
Role of ranulas in early diagnosis of Sjögren’s syndrome: A case report
2021-08-04 05:25NaChenDaShunZengYuTongSu
World Journal of Clinical Cases 2021年20期
Na Chen, Da-Shun Zeng, Yu-Tong Su
Na Chen, Department of Endocrine and Metabolic Diseases, Shanghai Institute of Endocrine and Metabolic Diseases, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine,Shanghai, China
Na Chen, Shanghai National Clinical Research Center for metabolic Diseases, Key Laboratory for Endocrine and Metabolic Diseases of the National Health Commission of the PR China,Shanghai National Center for Translational Medicine, Shanghai, China
Da-Shun Zeng, Department of Oral Surgery, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou 325200, Zhejiang Province, China
Yu-Tong Su, Department of Rheumatology and Immunology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China
Abstract BACKGROUND Although the presentations of Sjögren’s syndrome (SS) are variable, ranging from mild dryness to wider systemic involvement, ranulas as early clinical signs were scarcely reported. Here, we present an adult patient with SS, who developed a unilateral simple ranula and was diagnosed primary SS 3 years later. We also provide a review of cases of SS and ranulas from 1980 to 2020.CASE SUMMARY A 22-year-old girl was found to have a left painless floor-of-mouth lesion 3 years ago, without obvious trauma or inducement. The diagnosis of a unilateral (left)simple ranula was made, and the ranula was surgically treated. Within 3 years after the ranula surgery, she developed acute lymphadenectasis in unilateral parotid twice without inducement, and ultrasonic examination revealed diffuse lesions in bilateral parotids and submandibular glands, which strongly suggested SS. Serologic tests and the unstimulated whole saliva flow rate confirmed the SS diagnosis.CONCLUSION Our study underlines that ranulas are early clinical signs of SS. As early diagnosis and early intervention of SS are important to obtain better outcomes, our findings underline the need for histopathological test after sublingual adenectomy and imaging detection of exocrine glands for the patients with ranulas.
Key Words: Sjögren’s syndrome; Ranulas; Early diagnosis; Parotitis; Case report
INTRODUCTION
Sjögren’s syndrome (SS) is a chronic systemic autoimmune disorder, characterized by lymphocytic infiltration of exocrine glands with a greater predilection in females[1].The reported prevalence ranges from 0.01% to 0.09% in the general population[2]. The symptoms are various and can involve the whole body, beyond sicca syndromes, and systemic manifestations include inflammatory arthritis, renal involvement, lung lesion,central nervous system involvement,etc.[3,4]. Due to insidious onset in early stage, it is difficult to diagnose SS at an early stage in time and accurately.
Ranulas are caused by extravasation of mucus from damage or obstruction of the sublingual gland or its duct[5]. Eating and external blunt trauma could cause damage to the sublingual duct[6], meanwhile, anatomical variations and chronic disease of the sublingual glands could lead to the obstruction[7]. Concomitant ranulas are uncommon in patients with SS. It is reported that ranulas developed as a complication of SS in children[8-10], and limited cases are found in adults[10-13]. However, the association between ranulas and SS remains unknown.
In the present review, we report a 22-year-old girl with a unilateral ranula who was diagnosed as having SS 3 years later. The clinical presentation, laboratory tests, and treatment are described. According to this case and literature review, we aim to draw the attention of early clinical signs "ranulas" for SS, which are easily neglected or inappropriately treated although they are the hints to early diagnosis of SS.
CASE PRESENTATION
Chief complaints
On March 1, 2019, a 22-year-old girl came to our outpatient clinic asking for serologic testing for SS.
History of present illness
The patient denied having dry eyes, dry mouth, parotid enlargement, or other clinical manifestations.
History of past illness
The patient was referred to oral surgery department for evaluation of a left painless floor-of-mouth lesion 3 years ago. The lesion had been present for 1 mo and the patient showed no difficulty eating, drinking, or speaking. Before ranula presentation, there was no obvious trauma or inducement. A pink, fluctuant, dome-shaped bulge in the floor of the mouth on the left side of the patient's lingual frenulum was found in an oral examination(Figure 1).Palpation revealed that the bulge was confined to the soft tissue. Based on these manifestations, the diagnosis of a unilateral (left) simple ranula was made. Her oral surgeon at the time did not consider anything more than a ranula,and did not perform any further tests. The patient underwent a surgery to remove the entire unilateral sublingual gland with the ranula while the lingual nerve was preserved. The pathology showed a sublingual gland (left) with chronic inflammation,lymphocytic infiltration, and focal mucus extravasation (Figure 2). There was no ranula on her right sublingual gland so far.

Figure 1 Clinical picture of the unilateral (left) simple ranula.
In 2017, 10 mo after the ranula surgery, the patient developed acute left submaxillary parotid lymphadenectasis without inducement. Ultrasonic (US) examination revealed patchy hypoechoic areas in the left parotid. Two years after the first parotid lymphadenectasis, she developed acute right parotid gland swelling without inducement as before. US examination revealed scattered, foveolate hypoechoic areas,and lymphadenectasis in bilateral parotids. Treatment with antibiotic and glucocorticoid were given. 1 mo later, US reexamination still revealed diffuse lesion in bilateral parotids and submandibular glands, which strongly suggested SS.
Personal and family history
There was no family history of autoimmune disorders.
Physical examination
No abnormality was found on physical examination.
Laboratory examinations
Serologic tests showed an antinuclear antibody (ANA) titer of 1:320, with antibody positivity for the extractable nuclear SS-related antigen A (SSA) as well as an elevated erythrocyte sedimentation rate of 33 mm/h (reference range 0-20 mm/h for females),rheumatoid factor (RF) of 441 IU/mL (reference range 0-20 IU/mL), and IgG of 20.10 g/L (reference range 8.6-17.4 g/L). The unstimulated whole saliva flow rate was 1.7 mL/min (reference range > 2 mL/min). Ophthalmologically, the Schirmer test results were 30 mm on both eyes in 5 min (reference range > 10 mm). The patient’s characteristics and laboratory data are shown in Table 1.
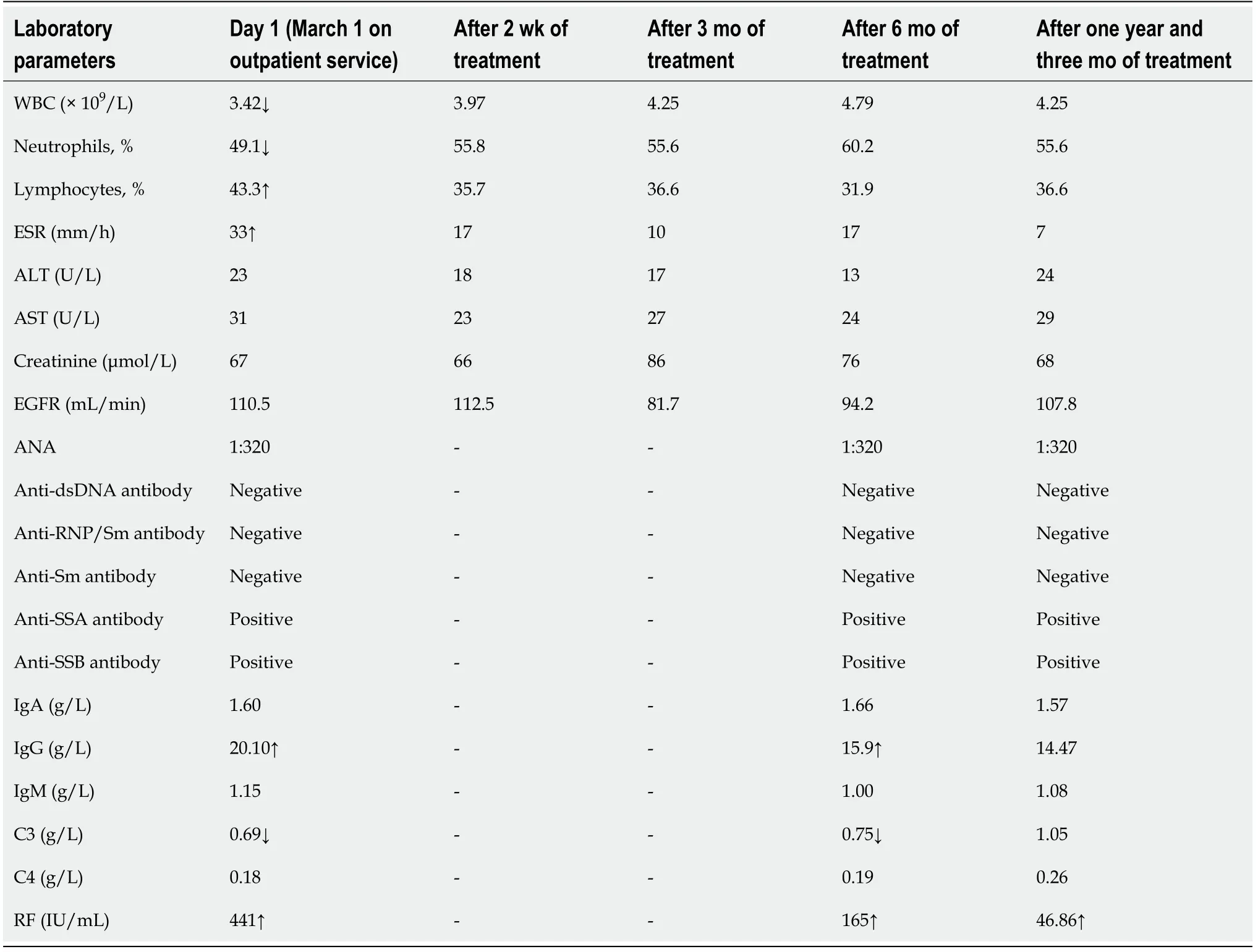
Table 1 Laboratory parameters of the patient with primary Sjögren’s syndrome who had a ranula before
FINAL DIAGNOSIS
Along with the characteristic lesions in salivary glands, a diagnosis of primary SS was made.
TREATMENT
Treatment with hydroxychloroquine sulfate tables (400 mg/d) and total glycosides of paeony root capsule (1200 mg/d) was started.
OUTCOME AND FOLLOW-UP
The parotitis did not relapse during the 2-year follow-up.
DISCUSSION
Search strategy
A review of the literature for ranulas with SS was carried out based on the following databases: Web of Science, Scopus Database, and PubMed/MEDLINE up to December 2020. The search was performed with the following MESH terms: “Sjögren’s syndrome” and “ranulas” or “floor-of-mouth mucocele”. The studies reported on children or adults diagnosed with SS with ranulas in the past 40 years (from 1980 to 2020) were included.
Literature review
Four series[9-12] and two isolated cases of pSS with ranulas[8,13] have been published,which contain a total of 17 patients including our case (Table 2). Among the 17 patients described, 15 were women and two were men. The turnout is consistent with previousreports that pSS is a women dominant disease[13]. Ranulas were detected before pSS diagnosis in nine patients, and ranulas were detected simultaneously with pSS diagnosis in six patients[14]. Only three patients were detected with ranulas after pSS was diagnosed[15]. This statistic suggests that ranulas may be the early clinical signs rather than the manifestations in the late period of pSS, according to the studies by Satoet al[11] and Takagiet al[10]. The time interval from discovery of ranulas to the diagnosis of pSS is 0 to 7 years, which indicates that pSS occurs insidiously. In addition to presenting with unilateral or bilateral ranulas, six (6/17) patients were reported to have sicca symptoms including recurrent parotitis, dry eyes, dry mouth, and dental caries[8,9,12,13], and only one (1/17) patient was reported to have extra-glandular system involvement (joint pain)[9]. Six surgical pathological specimens showed the lymphocytic infiltration. Anti-ANA and anti-SSA were detected in all patients. With regard to the treatment of ranulas, ten (10/17) patients were surgically treated, one(1/17) naturally resolved, and six (6/17) were uncertain. The detailed treatment of pSS was not described in most patients. It may be because that the cases were reported by oral surgeons or otolaryngologists.

Table 2 Review of primary Sjögren’s syndrome patients associated with ranulas
SS is a complex and multisystem disorder. The SS patients with both glandular and extra-glandular features suffer from a poor prognosis. The advanced stage symptoms of tooth loss, severe fatigue, and joint and muscle pain impair the quality of life.Moreover, the development of lymphomas increases the mortality[16]. In clinical practice, dryness such as dry eyes and dry mouth often indicates that glandular secretion has been disrupted by chronic soakage of inflammatory cells, which may be too late for treatment and would impair the effect of intervention.
There are several diagnostic criteria for SS in the past two decades, including the 1999 revised Japanese Ministry of Health Criteria for diagnosis of SS (JPN), 2002 American-European Consensus Group Classification Criteria for SS, 2012 ACR Classification Criteria for SS, and 2016 ACR-European League Against Rheumatism Classification Criteria[17]. However, these criteria are mainly to confirm the diagnosis of SS when symptoms have progressed to a certain level, but not to identify the early symptoms. Several valuable biomarkers have been recently identified for early auxiliary diagnosis/stratification of SS[18]. For example, tissue specific autoantibodies,such as parotid secretory protein, salivary protein-1, carbonic anhydrase 6, can be detected before the classic autoantibodies[15,19]. However, in the absence of the typical clinical symptoms of SS (such as dry eyes, dry mouth, or recurrent parotitis),these tests are not routinely performed. Besides, the diversity of symptoms also makes early diagnosis and intervention of SS difficult. Therefore, it is vital to detect early clinical signs in order to treat SS properly in its early stage and to achieve better clinical outcomes.
Ranulas were detected before or at the same time of SS diagnosis in 82.35% (14/17)of patients, which is much higher than the incidence of ranulas after SS diagnosis as a complication (3/17). Ranulas are rare diseases, which have a predominance among teenagers and young adults, and the incidence is 2 per 1000[20]. Recently, Takagiet al[10] examined 50 patients with ranulas undergoing magnetic resonance imaging(MRI). Eleven patients were suspected to have SS, and seven of them were then confirmed by the rheumatologist according to the Japanese Ministry of Health criteria(1999)[10]. It is worth noting that the incidence of SS patients was significantly increased among patients with ranulas. The combination of these patients and ours suggests that ranulas may be the early clinical signs of SS.
SS is characterized by lymphocytic infiltration of exocrine glands including the sublingual gland. Among patients with SS in early stage, ranulas usually appear without obvious trauma or cause. Satoet al[11] hypothesized that ranulas could be caused by the constriction of ducts in the early stage of SS, especially when the obstruction is close to the opening. Considering that acinar atrophy and loss occur in the advanced stage, ranulas are rarely due to the decrease of saliva levels[21]. Indeed,only three patients had a ranula after SS diagnosis in our review.
Recurrent parotitis is a common symptom of SS, which is caused by an ascending ductal infection and the assistant of decreased salivary duct lavage[22], whereas ranulas usually happen when saliva production is unaffected. This suggests that ranulas occur earlier than parotitis. In our case, the first manifestation of parotitis developed 10 mo after the unilateral ranula. Besides, the patient reported by Takagiet al[10] developed parotitis 9 mo after SS diagnosis, and the patient reported by Liebermanet al[9] had no parotitis or parotid gland swelling throughout. Oral lesions are characteristics of Sjögren syndrome in childhood. No parotid mucocele or submandibular gland mucocele has been reported in SS. We hypothesized that this might be the structure of the glands themselves. The duct of the parotid or submandibular gland is covered with thicker glandular tissue and muscle; however,the sublingual gland is exposed at the base of the mouth.
The ranulas are routinely treated by marsupialization or sublingual gland surgical removal[14]. Patients with new-onset ranulas usually visited stomatology or otolaryngology department, and the doctors would not routinely perform serological examinations or detailed glandular tests, unless patients show other symptoms of autoimmune diseases. Therefore, SS was easily neglected even with the discovery of ranulas. In the five patients diagnosed with ranulas and SS simultaneously, the results of MRI examinations in four patients revealed chronic sialadenitis[8,11], and the surgical pathological specimen of one patient showed lymphocytic infiltration, which prompted the imaging detection of exocrine glands and serological examinations of SS in patients who had not yet developed symptoms such as dry mouth, dry eyes, or parotitis. Thus, we recommend ranula patients to undergo postoperative pathological examination and imaging detection, which can be helpful for early detection of SS.Besides, US is a convenient and inexpensive procedure and should be considered a suitable tool for diagnosing juvenile SS[10].
CONCLUSION
In the present review, we summarize all published papers on SS and ranulas. We hope that these cases will raise the awareness of clinicians that ranulas are early clinical signs of SS. As early diagnosis and early intervention of SS are important to obtain better outcomes, we recommend histopathological test after sublingual adenectomy and imaging detection of exocrine gland for the patients with ranulas.
ACKNOWLEDGEMENTS
We thank the Innovative Research Team of High-level Local Universities in Shanghai.
 World Journal of Clinical Cases2021年20期
World Journal of Clinical Cases2021年20期
- World Journal of Clinical Cases的其它文章
- Obesity in people with diabetes in COVID-19 times: Important considerations and precautions to be taken
- Revisiting delayed appendectomy in patients with acute appendicitis
- Detection of short stature homeobox 2 and RAS-associated domain family 1 subtype A DNA methylation in interventional pulmonology
- Borderline resectable pancreatic cancer and vascular resections in the era of neoadjuvant therapy
- Esophageal manifestation in patients with scleroderma
- Exploration of transmission chain and prevention of the recurrence of coronavirus disease 2019 in Heilongjiang Province due to inhospital transmission