
Hemoglobin Fukuoka caused unexpected hemoglobin A1c results: A case report
2021-08-04 05:25XuePingLinQiuRongYuanShiQiongNiuXiJiangZhiKunWuZhaoFanLuo
World Journal of Clinical Cases 2021年20期
Xue-Ping Lin, Qiu-Rong Yuan, Shi-Qiong Niu, Xi Jiang, Zhi-Kun Wu, Zhao-Fan Luo
Xue-Ping Lin, Qiu-Rong Yuan, Shi-Qiong Niu, Xi Jiang, Zhi-Kun Wu, Zhao-Fan Luo, Department of Clinical Medical Laboratory, The Seventh Affiliated Hospital of Sun Yat-sen University,Shenzhen 518107, Guangdong Province, China
Abstract BACKGROUND Glycated hemoglobin (Hb) (HbA1c) is an indicator that is used to diagnose and monitor the treatment of diabetes. Many factors can affect the detection of HbA1c.One of the most important of these factors is the Hb variant. Here, we report a rare Hb variant and evaluate its effect on HbA1c.CASE SUMMARY A 35-year-old man was suspected of harboring an Hb variant following the measurement of HbA1c with the Variant II Turbo 2.0 Hb detection system during a routine examination. Subsequently, we used the Arkray HA-8160 and ARCHITECT c4000 system to reanalyze HbA1c. Finally, the Hb variant was detected with a Capillary2FP analyzer that operates on the principle of capillary electrophoresis. We also used gene sequencing to investigate the mutation site.The value of HbA1c detected with the Variant II Turbo 2.0 system was 52.7%.However, the Arkray HA-8160 system did not display a result while the ARCHITECT c16000 system showed a result of 5.4%. The Capillary2FP analyzer did not reveal any abnormal Hb zones. However, gene sequencing identified the presence of a mutation in the Hb β2 chain [CD2(CAC>TAC), His>Tyr, HBB:c.7C>T]; the genotype was Hb Fukuoka.CONCLUSION Hb variants could cause abnormal HbA1c results. For patients with Hb variants,different methods should be used to detect HbA1c.
Key Words: Hemoglobin Fukuoka; Hemoglobin A1c; Hemoglobin variant; High-performance liquid chromatography; Enzymatic method; Case report
INTRODUCTION
Hemoglobin A1c(HbA1c) is the main indicator recommended by the American Diabetes Association and the World Health Organization for the diagnosis of diabetes[1]. HbA1cis a stable compound that covalently bonds glucose and hemoglobin(Hb)β-chain Nterminal valine residues in human blood. It reflects the average blood glucose concentration over the previous 2 mo to 3 mo. However, the results of the HbA1care affected by a wide range of factors, including Hb variants, severe hemolytic anemia, and severe liver disease,etc. The most common factors that interfere with HbA1ctests are Hb variants[2,3]. In this paper, we report a case with abnormal HbA1cvalues, which was eventually diagnosed as a rare Hb mutation.
CASE PRESENTATION
Chief complaints
A 35-year-old man arrived at our hospital for a physical examination in November 2018.
History of past illness
The patient had no special past history.
Personal and family history
The patient had no special personal and family history.
Physical examination
Normal physical examination without any obvious signs of abnormality.
Laboratory examinations
The HbA1cresult of 52.7% was out of the expected detection range (Figure 1A). The HbA1cof the patient was remarkably elevated in comparison to the reference range(4.0%-6.4%). Data arising from routine blood analyses are shown in Table 1. The patient had normal liver function, normal fasting glucose, and no previous history of diabetes. The HbA1ctest was performed using the Biorad Variant II Turbo 2.0 automatic glycated Hb analyzer (Biorad, United States); the HbA1cvalue was abnormally elevated, although the patient had no history of diabetes. Therefore, we suspected that the patient possessed Hb variants that interfered with the results of the HbA1ctest.
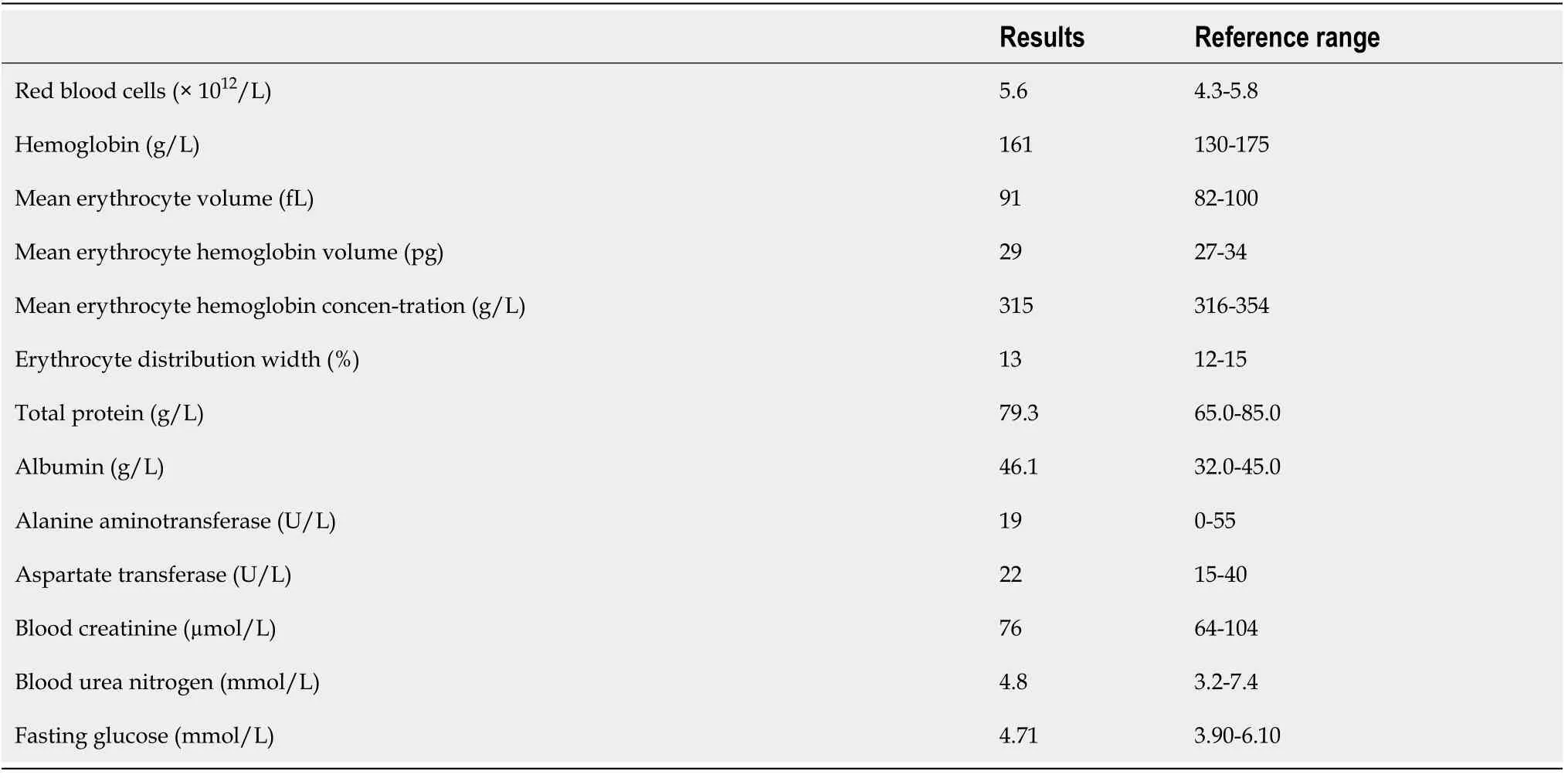
Table 1 Routine blood data
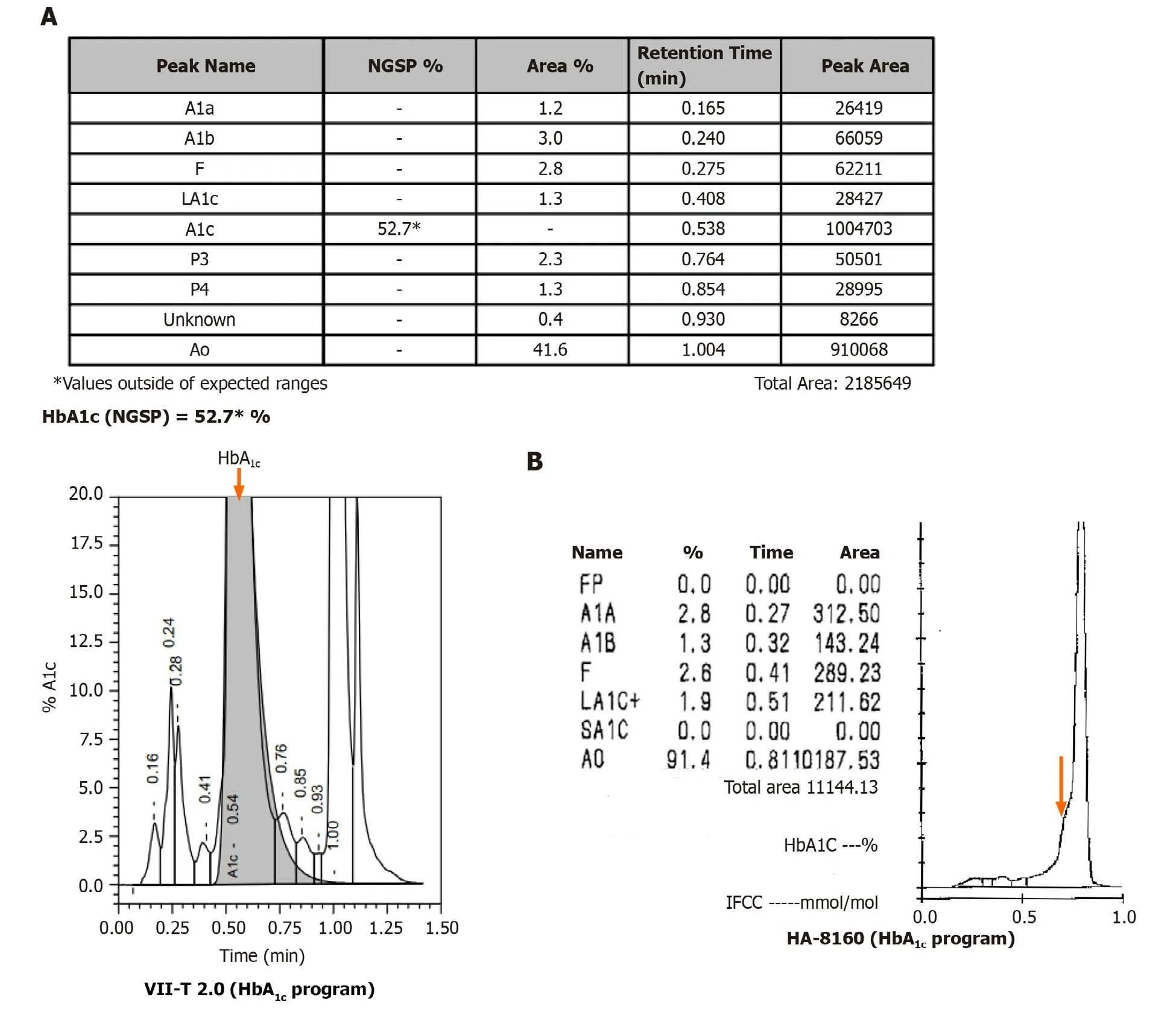
Figure 1 Detection of hemoglobin A1c with a Variant II Turbo 2.0 system and an Arkray HA-8160 system.A:The peak of hemoglobin A1c(HbA1c)was abnormally elevated (orange arrow); B: The HbA1c peak did not appear, and there was an abnormal protruding peak on the left of peak A0 (orange arrow). HbA1c:Hemoglobin A1c.
Further investigations for Hb variants
We attempted to confirm the HbA1cvalue by using the Arkray HA-8160 automatic glycated Hb analyzer (Arcolai, Japan), which features high-performance liquid chromatography (HPLC), and the ARCHITECT c4000 system (Abbott, United States),which operates by enzymatic methods. The Arkray HA-8160 system returned no result; the instrument showed that the HbA1cpeak did not appear, and there was anabnormal protruding peak on the left of peak A0(Figure 1B). The ARCHITECT c16000 enzyme assay returned a result of 5.4%.
Next, we used the Capillary2FP automated Hb analyzer (Sebia, France) to find the presence of abnormal Hb. Capillary electrophoresis showed no abnormal Hb bands(Figure 2).
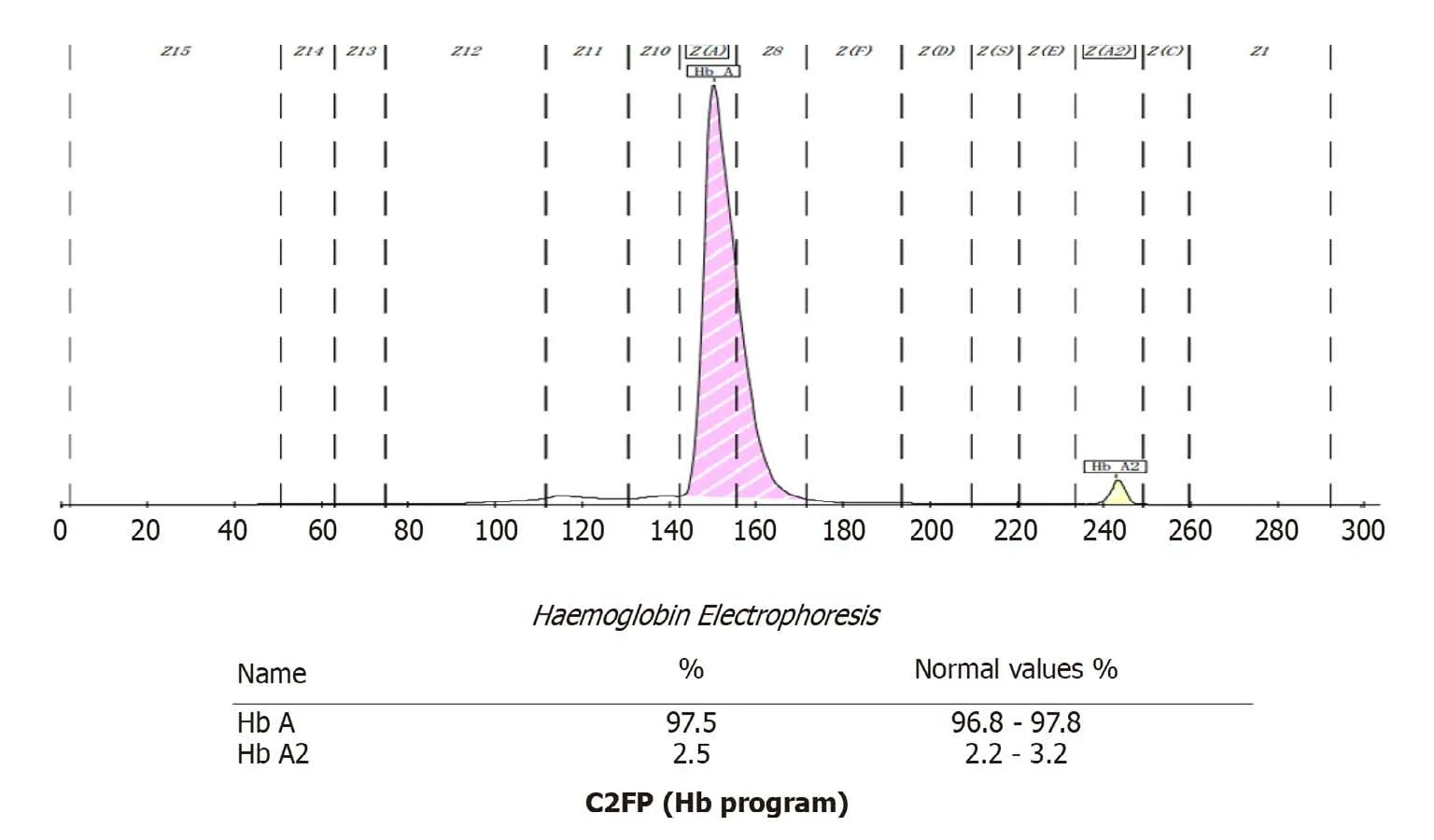
Figure 2 A Capillary2FP system was used to find the hemoglobin variant. Hb: Hemoglobin.
In addition, the patient's genomic DNA was extracted using a Genomic DNA Isolation Kit (Kaipu, China) and theHBA1,HBA2, andHBBgenes were amplified with specific forward/reverse primers and sequenced on an ABI3500 sequencer.HBA1forward primer was 5´-CGCGCCAGCCAATGAGC-3´ andHBA1reverse primer was 5´-ACACACA TGGCTAGAACCTCTCTG-3´.HBA2forward primer was 5´-GGGCT CCGCGCCAGCCAA-3´ andHBA2reverse primer was 5´-CAAGGACCTCTCT GCAGCT-3´.HBBforward primer was 5´-TACGGCTGTCATCACTTAG-3´andHBBreverse primer was 5´-GCCACACTGAGTGAGCTGCACT-3´. We extracted a sample of whole blood from the patient and extracted genomic DNA. This was used as a template to amplify theHbgene. Polymerase chain reaction amplicons were then sequenced. No thalassemia mutation types were found in the sequencing range for α1 and α2. However, the β-globin gene possessed a histidine > tyrosine (CAC >TAC)mutation in the 7thamino acid, C>T (Figure 3). Next, we searched the HbA1cvariant library website (http://globin.bx.psu.edu/hbvar/menu.html), which revealed that the Hb genotype was Hb Fukuoka (HBB:c.7C>T). Finally, the patient was confirmed to possess a heterozygous Hb Fukuoka mutation.

Figure 3 Gene sequencing results revealed a β chain mutation in the gene [CD2(CAC>TAC), His>Tyr, HBB:c.7C>T] (orange arrow).
FINAL DIAGNOSIS
Finally, the patient was confirmed to possess a heterozygous Hb Fukuoka mutation.
TREATMENT
The patient was not treated.
OUTCOME AND FOLLOW-UP
For patients with Hb variants, we recommend the use of an assay that is not affected by interference caused by Hb variants.
DISCUSSION
The guidelines relating to diabetes mellitus that were published by the American Chemical Society in 2011 suggest that a patient should receive further research/investigation if HbA1c> 15% or if the laboratory data are inconsistent with clinical manifestations. The guidelines also recommend the use of different test principles and methods so that the patient can be re-tested[4]. In this case, the patient’s HbA1cwas 52.7%,significantly higher than 15%. The patient had no history of diabetes. Laboratory data were all within the normal quantitative range, including Hb, kidney and liver function parameters, and fasting blood glucose. Therefore, it was necessary to retest this patient and identify reasons that might underlie the abnormal HbA1cresult.
Biorad Variant II Turbo 2.0 and Arkray HA-8160 Glycation Hemoglobin analyzers are based on HPLC technology. Using this technology, it is possible to separate Hb fractions by differential affinity to the internal surface of the column or to the buffer.The greater the affinity to the buffer, the faster the elution, and the shorter the retention time. The greater the affinity to the analytical column, the slower the elution,and the longer the retention time. In this case, the Biorad Variant II Turbo 2.0 returned an HbA1cresult of 52.7%, and no result was detected by Arkray HA-8160. Therefore,we considered the possibility of interference caused by Hb variants. Hb variants can affect the separation of variants from HbA1cor HbA by changing their charge, coeluting with HbA1c, and replacing glycosylation sites[5,6]. The NGSP website has declared that the common variants including S, C, D, and E have no effect on Biorad Variant II Turbo 2.0 (http://ngsp.org/factors.asp). However, some rare Hb variants can affect HbA1cwith HPLC[7,8]. The ARCHITECT c16000 uses enzymatic methods to detect HbA1cvalues. By lysing the whole blood sample and performing extensive proteolytic digestion, the Hb β chain releases amino acids, especially the glycated Nterminal valine. The signal generated by the glycosylated valine in the subsequent color-based reaction can then be used to calculate the HbA1c. At the analytical level,these methods are unaffected by the presence of Hb variants, such as HbC, HbD, HbE,and HbS. However, this method is unable to detect Hb variants[9]. Therefore, an HbA1cresult of 5.4% can accurately reflect the glycated Hb of the patient. The Capillary 2FP system operates on the principle of capillary electrophoresis and was used to investigate for the presence of an Hb variant. The Capillary 2FP system showed no abnormal Hb bands. Gene sequencing identified the variant as an Hb Fukuoka heterozygote. This variant was first reported in Japan in 1985, and subsequently reported by both Haranoet al[10] and Farahet al[11]. Haranoet al[10] found abnormal Hb peak in a diabetic patient's HbA1ctest in 1990, and identified that the patient had Hb Fukuoka.Furthermore, Farahet al[11] identified the presence of Hb Fukuoka by performing electrophoresis examinations in a patient with anemia. As far as we know, this case was the first case to be discovered in China.
Several methods can be used to detect glycosylated Hb, including electrophoresis,immunoturbidimetric assay (immunoassay), enzymatic assay, boronate affinity, ionexchange HPLC, or capillary electrophoresis. Laboratories should be aware of the limitations of their methods with respect to interference from other Hb variants and suggest alternative HbA1cquantification methods[12,13].For patients with Hb variants, we recommend the use of an assay that is not affected by interference caused by Hb variants; this strategy will help avoid erroneous results that can mislead data in clinical practice[14]. Glycated albumin and fructosamine are recommended as alternative indicators to monitor glycaemia when HbA1cis disturbed[15].
CONCLUSION
The chromatographic pattern of abnormal Hb variants differs from that of normal samples, making it difficult for some instruments to determine accurate HbA1cvalues.HbA1cis an important indicator for the diagnosis, treatment, and monitoring of diabetes mellitus, and the accuracy of HbA1cresults is of paramount importance. But meanwhile, it is important for laboratory staff to be familiar with the factors that may cause interference, and to be able to communicate with clinicians in a timely manner to clarify the situation and make clinical suggestions. The ultimate goal is to ensure accurate and realistic test results so as to help clinical diagnosis.
ACKNOWLEDGEMENTS
We are grateful for instructive discussion with Professor Luo ZF.
 World Journal of Clinical Cases2021年20期
World Journal of Clinical Cases2021年20期
- World Journal of Clinical Cases的其它文章
- Obesity in people with diabetes in COVID-19 times: Important considerations and precautions to be taken
- Revisiting delayed appendectomy in patients with acute appendicitis
- Detection of short stature homeobox 2 and RAS-associated domain family 1 subtype A DNA methylation in interventional pulmonology
- Borderline resectable pancreatic cancer and vascular resections in the era of neoadjuvant therapy
- Esophageal manifestation in patients with scleroderma
- Exploration of transmission chain and prevention of the recurrence of coronavirus disease 2019 in Heilongjiang Province due to inhospital transmission