UI.This was also one of the strengths of the informants during the face of post-stroke UI.
4.3.Theme 3:Conducted themselves with self-control and stayed motivated
Self-control described how informants chose and found ways to deal with the situation that they experienced.This relates to the belief values that informants had.In Parse’s theory, it is stated that beliefs reflect what is important in an informant’s life related to his health, which is the basis for informants to make choices about how to think, act, and feel.18The theory also mentioned that health cannot be given or taken, controlled or manipulated, assessed, or diagnosed.On the contrary, health is the way people live their values according to their wishes, hopes, and dreams.For this reason, it was necessary to provide some advice and guidance—including spiritual guidance—that could improve patient self-control when managing poststroke UI.
Human beings have various physical, psychological, social, emotional, intellectual, developmental, cultural, and spiritual needs.Therefore, one of the most important components of nursing care is spiritual care.In the context of spiritual nursing, nursing is a spiritually driven profession that aims to improve people’s morale and nourish their souls.21Religious beliefs can help people cope with uncertain circumstances, including in the face of stressful life events.22Positive thinking is important in achieving goals.Positive thinking makes a person to contribute in constructively and creatively.Positive thinkers face the situation with optimism.If they face a stressful situation they judge that it can be controlled and use coping strategies that are functional, efficient, and problem-focused.23Positive thinking can also be used to improve the quality of life.24Spiritual care has a strong influence on health dynamics, attitudes, and behavior and it should not be considered as an element separate from normal nursing care.25
4.4.Theme 4:Performed daily activities independently according to ability
In Orem’s theory (self-care deficit theory of nursing), Orem believes that humans have the ability to care for themselves and whenever this ability is distorted, nurses help individuals to regain their abilities by providing direct care.26In this study, the informant’s independence in carrying out activities of daily living was shown by the ability of the informant to eat and wear a dress without the help of a caregiver, but some activities were still under the caregiver’s supervision such as walking, shopping at a stall, and visiting neighbors who also had a stroke.This illustrates the conditions included in the supportive–educative system in the nursing system (Orem’s theory), where individuals were able to perform actions needed to carry on with day-to-day living, able to learn to take actions that were externally required, or able to take part in therapeutic self-care but failed to do so in the absence of the caregiver’s assistance.20So, their day-to-day life requires guidance from health workers and caregivers.However, in conducting selfcare activities, one should recognisse the active role played by patients in their healthcare rather than the passive one.
4.5.Theme 5:Availing of family support and peers’ attention
Family involvement in patient care is needed, including peer involvement to patient support.Family support and peers’ attention were also some of the things that made patients successfully overcome post-stroke UI.Families contributed to maintain patient welfare by providing emotional and practical support.There had been many previous studies that have shown the effectiveness of care by involving families in patient care, such as this result’s study:there was a significant relationship between costs and only a minimal amount of help was available from healthcare professionals in families involved in supportive care.27
However, involving families as caregivers in patient care needs to be equipped with knowledge and skills related to patient care, and caregivers must also be able to take care of their own health when caring for patients.In this study, we found that caregivers experienced fatigue when caring for patients at home.It was also found in other studies that caregivers reported fatigue and lack of rest, due to increased responsibility for the health of informants, and this resulted in a negative impact on the physical health of caregivers.28Caregivers realized that it was important to take care of their personal health, so that they could continue to care for their sick family members.28
Besides caregivers, peers’ attention was also needed.In this study, the informant felt very happy with the presence of a friend who also experiencing the same disease as the informant.They shared information about the things that they did to achieve their healing.Attention from peers who also experienced the same disease could help reduce feelings of isolation and fear, where peer support could be made available by sharing experiences and providing information about health services that they need.29
Family support and peers’ attention were often recommended as a source of emotional, instrumental, information, and affirmative support for people with chronic conditions.Peers’ attention could offer unique types of relationships, which provided a generalization of experience, social validation, and encouraged feelings of empowerment.In general, peers’ attention was associated with decreased loneliness and feelings of difference, increased social competence, social acceptance, and increased acceptance of chronic conditions.29Family and peer support programs seemed to be one of the effective ways to meet patient needs.Orem believed that the lack of social support to convince patients in complex care situations leads to limitations in self-care behavior.
5.Conclusions
This study highlighted the importance of the patient’s ability to achieve success in facing a post-stroke UI.This success could be achieved by the ability of patients to provide information to get to know and understand the conditions that they experienced and the ability of patients to undertake measures to overcome the post-stroke UI following their belief values.The study conducted stressed the need for self-control and to stay motivated in the face of their illnesses, which also included the ability of patients to carry out their daily activities independently, and social support from nurses, families, and peers who were also needed to achieve the success of patients in facing post-stroke UI.This study was used as an input in developing a post-stroke UI management model based on Humanbecoming theory and self-care deficit theory of nursing.
Acknowledgments
The authors acknowledge the Faculty of Nursing, Universitas Indonesia, Depok-Indonesia, for all valuable support.
Ethical approval
This study was approved by the ethical committee of the Faculty of Nursing Universitas Indonesia, with No.SK-242/UN2.F12.D1.2.1/ETIK.FIK.2019.
Conflicts of interest
All contributing authors declare that no conflicts of interest exist.

- Frontiers of Nursing的其它文章
- Effect of simulation-based teaching on nursing skill performance:a systematic review and meta-analysis
- Application of machine learning algorithm for predicting gestational diabetes mellitus in early pregnancy†
- Nurses’ views of fundamental relational skills used in clinical practice:a cross-sectional pilot study
- Topical use of ozone effectively alleviates the acute symptoms and quality of life of patients with moderate to severe bullous pemphigoid:a randomized controlled trial†
- Mediating effect of work engagement between job characteristics and nursing performance among general hospital nurses
- Training program for caregivers to prevent pressure ulcers among elderly residents at geriatric homes