
Effects of angiotensin receptor blockers and angiotensin-converting enzyme inhibitors on COVID-19
2021-08-04 05:25XiaoLongLiTaoLiQiCongDuLiYangKunLunHe
World Journal of Clinical Cases 2021年20期
Xiao-Long Li, Tao Li, Qi-Cong Du, Li Yang, Kun-Lun He
Xiao-Long Li, Department of Diagnostic Radiology, PLA General Hospital, Beijing 100853,China
Tao Li, Li Yang, Department of Radiology, The First Medical Center of PLA General Hospital,Beijing 100853, China
Qi-Cong Du, Department of Diagnostic Radiology, The First Medical Center of PLA General Hospital, Beijing 100853, China
Kun-Lun He, Translational Medical Research Center, Key Laboratory of Ministry of Industry and Information Technology of Biomedical Engineering and Translational Medicine, Medical Innovation Research Division of Chinese PLA General Hospital, Beijing 100853, China
Abstract BACKGROUND The World Health Organization reported that 28637952 people worldwide had been infected with severe acute respiratory syndrome coronavirus 2, the causative agent of coronavirus disease 2019 (COVID-19), by September 13.AIM The aim was to investigate whether long-term use of renin-angiotensin-aldosterone system (RAAS) inhibitors for the treatment of hypertension aggravates the performance of COVID-19 patients with hypertension.METHODS This was a retrospective analysis of lung computed tomography (CT) data and laboratory values of COVID-19 patients with hypertension who were admitted to Huoshenshan Hospital, Wuhan, Hubei Province, between February 18 and March 31, 2020. Patients were divided into two groups. Group A included 19 people who were long-term users of RAAS inhibitors for hypertension; and group B included 28 people who were randomly selected from the database and matched with group A by age, sex, basic diseases, and long-term use of other antihypertensive drugs. All patients underwent a series of CT and laboratory tests. We compared the most severe CT images of the two groups and the laboratory examination results within 2 d of the corresponding CT images.RESULTS The time until the most severe CT images from the onset of COVID-19 was 30.37 ±14.25 d group A and 26.50 ± 11.97 d in group B. The difference between the two groups was not significant (t = 1.01, P = 0.32). There were no significant differences in blood laboratory values, C-reactive protein, markers of cardiac injury, liver function, or kidney function between the two groups. There was no significant difference in the appearance of the CT images between the two groups.The semiquantitative scores of each involved lobe were 11.84 ± 5.88 in group A and 10.36 ± 6.04 group B. The difference was not significantly different (t = 0.84, P= 0.41).CONCLUSION Chest CT is an important imaging tool to monitor the characteristics of COVID-19 and the degree of lung injury. Chronic use of RAAS inhibitors is not related to the severity of COVID-19, and it does not worsen the clinical process.
Key Words: COVID-19 infection; Hypertensive patients; Angiotensin-converting enzyme inhibitors; Angiotensin receptor blockers
INTRODUCTION
The World Health Organization reported that 28,637,952 people worldwide had been infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of coronavirus disease 2019 (COVID-19), by September 13. Animal experiments have shown that angiotensin-converting enzyme 2 (ACE2) is abundantly expressed in lung, heart and other tissues, and coronaviruses use it as a functional receptor to invade human cells[1-3]. Inhibitors of the renin-angiotensin-aldosterone system (RAAS), namely angiotensin receptor blockers (ARBs) and ACE inhibitors, are first-line drugs for the treatment of hypertension. Some scholars believe that the use of RAAS inhibitors by COVID-19 patients with hypertension will aggravate COVID-19[4-6]. Some investigators also believe that ARBs and ACE inhibitors can inhibit both the activity of the RAAS and the progression of respiratory injury, thus playing a protective role in COVID-19 patients[7-9]. However, those assumptions are mainly based on animal experiments and lack clinical evidence. This study aimed to investigate whether the use of RAAS inhibitors by COVID-19 patients with hypertension aggravated the severity of pneumonia.
MATERIALS AND METHODS
Case data
COVID-19 patients with hypertension who were hospitalized in Huoshenshan Hospital in Wuhan, Hubei Province, between February 18 and March 31, 2020 were analyzed retrospectively. COVID-19’s diagnostic criteria refer to the National Health Commission’s "diagnosis and treatment plan of pneumonia infected by corona virus disease 2019" (trial version 7)[10]. All patients were positive for 2019 novel coronavirus by a laboratory nucleic acid assay (real-time fluorescence polymerase chain reaction,RT-PCR) of pharyngeal swab samples. The standard of cure and discharge required a return of body temperature to normal for more than 3 d, improved respiratory symptoms, significant improvement of the exudative lesions on chest CT, and negative RT-PCR assays of throat swabs with intervals of more than 24 h. COVID-19 patients with hypertension were divided into two groups. Group A included COVID-19 patients with long-term use of ACE inhibitors or/and ARBs recorded in their medical records. Group B included COVID-19 patients with long-term use of other antihypertensive drugs (calcium channel blockers, diuretics, β-adrenoceptor blockers). Group A and group B were matched by age, sex, and underlying diseases, and were randomly selected from the database with a ratio of 1:1.5.
The clinical histories, laboratory test results, and epidemiological histories of the patients were collected. The patients were stratified by mild, normal, severe, and critical disease following the “diagnosis and treatment of pneumonia infected by corona virus disease 2019 (trial version 7)” criteria[10]. All patients underwent a series of CT and laboratory examinations. The most severe CT findings and laboratory results obtained in the two groups within 2 d of the CT examination were compared.Laboratory tests included routine blood counts, C-reactive protein, liver function,renal function, and myocardial injury markers, myoglobin, hypersensitive troponin I and creatine kinase (CK), and the heart failure marker B-type natriuretic peptide. The difference in severity of COVID-19 in patients with hypertension in group A and group B was determined by comparing the chest CT findings.
Image analysis
Chest CT images were read independently by two chest radiology specialists without knowing the clinical laboratory results and patient grouping, and resolved by discussion when there were differences. COVID-19 CT signs included ground glass density (GGD), consolidation, paving stone sign (thickening of the interlobular septum and intralobular septum on the GGD background), fibrous band, air bronchus sign,thickening of small blood vessels, and pleural exudation[11]. We used a semiquantitative scoring system to evaluate the degree of lung involvement based on the number of lobes involved[12], that is, five lobes on both sides. According to the lung parenchyma volume ratio of pneumonia to lobe, the score was 0-5 points in each lobe.The score was 0 if there were no lesions. The subsequent scores, defined as percentages of the lobe volume, were one point if the lesion volume was < 5%, two points if the lesion volume was 5%-25%, three points if the lesion volume was 26%-49%, four points if the lesion volume was 50%-75%, and five points if the lesion volume was > 75%. The total score was the sum of the cumulative scores of each lung lobe. Theoretically, the pulmonary lesions scores could be between 0 and 25 points.
Statistical analysis
Comparison of the characteristics of COVID-19 patients in the two groups who were treated with different antihypertensive drugs included age, sex, laboratory results,time from chest CT examination to onset, and chest CT score. The Kolmogorov-Smirnov test was used to determine whether the laboratory results and CT scores of the two groups were normally distributed. The values of normally distributed data were reported as means ± SD. Between-group differences were compared byt-tests.Measurement data that were not normally distributed were reported as medians (M)and quartiles (Q1, Q3), and between-group differences were compared by the Wilcoxon signed-rank test. Categorical variables were reported as frequencies and percentage and between-group comparisons were performed byχ2or Fisher exact tests. A two-tailedPvalue of < 0.05 was statistically significant. SPSS 21.0 (SPSS Inc.,Chicago, IL, United States) was used for the statistical analysis.
RESULTS
Clinical features
Forty-seven COVID-19 patients with hypertension were evaluated and compared, 19 in group A and 28 in group B. The clinical data are shown in Table 1. There were no significant differences in age and sex between the two groups. Initial clinicalsymptoms included fever, cough, chest tightness, shortness of breath, fatigue, and diarrhea. The average hospital stay was 11.56 ± 4.82 d in group A and 12.83 ± 5.35 d group B. The difference was not significant. In addition, there were no significant differences in the number of patients needing mechanical ventilation, the number admitted to the intensive care unit, or the number of deaths in the two groups.
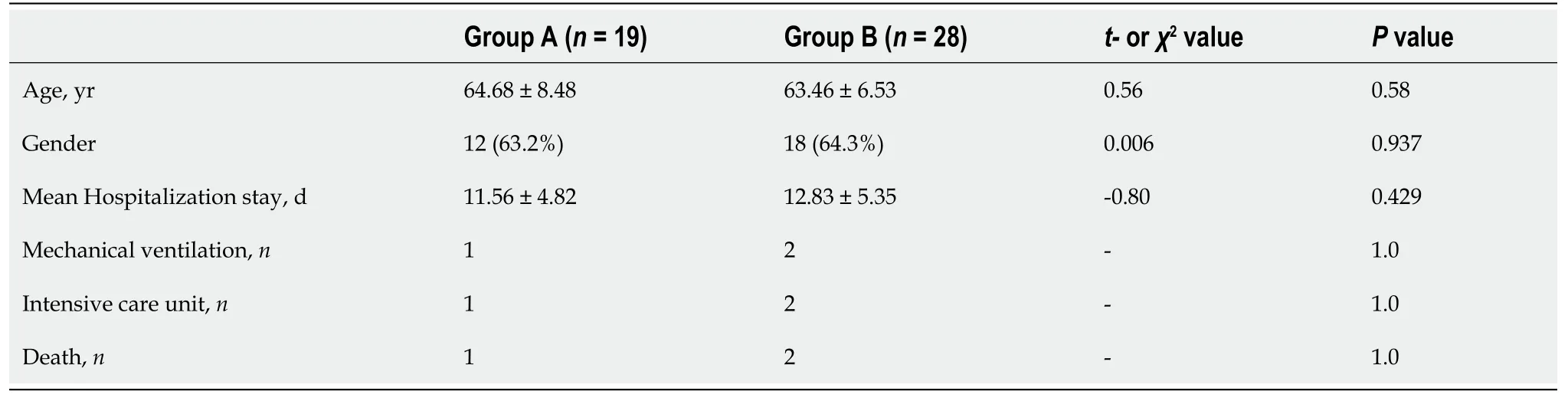
Table 1 Comparison of the clinical data of coronavirus disease 2019 patients treated with antihypertensive drugs
Laboratory examination
The laboratory results of the two groups are shown in Table 2. There were no significant differences in the routine blood count, C-reactive protein, myoglobin,hypersensitive troponin I, CK, B-type natriuretic peptide, liver function, and renal function between the two groups.
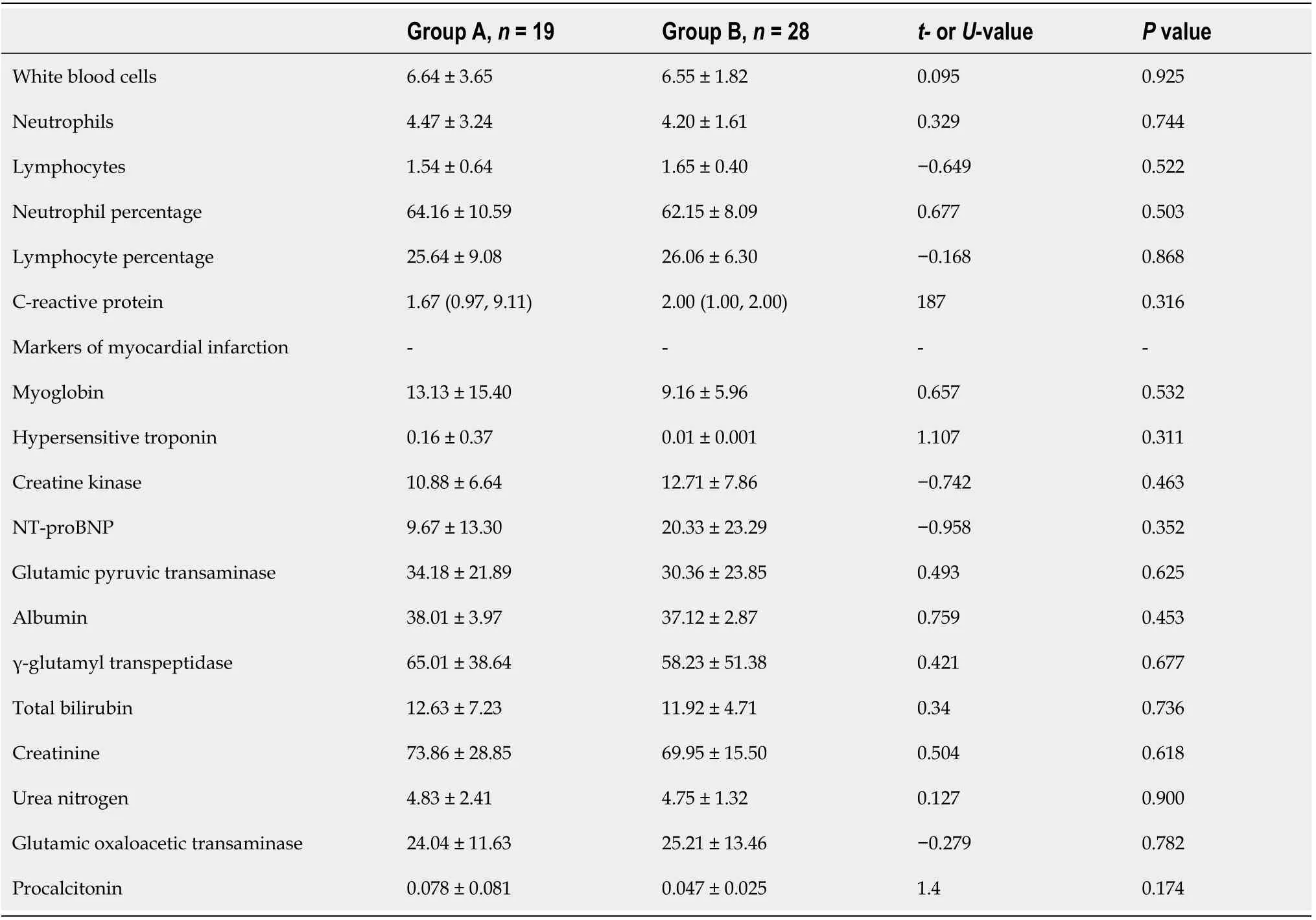
Table 2 Comparison of laboratory examination results of coronavirus disease 2019 patients currently using different antihypertensive drugs
CT performance
The time between the onset of disease and the CT images were 30.37 ± 14.25 d in group A and 26.50 ± 11.97d in group B. The difference was not significant (t= 1.01,P= 0.32).The peak of the course of disease was characterized in both groups by large GGD shadow, paving stone-like changes, and consolidation accompanied by thickening of small blood vessels, and air bronchial signs. The GGD shadow, paving stone sign, and consolidation gradually decreased and the fibrous band gradually increased (Figure 1)with recovery from the disease. There were no significant between-group differences in the GGD shadow, paving stone change, consolidation, and fibrous band formation.The total cumulative lung scores (Table 3) were 11.84 ± 5.88 in group A and 10.36 ±6.04 in and group B. The difference was not significant (t= 0.84,P= 0.41).
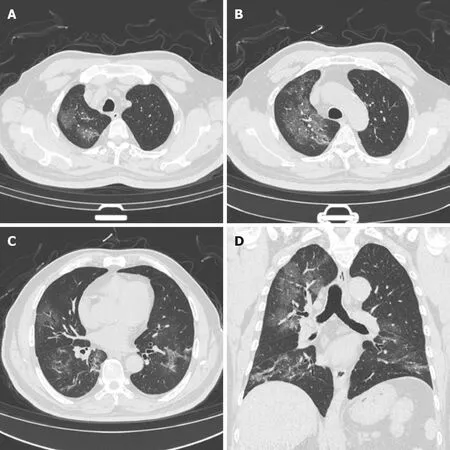
Figure 1 CT images from a 61-year-old male patient with a total lung score of 16 obtained 14 d after the onset of disease. A: A large ground glass density shadow of the right upper lobe; B: A large ground glass density of the right upper lobe with a small amount of flaky consolidation; C: A ground glass density shadow of the middle lobe of the right lung, paving-stone lesions of the lower lobe of the left lung, and a striped shadow in the lower lobe of both lungs; D:Coronal reconstruction images show a ground glass density shadow in the right upper lung. Both lower lungs are dominated by fibrous strips.

Table 3 Comparison of the computed tomography characteristics of coronavirus disease 2019 patients currently using various antihypertensive drugs, n (%)
DISCUSSION
The results showed that in COVID-19 patients with hypertension, chronic use of ACE inhibitors and/or ARBs did not worsen the clinical process compared with taking other antihypertensive drugs. In addition, there were no significant differences in the clinical characteristics or the results of routine blood, myocardial enzyme, liver function, renal function testing, or chest CT pneumonia findings.
SARS-CoV-2 enters the cell by binding to a protein called ACE2 followed by virus replication and cell death[13]. The ACE2 protein is widely distributed in the vascular endothelial cells of many tissues of the kidneys, heart, intestine, and liver. Animal experiments show that intravenous administration of ACE inhibitors and/or ARBs upregulates ACE2, thus worsening the clinical process of COVID-19[14]. However,clinical studies have shown that ACE inhibitors and ARBs may play a protective role against pneumonia[15]. This study showed that there were no significant differences in routine blood values, C-reactive protein, myocardial enzyme activity, liver function,renal function, chest CT pneumonia characteristics, or lung CT scores between COVID-19 patients treated with ACE inhibitors and ARBs and COVID-19 patients treated with other antihypertensive drugs. The results are consistent with recent studies showing that the use of ACE inhibitors and ARBs had nothing to do with the severity of COVID-19[16,17].
As a noninvasive and rapid imaging diagnostic tool, chest CT is an important means of diagnosing COVID-19. The sensitivity of chest CT to detect COVID-19 pneumonia is 98%[18]. The main imaging findings of COVID-19 include ground glass opacity,compaction, and paving stone-like changes[19]. Chest CTs can also monitor the progress and prognosis of the disease. Zhanget al[20] divided the course of COVID-19 into early, progressive, peak, and recovery stages. Ground glass opacity was mainly seen in the early stage and progressed to consolidation and paving stone-like changes as the disease evolved. In addition, the ground glass opacity can have a mixed form in the peak stage, and the fibrous band lesions can significantly increase in the recovery stage. Consolidation, paving stone-like lesions, and ground glass lesions decreased gradually, so the stages were not completely separated. This study showed that the most serious chest CT signs and chest CT lung-involvement scores were not significantly different between COVID-19 patients with hypertension treated with ACE inhibitors and ARBs and COVID-19 patients treated with other antihypertensive drugs.
This study had the following shortcomings: (1) The sample size was small and may be biased; and (2) It was a short-term retrospective study. We performed few preliminary exploratory evaluations. In addition, some patients had residual lung lesions when they met the discharge criteria. Long-term follow-up of large patient samples is still needed to monitor the outcome of pulmonary lesions.
CONCLUSION
Overall, this study shows that the clinical process of chronic treatment of hypertensive COVID-19 patients with ACE inhibitors and ARBs did not worsen their pneumonia.Chest CT is an important imaging method to monitor the characteristics of COVID-19 and the degree of lung involvement.
ARTICLE HIGHLIGHTS
Research background
The World Health Organization reported that 28637952 people worldwide had been infected with severe acute respiratory syndrome coronavirus 2, the causative agent of coronavirus disease 2019 (COVID-19), by September 13.
Research motivation
Some investigators believe that the use of RAAS inhibitors by COVID-19 patients with hypertension aggravates COVID-19. Some also believe that angiotensin receptor blockers (ARBs) and angiotensin-converting enzyme (ACE) inhibitors can inhibit the activity of the RAAS and as well as the progression of respiratory injury, thus playing a protective role in COVID-19 patients. However, those assumptions are based on animal experiments and lack clinical evidence. This study intended to resolve whether the use of RAAS inhibitors by COVID-19 patients with hypertension aggravated their degree of pneumonia.
Research objectives
The objective was to investigate whether long-term treatment with RAAS inhibitors aggravated the performance of COVID-19 patients with hypertension.
Research methods
This was a retrospective analysis of lung computed tomography (CT) data and laboratory values of COVID-19 patients with hypertension who were admitted to Huoshenshan Hospital, Wuhan, Hubei Province, between February 18 and March 31,2020. Patients were divided into two groups. Group A included 19 people who were long-term users of RAAS inhibitors for hypertension and group B included 28 people who were randomly selected from the patient database and matched with group A by age, sex, other diseases, and long-term use of other antihypertensive drugs. All patients underwent a series of CT and laboratory tests. We compared the most severe CT images of the two groups and the laboratory examination results within 2 d of obtaining the corresponding CT images.
Research results
Chest CT is an important imaging tool to monitor the characteristics of COVID-19 and the degree of lung injury. Chronic use of RAAS inhibitors was not related to the severity of COVID-19, and they did not worsen the clinical course.
Research conclusions
The clinical responses to the long-term treatment of hypertensive COVID-19 patients with ACE inhibitors and ARBs did not worsen their pneumonia. Chest CT is an important imaging method to monitor the characteristics of COVID-19 and the degree of lung involvement. This study showed that the most serious chest CT signs and chest CT scores of lung involvement were not significantly different between COVID-19 patients with hypertension treated with ACE inhibitors and ARBs and COVID-19 patients treated with other antihypertensive drugs. Animal experiments show that intravenous administration of ACE inhibitors and/or ARBs upregulates ACE2, thus worsening the clinical course of COVID-19. Clinical studies have shown that ACE inhibitors and ARBs may play a protective role against pneumonia This study showed that there were no significant differences in routine blood values, C-reactive protein,myocardial enzyme activity, liver function, renal function, chest CT pneumonia characteristics, or lung CT scores between COVID-19 patients treated with ACE inhibitors and ARBs and COVID-19 patients treated with other antihypertensive drugs. The results are consistent with recent studies finding that the use of ACE inhibitors and ARBs had nothing to do with the severity of COVID-19.
Research perspectives
This study has two shortcomings: (1) The sample size was small and may be biased;and (2) It was a short-term retrospective study. We performed few preliminary exploratory evaluations. In addition, some patients had residual lung lesions when they met the discharge criteria. The best perspective for future research is to conduct that long-term follow-up of large samples to monitor the outcome of pulmonary lesions.
 World Journal of Clinical Cases2021年20期
World Journal of Clinical Cases2021年20期
- World Journal of Clinical Cases的其它文章
- Obesity in people with diabetes in COVID-19 times: Important considerations and precautions to be taken
- Revisiting delayed appendectomy in patients with acute appendicitis
- Detection of short stature homeobox 2 and RAS-associated domain family 1 subtype A DNA methylation in interventional pulmonology
- Borderline resectable pancreatic cancer and vascular resections in the era of neoadjuvant therapy
- Esophageal manifestation in patients with scleroderma
- Exploration of transmission chain and prevention of the recurrence of coronavirus disease 2019 in Heilongjiang Province due to inhospital transmission