
Assessment of the safety and efficacy of acupuncture in erectile dysfunction treatment
2021-06-22 06:37MunirahMansourAlamro
Munirah Mansour Alamro
Centre for Traditional Chinese Medicine, University of Malta, Msida MSD 2080, Malta
Abstract Objective: To assess the safety and efficacy of acupuncture in erectile dysfunction treatment.
Keywords: Acupuncture Therapy; Traditional Chinese Medicine; Erectile Dysfunction; Men; Systematic Review
Erectile dysfunction (ED) is an extremely prevalent health problem that has been reported to affect about 30 million men in the USA. It is a common worldwide clinical problem, with tens of thousands of new cases being reported per year[1]. Worldwide, the affected people are predicted to increase from 152 million in 1995 to 322 million in 2025[1]. Some of the significant risk factors for ED include age, smoking, hypertension,obesity, coronary artery disease, lifestyle, hyperlipidemia,trauma, prostatic hypertrophy, diabetes, and depression[2]. Moreover, approximately 20% of the cases have added psychological reasons[2]. ED is recognized to impact the psychological, social, and physical health of the families and their quality of life[3-4]. In some cases,pharmacological treatment options for ED are available.Therapeutic options in the form of specific orallyadministered pharmacological agents (e.g., sildenafil,vardenafil, and tadalafil) and intracavernous injection are available to manage ED. However, some individuals prefer to avoid using these therapeutic options for a variety of reasons including side effects, drug interactions, and cost of medication[4].
Complementary and alternative medicine (CAM) has been extensively used to treat ED[5]. Acupuncture,defined as the insertion of needles into the skin and underlying tissues at acupoints for preventive or therapeutic purposes, is one of the most important components of CAM[6]. Contemporary researches proposed that the neurophysiological influence of acupuncture, as a result of neurotransmitter modulation and central nervous system activation, may positively affect the pathophysiology of ED[7-8]. The present study is a review of the relevant available published literature serving as a meta-analysis to assess the therapeutic role of acupuncture in the management of ED.
1 Methods
1.1 Databases
A systematic search was carried out to identify relevant studies using seven electronic databases including Popline, World Health Organization (WHO)Global Health Library (GHL), System for Information on Grey Literature in Europe (SIGLE), Scopus, Institute for Scientific Information (ISI) Web of Science, PubMed and Virtual Health Library (VHL). A manual search was further conducted for relevant publications from references of the included articles, relevant papers in PubMed and Google Scholar, and primary studies that had cited the included papers. The literature list was further augmented by hand-searching using each keyword to avoid missing any relevant publications.
1.2 Search methods
1.2.1 Search strategy
The search term used was ‘Acupuncture’ AND(‘Erectile Dysfunction’ OR ‘Sexual Dysfunction’ OR‘Impotence’). There were no restrictions for the study design, age, area, and publication year. Only English articles were chosen.
1.2.2 Inclusion criteria
Original publication reporting acupuncture for ED patients despite it was the main treatment or in combination; animal studies were included; no restriction made for the area, study design, and publication year.
1.2.3 Exclusion criteria
Unreliably extracted data; only abstract studies or studies where the full paper was not available; books,conference, and thesis; overlapped data sets;in vitrostudies; previous systematic reviews, meta-analyses and literature reviews on our topic of interest; non-English studies.
1.2.4 Screening
Duplication was removed using EndNote version X8.An initial eligibility assessment of the retrieved titles and abstracts was performed. Full texts of the eligible articles were then retrieved and reviewed for inclusion in the systematic review and were further screened for inclusion in the meta-analysis. In both steps of the screening, inclusion or exclusion of a study was considered conclusive. Any queries during the process were resolved by discussion and consensus with the supervisor.
1.3 Data extraction
Based on a pilot review and extraction, a data extraction form was developed using Microsoft Excel file.I extracted data from the included studies using the excel sheet. Before the initiation of analysis, rechecking was carried out by me and re-checked again for accuracy. All the queries were resolved by discussion and consensus with the supervisor. Papers published by the same research group and studying the same factors were checked for potential duplicate data based on the year of patient recruitment and the hospital where the patients were recruited and confirmation from the authors.
1.4 Quality assessment
Risk of bias in the included studies was evaluated.Methodological quality assessment was done using the National Institutes of Health (NIH) quality assessment tool for cohort and cross-sectional studies (2014)[9].Quality assessment of each study was obtained through a scoring system, including 14 questions. The criterion was judged as following: a score of 13 to 14 was good, 9 to 12 was fair, and studies scored below 9 were considered to have poor quality for cohort and crosssectional studies[10]. Furthermore, the Cochrane quality assessment tool was used to determine the quality of randomized studies[11]. Any queries were solved by consulting the supervisor.
1.5 Statistical analysis
Meta-analysis was performed using the comprehensive meta-analysis software version 3 when there was more than one study. The adjusted and nonadjusted hazard ratios (HR) were pooled for mortality events. Also, raw data were used to calculate the pooled risk ratio (RR) for mortality. Mean difference (MD) was used to analyze continuous outcomes. Odds ratio (OR)was used to pool other outcomes. Fixed effect model with the method of Mantel N,et al[12]was used when there was no evidence of heterogeneity between studies.Otherwise, the random effects model was chosen.Heterogeneity between studies was estimated using theQ-test, andI-squared (I2) test which describes the percentage of variability in effect estimates that is because of heterogeneity beyond sampling error[13-14].Significant heterogeneity was considered whenP<0.10,or theI2>50%[11]. Further sensitivity analysis was carried out by removing one study each time to investigate their impact on the effect size magnitude. Furthermore, metaregression and subgroup analyses were performed when there were ten or more studies in the analysis and comparable groups, respectively. Begg CB,et al[15]used funnel plot and Egger M,et al[16]used regression test to evaluate the presence of publication bias, when there were ten or more studies in the analysis[17]. The publication bias was significant whenP<0.10. If publication bias was found, the trim and fill method of Duvall and Tweedie was done by adding studies that seemed to be missing[18-19]to enhance the symmetry[20].The adjusted pooled effect size and its 95% confidence interval (CI) were computed after the addition of potential missing studies.
2 Results
2.1 Literature search
The literature search yielded 2 818 reports after removing duplicates using Endnote software. There were 21 studies eligible for full-text screening and five of which were subsequently included. After two studies that were identified from the manual search were added, a total of 7 studies were included for the systematic review and meta-analysis. Five of these were used for quantitative and qualitative analysis, while two were only used for qualitative analysis (Figure 1 and Table 1)[21-26]. These publications included four clinical trials, one pilot study,one case report, and one animal study.
2.2 Study and patient characteristics
The characteristics of studies included for quantitative analysis are summarized in Table 1. A total of 167 patients were included. Of these, 60 had sexual dysfunction of a non-organic cause, 39 had a psychogenic ED, 19 had ED caused by medication, one had ED caused by type 2 diabetes mellitus and one because of hypertension. Three studies reported the outcome measurement according to the patients’perception. One study reported outcome according to the sexual function visual analog scale (SFVAS) and the Arizona sexual experience questionnaire (ASEXQ)[24].Another study reported outcome according to the international index of erectile function 5 (IIEF5)[26]. The treatment duration varied between 6 weeks and 30 months; the 20-minute session was the most common duration.
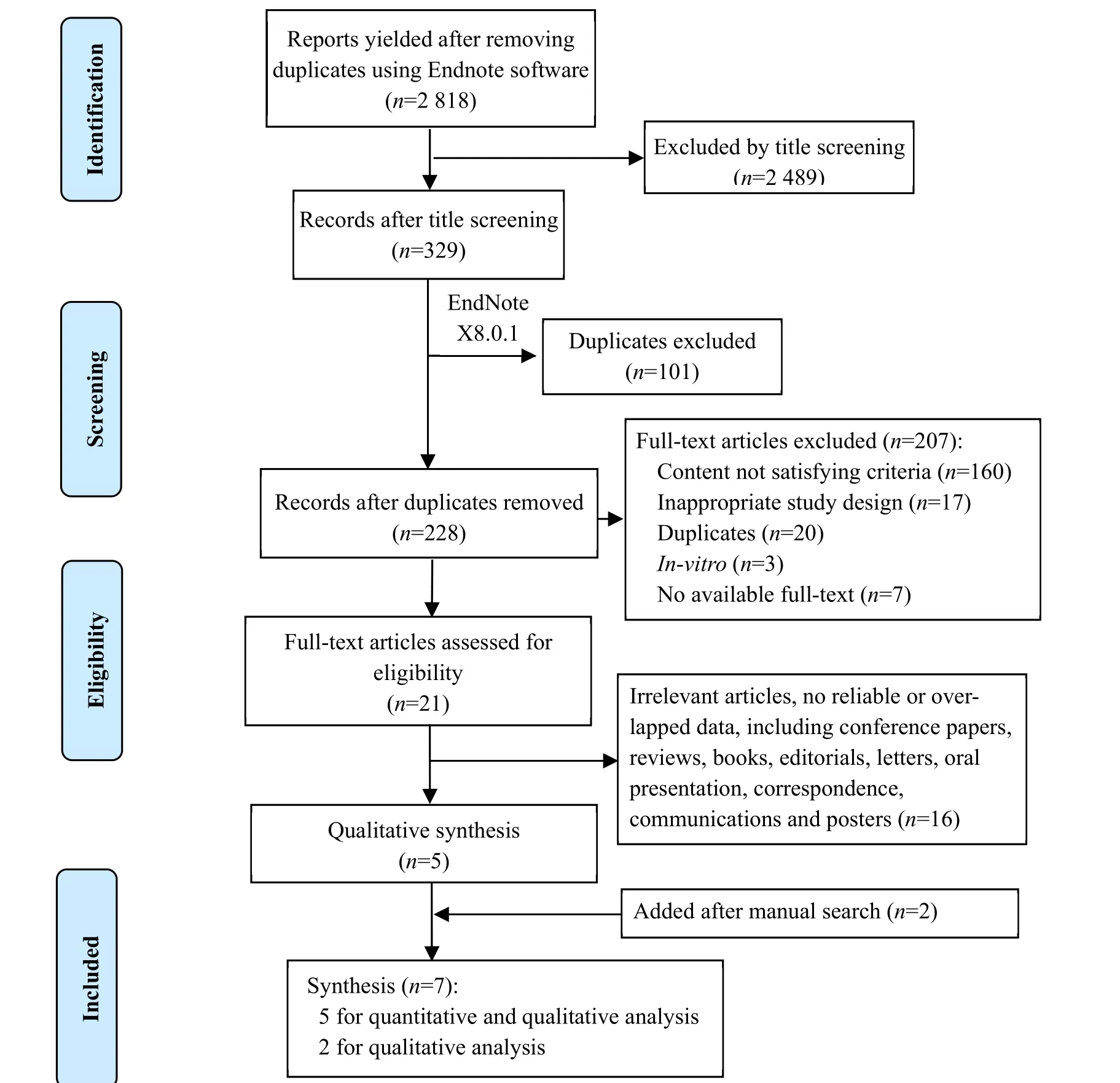
Figure 1. Flow chart of study selection

Table 1. The characteristics of studies included for quantitative analysis
2.3 Quality assessment
Results of quality assessment are summarized in Table 2. There were two studies with overall risk of bias as low, one study with overall risk of bias as moderate and two studies with overall risk of bias as high.
2.4 Quantitative results
2.4.1 Acupuncture in comparison with placebo needles
Two studies of total 59 patients studying the effectiveness of acupuncture for ED in comparison with placebo needles showed that acupuncture had significantly positive results against placebo needle with[OR (95% CI)=4.06 (1.177-14.030),P=0.027], (Figure 2).
2.4.2 Acupuncture in comparison with hypnosis for ED
One study of 31 patients reported the comparison between acupuncture and hypnosis as methods for ED treatment[21]. Interestingly, there was no significant between-group difference withP=0.375.
2.4.3 Acupuncture in comparison with warm needling
One study with 46 ED patients compared warm needling with acupuncture[26]. Interestingly, the overall effective rate in the warm needling group was 91.3%,versus 75.0% in the traditional acupuncture group, and the between-group difference was statistically significant withP<0.05.
2.4.4 Acupuncture for sexual dysfunction caused by antidepressant
One study reported 18 patients with ED due to antidepressant were treated with acupuncture[24]. The study showed significant improvement in all areas of sexual functioning, as well as in both depressive and anxiety symptoms.
2.4.5 Acupuncture for sexual dysfunction of psychogenic cause
Engelhardt PF,et al[23]reported a study of 19 ED patients with psychogenic cause treated with acupuncture; surprisingly the results were satisfactory with 68.4% effective rate and a significant difference with the placebo group (P=0.0017).

Table 2. Quality assessment of the included studies
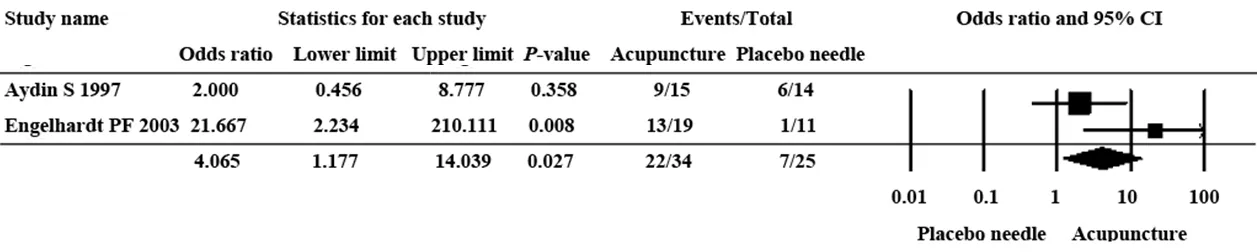
Figure 2. Acupuncture in comparison with placebo needle for ED
2.5 Qualitative analysis
2.5.1 Acupoint used for acupuncture
Different acupoints were used in the different studies[21-24]. Aydin S,et al[21]in their study used disposable sterile No. 30 needles at Qichong (ST 30),Zusanli (ST 36), Zhaohai (KI 6), Guanyuan (CV 4) and Qihai(CV 6). Qichong (ST 30) is found two fingerbreadths lateral to the symphysis on the lower edge of the pubic bone and the needle is inserted downwards. Zusanli(ST 36) lies on the point of intersection of the lines half a fingerbreadth lateral to the linea interossei of the tibia and two fingerbreadths below the head of fibula.Zhaohai (KI 6) lies one fingerbreadth below the internal malleolus. Guanyuan (CV 4) lies three fingerbreadths above the symphysis. Qihai (CV 6) is found two fingerbreadths below the navel[21]. Liu P,et al[26]in their study used Qihai (CV 6), Guanyuan (CV 4), Zhongji (CV 3),Yaoyangguan (GV 3) and bilateral Taixi (KI 3), Shenshu(BL 23), Ciliao (BL 32) and Yanglingquan (GB 34). Kho HG,et al[22]used Guanyuan (CV 4), Baihui (GV 20), bilateral Sanyinjiao (SP 6), Taixi (KI 3) and Shenmen (HT 7).Interestingly, Khamba B,et al[24]used 34-gauge disposable stainless-steel needles bearing and retained the needles for 15 min at nine common acupoints for 12 sessions. According to the traditional Chinese medicine technique, five of the acupoints were reinforced using thrusting and rotation manipulations in the clockwise direction at 5-minute and 10-minute for Mingmen (GV 4),bilateral Taixi (KI 3) and Shenshu (BL 23). The even reinforcing-reducing manipulation during which the needles were retained untouched for the duration of treatment, was applied to bilateral Shenmen (HT 7) and Neiguan (PC 6).
2.5.2 Other narrative data
Hiroshi T,et al[25]reported a 61-year-old man who suffered from ED for two years since his diagnosis with type 2 diabetes mellitus. Initially, sildenafil citrate, which is a phosphodiesterase type 5 inhibitor, efficiently treated his ED. Nonetheless, the patient's response to this medication deteriorated over time, until he was no longer able to achieve an erection, despite treatment.The authors used manual acupuncture at Zhongliao(BL 33) which induced beneficial effects according to the IIEF5. The patient reported an improvement suggesting that the combination of acupuncture and sildenafil had a good impact. Huang AC,et al[27]investigated the interactive activity of electroacupuncture (EA) on the pharmacokinetics of sildenafil and their synergistic effect on penile blood flow in rats. The pharmacokinetic studies confirmed that sildenafil was significantly increased by the administration of low-frequency EA. Moreover, the pharmacodynamic studies using Doppler imaging revealed an elevated blood flow in the rat penis compared with the lower body during combined treatment of sildenafil and low-frequency EA. These data show a potential synergistic therapeutic effect of EA and sildenafil for the treatment of ED.
3 Discussion
3.1 Summary of the main results
A total of seven studies have been included in this systematic review and meta-analysis. According to these studies, sexual dysfunction of non-organic cause is the major cause for ED. The acupuncture treatment duration varied between 6 weeks to 30 months; the 20-minute session was the most common duration of treatment.Regarding quality assessment, there were two studies with an overall risk of bias as low. Acupuncture showed significantly positive results compared with placebo needling; no significant association has been shown between acupuncture and hypnosis as methods for ED treatment; while a statistically significant association was reported when comparing warm needling with acupuncture. Of particular concern to ED causes, since antidepressant drugs are a significant cause for ED,acupuncture appeared to be an effective method for the treatment of psychogenic ED. The present analysis included five different studies which considered the acupoints used for acupuncture with different acupoints being used as detailed earlier. Combination of acupuncture appeared to show a beneficial effect of acupuncture as adjunctive therapy for ED participants with type 2 diabetes mellitus when compared with other conventional therapies (initially treated with sildenafil citrate). The present review also suggested a synergistic therapeutic effect of EA and sildenafil for the treatment of ED.
3.2 Comparison with previous studies
There are three published review studies on this topic.One included 3 RCTs, including 183 participants with ED[28], comparing acupuncture and psychological therapy with acupuncture and psychological therapy.The included RCTs in this review failed to present a specific therapeutic effect of acupuncture and had methodological flaws as observed by the authors.Another recent study included only a Chinese database and involved 6 RCTs. In these studies, the control treatment included only Chinese herbal medicine and the details of treatment information were not specified[29]. The third review was performed using analyses depending on different comparisons and reported that although the strength of the evidence was weak, the findings revealed there was a potential add-on effect of acupuncture for ED patients. A total of 31.8% of the included trials had reported adverse information from acupuncture. This review provided the latest evidence published of acupuncture for ED[30]. The findings of these three reviews were not finally pooled because of clinical and statistical heterogeneity, which failed to show a definite therapeutic effect of acupuncture for ED. Compared to the previous two reviews, this updated review covered a broader combination of studies, including acupuncture with moxibustion, acupoint injection and different comparisons, and additional outcome assessments.
3.3 Limitations
The present study possesses some limitations of note.Firstly, there is a possibility that relevant research papers were missed (e.g., those not written in English), resulting in selection bias. Secondly, although the Cochrane Library was checked, grey literature in other databases may have been missed. Thirdly, although the review and extraction processes were conducted independently and double-checked, it was still subjective and dependent on the reports of articles, rather than the direct assessment of the studies. The analysis was further limited by the fact that the methods used for the assessment of ED varied between studies. Furthermore, there was limited information in the reported studies regarding the use of medications such as beta-blockers, diuretics,phosphodiesterase inhibitors, testosterone, and antihypertensive agents that may have contributed to ED.Finally, the studies on acupuncture treatment of ED have the deficiency of small sample size and low overall quality,which may affect the authenticity of this review and its conclusions. It is therefore essential that there need to be more rigorous and reasonable multicenter RCTs to explore the clinical efficacy of acupuncture for ED to make the conclusions more objective and reasonable.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
I would like to express my appreciation to Prof. Dr.Charles Savona-Ventura for his keen interest in the progress of this work. He has been very generous in providing me with knowledge and scientific materials. Sincere thanks to Dr. Samer Saad Ali Adwal for his support throughout the year. Special thanks to all the Chinese doctors involved in the course for the supervision and help at all stages of this study.
Received: 8 July 2020/Accepted: 6 November 2020
 Journal of Acupuncture and Tuina Science2021年3期
Journal of Acupuncture and Tuina Science2021年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation of heat-sensitive moxibustion for acute ischemic stroke
- Efficacy observation of Zhi Shen Tiao Sui acupuncture method for depression after ischemic stroke
- Clinical observation on acupoint pressure plus longsnake moxibustion for upper-limb spastic hemiplegia after cerebral infarction
- Clinical efficacy observation of acupoint threadembedding in treating obese patients with food addiction
- Effect of mild moxibustion on cancer-related fatigue,serum ghrelin and adiponectin in patients undergoing chemotherapy after colorectal cancer surgery
- Effects of acupuncture plus spinal manipulations on physical functioning and biochemical indicators in patients with ankylosing spondylitis