
Resting energy expenditure in cirrhotic patients with and without hepatocellular carcinoma
2021-07-01 02:28AnaCristhinaHenzClaudioAugustoMarroniDaniellaMirandadaSilvaJoiseMunariTeixeiraThiagoThomSilveiraShaianeFerreiraAndresaThomSilveiraNataliaPerinSchmidtJessicaTainaSteinRobertaGoulartRaynSabrinaAlvesFernandes
Ana Cristhina Henz,Claudio Augusto Marroni,Daniella Miranda da Silva,Joise Munari Teixeira,Thiago Thomé Silveira,Shaiane Ferreira,Andresa Thomé Silveira,Natalia Perin Schmidt,Jessica Taina Stein,Roberta Goulart Rayn,Sabrina Alves Fernandes
Ana Cristhina Henz,Sabrina Alves Fernandes,Department of Nutrition,Centro Universitário Metodista (IPA),Porto Alegre 90420-060,RS,Brazil
Claudio Augusto Marroni,Department of Gastroenterology and Hepatology,Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA),Porto Alegre 91760470,RS,Brazil
Daniella Miranda da Silva,Postgraduate Program in Hepatology,Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA),Porto Alegre 90050170,RS,Brazil
Joise Munari Teixeira,Postgraduate Program in Medicine,Hepatology,Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA),Porto Alegre 90050170,RS,Brazil
Thiago Thomé Silveira,Shaiane Ferreira,Andresa Thomé Silveira,Natalia Perin Schmidt,Jessica Taina Stein,Roberta Goulart Rayn,Hepatology Graduate Program,Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA),Porto Alegre 90050170,RS,Brazil
Abstract BACKGROUND The diagnosis of malnutrition in patients with independent hepatocellular carcinoma (HCC) varies from 20% to 50%,is related to important complications and has a direct impact on the prognosis.Determination of the resting energy expenditure (REE) has become an important parameter in this population,as it allows therapeutic adjustments to recover their nutritional status.The REE in cirrhosis,with and without HCC,is not clearly defined,and requires the identification and definition of the best nutritional approach.AIM To evaluate the REE of patients with cirrhosis,with and without HCC.METHODS This is a prospective observational study evaluating the REE of 118 patients,33 with cirrhosis and hepatocellular carcinoma and a control group of 85 patients with cirrhosis without HCC,using indirect calorimetry (IC),bioimpedance,and predictive formulas.RESULTS The REE determined by IC in cirrhotic patients with HCC was 1643 ± 364 and in those without HCC was 1526 ± 277 (P =0.064).The REE value as assessed by bioimpedance was 1529 ± 501 for those with HCC and 1660 ± 385 for those without HCC (P =0.136).When comparing the values of REE determined by IC and predictive formulas in cirrhotics with HCC,it was observed that only the formulas of the Food and Agriculture Organization (FAO)/World Health Organization (WHO) (1985) and Cunningham (1980) presented values similar to those determined by IC.When comparing the REE values determined by IC and predictive formulas in cirrhotics without HCC,it was observed that the formulas of Schofield (1985),FAO/WHO (1985),WHO (2000),Institute of Medicine (IOM) (2005) and Katch and McArdie (1996) presented values similar to those determined by IC.CONCLUSION The FAO/WHO formula (1985) could be used for cirrhotic patients with or without HCC;as it is the one with the values closest to those obtained by IC in these cirrhotic patients.
Key Words: Carcinoma;Hepatocellular;Liver cirrhosis;Calorimetry;Indirect;Rest energy expenditure
INTRODUCTION
The main causes of liver cirrhosis worldwide are alcoholic liver disease and chronic hepatitis B virus and/or hepatitis C virus infections.Over a period of 15 to 30 years,chronic liver diseases can lead to liver cirrhosis and its complications.The prognosis is highly variable and influenced by several factors,such as etiology,severity of liver disease,presence of complications and comorbidities[1].
The prevalence of sarcopenia in patients with hepatocellular carcinoma (HCC) varies from 27.5%[2]to 78.2%[3]and malnutrition affects 20% to 50% of patients with cirrhosis,and both are related to important complications and have a direct impact on prognosis.
Early nutritional diagnosis has significant relevance in cirrhotics,as it reflects positively on their recovery,enables specific therapeutic interventions and prevents the appearance of complications[4-8].
Daily intake should be sufficient to meet the body's demands[9]and can be measured directly or indirectly[10].Resting energy expenditure (REE) is the energy needed to maintain physiological processes;during indirect measurement,an interval of 4 h is necessary since the last meal,and a rest of 30 min before the examination[11].
Indirect calorimetry (IC) is the gold standard for measuring REE[11-13],it is noninvasive and safe,it uses the calorimeter to measure REE through gas exchange and,in a formula,using the Weir Equation (QR=0.83) evaluates the volume of oxygen consumed,the volume of carbon dioxide produced and the nitrogen excreted,since each calorie consumed requires a certain amount of oxygen to be converted into energy,which are good predictors of REE changes[14].
Other methods,such as electrical bioimpedance (BIA) and predictive formulas,commonly used in clinical practice,can also be used to predict REE.
The aim of this study is to evaluate the REE of patients with cirrhosis,with and without HCC,measured by IC and to compare the results with those obtained by BIA and predictive formulas,in order to identify which is the best method of evaluation[15].
MATERIALS AND METHODS
The study included 118 patients,aged ≥ 18 years,of both sexes,divided into two groups.One group consisted of 33 patients with cirrhosis and HCC and a control group of 85 patients with cirrhosis but without HCC,who attended the Department of Gastroenterology and Liver Transplantation of Irmandade da Santa Casa de Misericórdia de Porto Alegre,RS,Brazil,from March 2017 to August 2018.
Hospitalized cirrhotics or those participating in dietary or physical activity programs for weight gain,and/or in a rehabilitation program were excluded;patients with neoplasms other than HCC and those who did not have physical and motor conditions for anthropometric and functional evaluation were also excluded.
All participants agreed to participate in the research by reading and signing the informed consent form.This research protocol was approved by the Research Ethics Committee of Irmandade Santa Casa de Misericórdia de Porto Alegre (number 2387800).
Data from the electronic medical records of the patients,related to the diagnosis,staging by the Child-Pugh score,age and sex of the participants were collected.The diagnosis of cirrhosis and/or HCC was made by clinical,laboratory,imaging and/or,eventually,liver biopsy.The classification of patients with HCC was carried out using the Barcelona Clinic Liver Cancer Group (BCLC) staging system[16].
Current body weight was measured using a Filizola® anthropometric scale with 0.1 kg precision,previously calibrated.Height was measured with a stadiometer fixed to the wall,with the patient in an upright position and barefoot.Body mass index (BMI) was calculated by dividing the weight by height squared {BMI=Weight (kg)/[Height (cm)]2} and classification according to the Food and Agriculture Organization (FAO)/World Health Organization (WHO)[17].
The IC was measured by the Korr® MetaCheck calorimeter,with the patient fasting for 4 h and resting for 30 min before starting the assessment.The measurement was made under conditions of absolute rest for 10 to 30 min,with the patient sitting and using a rigid breathing mask,in a stable condition,and the calculation of energy expenditure was based on the consumption of O2(VO2),CO2production (VCO2) and urinary urea nitrogen,using the formula REE={[3.9 (VO2)] + [1.1 (VCO2)]},described by WEIR,1949[18,19].
The BIA evaluation used the Biodynamics device model 450,with an electric current intensity of 800 µA,frequency of 50 kHz and disposable electrodes of the HeartBeat® brand.The patient was in the dorsal decubitus,comfortable and relaxed position,without shoes,socks,watch,bracelets and necklaces,with legs spread,hands open and supported on the stretcher.A distal electrode was placed at the base of the middle toe of the right foot and the proximal electrode just above the line of the right ankle joint,between the medial and lateral malleolus.Another set of electrodes were also placed,the distal electrode at the base of the middle finger of the right hand and the proximal electrode just above the line of the right wrist joint,coinciding with the styloid process[20].
The predictive formulas for calculating the energy expenditure used in this study are listed in Table 1[21-27].
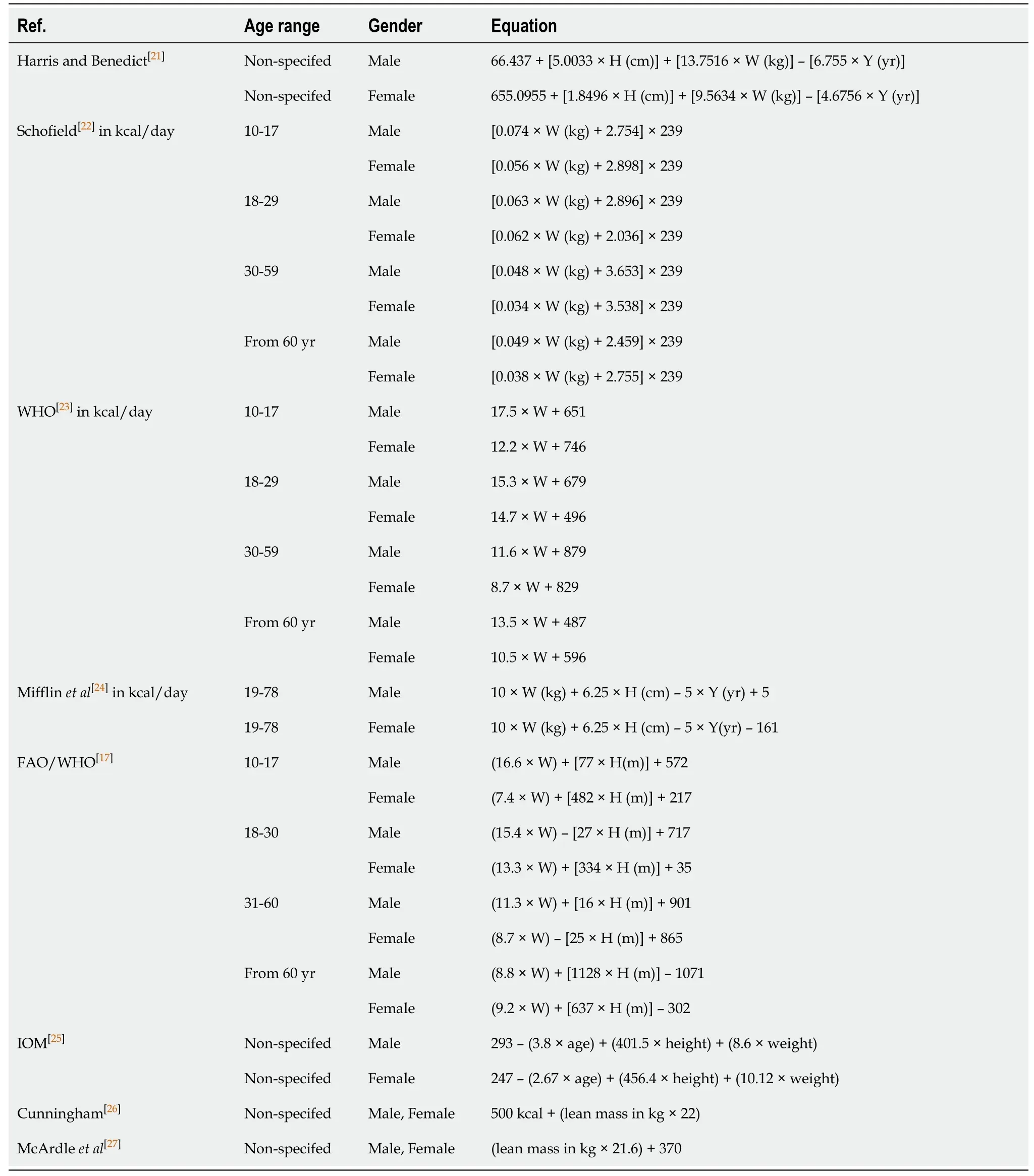
Table 1 Predictive formulas for calculating energy expenditure[8]
Sample size calculation
The sample size for patients with HCC was by convenience sample,and the sample from the control group with cirrhosis was based on the study by Teramotoet al[28],comparing the measured and predicted energy expenditure in patients with liver cirrhosis,considering an 80% power and significance level of 5%,thus obtaining the sample number of 85 patients.
Statistical analysis
Quantitative variables were described by mean and standard deviation and categorical variables by absolute and relative frequencies.
To compare means between genders,the Studentt-test for independent samples was applied.Population estimates were performed using the 95% confidence interval.
To compare groups,the Studentt-test for independent samples (quantitative variables) and Pearson's Chi-square (categorical variables) were applied.
To compare means between the estimated energy expenditure formulas with indirect calorimetry,the Studentt-test for paired samples was used.
To assess the association between anthropometric variables and indirect calorimetry,Pearson's correlation coefficient was used.
The level of significance adopted was 5% (P<0.05) and the analyses were performed using the Statistical Package for Social Sciences 21.0 software for Windows.
RESULTS
The mean age of cirrhotic patients with HCC was 62.8 ± 8.1 years and in those without HCC was 56.7 ± 9.4 years (P=0.001);78.8% of those with HCC were male and 56.5% of those without HCC were female (P=0.001).The clinical characterization of cirrhotic patients was performed using the Child-Pugh score,which identified similarities between the two groups (P=0.224).According to the BCLC staging in our study,most patients with HCC were classified as 0,A and B,as shown on Table 2.
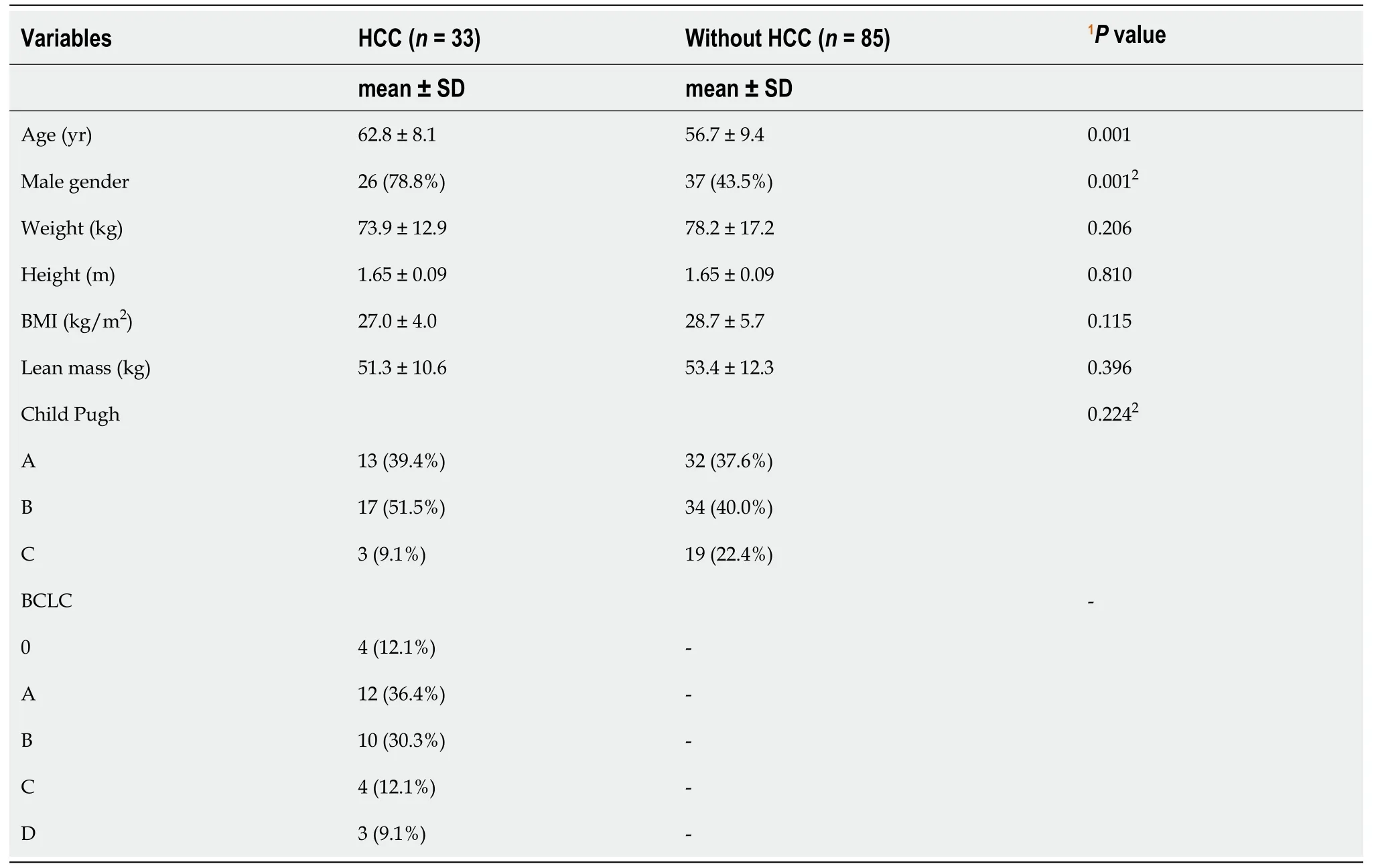
Table 2 Sample characterization - cirrhotics with and without hepatocellular carcinoma (n =118)
The REE determined by IC in cirrhotics with HCC was 1643 ± 364 and in those without HCC was 1526 ± 277 (P=0.064),as shown on Table 3.

Table 3 Energy expenditure at rest by indirect calorimetry in cirrhotics with and without hepatocellular carcinoma (n =118)
The REE value assessed by BIA was 1529 ± 501 for those with HCC and was 1660 ± 385 for those without HCC (P=0.136).In the comparison between the REE determined by the IC,the group with HCC did not show a significant difference and the group without HCC did show a significant difference (P=0.001),as shown on Table 4.

Table 4 Resting energy expenditure by electrical bioimpedance in cirrhotics with and without hepatocellular carcinoma,compared with indirect calorimetry (n =118)
The estimated REE values of cirrhotics with and without HCC,using the predictive formulas of Harris and Benedict[21],Schofield[22],WHO[23],Mifflinet al[24],FAO/WHO[17],IOM[25],Cunningham[26]and McArdleet al[27]showed that only the Harris and Benedict[21]formula (P<0.001) and the IOM formula[25](P=0.001) demonstrated a difference between the two groups,as shown on Table 5.
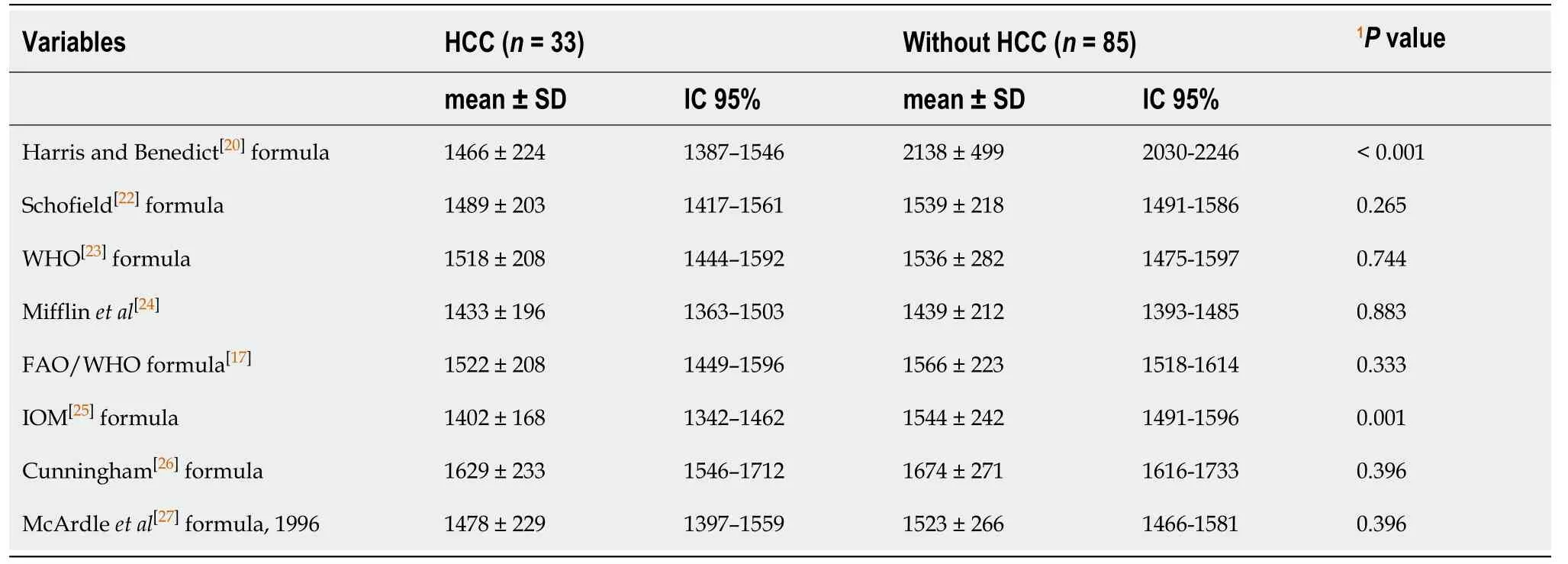
Table 5 Resting energy expenditure calculated using predictive formulas in cirrhotics with and without hepatocellular carcinoma (n =118)
When comparing the REE values determined by the IC and the predictive formulas in cirrhotics with HCC,it was observed that only the formulas of the FAO/WHO[17]and Cunningham[26]presented values similar to those determined by the IC,the others underestimated these values,as shown on Table 6.
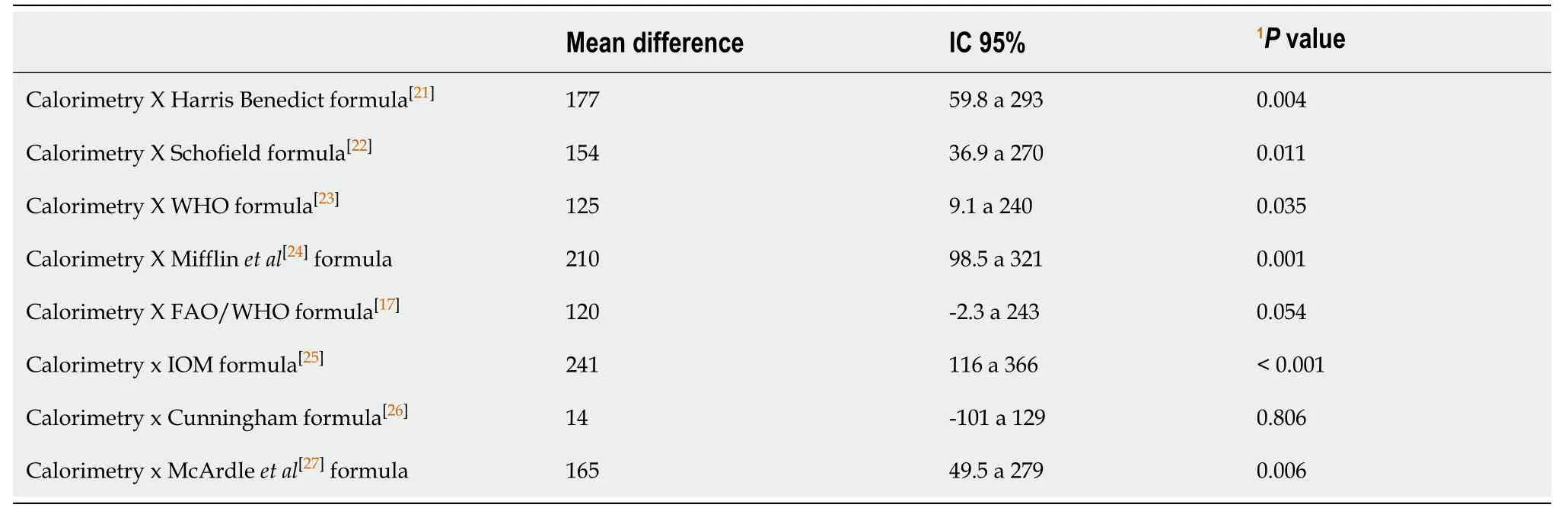
Table 6 Differences between resting energy expenditure calculated using predictive formulas in cirrhotic patients with hepatocellular carcinoma,compared with indirect calorimetry (n =118)
When comparing the REE values determined by the IC and the predictive formulas in cirrhotics without HCC,it was observed that the formulas of Schofield[22],WHO[23],FAO/WHO[17],IOM[25]and McArdleet al[27]presented similar but erratic values to those determined by the CI,as shown on Table 7.
DISCUSSION
Cirrhotic patients have an imbalance in energy metabolism,which contributes to protein-calorie malnutrition and a worse prognosis[5,27-32].When HCC is associated with cirrhosis,clinical conditions and additional needs may worsen such as dietary restrictions.To date,there is no established standard and significant evidence to justify increased REE in these patients.Several studies,with different methodologies,such as IC,BIA and predictive formulas,have evaluated REE in cirrhotics with and without HCC[13,14,27,30,33-36].
In the present study,118 cirrhotic patients were evaluated,33 with HCC (62.8 ± 8.1 years and 78.8% male),and 85 without HCC (56.7 ± 9.4 years and 56.5% female) (P=0.001) which is in accordance with the findings of the literature,where more older men present with HCC[30,32,37,38].
Anthropometry showed that the BMI in those with HCC was 27 kg/m2(± 4.0) similar to that of the control group,and in cirrhotics without HCC,BMI was 28.7 kg/m2(± 5.7).We identified a low prevalence of malnutrition,with overweight,but we must consider that the BMI underestimates the prevalence of malnutrition in cirrhotic patients,as body weight can represent significant changes due to frequent hydroelectrolytic disorders (edema and ascites),and these findings are concordant with previous studies carried out in cirrhotic[23,39-41]and cancer patients[42,43].These results are also in line with studies carried out in cirrhotic patients,with and without HCC[14,30,31,34,37].A publication by Fernandeset al[31],did not identify BMI as a safe method of assessing nutritional status in this population,due to inherent changes in body weight.
Considered as the gold standard for measuring REE,IC is a safe and non-invasive method,capable of determining nutritional needs through gas exchange[11,44,45].
In our study,the average REE calculated by IC in cirrhotic patients with HCC was 1643 ± 364 calories and that of cirrhotics without HCC was 1526 ± 277 calories (P=0.064).These results are similar to those found by Segadilhaet al[45],where REE was 1568 ± 374 calories in a population of 97 elderly cirrhotic patients hospitalized in Rio de Janeiro,and similar to those found by Pintoet al[44],of 1534 ± 300 calories,who studied a population of 45 cirrhotic patients listed for liver transplantation,which corroborates the expectation of correct caloric prediction by the method used[44].
Our REE findings,determined by BIA,in cirrhotics with HCC were 1529 ± 501 calories and 1660 ± 385 calories in those without HCC (P=0.136).These values differ from those of Pintoet al[44],in their study with 53 cirrhotic patients with HCC in the liver pre-transplant,who found the average REE calculated by the BIA was 1817 calories,while that calculated by IC was 1651 calories,similar to our findings.
When comparing the REE determined by BIA with the IC value,we found that the group with HCC did not show a significant difference (P=0.136),and the group without HCC did show a significant difference (P=0.001).
Table 1 shows the predictive formulas used to calculate the REE,with their peculiarities.
Table 6 shows the estimated REE values in cirrhotics with and without HCC,and it can be seen that,with the exception of the Harris Benedict (1919)[22]and IOM (2005)[25]formulas,which show significant differences between the two groups (P<0.001),the others show similar values.
A comparison of the REE data from the IC with those estimated by the predictive formulas,in relation to cirrhotics with HCC,shows that only the FAO/WHO[17](P=0.054) and Cunningham[26](P=0.806) formulas have similarity,and the other six were different (P<0.05);in cirrhotics without HCC the inverse was noted,where five values were similar (P>0.05) and three were different (P<0.05).These findings prevent the determination of a uniform rule.The disparities in our data are consistent with numerous findings in the literature that demonstrate different values for the various methods[14,28,34-36,46].
The applicability of predictive formulas,even with their practicality and low cost,is controversial because they are very erratic,and underestimate or overestimate the REE[35,23],and are thus unreliable.
Our results suggest that the predictive formulas do not provide precise REE values because when using the body weight of cirrhotics,they may incur an intrinsic error,due to water retention (ascites and edema) that directly affects the calculation of REE[38,39].
Studies on other diseases,such as that by Zanellaet al[11],who compared the calculation of REE by IC with predictive formulas and BIA,in patients with pulmonary hypertension,showed that IC obtained values were different to all the other methods,which underestimated the predicted REE by more than 200 kcal,except that of the Cunningham's formula[26],and the formula by McArdleet al[27]showed the greatest difference in the REE estimate in the studied population[15].
The use of IC for determining the REE in routine clinical practice has some difficulties,related to difficulty in buying the device,which has a high cost,the time needed to perform the test and the possible lack of cooperation in patients[35].
Thus,based on the data from our study,we suggest the use of BIA values for cases with HCC or those of the FAO/WHO formula[17]for those with or without HCC;the Cunningham formula[26]could be used in cases without HCC and the formula by McArdleet al[27]for those with HCC,as they are the ones closest to those obtained by IC in these cirrhotic patients[23].
The choice of these formulas in the present study is not in line with the recommendation by Plauthet al[47]in the guidelines of the European Society for Parenteral and Enteral Nutrition of 1997 for nutrition in liver diseases and transplants,where it was suggested that the Harris and Benedict predictive formula[21]should be applied to estimate REE in patients with cirrhosis when IC is not available in a clinical setting[47].
Our results demonstrate that the formulas of Harris and Benedict[21]and IOM[25]were the ones that showed the greatest differences when compared to the determination of REE by IC,which is why we do not recommend these predictive formulas.
The determination of REE by IC,BIA or by any recommended predictive formula,in cirrhotics with or without HCC,is essential for the nutritional diagnosis.Individualized treatment and specific nutritional interventions can delay the emergence of malnutrition and poor clinical evolution[48].
Thus,we emphasize that the same method of evaluation in different populations can present different correlations with the available predictive formulas.
CONCLUSION
The REE by IC in cirrhotic patients with and without HCC was similar.When comparing the IC values with those of the BIA,we found that in patients with HCC,the values were similar.The values estimated by the predictive formulas are very erratic and disparate,when compared to IC.The FAO/WHO formula[17]could be used for those with or without HCC;Cunningham formula[26]in those without HCC and the McArdleet al[27]in those with HCC,as they are the ones with the closest values to those obtained by IC in these cirrhotic patients[23,49].Apparently,the presence of HCC in cirrhotics does not appear to significantly alter the REE.
ARTICLE HIGHLIGHTS
Research background
The diagnosis of malnutrition in patients with hepatocellular carcinoma (HCC) varies from 20% to 50%,as it is related to important complications and has a direct impact on prognosis.Determination of the resting energy expenditure (REE) has become an important parameter in this population,as it allows therapeutic adjustments to recover their nutritional status.The REE in HCC is not clearly defined,and requires the identification and definition of the best nutritional approach.
Research motivation
The diagnosis of malnutrition in patients with HCC varies from 20% to 50%,is related to important complications and has a direct impact on prognosis.Determination of the REE has become an important parameter in this population,as it allows therapeutic adjustments to recover their nutritional status.The REE in HCC is not clearly defined,and the identification and definition of the best nutritional approach is necessary.
Research objectives
The aim of this study is to evaluate the REE of patients with cirrhosis,with and without HCC,measured by IC and to compare these values with those obtained by bioimpedance (BIA) and predictive formulas,in order to identify which is the best method of evaluation.
Research methods
This prospective observational study included 118 patients,aged ≥ 18 years,of both sexes,divided into two groups.One group consisted of 33 cirrhotic patients with HCC and a control group of 85 cirrhotics without HCC,attending the Department of Gastroenterology and Liver Transplantation of Irmandade da Santa Casa de Misericórdia de Porto Alegre,RS,Brazil,from March 2017 to August 2018.Quantitative variables were described by mean and standard deviation and categorical variables by absolute and relative frequencies.
Research results
The REE determined by indirect calorimetry (IC) in cirrhotic patients with HCC was 1643 ± 364 and in those without HCC was 1526 ± 277 (P=0.064).The REE value as assessed by BIA was 1529 ± 501 for those with HCC and was 1660 ± 385 for those without HCC (P=0.136).When comparing the values of REE determined by IC and predictive formulas in cirrhotics with HCC,it was observed that only the formulas of FAO/WHO (1985) and Cunningham (1980) presented values similar to those determined by IC.When comparing the REE values determined by the IC and predictive formulas in cirrhotics without HCC,it was observed that the formulas of Schofield (1985),FAO/WHO (1985),WHO (2000),IOM (2005) and Katch and McArdie(1996) presented values similar to those determined by IC.
Research conclusions
The REE determined by IC in cirrhotic patients with HCC was 1643 ± 364 and in those without HCC was 1526 ± 277 (P=0.064).The REE value assessed by BIA was 1529 ±501 for those with HCC and 1660 ± 385 for those without HCC (P=0.136).When comparing the values of REE determined by IC and predictive formulas in cirrhotics with HCC,it was observed that only the formulas of FAO/WHO (1985) and Cunningham (1980) presented values similar to those determined by IC.When comparing the REE values determined by the IC and predictive formulas in cirrhotics without HCC,it was observed that the formulas of Schofield (1985),FAO/WHO(1985),WHO (2000),IOM (2005) and Katch and McArdie (1996) presented values similar to those determined by IC.
Research perspectives
The REE as assessed by IC in cirrhotics with and without HCC was similar.When comparing the IC values with those of the BIA,we found that in patients with HCC,the values were similar.The values estimated by the predictive formulas were very erratic and disparate,when compared to IC.The FAO/WHO formula could be used for those with or without HCC;the Cunningham formula in those without HCC and the McArdle in those with HCC,as they are the ones with the closest values to those obtained by IC in these cirrhotic patients.Apparently,the presence of HCC in cirrhotics does not appear to significantly alter the REE.
 World Journal of Gastrointestinal Pharmacology and Therapeutics2021年1期
World Journal of Gastrointestinal Pharmacology and Therapeutics2021年1期
- World Journal of Gastrointestinal Pharmacology and Therapeutics的其它文章
- Increased colon transit time and faecal load in irritable bowel syndrome
- Clinical features and relative factors of constipation in a cohort of Chinese patients with Parkinson's disease