
Investigation of the factors influencing surgical treatment of duodenal gastrointestinal stromal tumors
2021-08-25 05:48:06YunZiWuYangLiMingWuXiaoHaoZhengYanTaoTianYiBinXie
Yun-Zi Wu,Yang Li,Ming Wu,Xiao-Hao Zheng,Yan-Tao Tian,Yi-Bin Xie
Yun-Zi Wu,Yang Li,Xiao-Hao Zheng,Yan-Tao Tian,Yi-Bin Xie,Department of Pancreatic and Gastric Surgery,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China
Ming Wu,Department of Gastric Surgery,Yun Cheng Center Hospital,Yucheng 043300,Shanxi Province,China
Abstract BACKGROUND Duodenal gastrointestinal stromal tumor(DGIST)is a rare tumor with a specific anatomic site and biological characteristics.As the incidence of lymph node metastasis is very low,the main treatment method is surgery.Two main surgical techniques(local resection and Whipple)are performed in patients with DGISTs.The critical question is which surgical technique to choose.AIM To identify factors influencing the choice of surgery for DGISTs.METHODS The clinicopathological data of patients with DGISTs who underwent surgery between January 1999 and January 2021 were analyzed.We used the Student’s ttest or Mann-Whitney U-test and the χ2 test or Fisher’s exact test to determine the differences between the two groups of patients.Furthermore,we used logistic analysis to identify the relevant factors and independent factors related to the type of surgery.The Kaplan-Meier method was used to analyze the patient’s survival information and Cox regression analysis was performed to determine prognostic risk factors.RESULTS Overall,86 patients were analyzed,including 43 men(50%)and 43 women(50%).We divided the patients into two groups based on surgical technique(local resection or Whipple surgery).There were no differences in the age,mitotic figures,and complications between the two groups;however,the tumor size,tumor location,risk grade,postoperative hospital stay,and abdominal drainage time were significantly different.Based on univariate logistic analysis,the Whipple procedure was chosen if the tumor size was ≥ 5.0 cm,the tumor was located in the descending part of the duodenum,or the risk grade was medium or high.In our research,the five-year overall survival rate of patients was more than 90%.We also describe two DGIST patients with liver metastases at first diagnosis and analyzed their management in order to provide advice on complicated cases.CONCLUSION The Whipple procedure was performed if the primary tumor was in the descending part of the duodenum,tumor size was ≥ 5.0 cm,or the tumor risk grade was medium or high.
Key Words:Duodenal gastrointestinal stromal tumors;Whipple;Surgery;Tumor size;Tumor risk grade
INTRODUCTION
Duodenal gastrointestinal stromal tumors(DGISTs)account for 12%-18% of small intestinal stromal tumors and 1%-4% of all gastrointestinal stromal tumors[1,2].DGISTs rarely break the tumor capsule and seldom cause lymph node metastasis;therefore,surgery is the best method to cure this disease.However,the duodenum is located near the pancreas and biliary tract.A critical question in the surgical treatment of these tumors is which surgical procedure to choose.Two types of surgery are performed in patients with DGISTs:Local resection and Whipple surgery.Traditional Whipple surgery results in severe surgical injury;therefore,local resection is performed to preserve more healthy tissue[3,4].
In recent years,there have been some reports on DGISTs;however,there is a lack of large-scale reports as the incidence of DGISTs is low[5,6].In the present study,we excluded patients with liver metastasis.Therefore,understanding which surgical procedure preserves more normal tissue,especially normal anatomical structures is the main focus of our study.In this study,we investigated the factors influencing DGIST surgery and provide advice regarding the choice of surgery.
MATERIALS AND METHODS
Data collection
All DGISTs were referred to the National Cancer Center/Cancer Hospital,Chinese Academy of Medical Science and Peking Union Medical College,between January 1999 and January 2021.This study was approved by the Ethics Committee of the National Cancer Center/Cancer Hospital,Chinese Academy of Medical Science,and Peking Union Medical College.The diagnosis of DGIST was confirmed by immunohistochemical staining.Inclusion criteria are as follows:(1)Patients who underwent laparotomy;(2)Patients with DGISTs,as proven by pathology or immunohistochemistry(CD117,CD34,DOG1 and Ki67);(3)The tumor was located in the duodenum,as confirmed by preoperative abdominal computed tomography scan,ultrasound,endoscopy,upper gastrointestinal barium swallow,and surgery;and(4)Patients with GIST synchronous with other malignancies were excluded[7].The risk grade of DGIST was assessed by a pathologist.Clinicopathological parameters(age,sex,tumor size,and tumor location)were retrospectively reviewed and documented.The patients were divided into the local resection group and Whipple group.
Statistical analysis
According to the type of distribution,continuous variables are expressed as average(range)or median(quartile)and were compared using the Student’st-test or Mann-WhitneyU-test.Categorical variables are expressed as percentages and were compared using theχ2test or Fisher’s exact test.Furthermore,univariate and multivariate logistic analyses were used to assess the type of surgery.Kaplan-Meier survival analysis was performed using GraphPad Prism 9(GraphPad Software Inc.,San Diego,CA,United States)to compare overall survival.Cox proportional hazards regression analysis was used to identify risk factors for mortality.Statistical analyses were two-sided,and the threshold for statistical significance was defined asP< 0.05.Retrospective analyses were performed using SPSS v26(IBM Inc.,Armonk,NY,United States).
RESULTS
During the study period of 21 years,86 patients with histopathologically confirmed DGISTs underwent surgery at our hospital.Their clinical features are summarized in Table 1,and their pathological characteristics are summarized in Table 2.The patients included 43 men and 43 women,with a median age of 62.15 years(range,26-87 years).The tumors ranged from 2 cm to 28 cm in size and were distributed in different sections of the duodenum with the predominant location being the descending section(55.8%).Fifty-six(65.1%)patients underwent local resection,and 30 patients(34.9%)underwent the Whipple procedure.According to the GIST guidelines of the Chinese Society of Clinical Oncology,immunohistochemical parameters,such as CD34,CD117,DOG1,and SDHB,support the diagnosis of DGIST.
Patients were allocated to two groups according to the surgical procedure they underwent.The patients’ clinicopathological characteristics were also compared.There were no differences in age,sex,mitotic figures,and incidence of complications between the two groups;however,differences in tumor size,location,and risk grade were statistically significant.These results indicated that we were inclined to choose Whipple surgery when the tumor was in the descending part of the duodenum(P=0.017),had a medium/high risk score(P= 0.004),or was ≥ 5.0 cm in size(P= 0.015).Furthermore,patients who underwent Whipple surgery had a longer postoperative hospital stay(P= 0.000)and abdominal drainage time(P= 0.001,Table 3).
Logistic analysis was used to determine the factors that influenced the type of surgery(Figure 1).In univariate logistic analysis(Table 4),the risk factors for treatment included tumor size ≥ 5.0 cm(P= 0.026),tumor location in the descending part of the duodenum(P= 0.019),and medium/high risk score(P= 0.007).We then used these three parameters to build a multivariate logistic analysis model(Table 4).None of these parameters were independent factors for the type of surgery.
It is known that compared to local resection,Whipple surgery results in serious surgical injury and can result in a higher incidence of postoperative complications.In this study,we found no difference between patients who underwent Whipple surgery and those who underwent local resection(Table 5).
Overall,48 patients had tumors in the descending part of the duodenum.We determined the best surgical option for tumors in the descending part of the duodenum.We compared the clinical characteristics of patients who underwent the two types of surgery.Of these,only the duration of postoperative hospital stay(P=0.000)and abdominal drainage time(P= 0.001)were statistically significant(Table 6).
Consistent with previous reports,DGIST is a low-grade malignant tumor with a good prognosis.We used the Kaplan-Meier method to assess the survival curves.The results showed that more than 90% of all patients lived longer than 5 years(Figure 2).Cox regression analysis was used to identify risk factors for mortality.The differences were not statistically significant(Table 7).
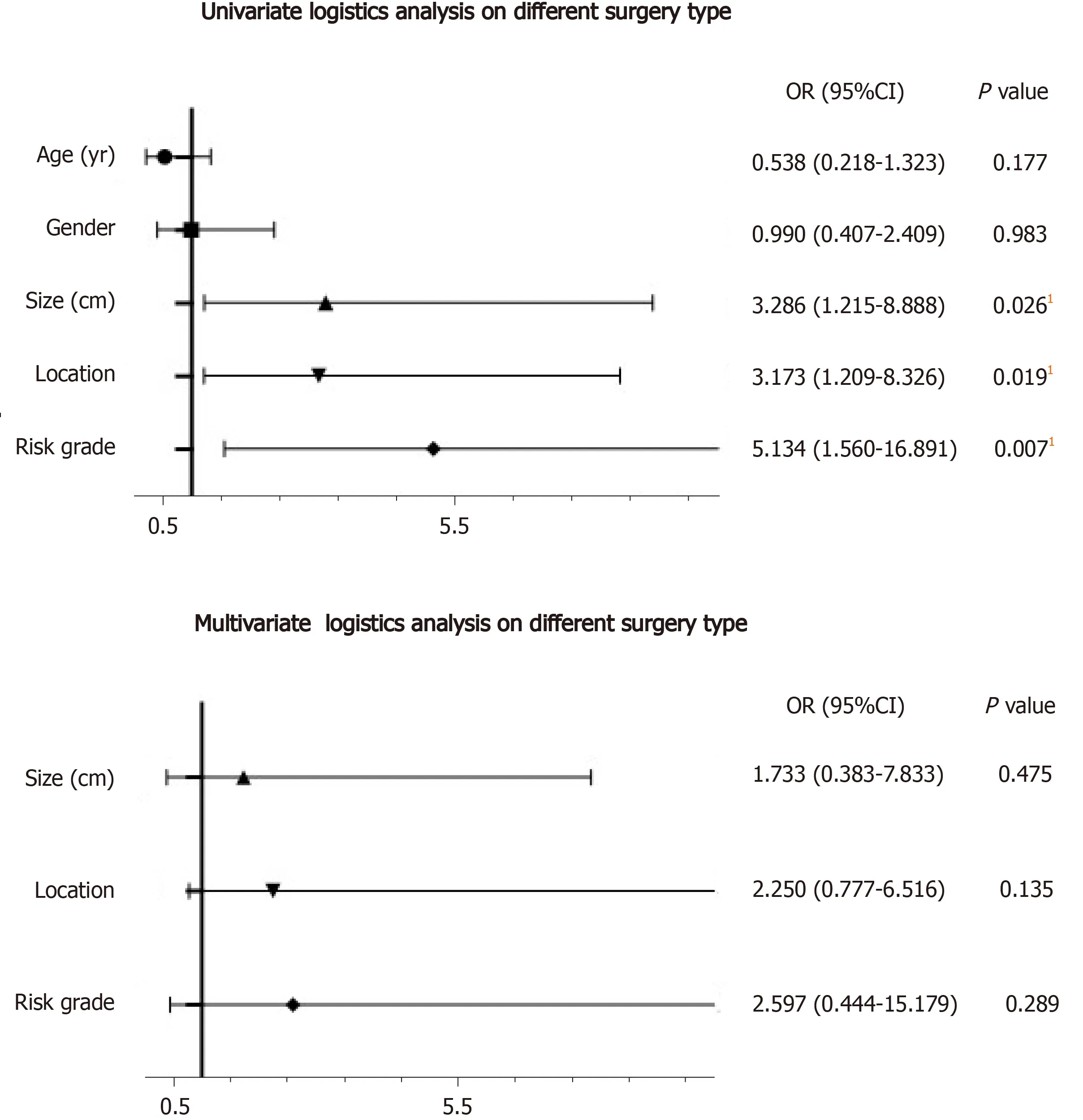
Figure 1 Univariate and multivariate logistic analyses of different surgical procedures.1Statistically significant.
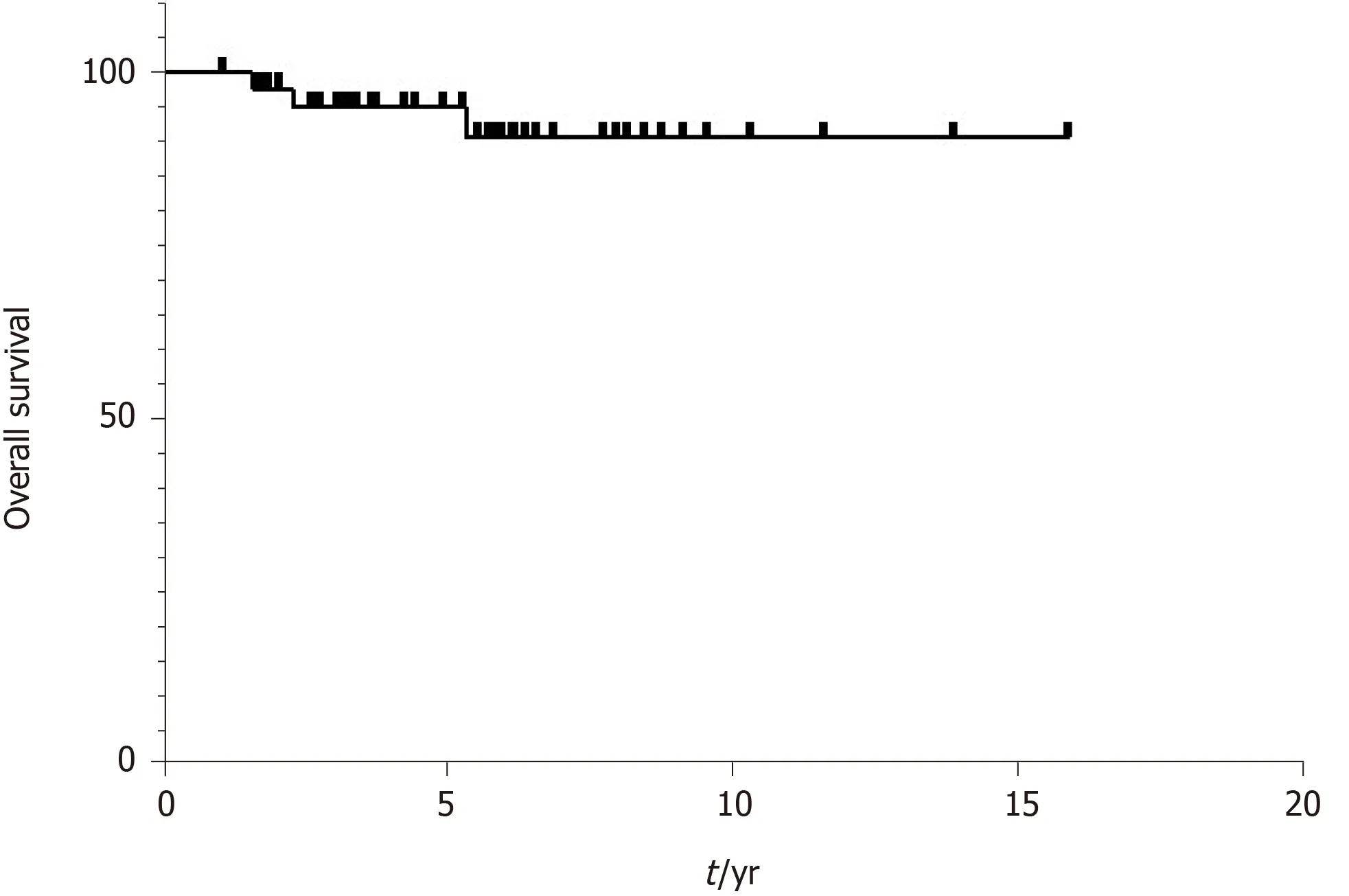
Figure 2 Kaplan-Meier survival graphs of overall survival in patients with duodenal gastrointestinal stromal tumors.
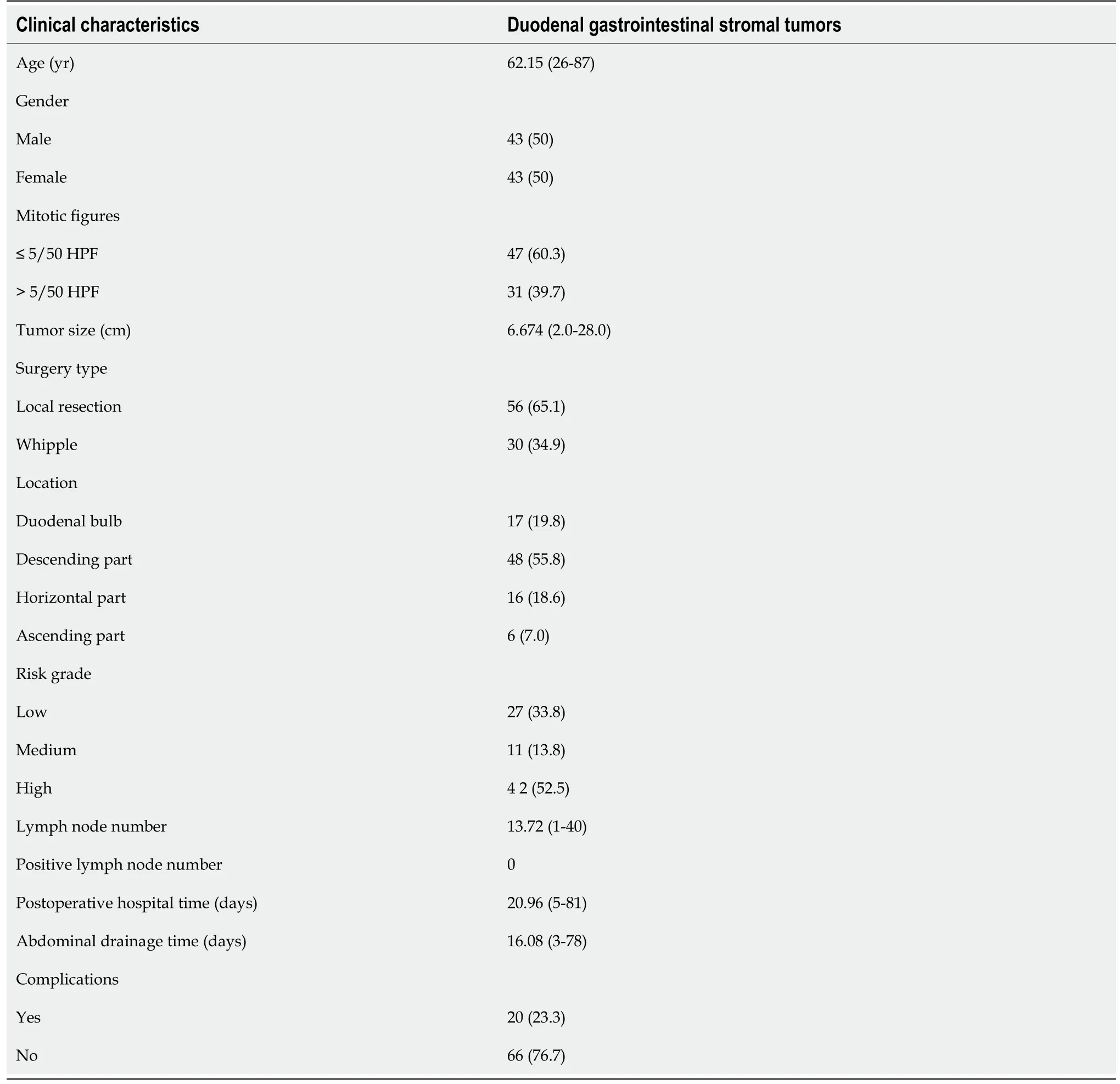
Table 1 Clinical characteristics of 86 patients with duodenal gastrointestinal stromal tumors,n (%)
Although the biological characteristics of DGISTs include low-grade malignancy,some patients still develop synchronous liver metastases.We describe the treatment of two patients with synchronous liver metastases(Table 8).Patient 1 was diagnosed with duodenal stromal tumor with liver metastasis.Due to the large metastatic liver tumor,he first received liver resection and gastro-jejunal circuit to relieve symptoms followed by imatinib for 2 years after surgery.Tumor shrinkage was observed in the patient and he then underwent the Whipple procedure for radical treatment of the tumor.Patient 2 was diagnosed with duodenal stromal tumor with multiple liver metastases which were located in the left liver.Considering that the surgical risk in this patient was high,he received imatinib for 16 mo.The primary DGIST and all the liver tumors reduced in size and he then underwent the Whipple procedure and left liver resection followed by imatinib treatment after surgery.
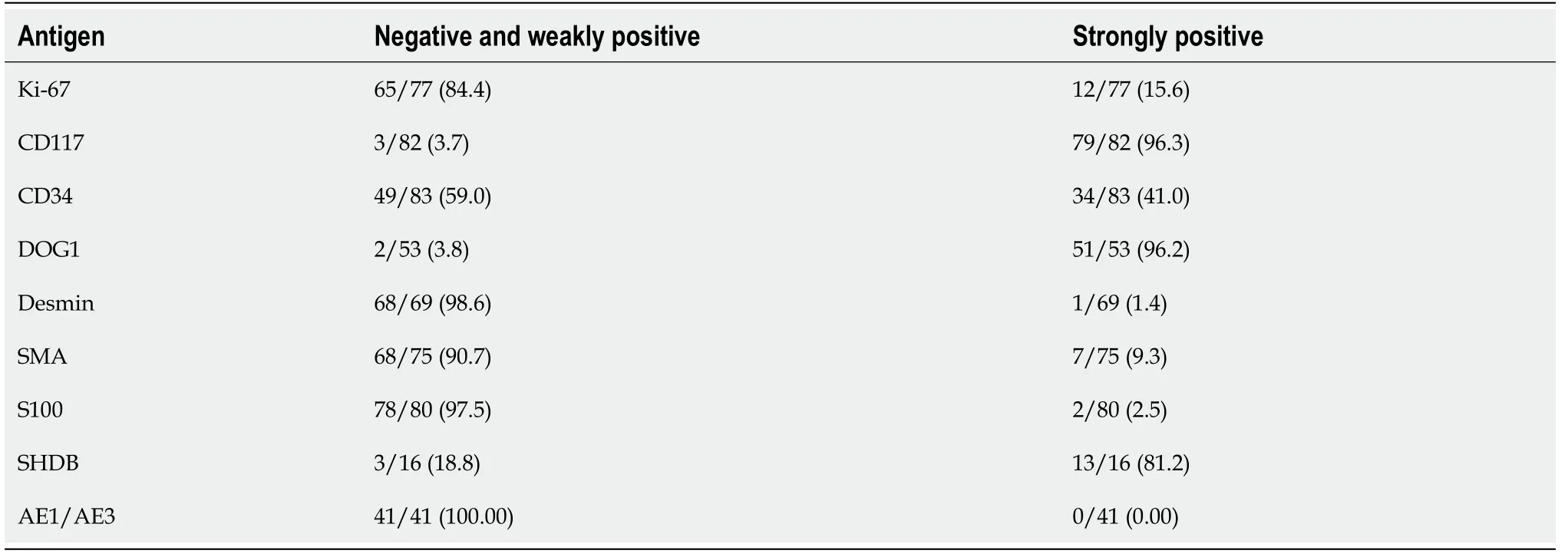
Table 2 Immunohistochemical findings in duodenal gastrointestinal stromal tumors,n(%)
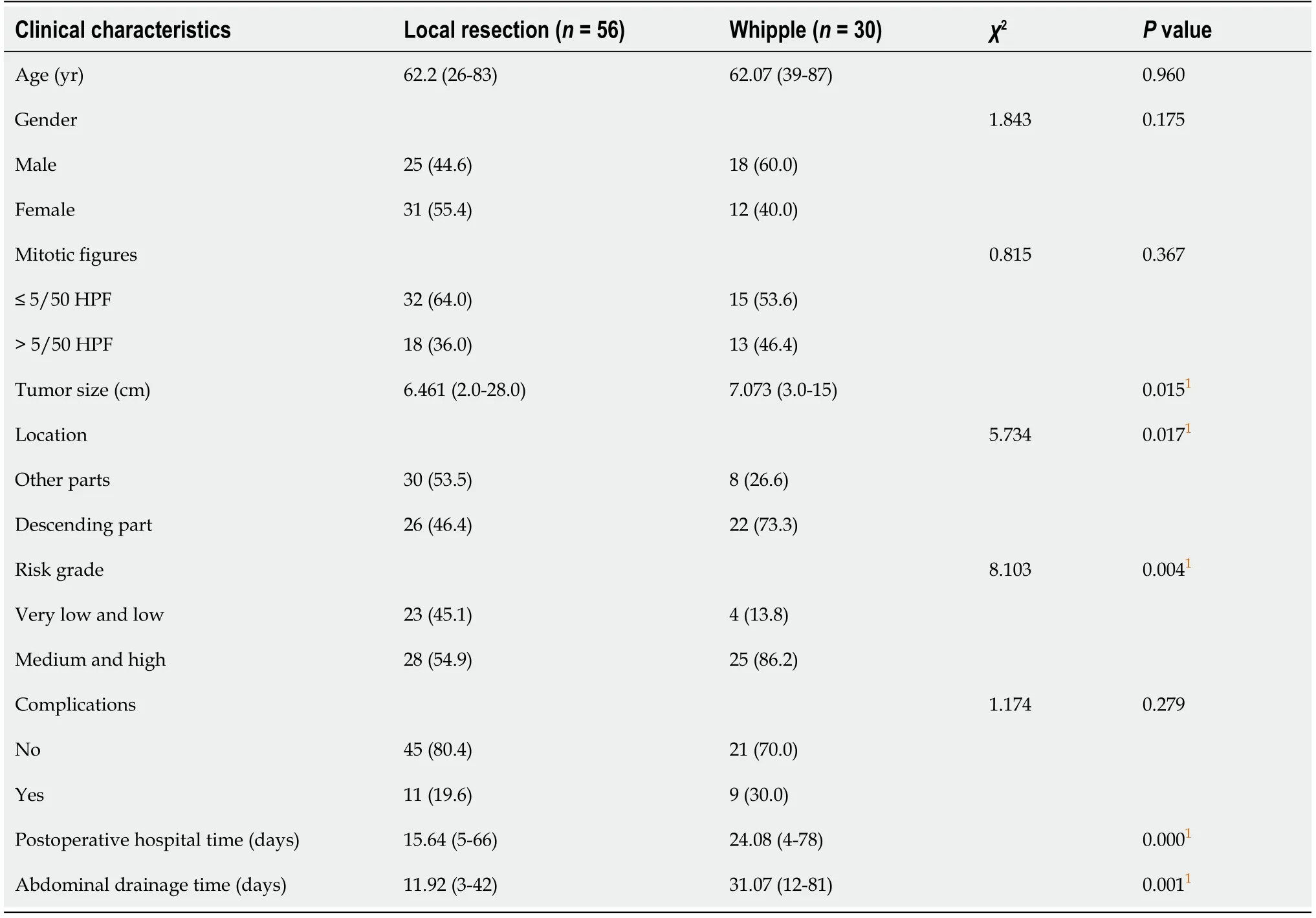
Table 3 Clinical characteristics of 86 patients with duodenal gastrointestinal stromal tumors treated with different surgical procedures,n(%)
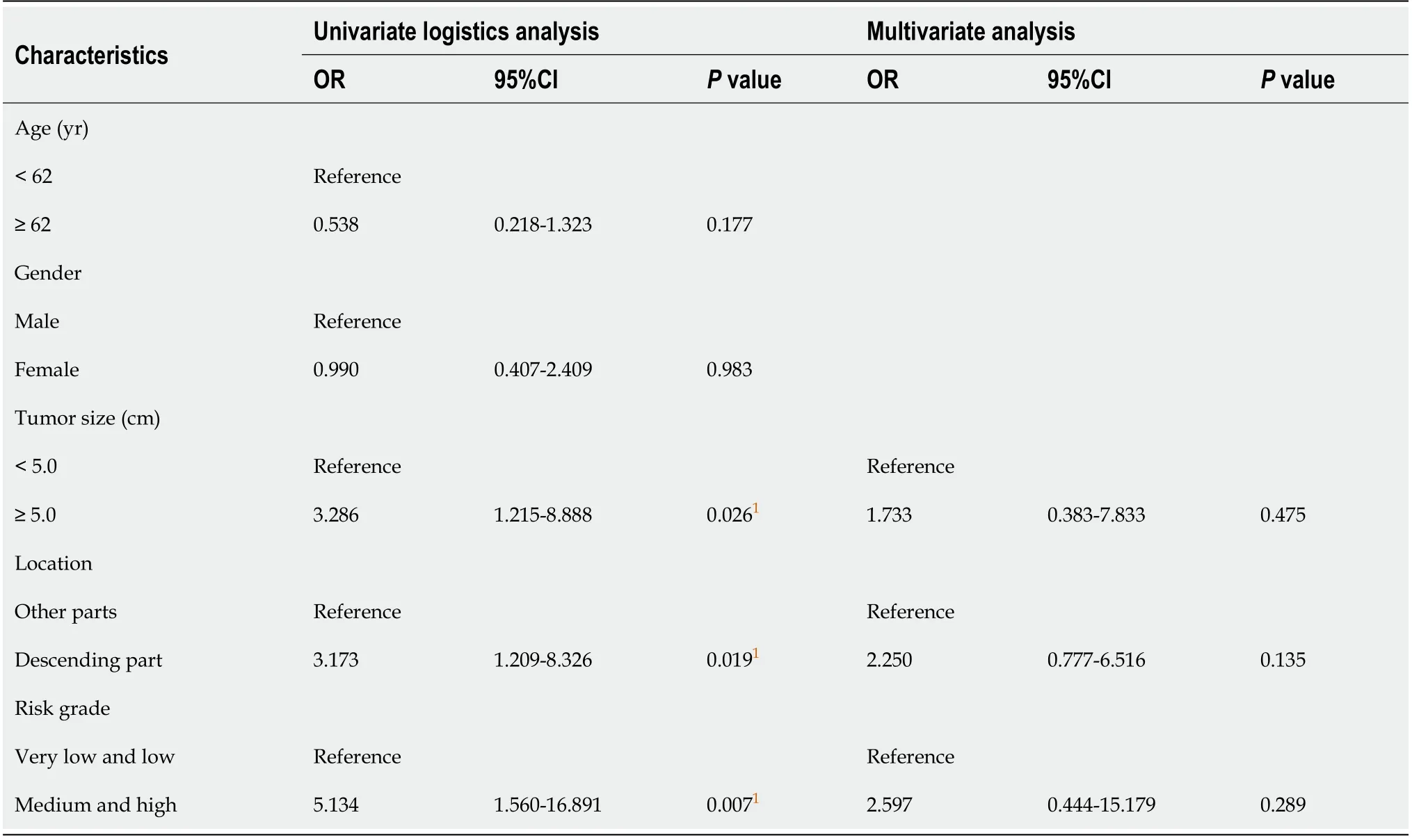
Table 4 Univariate and multivariate logistic analyses of different surgical procedures
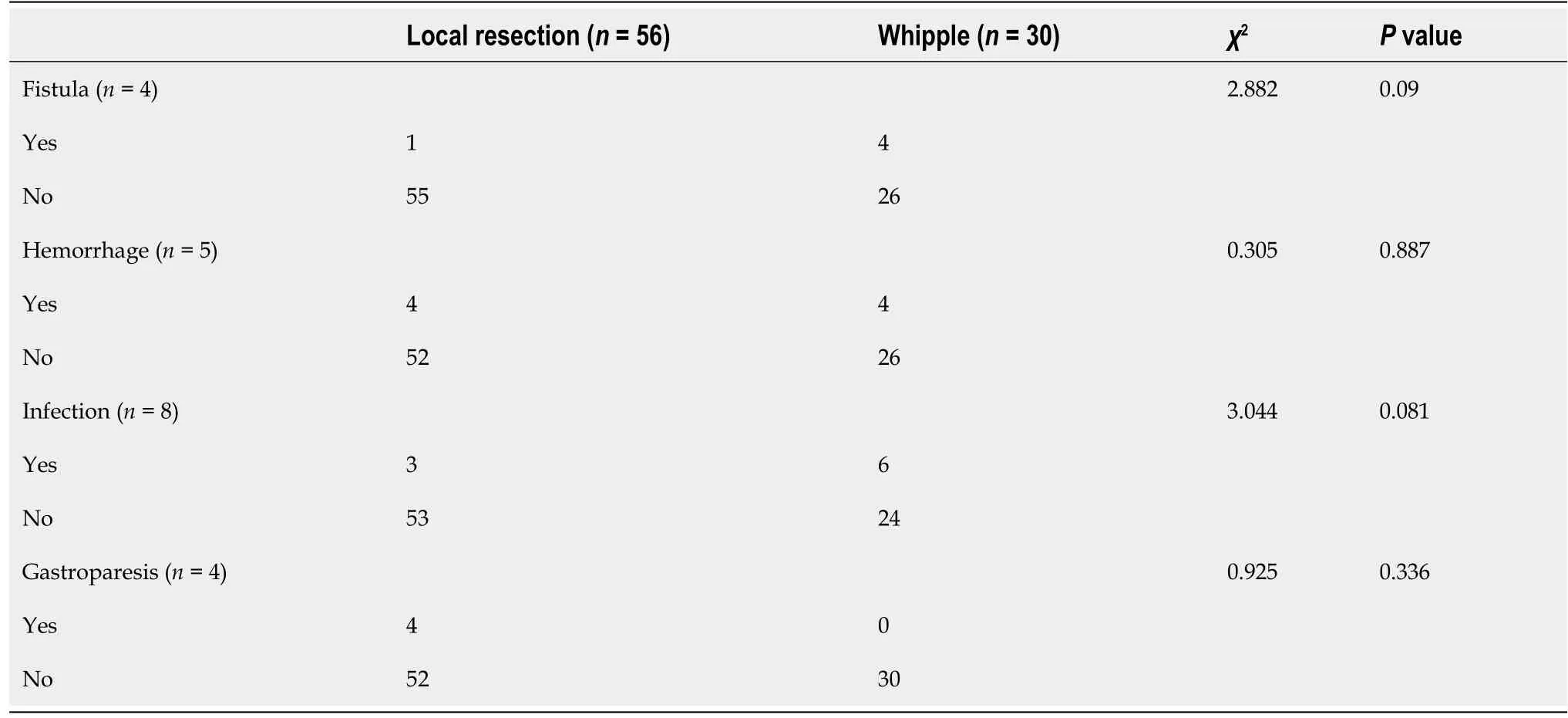
Table 5 Postoperative complications in patients who underwent different types of surgery
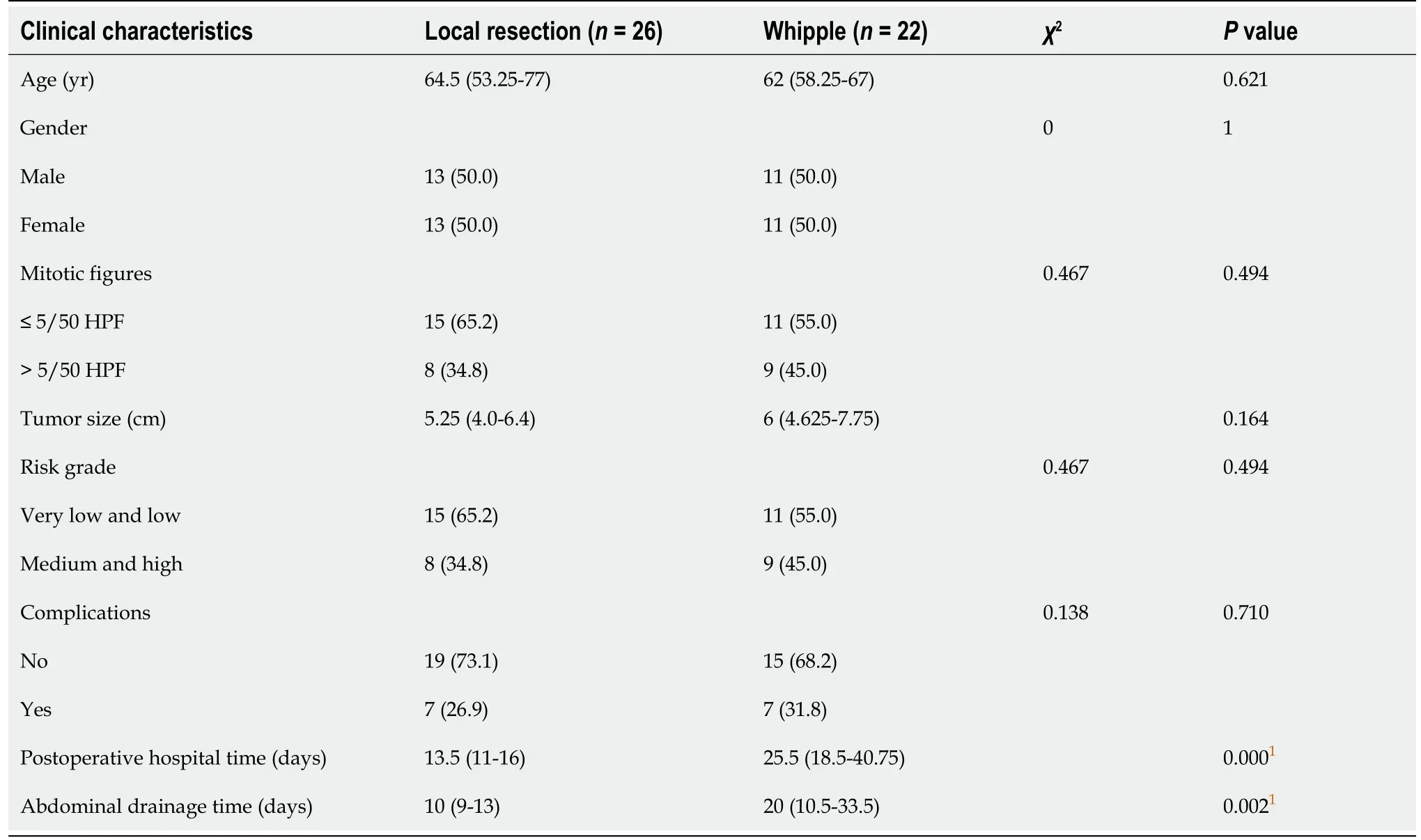
Table 6 Clinical characteristics of 48 patients with duodenal gastrointestinal stromal tumors in the descending section treated with different types of surgery,n(%)
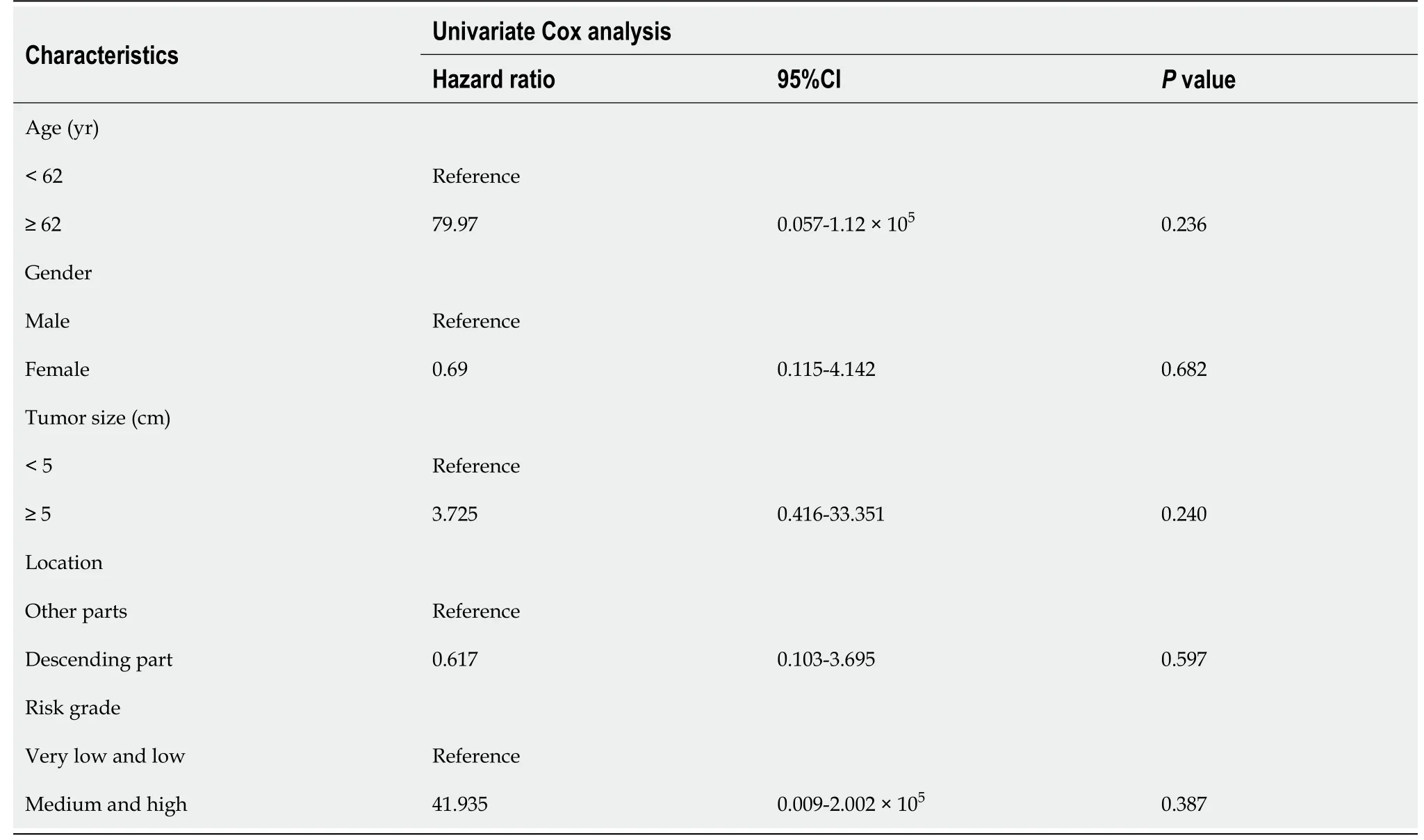
Table 7 Cox regression analysis of duodenal gastrointestinal stromal tumor patients

Table 8 Clinical characteristics of patients with synchronous liver metastases
DISCUSSION
In this study,we retrospectively analyzed 86 patients with DGISTs treated between 1999 and 2021.We also described two patients with DGISTs and synchronous liver metastases.Previous studies have demonstrated that local resection has obviousadvantages over pancreaticoduodenectomy in terms of surgical trauma,surgical complications,and postoperative recovery;however,there was no difference in the long-term oncological efficacy between the two surgical methods in the treatment of DGISTs[8-10].Additionally,postoperative adjuvant treatment can result in a better prognosis[11-13].In recent years,several clinical studies and meta-analyses have suggested that surgical resection of GISTs should adhere to the principle of local resection[14,15].
Based on the results of this study,the clinicopathological parameters of our patients were similar to the basic characteristics of DGISTs in China[16,17].There were no differences in the incidence rate between different genders with a median age of 62.15years(range,26-87 years).The tumors ranged from 2 cm to 28 cm in size and were distributed in different parts of the duodenum with the predominant location being the descending section(55.8%).Fifty-six(65.1%)patients underwent local resection,and 30 patients(34.9%)underwent the Whipple procedure.Almost 90% of patients lived longer than five years.Furthermore,by comparing the difference between the two groups of patients,we suggest performing the Whipple procedure if the primary tumor is in the descending part of the duodenum,tumor size is ≥ 5.0 cm,or the tumor risk grade is medium or high.We believe that the use of extended radical surgery(Whipple procedure)in patients with DGISTs will not improve their prognosis;rather,it will increase surgical trauma and postoperative complications,and reduce the quality of life of patients postoperatively.
GISTs have unique biological characteristics,and they rarely result in lymph node metastasis;therefore,surgical resection of GISTs does not require excessive tumor margins and resection of lymph nodes.Surgical resection of DGIST does not need to involve the scope of surgical resection for duodenal cancer or require pancre-aticoduodenectomy and peripheral lymph node dissection.Some patients diagnosed with synchronous liver metastases underwent surgery followed by the administration of imatinib.
Due to the long operation time related to Whipple surgery,extensive trauma,and high surgical risk,Whipple surgery will inevitably increase the number of postoperative complications,even if it is performed by a skilled surgeon.Postoperative pain,prolonged postoperative treatment,and delayed postoperative adjuvant treatment reduce the quality of life of patients and affect their prognosis.
Even if the tumor is located in the descending part of the duodenum,Whipple surgery seems to be appropriate.However,in most instances,to promote speedy recovery,local resection should be the first choice with administration of postoperative adjuvant treatment as soon as possible[18,19].However,the premise is the definitive diagnosis of DGISTs.Percutaneous or endoscopic ultrasonography-guided fine-needle aspiration can be used before surgery[20-22].When histopathological diagnosis is confirmed,preoperative GIST treatment can be administered in order to increase surgical safety.When the tumor has reduced in size[23],local resection of the intestine can eliminate the tumor with less trauma.
Due to the low incidence rate of DGISTs,the number of cases available for analysis is limited.Multicenter analysis and high standard meta-analysis are necessary.As reported in previous research[24,25],based on our results,primary tumor size,primary tumor location and the risk grade can affect the surgical procedure.The critical point of tumor size should be further identified using a more effective statistical model[26].In addition,primary tumor location should be further subdivided as well as different types of tumor growth(such as exophytic tumor).If the tumor is located in the descending part of the duodenum,the relationship between the primary tumor and duodenal papilla,pancreas as well as the bile duct should be assessed.In this retrospective study,tumor pathological reports were different during different times.It is also necessary to re-analyze pathological specimens using unitary standards.Furthermore,DGISTs patients have a good prognosis.This means that we should have a standardized follow-up for our patients using the guidelines[27].Finally,imatinib administration is important in patient management[28-30].In our retrospective study,some patients were lost to follow-up;therefore,we could not correctly estimate postoperative adjuvant treatment.
There are some limitations in this study.First,the sample size was relatively small,and may influence the clinical application value.Second,this was a retrospective study,and a prospective study should be performed in the future.
CONCLUSION
If the primary tumor is in the descending part of the duodenum,tumor size is ≥ 5.0 cm,and tumor risk grade is medium or high,Whipple surgery should be performed.
ARTICLE HIGHLIGHTS
Research background
Duodenal gastrointestinal stromal tumors(DGISTs)rarely break the tumor capsule and lymph node metastases seldom occur.However,the duodenum is located near the pancreas and biliary tract.Traditional Whipple surgery results in severe injury;thus,it is necessary to preserve as much normal tissue as possible.
Research motivation
The present study attempted to identify the factors influencing the surgical treatment of DGISTs and to determine the best surgical procedure.
Research objectives
This study aimed to investigate the factors influencing DGIST surgery and provide advice regarding the best surgical technique.
Research methods
The clinicopathological data of patients with DGISTs who underwent surgery from January 1999 to January 2021 were analyzed.The Student t test or Mann-WhitneyUtest andχ2test or Fisher’s exact test were used to identify differences between the two groups of patients treated with different surgical techniques.Logistic regression analysis was carried out to assess the relevant factors influencing the choice of surgical procedure.
Research results
There were no differences in age,mitotic figures and complications between these two groups,while the tumor size,tumor location,risk grade,postoperative hospital time,and abdominal drainage time showed statistically significant differences.Using univariate logistic analysis,if the tumor was ≥ 5.0 cm in size,located in the descending part of the duodenum or the risk grade was medium or high,Whipple surgery was performed.
Research conclusions
If the primary tumor was in the descending part of the duodenum,was ≥ 5.0 cm in size and the risk grade was medium or high,Whipple surgery was performed.
Research perspectives
Although we investigated the factors influencing the surgical treatment of duodenal gastrointestinal stromal tumors and assessed the best surgical procedure for these patients,a prospective study should be performed to confirm these findings.
 World Journal of Gastrointestinal Oncology2021年8期
World Journal of Gastrointestinal Oncology2021年8期
- World Journal of Gastrointestinal Oncology的其它文章
- Diagnostic value of four serum exosome microRNAs panel for the detection of colorectal cancer
- Development of a prognostic prediction model based on microRNA-1269a in esophageal cancer
- Diffuse reduction of spleen density is a novel prognostic marker for intrahepatic cholangiocarcinoma after curative resection
- Neutrophil-to-lymphocyte ratio and carbohydrate antigen 19-9 as prognostic markers for advanced pancreatic cancer patients receiving first-line chemotherapy
- STAT3-mediated activation of mitochondrial pathway contributes to antitumor effect of dihydrotanshinone I in esophageal squamous cell carcinoma cells
- Plasma MMP-2 and MMP-7 levels are elevated first month after surgery and may promote growth of residual metastases