
Rapid diagnosis of disseminated Mycobacterium mucogenicum infection in formalin-fixed, paraffin-embedded specimen using nextgeneration sequencing: A case report
2021-08-04 05:25JingLiuZiYingLeiYiHuaPangYingXiongHuangLeJiaXuJianYunZhuJiaXingZhengXiaoHuaYangBingLiangLinZhiLiangGaoChaoZhuo
World Journal of Clinical Cases 2021年20期
Jing Liu, Zi-Ying Lei, Yi-Hua Pang, Ying-Xiong Huang, Le-Jia Xu, Jian-Yun Zhu, Jia-Xing Zheng, Xiao-Hua Yang, Bing-Liang Lin, Zhi-Liang Gao, Chao Zhuo
Jing Liu, Zi-Ying Lei, Yi-Hua Pang, Le-Jia Xu, Jian-Yun Zhu, Jia-Xing Zheng, Xiao-Hua Yang, Bing-Liang Lin, Zhi-Liang Gao, Department of Infectious Diseases, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou 510630, Guangdong Province, China
Ying-Xiong Huang, Department of Emergency, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou 510000, Guangdong Province, China
Le-Jia Xu, Department of Pharmacy, The Third Affiliated Hospital of Sun Yat-Sen University,Guangzhou 510630, Guangdong Province, China
Chao Zhuo, State Key Laboratory of Respiratory Disease, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou 510120, Guangdong Province, China
Abstract BACKGROUND Mycobacterium mucogenicum (M. mucogenicum) belongs to the group of rapidly growing Nontuberculous mycobacteria. This microorganism is associated with a wide spectrum of infectious diseases. Due to a low detection rate or the time required for conventional culture methodology, a rapid and broad-spectrum method is necessary to identify rare pathogens.CASE SUMMARY A 12-year-old immunocompetent girl presented with painful masses for five months. The first mass was found in the right upper quadrant of the abdomen,and was about 1 cm × 1.5 cm in size, tough but pliable in texture, with an irregular margin and tenderness. An abscess gradually formed and ulcerated with suppuration of the mass. Three new masses appeared on the back one by one.Chest computed tomography showed patchy and streaky cloudy opacities in both lungs. Needle aspiration of the abscess was performed, but the smear and conventional culture were negative, and the pathological examination showed no pathogens. We then performed next-generation sequencing using a formalinfixed, paraffin-embedded specimen to identify the pathogen. A significantly high abundance of M. mucogenicum was detected. The patient’s abscesses gradually decreased in size, while inflammation in both lungs improved following 12-wk of treatment. No recurrence was observed four months after the end of the one-year treatment period.CONCLUSION Next-generation sequencing is a promising tool for the rapid and accurate diagnosis of rare pathogens, even when using a formalin-fixed, paraffin-embedded specimen.
Key Words: Mycobacterium mucogenicum; Next-generation sequencing; Disseminated infection; Formalin-fixed, paraffin-embedded specimen; Rapid diagnosis; Case report
INTRODUCTION
Nontuberculous mycobacteria (NTM) were initially recognized as pathogens in the mid 1950’s[1]. More and more species were discovered due to recognition by medical workers and improvements in examination techniques. Some species may cause diseases in humans[1]. NTM has been reported to include more than 170 species worldwide, including two types: rapidly growing mycobacteria (RGM) and slow growing mycobacteria[2].Mycobacterium mucogenicum(M. mucogenicum) belongs to the group of RGM, and is considered an environmental organism with a worldwide distribution. It is associated with a wide spectrum of clinical diseases, including osteomyelitis, respiratory tract, bloodstream, and disseminated infections in both immunocompetent and immunosuppressed individuals[3]. However, the time required and low detection rate to identify this pathogen usually leads to delayed or missed diagnosis.Thus, a rapid and broad-spectrum method is necessary to identify rare pathogens.Next-generation sequencing (NGS) is an unbiased approach whose RefSeq contains 4152 whole genome sequences of viral taxa, 3446 bacterial genomes or scaffolds, 206 fungi related to human infection, and 140 parasites associated with human diseases. It identifies the nucleotides in the target samples and compares the detected nucleotides against the catalogue library of pathogens, thereby listing the possible causative agents in the clinical samples[4].The specimens examined are usually fresh ones, such as blood, pus, bronchoalveolar lavage fluid, cerebrospinal fluid, lymph nodes, tissue, and so on[5-7]. However, there are few reports on formalin-fixed, paraffin-embedded(FFPE) specimens, and it is unclear whether the clinical significance of the detection results using FFPE is useful.
Here, we report a case with disseminated infection ofM. mucogenicumdetected by NGS using a FFPE specimen.
CASE PRESENTATION
Chief complaints
A 12-year-old Han Chinese girl (30 kg), who was a middle school student, presented to our hospital with several masses on the abdomen and back with low-grade fever for five months.
History of present illness
Five months previously, a painful tender mass was found in the right upper quadrant of the girl’s abdomen. The patient reported low-grade fever with a temperature of 37.5℃ and fatigue. Chinese herbal medicines for external application were used for the mass; however, the mass enlarged and an abscess gradually formed, and then ulcerated with suppuration. Subsequently, three other masses appeared, one by one,with one on the left back and two on the right back, which were similar to the first mass (Figure 1). She also had a mild cough without sputum. There was no night sweating, diarrhea, or nausea.

Figure 1 These images show the successive changes (from A to D) of the skin lesion on the lower right back over several months up to September 30, 2018.
History of past illness
The patient did not recall any previous back or abdominal injury.
Personal and family history
The patient and her family had no previous medical history.
Physical examination
The patient’s temperature was 37.5℃, heart rate was 105 bpm, respiratory rate was 20 breaths/min, blood pressure was 105/62 mmHg and oxygen saturation in room air was 99%. Four painful subcutaneous masses were palpable, one on the right upper abdomen, one on the left back, and two on the right back. The masses ranged from 3.0 to 4.0 cm in diameter, were tough but pliable in texture, with tenderness, an irregular margin and discharging pus. Moist rales were found at the bottom of both lungs.
Laboratory examinations
Complete blood cell counts showed that the white blood cell count (WBC) was 25.24 ×109/L with 40% neutrophils, 8.20% lymphocytes, red blood cell count (RBC) was 2.48 ×1012/L, and hemoglobin (HGB) was 54 G/L. The erythrocyte sedimentation rate (ESR)was > 140 mm/h and procalcitonin (PCT) was 2.39 ng/mL.
Imaging examinations
Whole abdomen computed tomography (CT) on September 13thshowed obvious swelling of both bilateral psoas, iliopsoas and back muscles, suggesting infection and multiple abscesses, peritonitis and a moderate amount of ascites. The chest CT on September 21stshowed massive pleural effusion in the left chest, a small amount of pleural effusion on the right, patchy and streaky cloudy opacities in both lungs,suggesting inflammation (Figure 2). Color Doppler echocardiography on September 28thshowed a markedly enlarged right atrium and left atrium, aortic insufficiency,tricuspid insufficiency, pulmonary hypertension, mild to moderate pericardial effusion, left ventricular contractile and diastolic dysfunction.
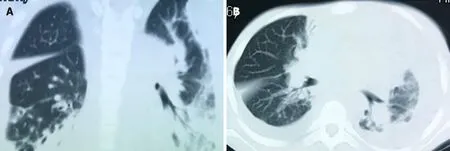
Figure 2 The chest computed tomography on September 21, 2018 shows a massive pleural effusion on the left, a small pleural effusion on the right, patchy and streaky cloudy opacities on both lungs, suggesting inflammation. A: The sagittal plane; B: The horizontal plane.
Further diagnostic work-up
As the patient had signs of heart failure and multiple abscesses, she was transferred to the intensive care unit of the local hospital. A series of assays were performed as follows: C-reactive protein (CRP) 74.2 mg/L, serum amyloid A (SAA) 421 mg/L, PCT 1.69 ng/mL, creatine kinase isoenzyme MB (CKMB) 0.97 ng/mL, and N-terminal prohormone of brain natriuretic peptide (NT-proBNP): 18136 pg/mL. Her hepatic and renal function were normal. HIV screen was negative, and CD4and CD8counts were normal. Tuberculosis-antibody and T-SPOT were negative. All autoantibodies were negative except for anticardiolipin antibodies. She was treated with intravenous piperacillin-tazobactam for 9 d, plus linezolid for 3 d for anti-infection, and deslanoside and digoxin for anti-heart failure. The child’s chest congestion and polyserositis improved after these treatments, but the abscesses and lesions in both lungs did not improve. Abscess aspiration and drainage were then performed. No pathogens were found in pus from the abscess, ascites or sputum smear including acid-fast smear. Multiple culture of blood, aspirated pus, ascites and sputum,including common bacteria and fungi culture, as well as incubation in Loewenstein-Jensen medium at 37℃ for 42 d, were all negative. Adenosine deaminase (ADA) in abscess drainage fluid was 2 U/L. The pathological manifestations in abscess tissue from the right psoas showed numerous lymphocytes and neutrophils infiltration. A small number of multinuclear giant cells, and granulation tissues were found,indicating suppurative and granulomatous inflammation (Figure 3). Due to her cardiac insufficiency, fiber bronchoscopy was not feasible at the time.

Figure 3 The pathological manifestations of abscess tissue on the lower right back shows numerous lymphocytes and neutrophils infiltration, a small number of multinuclear giant cells and granulation tissues were found, which confirmed suppurative and granulomatous inflammation. A: Magnification of 200 ×, B: Magnification of 400 ×.
Therefore, NGS of the patient’s FFPE specimen was performed to identify the causative pathogen.
FINAL DIAGNOSIS
Two days later, a significantly high abundance ofMycobacteriumwas detected with 9261 reads, 6225 of which matchedM. mucogenicum. Two other pathogens were also found:Aggregatibacter(7246 reads, includingAggregatibacter actinomycetemcomitans6912 reads andAggregatibacter segnis4 reads) andMeiothermus(6938 reads, includingMeiothermus silvanus6461 reads andMeiothermus ruber287 reads) (Figure 4). The former is normally found in the human oropharynx, which seldom causes disease, but occasionally causes infective endocarditis, pneumonia, brain abscess,etc.There are no reports on skin infections caused byAggregatibacter. The latter is a Gram-negative thermophilic bacterium. To the best of our knowledge, there are no reports of human diseases caused byMeiothermus.
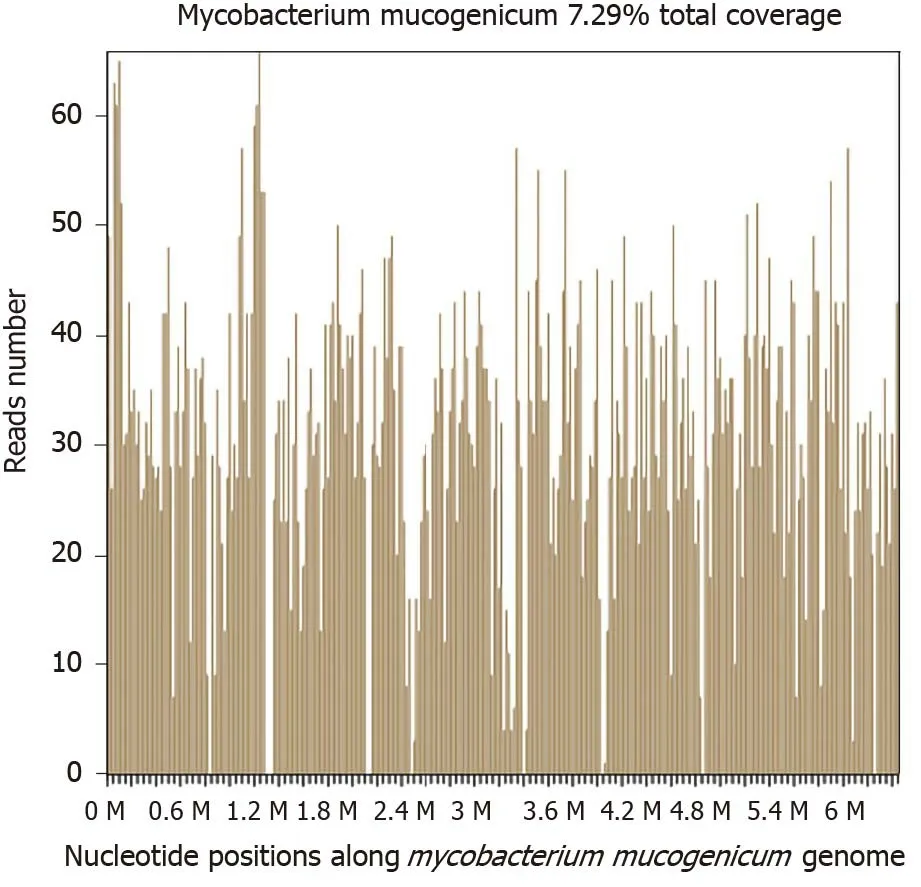
Figure 4 Sequencing results and phylogenetic analysis show nucleotide positions in the Mycobacterium mucogenicum genome.
In addition, the patient and her parents underwent analysis of genes related to immunologic function, but no clinically significant findings were observed. No evidence of interferon-γ receptor deficiency or hyper-IgE syndrome was found.
TREATMENT
M. mucogenicumwas treated as the causative pathogen of the abscesses.M.mucogenicumis closely related to theM. fortuitumgroup[8],which is usually sensitive to clarithromycin, trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline,quinolones, aminoglycosides and so on as suggested by the SANFORD GUIDE[9].Due to the limitation of quinolones and aminoglycoside antibiotics use in children in China, she was given clarithromycin 250 mg bid plus TMP-SMX 2#bid plus doxycycline 50 mg bid.
OUTCOME AND FOLLOW-UP
All abscesses decreased in size (Figure 5), her cough disappeared, anemia recovered and the child gained weight 12 d later. The WBC count, neutrophils%, ESR, CRP, PCT,NT-proBNP, and CKMB gradually returned to normal. The wounds healed gradually with scars within 12 wk (Figure 6), while inflammation in both lungs significantly improved but not all was absorbed and a little fibrosis was present, suggesting chronic infection (Figure 7). There were no notable adverse reactions in this patient during the one-year treatment period. The patient had a normal biochemical index with no recurrence four months after the end of the one-year treatment period (Figure 8).

Figure 5 These images show the four wounds on the 12th day after anti-nontuberculous mycobacteria treatment. A: A mass on the right upper abdomen; B: A mass on the left lower back; C: Two masses on the right back.

Figure 6 These images show the four wounds on the 90th day after anti-nontuberculous mycobacteria treatment. A: A mass on the right upper abdomen, B: A mass on the left lower back; C: Two masses on the right back.
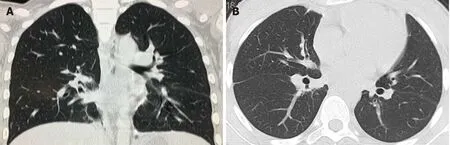
Figure 7 The chest computed tomography on January 23, 2019 shows pleural effusion on both sides were absorbed completely, and patchy and streaky cloudy opacities on both lungs were improved compared with the images in Figure 2. A: The sagittal plane; B: The horizontal plane.
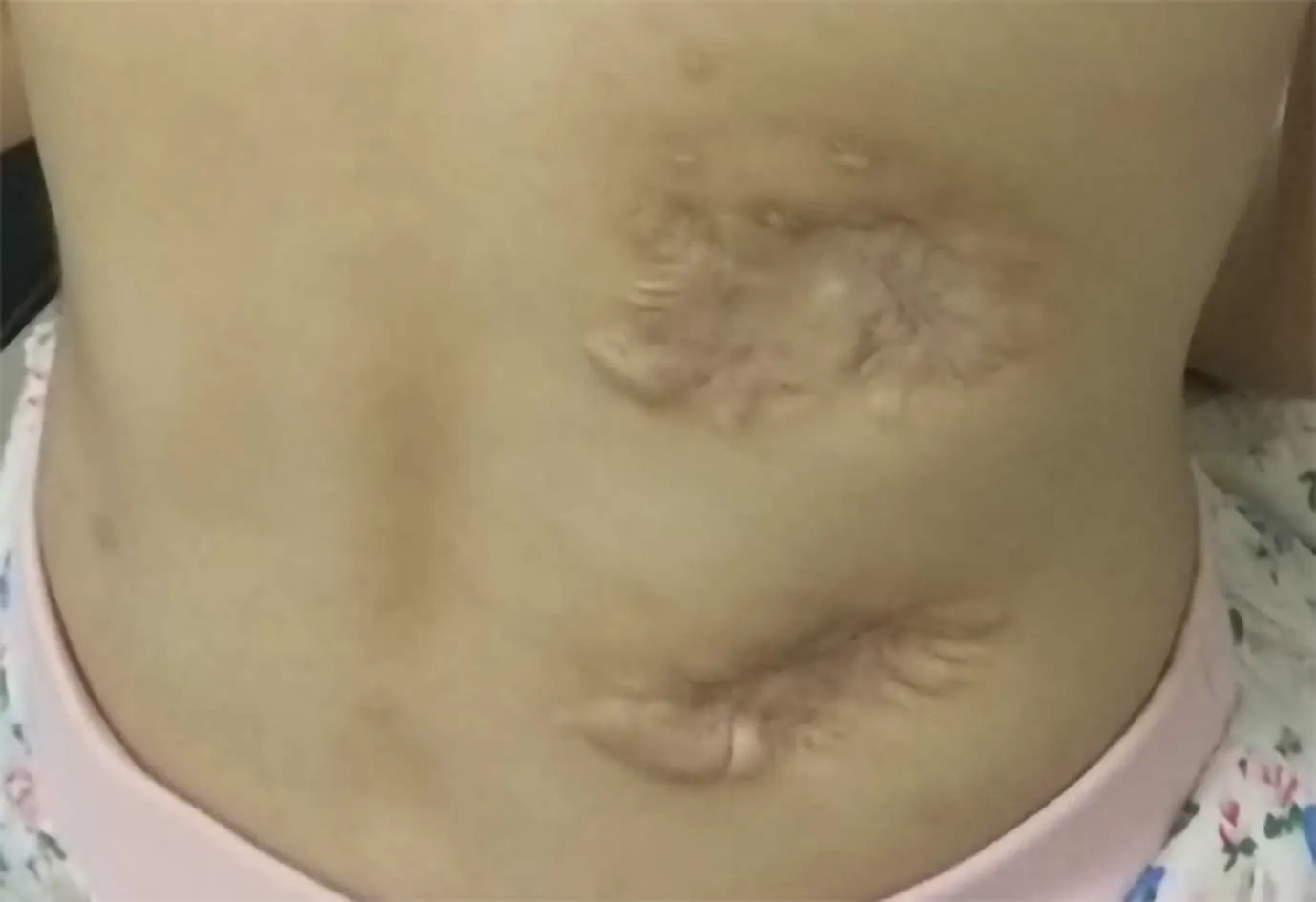
Figure 8 This image shows two masses on the right back in February, 2021.
DISCUSSION
M. mucogenicum, a ubiquitous RGM, has been recognized as a species since 1995. The organism was first calledM. chelonae-like organism and caused diseases in humans in 1982, and during two outbreaks of peritonitis associated with peritoneal dialysis in the United States in 1976 and 1978[10].M. mucogenicumis more closely related to theM.fortuitumgroup by 16S rDNA sequencing than otherMycobacteriumgroups[8].The mucoid surface provides the ability to form a protective biofilm, which contributes to infection of central venous catheters and skin soft-tissue usually post-trauma, which are clinically the most common sites ofM. mucogenicuminfections[11]. Moreover, it can cause respiratory infections, bloodstream infections, osteomyelitis, and disseminated infections, which are common in immunocompromised hosts[3,12]. Equipment exposed toM. mucogenicumcontaminated water can lead to nosocomial infections,including central venous catheter-related and hemodialysis-related infections[1,13].
There was no evidence of immunodeficiency in our patient, even after the detection of genes related to immunologic function in the patient and her parents. Undoubtedly,it was necessary to determine the source of infection, but we did not have evidence of pneumonia with NTM infection. We could not perform fiber bronchoscopy in this patient as she had cardiac insufficiency. However, her pneumonia rapidly improved after anti-NTM treatment. It is unlikely that the infection was nosocomial. Due to the pulmonary lesions and multiple skin lesions and the good therapeutic effect, it is reasonable to presume that the source of infection with this microorganism wasviathe upper or lower respiratory tract, then a bloodstream infection, followed by a skin softtissue infection.
For identification of this microorganism, there are several major methods. The first is conventional culture methodology. This is still difficult and delays in culture lead to missed diagnosis[14]. The second is DNA sequencing with 16S rRNA gene, rpoB, and hsp65 being recognized as useful targets[15-17]. However, due to its targeting,limitations are unavoidable in the identification of uncertain pathogens. The third is matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDITOF MS). Several investigators have demonstrated that MALDI-TOF MS can accurately identify mycobacteria[18,19]. However, these methods are not available in many laboratories.
In the present study, smears and cultures for bacteria, fungi and tuberculosis culture were all negative. Moreover, the results of the biopsy on the right psoas were not satisfactory. Therefore, we performed NGS using a FFPE specimen. Metagenomic NGS has emerged as a promising technological platform for directly identifying and classifying pathogens in complex clinical specimens from patients in a short time at reasonable cost[4]. It works well with short nucleic acid sequences, thus, it can be used to analyze fragmented DNA and RNA extracted from standard FFPE clinical specimens in theory. FFPE specimens have gained interest as an alternative to fresh/frozen tissue for storage, due to FFPE tissue validation in archival samples of biomarkers of exposure, prognosis and disease[20]. FFPE tissue processing remains the most economical approach for longitudinal tissue specimen storage. The ability to apply high throughput genomic applications to FFPE specimens can expand clinical study[21]. We have performed the mNGS technique to analyze the presence of pathogens in FFPE tissues which is one of the most widely available techniques for preserving clinical specimens. The macromolecules extracted from blocks stored for over 11-12 years, 5-7 years, or 1-2 years were not significantly different to recently prepared blocks[22]. FFPE tissue specimens are collected following IRB-approved protocols and stored on site in our climate-controlled biorepository. The FFPE tissue can match both clinical and molecular research endpoints. FFPE specimens collected in a routine clinical environment are a good source of DNA that can be applied in mNGS analysis for clinical pathogen detection[23]. In previous research, FFPE specimens were used for whole genome sequencing, mainly in cancer patients[23,24]. Using FFPE tissue for pathogen identification was also reported in recent years, such as 16S PCR of brain tissue[25], RNA sequencing of 1918 influenza samples[26] and corneal infection diagnosis[27].
To our knowledge, this is the first report onM. mucogenicumconfirmed by NGS using a FFPE specimen. In this study, it was feasible to use metagenomic NGS of DNA extracted from a FFPE clinical specimen to identify the causative microorganism. This method holds great promise for the relatively rapid detection of microorganisms,including rare pathogens and cases in which conventional cultures were not attempted or failed to yield positive results.
Following combination therapy with clarithromycin, doxycycline and TMP-SMX,the patient was treated for over 1 yr, and improvement was observed. However, the optimal duration of antimicrobial therapy for disseminated infection withM.mucogenicumis unknown. It is certain that prolonged therapy for one to two years even more contributes to the eradication of infection and reduces the chance of recurrence[1].
CONCLUSION
Next-generation sequencing is a promising tool for the rapid and accurate diagnosis of rare pathogens based on negative results with the conventional culture, even when using a formalin-fixed, paraffin-embedded specimen.
ACKNOWLEDGEMENTS
We thank the patient and her parents for their support and cooperation in publishing this work. We also thank the doctors of the local hospital and another hospital in Guangzhou for the patients’ initial diagnosis and treatment, and the doctor of the First Affiliated Hospital of Sun Yat-Sen University for the patient’s pathological diagnosis.We also thank BGI Genomics Co., Ltd for identification ofM. mucogenicum.
 World Journal of Clinical Cases2021年20期
World Journal of Clinical Cases2021年20期
- World Journal of Clinical Cases的其它文章
- Obesity in people with diabetes in COVID-19 times: Important considerations and precautions to be taken
- Revisiting delayed appendectomy in patients with acute appendicitis
- Detection of short stature homeobox 2 and RAS-associated domain family 1 subtype A DNA methylation in interventional pulmonology
- Borderline resectable pancreatic cancer and vascular resections in the era of neoadjuvant therapy
- Esophageal manifestation in patients with scleroderma
- Exploration of transmission chain and prevention of the recurrence of coronavirus disease 2019 in Heilongjiang Province due to inhospital transmission