
Revisiting delayed appendectomy in patients with acute appendicitis
2021-08-04 05:25JianLi
World Journal of Clinical Cases 2021年20期
Jian Li
Jian Li, Department of General Surgery, The Third Hospital of Mianyang, Sichuan Mental Health Center, Mianyang 621000, Sichuan Province, China
Abstract Acute appendicitis (AA) is the most common acute abdomen, and appendectomy is the most common nonelective surgery performed worldwide. Despite the long history of understanding this disease and enhancements to medical care, many challenges remain in the diagnosis and treatment of AA. One of these challenges is the timing of appendectomy. In recent decades, extensive studies focused on this topic have been conducted, but there have been no conclusive answers. From the onset of symptoms to appendectomy, many factors can cause delay in the surgical intervention. Some are inevitable, and some can be modified and improved. The favorable and unfavorable results of these factors vary according to different situations. The purpose of this review is to discuss the causes of appendectomy delay and its risk-related costs. This review also explores strategies to balance the positive and negative effects of delayed appendectomy.
Key Words: Acute appendicitis; Appendectomy; Delay; Perforation; Postoperative complications
INTRODUCTION
A total of 7%-10% of patients in the emergency department (ED) present with acute abdominal pain, and acute appendicitis (AA) is diagnosed in the majority of these patients[1]. Since the nineteenth century, appendectomy has been widely accepted as the standard treatment for AA and has become the most common nonelective procedure performed by general surgeons. From the onset of symptoms to the ED visit and the subsequent appendectomy, delays contributable to various factors are inevitable. It is generally thought that untreated appendicitis will eventually progress to perforation, with an associated drastic increase in morbidity and mortality, leading to the traditional concept that appendectomy should be performed expeditiously after a diagnosis is made. However, in the last two decades, extensive research has been conducted on the association between delay in appendectomy and the outcomes of patients, and data on this topic are controversial, especially findings regarding inhospital delay (Figure 1). The purpose of this review is to discuss the causes of appendectomy delay and its risk-related costs. This review also explores strategies to balance the positive and negative effects of delayed appendectomy.
WHY TO DELAY AN APPENDECTOMY
Spontaneous resolution
The principle of early operation to prevent perforation has been the standard management for patients with suspected AA for more than 100 years, which is based on a theory that untreated appendicitis will eventually progress to perforation, with an associated increase in morbidity and mortality. However, from the beginning of the 20thcentury to the contemporary era, spontaneous resolution of AA has been recognized by many surgeons, although the implications of this possibility were seldom taken into account[2]. An increasing amount of circumstantial evidence suggests that not all patients with appendicitis will progress to perforation and that spontaneous resolution of untreated, nonperforated appendicitis may be a common event[3-5]. In addition, time series analysis found that the incidence of AA decreased overall, which was mainly attributed to nonperforated but not perforated AA,suggesting that a disconnect exists between the two types of appendicitis[6]. These observations led to a debating theory proposed by Andersson that AA can be divided into two separate subtypes with different fates[2]. The reversible form is simple inflamed appendicitis, which can present as phlegmonous (pus-producing) or advanced inflammation (but without gangrene or perforation) that needs appendectomy or, alternatively, as mild inflammation that can resolute either spontaneously or with antibiotic therapy; this form of AA will not proceed to gangrene and perforation. In contrast, the more severe inflammatory form proceeds to gangrene and perforation rapidly (Figure 2)[7]. Data to support separate types of inflammation also arise from laboratory and genetic studies reporting that the highly inflammatory Th17 subset was mainly found in sera from patients with gangrenous appendicitis but not in phlegmonous appendicitis, and the perforation might be the result of immunemediated tissue destructionviaan exaggerated immune response rather than caused by delaying appendectomy[8,9].

Figure 1 Timeline of the key events in the history of and research into surgery delay in patients with acute appendicitis. AA: Acute appendicitis; EAES: European Association for Endoscopic Surgery; COVID-19: Coronavirus disease 2019; ED: Emergency department; HD: Hospital day; RCT:Randomized controlled study; WSES: World Society of Emergency Surgery.

Figure 2 Subtypes of acute appendicitis with different fates determined by inflammation progression and interventions. NOM: Non-operative management.
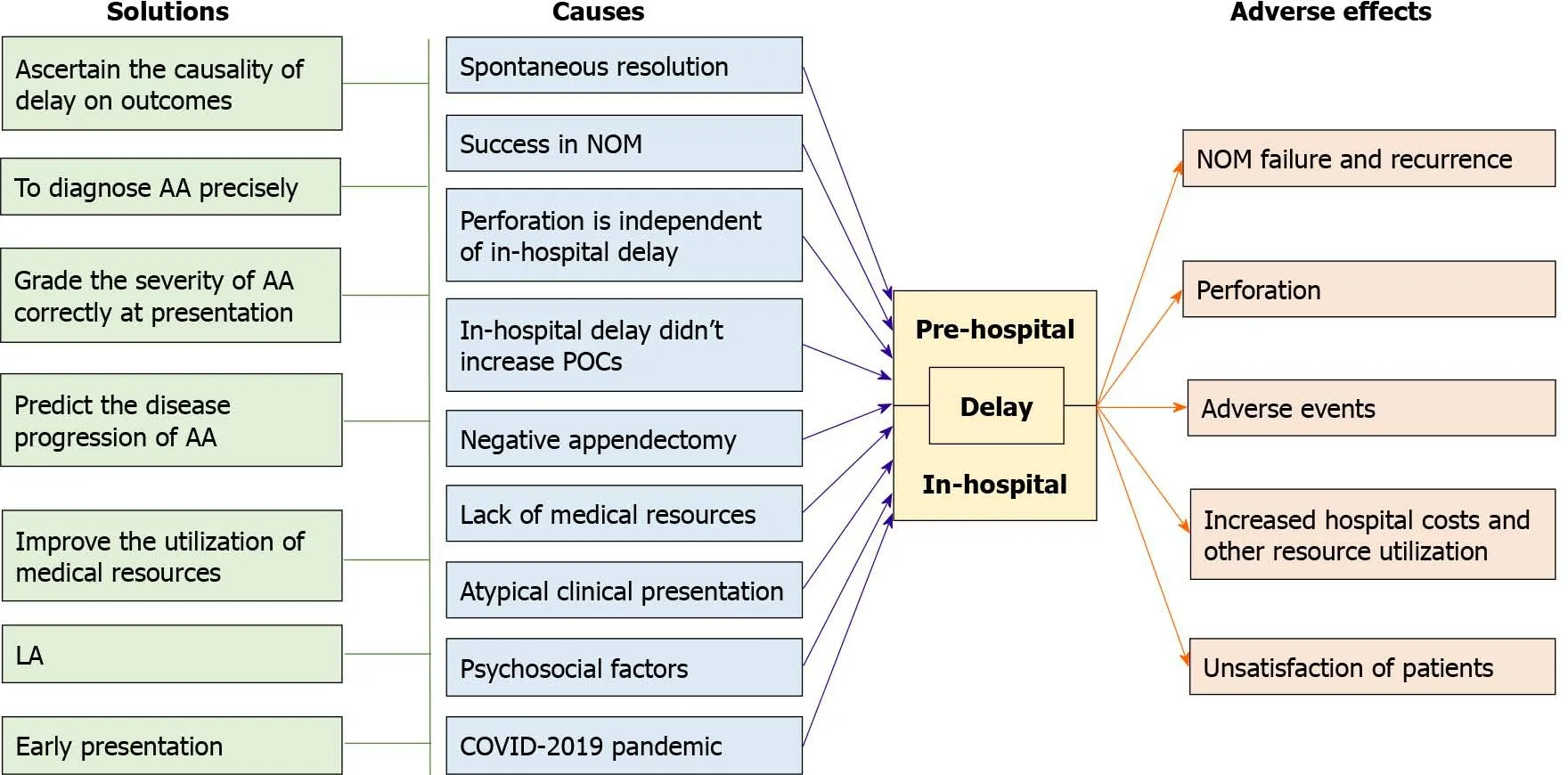
Figure 3 Causes, adverse effects, and resolutions of preoperative delay in patients with acute appendicitis.AA: Acute appendicitis; COVID-19:Coronavirus disease 2019; LA: Laparoscopic appendectomy; NOM: Non-operative management; POCs: Postoperative complications.
Success in nonoperative management
Over the past two decades, there has been increasing interest in the nonoperative management (NOM) of uncomplicated AA aimed at avoiding postoperative complications (POCs) and the higher costs of surgical interventions[10,11]. As early as 1959,Coldrey E treated 471 unselected patients with suspected AA conservatively, with low mortality and morbidity rates[12]. In 1995, Erikssonet al[13] reported the first randomized controlled trial (RCT) and demonstrated that antibiotic treatment in patients with AA was effective. In the following years, many RCTs or prospective interventional studies have been reported (Table 1). One of them was the famous Appendicitis Acuta (APPAC) multicenter randomized trial, which revealed that most patients(72.7%) randomized to antibiotic treatment for computerized tomography (CT)-proven uncomplicated AA did not require appendectomy during the 1-year follow-up period,and 82.9% of the 70 patients randomized to antibiotic treatment who subsequently underwent appendectomy had uncomplicated AA. There were no intra-abdominal abscesses or other major complications associated with delayed appendectomy in patients randomized to antibiotic treatment[14]. Between the second and fifth followup years, relapse only occurred in 16.1% of these patients, and the overall complication(surgical site infections, incisional hernias, abdominal pain, and obstructive symptoms) rate and sick leave were significantly reduced in the antibiotic group compared to the appendectomy group[15]. For pediatric patients with uncomplicated AA, the antibiotic-first strategy also appears to be effective, as the initial treatment success was 94.6%, with less morbidity, fewer disability days, and lower costs than surgery[16]. In pregnant females, although there is no high quantity evidence, some case reports have shown that it may be possible to manage uncomplicated AA nonoperatively[17,18].Systematic reviews and meta-analyses of studies comparing NOM with appendectomy concluded that the majority of patients with uncomplicated AA can be treatedviaan antibiotic-first approach, and it does not statistically increase the perforation rates in either adult or pediatric patients[10,11,19]. Therefore, with success in NOM,initial conservative treatment with antibiotics is preferred by some centers, and appendectomy is performed when NOM fails after 24-48 h, which obviously delays surgery in these patients.
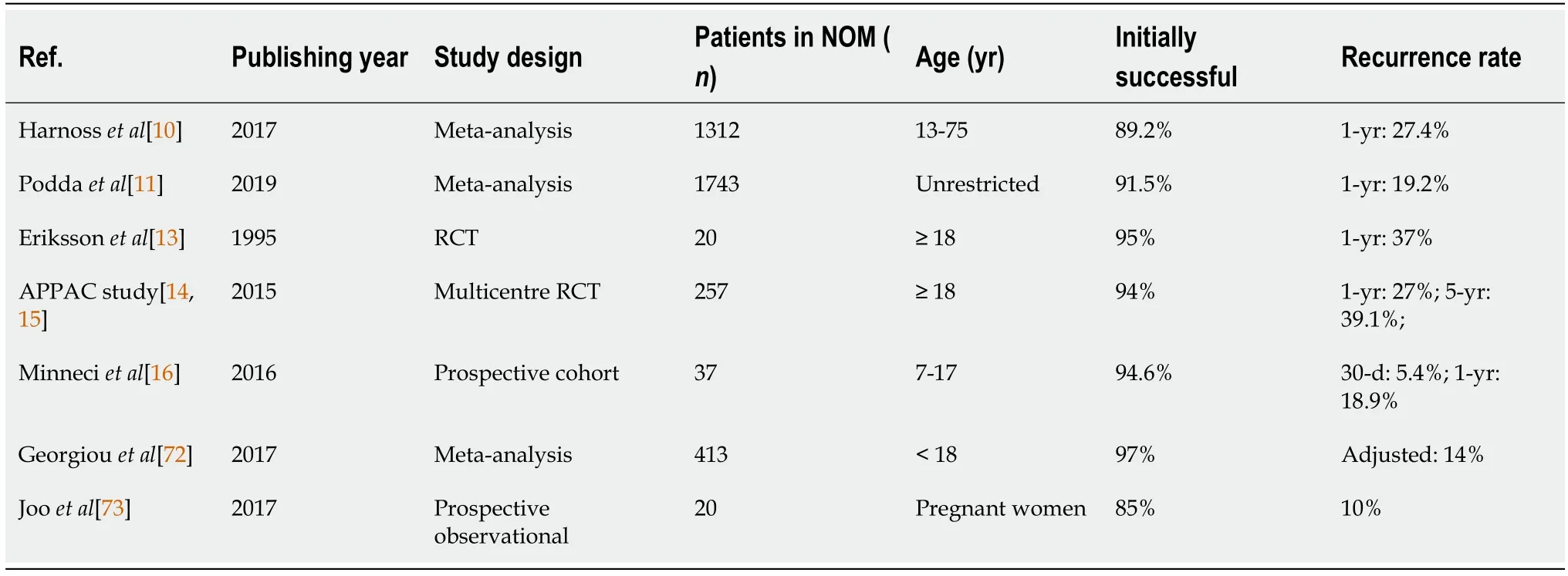
Table 1 Clinical trials and meta-analyses comparing primary antibiotic treatment vs surgery for acute appendicitis
Perforation is independent of in-hospital delay
Under the assumption that untreated appendicitis will eventually progress to perforation, with an associated drastic increase in morbidity and mortality, perforation was considered an indicator to evaluate the quality of the management of patients with suspected AA. At the end of the last century, an analysis of population-based studies showed that the low proportion of perforations was secondary to the detection of a larger number of patients with nonperforated appendicitis but not fewer perforations in surgical units with a radical attitude with wide indications for exploration.Therefore, the application of more extensive indications for exploration is unable to decrease the incidence of perforated appendicitis but leads to the detection of more cases with appendicitis that would otherwise not need surgical treatment[20]. This was supported by a large number of studies with various study designs that did not find an association between perforation and the in-hospital delay (Table 2). When patients were classified according to pathological findings, no differences in time from hospital arrival to surgery were found between patients with uncomplicated appendicitis(inflamed appendix) and complicated appendicitis (gangrenous or perforated)[21].When patients were classified based on categorical time blocks, the differences in the rates of complicated AA between different time blocks were not significant[22,23].Despite these unadjusted data, increased time to appendectomy was not associated with an increased risk of perforation after adjusting for several confounders in adults and children[24-26]. Several studies have analyzed databases with large samples, and the results indicated that time to surgery is not a significant predictor of perforation and complications[27-29]. For example, data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database demonstrated that the outcomes of appendectomy for AA were similar when the operation was performed on hospital day 1 or 2[29].

Table 2 Effects of delaying appendectomy on incidence of complicated appendi citis
Perforation independent of in-hospital delay was also demonstrated by metaanalysis and supported by guideline makers. The first meta-analysis included 11 studies conducted by The United Kingdom Surgical Collaborative and assessed the effect of in-hospital delay on the perforation rate using only unadjusted data. This meta-analysis did not find a difference in perforation rate based on time to operation[24]. A 2018 meta-analysis by van Dijket al[30] also demonstrated that delaying appendectomy does not appear to be a risk factor for complicated AA for up to 24 h after ED presentation by both unadjusted and adjusted data. Recently, the American Pediatric Surgical Association Outcomes and Evidence-Based Practice Committee stated that appendectomy performed within the first 24 h from presentation did not increase the risk of perforation in children[31]. Based on some of this evidence, the 2020 World Society of Emergency Surgery (WSES) guidelines concluded that an inhospital delay of up to 12-24 h is safe in uncomplicated AA patients[32].
These studies mentioned above have an obvious limitation: The severity of AA at ED presentation was not clear; therefore, some perforation may have occurred before hospital arrival, and the results could not explain the effect of in-hospital delay well.To overcome this limitation, apost hocanalysis of the Multicenter Study of the Treatment of Appendicitis in America: Acute, Perforated, and Gangrenous study employed upgrades in the appendicitis category (progression from simple appendicitis diagnosed by CT on admission to any higher grade diagnosed intraoperatively)to evaluate the effect of in-hospital delay on outcomes. The results of this study also showed that the duration from ED triage to appendectomy was not associated with increased rates of upgrades; however, a nonsignificant trend toward a higher grade of appendicitis was found for patients delayed more than 24 h[33]. This was consistent with the results of another single-center retrospective study in which upgrading appendicitis severity was examined[34].
In-hospital delay does not increase postoperative complications
POCs were common in patients following appendectomy, including surgical site infections (SSIs), revisits to the emergency department, leakage, ileus, and bowel obstruction. The majority of studies found that a specific in-hospital delay did not increase the rates of POCs for either children or adults, although the definition of surgery delay varied among these studies (Table 3)[26,31,35,36]. For example, patients from the American College of Surgeons NSQIP dataset did not show an increased risk of POCs between in-hospital delays of < 24 h and 24-48 h[37]. A 16-h delay from ED presentation or a 12-h delay from hospital admission to appendectomy was not associated with an increased risk for SSIs in pediatric patients[36]. In that study, the authors defined delayed surgery as more than 12 h from ED arrival to operation, and there were no significant differences in POCs between delayed cases and nondelayed cases[23]. The meta-analysis by van Dijket al[30] concluded that delaying appendectomy for up to 24 h after admission does not appear to be a risk factor for POCs;however, this was supported by unadjusted data, and no adjusted data were available.

Table 3 Effects of delaying appendectomy on incidence of postoperative complications
Negative appendectomy
Lack of medical resources
With a high estimated nationwide mean cost to hospital systems per patient, the operative management of AA represents a significant cumulative financial burden on the health-care system[40]. Traditionally, to prevent delay in treatment for AA and corresponding perforation, CT, ultrasound, magnetic resonance imaging, and diagnostic laparoscopy have been used liberally, whereas active observation has become less attractive. The increased use of these new diagnostic techniques has led to increased costs, but the effect in decreasing the rates of perforation and negative appendectomy is controversial[41,42]. A study aimed to compare the costs of antibiotics alonevsappendectomy in treating uncomplicated AA within the randomized controlled APPAC trial reported that the overall societal costs in the operative group were 1.6 times higher than those in the antibiotic group[43]. In this study,uncomplicated AA was proven by CT for patients in both the surgery and antibiotic alone groups. However, in clinical practice, if an active observation decision is made for a patient with suspected uncomplicated AA based on clinical presentations, these diagnostic workups are not required, which may decrease the costs further. Therefore,to decrease societal costs, some surgeons support delaying appendectomy until NOM fails.
On the other hand, as the operative volume has increased at most centers, delay in appendectomy resulting from the relative lack of resources, including surgeons and facilities, has become common. Currently, two models are employed to address emergency surgery, including appendectomy. In one model, appendectomy is performed electively by surgeons sporadically covering general surgery calls, while in another model [i.e., the acute care surgery (ACS) model], appendectomy is performed by surgeons specializing in emergency general surgery. Currently, the ACS model hasonly been applied in a minority of countries and hospitals[44]. Treating acute appendicitis as a surgical urgency condition may negatively affect surgeons, other providers, and patients. Emergency appendectomy will interrupt a busy day of elective operations of surgeons, and the therapy of other patients will be delayed or rescheduled. A surgeon taking a call at home may feel obligated to drive to the hospital to perform an emergency appendectomy in the middle of the night, thus requiring mobilization of the anesthesiologist and operating room nursing staff,leading to sleep deprivation of not only the surgeon, but affiliated staff[33].Furthermore, in current practice, not all hospitals have optimal imaging modalities at their disposal, and staff and operating rooms are not always available at night. In addition, some studies have reported that working or operating at night will increase morbidity and error rates[45-47]. Therefore, while both delay in diagnosis and delay in surgeon or operation room availability contributed to in-hospital delay, the second factor contributed most[23,48]. This may explain the finding that delayed patients were more likely to have arrived at the ED during the hours of 4 PM to 12 AM[23].
Atypical clinical presentation
The proportion of patients with perforation was higher in younger and older people,which was explained by the atypical presentation, leading to delay of appendectomy by the patient themselves or surgeons[49,50]. It is very difficult to achieve an accurate diagnosis for AA in children under 6 years of age due to the lower incidence of this disease and its atypical clinical presentation in the younger population[51,52].Younger patients with AA were diagnosed with acute gastroenteritis first because of the banality of this disease in younger children and because vomiting and diarrhea are common concomitant symptoms, while fever, anorexia, and transit alteration were less frequently observed[52-54]. Indeed, an initial misdiagnosis rate ranges from 28% to 57% in children and can reach 100% in those 2 years of age or younger[55]. All of these reasons result in delays (both prehospital and in-hospital) in appendectomy in pediatric patients. Female patients have also been found to be more likely to experience operative delay for appendicitis, which has been attributed to atypical symptoms and further diagnostic workup, such as CT examination[56,57]. Pregnancy may be another reason for delay in females. In a large retrospective series of pregnant women with suspected AA, more than half of patients were delayed for appendectomy for a repeat ultrasound (US) study because the initial US failed to ascertain the diagnosis, which increased the diagnostic yield of the US but did not increase the rate of perforation and affect maternal or fetal safety[58].
Psychosocial factors
All discussions have so far been focused mainly on in-hospital delay, which attracted most attention from clinicians, while the prehospital delay has been overlooked.However, as will be discussed in the following sections, prehospital delay may contribute most of the increased perforated appendicitis. Until now, studies on the causes of prehospital delay have been scarce. A study by our team was carried out to measure the association of a wide range of factors with prehospital delay among adult patients with AA. We found no associations between prehospital delay and economic factors, which can be explained by the popularization of insurance, more convenient transport, and the improvement of living conditions. Seeking medical help for AA is no longer a complicated, expensive, and time-consuming process. Although an uncommon clinical presentation may cause diagnostic delay, as mentioned above, it is not an important factor for patients in deciding whether to see a doctor; therefore, we also found no associations between prehospital delay and clinical presentations except for the severity of pain. We found that delayed ED presentation for AA was significantly associated with psychosocial factors, including living alone, a lack of knowledge of the disease, low social support, an unstable introvert personality trait,negative coping style, and symptoms occurring on a workday[21].
Coronavirus disease 2019 pandemic
Since December 2019, a new pandemic infectious disease,i.e., coronavirus disease 2019(COVID-19), has become a serious healthcare problem that has affected millions of people worldwide[59]. With fear among the population that they would contact the virus from patients with COVID-19, patients are likely to avoid hospitals as much as possible. Panet al[60] observed that 50.5% of patients with COVID-19 reported gastrointestinal symptoms, including lack of appetite, diarrhea, vomiting, and abdominal pain, which may lead to challenges in the diagnosis of AA during the pandemic. In addition, to prevent the transmission of COVID-19, RT-PCR tests and chest CT are conducted for in-hospital patients in some centers, which require laboratory specifications, and the results may take a long time[61,62]. All these changes since the COVID-19 pandemic have led to delayed ED presentation and diagnosis for most common medical conditions, including AA. However, the effects of the COVID-19 pandemic on the delay and outcomes of patients with AA varied across hospitals and countries. Some researchers reported a longer symptom progression time and increased incidence of complicated appendicitis during the COVID-19 lockdown period, which reflects patients’ reluctance to seek medical help even when the disease worsens[63-66]. In contrast, other researchers did not find increased diagnosis delay or worse outcomes in patients with AA during the pandemic lockdown[67,68]. In addition, the decreased admissions for selective surgery reduced the demand for surgical services and may have also contributed to shorter delays to imaging and theatre[66]. It is difficult to contribute the increased perforation proportion to the COVID-19 pandemic. As the number of COVID-19 cases increases,patients present as an emergency with appendicitis decreases, although an increased proportion of complicated AA has been observed, which can be explained not by a delay in seeking medical attention but rather by selection due to undiagnosed resolving appendicitis, consistent with the theory proposed by Andersson[2,69]. The preferred NOM by surgeons in the COVID-19 pandemic may be another explanation[70]. Therefore, the COVID-19 pandemic increased the prehospital delay but did not affect or decrease the in-hospital delay, with the increased proportion of complicated AA contributable to decreased uncomplicated AA and successful NOM[71].
COSTS OF DELAYING APPENDECTOMY
Nonoperative treatment failure and recurrence
In the APPAC randomized trial, AA relapsed in 27.3% of patients and underwent appendectomy within 1 year of initial presentation for AA, and 10% of them experienced complicated AA[14]. The 5-year follow-up results of this randomized trial reported that another 16.1% of these patients experienced relapse and underwent appendectomy between 1 and 5 years. Therefore, the cumulative incidence of appendicitis recurrence was 39.1% at 5 years, with 2.3% of them being diagnosed with complicated AA[15]. Additionally, a meta-analysis reported that the recurrence rate was 14% in pediatric patients with uncomplicated AA receiving antibiotic therapy without appendectomy[72]. A recent meta-analysis conducted by Poddaet al[11]reported that the complication-free treatment success rate was 82.3% for patients allocated to surgical therapy, which was higher than that of patients allocated to antibiotic therapy (67.2%), and the treatment failure rate was 8.5% for the first admission and 19.2% for the 1-year follow-up. The rates of complicated appendicitis with peritonitis identified at the time of surgical operation and surgical complications were equivalent between the two therapy groups[11]. For patients during pregnancy, a single study reported a 15% failure rate in these patients with uncomplicated AA treated conservatively, and the recurrence rate was 12% during the same pregnancy[73]. Therefore, the failure and recurrence rates of NOM are not low (Table 1). The failure of NOM may be attributed to the inability to make an accurate uncomplicated AA diagnosis when including patients and the inability to predict which patient will fail from NOM and will develop recurrence. Although failure and recurrence can be handled safely, these trials only recruited patients with good conditions, which cannot be extrapolated to other patients, such as those with systemic illness.
Perforation
Although the majority of studies reported that there was no association between perforation rates of AA and in-hospital delay, some studies indeed found a positive correlation between perforation rates and in-hospital delay or a much longer duration from presentation to appendectomy (Table 2). A large multi-institutional study from Sweden and a single-center study from Italy reported an increase in perforation when the time from admission to surgery was longer than 12 h[74,75]. After adjusting for potential confounders, Meltzeret al[76] found a 2% increase in the odds of perforation every hour increase in the time from ED triage to incision. Papandriaet al[77] utilized the Nationwide Inpatient Sample (NIS) and Kids’ Inpatient Database to examine perforation rates based on the surgery day from admission and found an increased risk of perforation beginning on hospital day 2 for adults and day 3 for children.Therefore, contrary to WSES, the European Association for Endoscopic Surgery stated that delaying an appendectomy increases the risk of perforated AA and therefore recommended that appendectomy be performed as soon as possible[78].
In contrast to the increasing interest in the effects of in-hospital delay on the outcomes of appendectomy, prehospital delay has been neglected by professionals.Even though perforation only occurs in specific patients and others will never progress to severe disease, perforation is a time-dependent event, and there is a direct association between the time from symptom onset to surgery and findings of perforation intraoperatively (Table 2)[79-81]. Indeed, after 36 h of symptom onset, the risk of perforation increases by 5% every 12 h[82]. When compared to 60-72 h after the onset of symptoms, a significant increase in the likelihood of perforated AA occurred after 72 h in the cohort reported by Elnielet al[80]. The only meta-analysis currently available to evaluate the effects of prehospital delay and total delay on rates of perforation was conducted by our team. Although unadjusted data were used, the results showed that the rates of complicated appendicitis were associated with the duration from symptom onset to presentation or operation[83]. These studies suggested that the main factor associated with perforated appendicitis is prehospital delay, and the effects of in-hospital delay may be masked by selection biases.
Edward s heart soared with joy as he spent the next month trying to make the cabin into a home. At last, the day he had been waiting for his whole life arrived. With a bouquet5 of fresh-picked daisies in hand, he left for the train depot(,). Steam billowed and wheels screeched6 as the train crawled to a stop.
Postoperative complications
Consistent with perforation, some studies have reported that delayed appendectomy will lead to more POCs, with significant differences in different time blocks (Table 3).Some studies found an increase in POCs if appendectomy was delayed by 24 h, while other studies demonstrated differences in the incidence of POCs when surgery was performed greater than 48 h after admission[37,84]. One of these studies analyzed over 600000 pediatric and adult AA patients and reported that the incidence of operative drainage and bowel resections was higher in patients undergoing appendectomy greater than 1 d after admission[84]. Another study analyzed 69926 patients with AA and reported that a delay of more than 48 h was associated with a two-fold increase in the risk of POCs[37]. Data from the American College of Surgeons NSQIP demonstrated that appendectomies performed on hospital day 3 had significantly worse outcomes, with increased 30-d mortality (0.6%) and all major POCs (8%),especially for patients with decreased baseline physical status[29]. Moreover, an increase in SSIs was observed when a shorter interval (6 h) was used as the cutoff to define early and delayed appendectomy in one retrospective study[85]. Although there are few studies on the association between prehospital or total delay and POCs following appendectomy, the majority of them reported a positive association in both pediatric and adult patients[22,36]. In addition, regarding complicated AA, some authors delayed appendectomy after initial antibiotic treatment. However, a population-level study with a 1-year follow-up period found that late appendectomy led to more POCs than early appendectomy[86].
Increased hospital costs and other resource utilization
Although no difference in LOS was found when comparing surgery delay intervals between ≤ 10 h and > 10 h, studies identified increased LOS associated with time from admission to appendectomy more than 18 h or 24 h[87,88]. One study using NIS data suggested that the LOS and hospital costs were increased for patients undergoing appendectomy the morning after admission or on a weekday[89]. In children, it has been demonstrated that delay of appendectomy is associated with increased hospital charges[90,91]. In adults, Aikenet al[23] used actual hospital cost data as calculated by cost-accounting algorithms that account for the supplies, labor, equipment, and facilities associated with each admission and procedure, which better reflects the cost to the hospital system than most surrogates, such as charges, cost-to-charge ratios, or reimbursements, to examine the effect of delayed appendectomy on resource utilization among adults undergoing nonelective laparoscopic appendectomy for AA.The authors reported that delayed appendectomy is associated with an increased LOS and increased total hospital costs compared with appendectomy within 12 h of presentation[23]. As no differences in postoperative LOS were found in these studies,preoperative delay alone may account for the increased costs. Longer preoperative delay was reflected in all cost categories but may be especially evident in direct variable cost and indirect fixed cost, resulting from the increased use of medications or consumables and LOS-associated facility costs in the hospital, respectively[23,90,91].
Dissatisfaction of patients
There have been limited studies addressing the relationship between the delay of appendectomy and patient satisfaction. One single-center study in England by Sidesoet al[92] surveyed 42 consecutive adult patients undergoing appendectomy for uncomplicated AA. In their practice model, appendectomy in patients who present after 10 PM will be delayed to the next morning. The survey results demonstrated that more than half (57%) of patients preferred an operation sooner after admission rather than delaying to the next morning, and all of these patients had poor sleep before the procedure[92].
APPRAISAL OF CURRENT STUDIES ON DELAYED APPENDECTOMY
Although extensive studies have been conducted on delay of appendectomy,regardless of whether their results support or against delay, only association but not causality can be proven. In addition, as mentioned above, not all enrolled subjects in these studies have confirmed the severity of disease. Therefore, it is unclear how many patients with AA have already progressed to complicated appendicitis upon arrival at the hospital. As complicated AAs are more likely among clinically ill patients and are more likely to be operated on earlier, this selection bias will mask the risk of developing perforated AAs in the group with uncomplicated AAs. In contrast to other authors who did not find an association or found a positive association between perforation and in-hospital delay, Beecheret al[93] found that perforation was associated with earlier operations. In addition, Almströmet al[26] analyzed the effect of inhospital delay in pediatric patients and found that timely operation (within 12 h) was associated with an increased hospital LOS. This contradiction may be attributed to patients presenting with perforated AA being taken to the operating room more expeditiously, which may negate any observable difference in perforation rates associated with increased time to appendectomy[26].
As mentioned above, most studies focused on in-hospital delay, and the prehospital delay of these patients was not clear. Although some cases of AA will never progress to perforation, the patients only experience perforation at some time point after the onset of symptoms but do not begin with a perforated AA. Due to the distribution differences in prehospital delay and AA patients with different fates, the results of these reported studies differed. Except for surgery delay, there are many risk factors for perforation, such as age, sex, antibiotic initiation, and genetic background;however, most studies did not adjust for confounders. Another reason for the inconsistent conclusions across studies is the various time intervals (from 6 h to 24 h)and various event points (ED arrival or admission) utilized to define surgery delay.Selection bias will result in different proportions of uncomplicated AAs, which also accounts for the inconsistent conclusions across studies.
HOW TO BALANCE THE POSITIVE AND NEGATIVE EFFECTS OF DELAYED APPENDECTOMY
Ascertaining causality between delay and outcomes
If surgery delay causally leads to perforation, it is not useful to determine how long it is safe for appendectomy to delay, and we just need to perform the operation as sooner as possible. To safely delay an appendectomy, we should ascertain that the delay will not lead to negative outcomes. As mentioned above, causality between delay and severity of AA cannot be found because of the limitations of currently available studies. To truly prove that an in-hospital delay is the reason for upgrading from simple to complicated appendicitis, the enrolled patients should be diagnosed with unambiguously simple AA and randomized to appendectomy at varying intervals of in-hospital delay. Currently, such a trial is lacking, and the highest quality evidence is observational data with contemporaneous controls and accounting for all known confounders. Zhanget al[94] planned to conduct a randomized, controlled trial across two academic institutions with blinded outcome assessors to examine whether delaying appendectomy until the following morningvsearly appendectomy overnight affects the rate of POCs in adult patients diagnosed with AA in the evening hours.This RCT will balance the selection bias and provide high-level evidence, and the results of this study are eagerly awaited.
Diagnosing AA precisely
Traditionally, the diagnosis of AA is mainly based on clinical presentations, which leads to higher rates of negative appendectomy. Clinical scoring systems,e.g., the Alvarado score, Appendicitis Inflammatory Response score, the new Adult Appendicitis Score, and Samuel’s Pediatric Appendicitis Score, can be used to identify low-risk patients, optimize the utility of diagnostic imaging, and decrease negative surgical explorations. The sensitivity and specificity of clinical scores varied among score systems and patient cohorts, and a tailored individualized clinical scoring system should be verified to stratify the risk and disease probability[32].Although the white blood cell (WBC) count, neutrophil percentage, and urinalysis are routinely utilized in auxiliary diagnosis or differential diagnosis for AA, other markers, such as C-reactive protein (CRP), bilirubin, granulocyte colony-stimulating factor, fibrinogen,interleukin, and procalcitonin (PCT), have been investigated[95]. Currently, although there is no unique biochemical marker that would be highly diagnostic of AA if positive, a combination of clinical presentations, laboratory biochemical markers, and imaging may significantly improve diagnostic sensitivity and specificity and eventually replace the need for CT in both adults and children[96]. However, due to the high rate of preoperative CT imaging, only 2% of patients underwent a negative appendectomy in the study by Abdul Jawadet al[33]. In another study from the United Kingdom, the authors reported an overall 10% negative appendectomy before the COVID-19 pandemic rate, resulting from the diagnosis of AA relying heavily on clinical examination. However, during the pandemic, more CT imaging resulted in more rapid confirmation of disease, shorter time to theatre and subsequently reduced length of stay, and higher positive appendectomy rates[66,71]. Therefore, along with the development of diagnostic workups, the accuracy of diagnosis has increased gradually, and the diagnostic delay will be reduced as short as possible.
Correct severity grading of AA at presentation
As mentioned above, a safely delayed appendectomy was concentrated on patients with uncomplicated AA. Undoubtedly, patients with diffuse peritonitis or abscess will be diagnosed with complicated AA. However, unfortunately, regarding diagnosis,there is also no ideal approach to stratify the severity of AA in all patients. Traditionally, temperature, abdominal signs, CRP, and the presence of free fluids on imaging are the most commonly used parameters to identify “high-risk” patients for complicated AA, but no single parameter can achieve good performance. Some new biochemical markers have been evaluated in recent years. In a recent meta-analysis,PCT was confirmed to be a more accurate biomarker in diagnosing complicated AA,with a pooled sensitivity of 0.89, specificity of 0.90, and diagnostic odds ratio of 76.73[97]. Recently, ischemia-modified albumin (IMA) levels have been used to predict the severity of AA. Kılıçet al[98] found that there were significant differences in CT findings and IMA levels between AA patients with and without perforation, and a strong positive correlation between IMA levels and CT findings was also found.Imaging has become standard in the diagnosis and evaluation of AA, with CT being the most accurate test. Both CT and ultrasound have been reported to be able to discriminate uncomplicated from complicated appendicitis, with a high specificity but low sensitivity[99]. Therefore, a prediction model based on scoring systems and clinical and imaging features was established,and 95%of the patients deemed to have uncomplicated AA were correctly identified[99].
Predicting disease progression of AA
Currently, the way to improve the success rate of the nonoperative approach and to reduce the rates of perforation and negative appendectomy is mainly based on correct selection of patients with uncomplicated AA. In addition, identifying patients with uncomplicated AA who will progress to perforation may be another feasible strategy.However, predicting the progression of AA has proven to be a challenge. In the study conducted by Hanssonet al[100], the selection criteria for patients who may benefit from antibiotic therapy as the first-line treatment were as follows: CRP < 60 g/L, WBC< 12 × 109/L, and age < 60 years. Patients with assumed appendicitis who fulfilled all criteria had an 89% probability of having phlegmonous appendicitis. The independent predictors of NOM success in another recent study included a longer duration of symptoms prior to admission (> 24 h), lower temperature, imaging-confirmed uncomplicated AA with a lower modified Alvarado score (< 4), and smaller appendiceal diameter[101]. The presence of an appendicolith has been identified as an independent prognostic risk factor for perforation and treatment failure in NOM of uncomplicated AA[102-104]. Two studies have found that patients with older age and poor physiological conditions are more likely to experience severity upgrades[33,74].Younger children are another age group with a significantly increased incidence of perforation. A recent study showed that the incidence was 100% for children younger than 2 years,83.3%for 2-3 years,71.4%for 3-4 years,78.6%for 4-5 years,and 47.3%for 5 years[105]. High perforation rates in younger children are associated with the fragility of the appendicular wall and with the relative immaturity of the large omentum[106]. Therefore, in patients with the characteristics described above, NOM or surgery delay should be employed cautiously.
Improving utilization of medical resources
One lesson that we learned from the changes in management of AA during the COVID-19 pandemic in some centers was that reduced demand for surgical services for elective surgery contributed to shorter delays to diagnostic workup and appendectomy. Furthermore, the mandated presence of a senior surgeon in operations performed during the pandemic not only contributed to a shorter operative time but also decreased the incidence of POCs[66]. This observation highlights the importance of improving the utilization of medical resources to shorten the appendectomy delay and improve outcomes. Actually, long before the COVID-19 pandemic, some strategies have been applied to improve the utilization of medical resources. One of them is the ACS model, which has been implemented in some countries and regions,with varied structures among them[44]. In a meta-analysis published in 2020, the authors included 16 studies on the ACS model in the management of AA, mainly carried out in North America and Australia. The results showed that following ACS introduction, the POCs were significantly reduced following appendectomy. There was a significant reduction in the time from ED arrival until admission and from admission to operation. LOS was reduced, and no statistical significance was detected for conversion of laparoscopy to open technique or rate of negative appendectomy[107]. Although there were insufficient data for cost analysis for appendectomy in this meta-analysis, we can infer that reduced total social costs will be achieved by these improvements within the ACS model.
Laparoscopic appendectomy
Open appendectomy (OA) has been the standard treatment for AA since it was first performed in 1894, usually with a longer LOS and more readmission for intestinal obstruction and postoperative adhesion. Laparoscopic appendectomy (LA) was first performed in 1983 and has been used for more than three decades[108]. Many studies with different designs have been conducted to compare the advantages between OA and LA. In conclusion, LA is often associated with longer operative times and higher operative costs, but it leads to less postoperative pain and POCs, shorter LOS, and earlier return to work and physical activity, leading to lower overall hospital and social costs[109,110]. Another possible advantage of LA is that the exploration can be applied for the entire abdominal cavity, leading to the identification of other emergency conditions and associated surgical treatment. Although other diseases were reported to be found both in LA and OA, no studies have compared the rates of negative appendectomy and the exploration results between two surgical strategies,and whether LA can decrease the mortality after negative appendectomy, which was reported to be high mainly during the period in which OA was performed, is uncertain. Therefore, although with equipment and technical limitations, LA is recommended as the preferred approach over OA for AA, where laparoscopic equipment and expertise are available.
Early presentation
An epidemiological study reported that the incidence of unperforated AA declined from 1970 to 1995; however, since then, the introduction of CT and laparoscopic appendectomy has led to an increased incidence of unperforated AA. Nonetheless, the number of cases of perforated AA increased slowly over time[6]. These results suggest that improvements in the diagnosis and treatment of AA only increased the detection rates of AA and decreased the negative appendectomy rate, with no help in decreasing the risk of perforation. On the other hand, perforation still results from delay before presentation and cannot be settled by modern in-hospital medicine. The results of the study from our team suggested that the prehospital delay is not determined by the disease and associated level of care but by psychosocial factors[21]. Therefore,promoting the early presentation of patients with AA mainly relies on psychosocial strategies rather than medical strategies. However, no studies have been conducted with such an aim. We believe that an effective campaign, such as to spread the scientific knowledge of AA and improve social support in populations, will promote the hospital visits of patients when symptoms are noticed and decrease the duration of symptoms before appendectomy and associated adverse effects.
CONCLUSION
Appendicitis continues to be the most common cause of ED visits because of its high prevalence worldwide. From the onset of symptoms to appendectomy, many factors can cause delays in surgical intervention. Some are inevitable, such as ascertaining the diagnosis, preoperative evaluation, and physician-patient communication, and some can be modified and improved, such as a lack of medical resources and psychosocial factors that hinder patients from seeking medical advises. Extensive studies have been carried out to explore the association between delaying appendectomy and its positive or negative effects, but there has been no conclusive answer to the question of acceptable in-hospital delay so far because of their inherent limitations. In addition,although spontaneous resolution and effectiveness of NOM have been documented to be common in patients with uncomplicated AA, accurate diagnosis and severity grading continue to remain a challenge. Therefore, in order to shorten the waiting time before appendectomy and to improve the prognosis of AA, it is important to ascertain the causality between delayed and complicated AA and associated adverse effects and to develop new biomarkers and advanced imaging technology. This will help facilitate the diagnosis and severity grading, to improve the utilization of medical resources,reduce medical costs, and develop and popularize advantageous therapy strategies,such as more effective NOM, LA, natural orifice transluminal surgery, and endoluminal surgery (Figure 3).
ACKNOWLEDGEMENTS
The author thanks the Health Commission of Mianyang City and the Science and Education Department of the Third Hospital of Mianyang for their support. Electronic search of PubMed was performed from its initiation until March, 2021. The following search strategy was followed: (appendicitis OR appendectomy OR appendicectomy)AND (early OR delay* OR tim* OR rupture* OR perforat*). The selection of original publications was based only on the author’s judgement. The space limitations of this review have unfortunately meant that I have not been able to separately cite many of the original publications that have contributed substantially to the literature. I sincerely apologize to the authors of these publications.
 World Journal of Clinical Cases2021年20期
World Journal of Clinical Cases2021年20期
- World Journal of Clinical Cases的其它文章
- Obesity in people with diabetes in COVID-19 times: Important considerations and precautions to be taken
- Detection of short stature homeobox 2 and RAS-associated domain family 1 subtype A DNA methylation in interventional pulmonology
- Borderline resectable pancreatic cancer and vascular resections in the era of neoadjuvant therapy
- Esophageal manifestation in patients with scleroderma
- Exploration of transmission chain and prevention of the recurrence of coronavirus disease 2019 in Heilongjiang Province due to inhospital transmission
- Effects of nursing care in fast-track surgery on postoperative pain,psychological state, and patient satisfaction with nursing for glioma