Treatment of advanced biliary tract cancers: from chemotherapy to targeted agents
2021-05-10 09:11RaffaellaCasolinoChiaraBraconi
Hepatoma Research 2021年12期
Raffaella Casolino, Chiara Braconi
1Wolfson Wohl Cancer Research Centre, Institute of Cancer Sciences, University of Glasgow, Glasgow G61 1QH, UK.
2Department of Medicine, University of Verona, Verona 37100, Italy.
3Department of Medical Oncology, Beatson West Of Scotland Cancer Centre, Glasgow G12 0YN, UK.
Abstract Biliary tract cancers (BTCs) are usually diagnosed at an advanced stage and have a dismal prognosis. The treatment of advanced disease is mainly based on systemic chemotherapy, which is demonstrated to improve survival in the first- and second-line setting. Following the results of phase III clinical trials, the combination of cisplatin and gemcitabine is the regimen of choice in the frontline, while 5-fluorouracil plus oxaliplatin is considered the standard after first-line progression in unselected patients. Recent advances in molecular biology have unravelled the molecular heterogeneity of BTCs and identified patient subgroups harbouring unique molecular aberrations such as isocitrate dehydrogenase (IDH) mutations and fibroblast growth factor receptor (FGFR)fusions that can be targeted by specific agents. This knowledge has opened the way to personalised medicine in BTCs. Molecules targeting IDH and FGFR are currently approved for the treatment of advanced, refractory,intrahepatic cholangiocarcinoma. Beyond targeted therapies, novel combinatorial approaches that target the immune microenvironment and the crosstalk between cancer and stroma are being explored based on strong preclinical rationale. This review discusses the current therapeutic opportunities for the management of patients with advanced BTCs and provides an overview of the promising new strategies on the horizon with a particular focus on ongoing clinical trials.
Keywords: Biliary tract cancers, cholangiocarcinoma, precision medicine, targeted therapies, fibroblast growth factor receptor, isocitrate dehydrogenase, chemotherapy
INTRODUCTION
Advanced stage is the most common clinical presentation of biliary tract cancers (BTCs). Given the paucity of specific early symptoms and the lack of early-detection programs, up to 80% of patients are diagnosed with unresectable tumours[1,2]. In addition, recurrence rate after surgery ranges between 50% and 79%, even for those patients diagnosed with early-stage cancer[3-5]. Advanced disease at presentation or relapse after local treatment, along with the scarce availability of active treatments and the significant chemo-resistance,make BTCs one of the deadliest solid tumours with a global five-year survival rate of 10%[6]. In this scenario,untreated patients have an overall survival (OS) of 3-4 months, while those receiving active treatment can reach up to 18-20 months with two therapeutic lines[7-10]. Systemic approach represents the standard of care of advanced biliary tract cancers (aBTCs) and aims at increasing survival, delaying disease progression,relieving symptoms, and improving/maintaining the quality of life. Historically, cytotoxic chemotherapy was the only available option and was associated with marginal improvements in oncological outcomes.More recently, emerging compounds targeting isocitrate dehydrogenase (IDH) 1 mutations and fibroblast growth factor receptor (FGFR) 2 fusions, as well as immune checkpoint inhibitors (ICIs), showed promising results in molecularly selected patients[11]. Thanks to advances in molecular biology, many other therapeutic vulnerabilities have recently been identified both in the tumour and in the surrounding microenvironment,providing a plethora of novel potential strategies to be further investigated for the treatment of BTCs[12].
In this paragraph, we aim to offer an overview of the current therapeutic approaches for the management of patients with aBTCs, and to discuss the novel opportunities on the near horizon.
UNSELECTED TREATMENT APPROACH: PAST, PRESENT AND FUTURE
The history of the therapeutic development in BTCs has been characterised by “all-comers” design of clinical trials exploring the efficacy of cytotoxic agents and targeted therapies. This “one size fits all” model has shown clinical benefit from chemotherapy, allowing the identification of current standard first and second-line regimens[7,8]. Chemotherapeutic drugs combination is demonstrated to increase efficacy by using different mechanisms of cytotoxic action. The two chemotherapy combinations regimens approved following positive results of phase III clinical trials include cisplatin and gemcitabine (CisGem) for frontline treatment and 5-fluorouracil plus oxaliplatin (FOLFOX) after first-line progression. More recently, two combinatorial regimens showed promising results in phase II studies for the first-line (cisplatin,gemcitabine, and nab-paclitaxel)[13]and second-line (5-fluorouracil and liposomal irinotecan; Nal-Iri)setting[14]. Clinical studies investigating targeted therapies and ICIs have been widely unsuccessful in unselected patients instead[15-24].
First-line chemotherapy
Limited data supported effective management of aBTCs before 2010. A pooled analysis of 104 small and nonrandomised trials, including 2810 patients conducted in 2007, showed combination chemotherapy with CisGem or oxaliplatin being the most active strategy[11]. The first evidence of superior regimen from randomised phase II study was reported in 2007, when CisGem demonstrated better time to progression compared to gemcitabine alone (8 monthsvs. 4 months, respectively) and improved disease control rate(DCR)[25]. This association became the standard first-line treatment for patients with metastatic BTCs since 2010, when the Advanced Biliary Tract Cancer (ABC-02) phase III trial demonstrated the superiority of CisGemvs. gemcitabine alone[7]. The median overall survival (mOS) resulted superior for the experimental arm compared to gemcitabine [11.7 monthsvs. 8.1 months, respectively; hazard ratio (HR) = 0.64; 95%confidence interval (CI): 0.52-0.8;P< 0.001]. The combination also demonstrated a better rate of partial response (PR) compared to the gemcitabine (26%vs. 16%, respectively)[7]. Similar results were reported in the Japanese BT22 randomised phase II trial that investigated the antitumour activity of the same agents(mOS 11.2 monthsvs. 7.7 months; HR = 0.69; 95%CI: 0.42-1.13;P= 0.139)[26]. The meta-analysis of the two trials confirmed significant improvement in progression-free survival (PFS) (HR = 0.64; 95%CI: 0.53-0.76;P< 0.001) and OS (HR = 0.65; 95%CI: 0.54-0.78;P< 0.001) of CisGem over gemcitabine for intra-and extrahepatic cholangiocarcinomas (iCCA and eCCA) and gallbladder cancer, with most marked efficacy among patients with good performance status (PS 0-1) (HR for PFS = 0.61; 95%CI: 0.51-0.74;P< 0.001; HR for OS= 0.64; 95%CI: 0.53-0.77;P< 0.001)[27]. Table 1 shows an overview of these three studies.
Subsequent studies explored the role of other compounds such as oxaliplatin and fluoropyrimidines.Oxaliplatin showed a more favourable toxicity profile than cisplatin, with mOS reaching 12.4 months and overall response rate (ORR) up to 50%[21,22], but its activity has never been tested in a head-to-head comparison with CisGem. Nonetheless, this agent may be adopted when cisplatin is contraindicated.Fluoropyrimidines have also been shown to be active in aBTCs studies, but their precise role is still controversial as a direct comparison with gemcitabine-based regimens is lacking[28,29].
Another treatment option in the first-line setting is represented by gemcitabine plus S-1 (a fluoropyrimidine derivative), as suggested by the FUGA-BT phase III trial showing non-inferiority of this regimen compared with CisGem in the Japanese population[30].
Whether intensifying chemotherapy could improve oncological outcomes by maintaining a good quality of life is still an unanswered question and is currently under clinical investigation. In the Japanese population,the association of cisplatin, gemcitabine, and S1 could represent a treatment option on the basis of a phase III trial, demonstrating an improved OS of the triplet compared with CisGem (13.5 monthsvs. 12.6 months;HR = 0.791; 90%CI: 0.620-0.996;P= 0.046)[31].
Results from a phase II trial evaluating cisplatin, gemcitabine hydrochloride (salt of an analogue of the antimetabolite nucleoside deoxycytidine with antineoplastic activity), and nab-paclitaxel demonstrated median PFS (mPFS) of 11.8 months, mOS of 19.2 months, 45% response rate (RR) and 84% DCR with this regimen[13]. The ongoing phase III SWOG-1815 clinical trial will establish whether the triplet is more efficacious than the standard CisGem (NCT03768414). Likewise, a phase III study comparing CisGemvs.FOLFIRINOX (oxaliplatin, irinotecan, and 5-fluorouracil) has recently completed recruitment(NCT02591030) and will define if non-gemcitabine regimes have a place in first-line. Furthermore, a phase II study is exploring the activity of Nal-Iri in combination with 5-fluorouracil (5-FU)/leucovorin (LV)vs.CisGem (NCT03044587)[12].
Second-line chemotherapy
Following a failure to first-line chemotherapy, 25%-40% of BTC patients are still fit to receive second-line chemotherapy[32]. The choice of second-line treatment is extremely limited, particularly in unselected patients. In daily practice, 5-FU-based chemotherapy has been the most widely adopted regimen, despite the absence of robust evidence and the poor clinical efficacy (mPFS of 2.5-5.5 months and a mOS of 7.5-13.5 months in published series)[33].
Only recently, the phase III ABC-06 study demonstrated the superiority of FOLFOXvs. active symptom control (ASC, i.e., proactive detection of biliary obstruction, sepsis, and symptom management) in patients progressing to CisGem[8]. This study enrolled 162 patients with aBTC, including 72% of CCA following progression on standard first-line CisGem. Patients were randomised to ASC (81 patients) or ASC plus FOLFOX (81 patients). The ABC-06 trial demonstrated a benefit from second-line chemotherapy in terms of OS (HR = 0.69; 95%CI: 0.50-0.97;P= 0.031). Even though absolute differences in mOS were modest (5.3months for ASC armvs. 6.2 months for ASC + FOLFOX arm), differences in the survival rate at 6 months (35.5% for ASC armvs. 50.6% for ASC + FOLFOX arm) and 12 months (11.4% for ASC armvs. 25.9% for ASC + FOLFOX arm) were clinically meaningful[8]. Based on this evidence, FOLFOX is currently considered the standard of care second-line chemotherapy for patients with aBTCs without driver mutations who remains fit following CisGem progression.

Table 1. First-line chemotherapy in Biliary tract cancers: an overview of pivotal studies
The efficacy and safety of FOLFIRINOX with two different dosages (standard and modified) was investigated in a recent phase II trial enrolling 40 patients who had disease progression or unacceptable toxicity after ≥ 3 cycles of CisGem. The mPFS and mOS were 6.2 and 10.7 months, and the toxicity profile was acceptable[34]. Therefore, in patients with aBTCs who progress after or are intolerant to CisGem, FOLFIRINOX could be considered as an option for salvage treatment, even though borderline fitness of BTC patients in second-line may limit its applications[12].
Recent data from the NIFTY randomised, phase IIb study presented at ASCO 2021 showed that Nal-IRI plus 5-FU/LV significantly improved PFS and OS compared to 5-FU/LV in BTC patients who progressed on prior GemCis[14]. mPFS per investigator review in Nal-IRI plus 5-FU/LV group and 5-FU/LV group was 3.9 months and 1.6 months respectively (HR = 0.48; CI: 0.34-0.69;P< 0.0001); mOS was 8.6 months and 5.5 months respectively (HR = 0.68; CI: 0.48-0.98;P= 0.0349); ORR was 14.8% and 19.3% and 2.3%, respectively (P= 0.0002)[14].
One of the main challenges for the completion of adequately powered studies is that, given the aggressive clinical behaviour of CCA, <40% of patients are considered eligible for second-line treatment while many others rapidly drop out of clinical trials due to clinical deterioration[35-39]. Amongst the subtypes of BTC, iCCA is usually associated with better performance status, with increased access to personalised approaches based on the tumour molecular profile,which will be discussed in the next chapter.
Prognostication
Reliable prognostic/predictive biomarkers to assist the therapeutic decision making in patients with aBTCs are still lacking. To date, only clinical prognostic factors independently associated with OS have been suggested, including Eastern Cooperative Oncology Group (ECOG) performance status (PS), blood tests(white blood cells and neutrophil count, haemoglobin and bilirubin levels), disease status, and gender, from the post-hoc analysis of CisGem pivotal trials[7,26,40]; and ECOG PS, prior resection, tumour grading, baseline carcinoembryonic antigen and carbohydrate antigen 19.9 (CA19-9), from the Italian Group of Cholangiocarcinoma, G.I.Co[36].
Recently, a prognostic score was derived by baseline neutrophil count, lymphocytes-monocytes ratio,neutrophil-lymphocytes ratio and albumin: the A.L.A.N. score. This prognostication has been shown to correlate with OS in a cohort of 123 aBTCs patients undergoing first-line chemotherapy. A.L.A.N. score was able to identify three classes of patients with significantly different OS (high-risk: median OS, 5 months;intermediate-risk: median OS, 12 months and low-risk: median OS, 22 months;P< 0.001)[14]. Many other clinical prognostic scores have been proposed, however, no standard currently exists[41-45].
The post-hoc analysis of ABC-01/02/03 trials of CisGem has also indicated a more favourable prognosis of iCCA and iCCA with liver-only disease. iCCA had a longer OS compared with other non-iCCA biliary tract cancers (HR = 0.58; 95%CI: 0.35-0.95;P= 0.03); liver-only iCCA patients also showed longer OS even though findings did not reach statistical significance (HR = 0.65; 95%CI: 0.36-1.19;P= 0.16)[40].
Despite being informative, evidence is yet to be confirmed in large, prospective, clinical studies, but until then, the optimal prognostication to adopt in the therapeutic decision of aBTCs remains uncertain.
To summarise, CisGem is the regimen of choice in the frontline, while FOLFOX is the standard after firstline progression in unselected patients [Figure 1]. Other options (i.e., single agents) may be carefully considered when the standard treatment is contraindicated or due to patient’s preferences. Several novel combinations are currently under clinical investigation. A selection of the most relevant ongoing clinical trials based on cytotoxic chemotherapy are shown in Table 2.
The allocation of locoregional strategies, complementary to chemotherapy, should be considered in the context of clinical studies.
Reliable prognostic and predictive biomarkers are still lacking and desirable, particularly in the second-line setting.
PRECISION MEDICINE: BIOLOGICAL RATIONALE AND THERAPEUTIC STRATEGIES
Advances in Next-Generation Sequencing technologies and large-scale initiatives from cooperative groups such as The Cancer Genome Atlas, the International Cancer Genome Consortium and others have allowed the characterisation of the molecular landscape of BTCs over the last decade, resulting in the identification of key actionable oncogenic drivers and signalling networks[46-54]. Firstly, biological differences according to anatomic location (iCCAsvs.eCCA), geographical location (Easternvs. Western), and etiology (Hepatitis B,fluke, other causes) have been identified. Secondly, somatic - potentially targetable - alterations have been described in up half of patients with BTC[55-58].

Table 2. Cytotoxic chemotherapy: selection of ongoing clinical trials
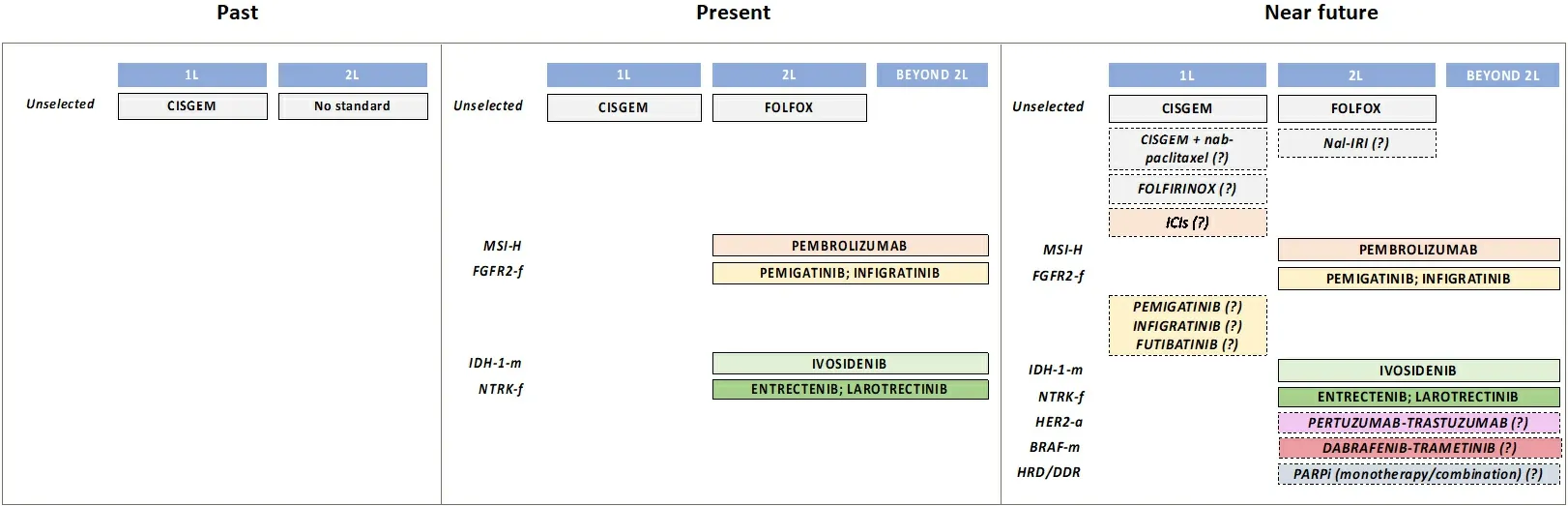
Figure 1. Evolution of systemic treatments of aBTCs. aBTCs: Advanced biliary tract cancers; L: line; ICIs: immune checkpoint inhibitors;m: mutations; f: fusions; a: amplifications; italic: under current clinical investigation; CISGEM: cisplatin + gemcitabine; FOLFOX: 5-fluorouracil + folinic acid + oxaliplatin; Nal-IRI: nanoliposomal irinotecan; FOLFIRINOX: 5-fluorouracil + folinic acid + oxaliplatin +irinotecan; PARPi: poly-ADP ribose polymerase inhibitors.
This evidence has paved the way for the precision medicine revolution in this rare group of malignancies.
The molecular landscape of BTCs: single genetic alterations, molecular networks and subgroups
Data from published and non-published studies available in the cancer genomic datasetc-bioportal[59]indicateTP53,ARID1A,IDH1,BAP1,PBRM1,KRAS,SMAD4andATMas the most frequent molecular alterations in BTCs. As already mentioned, different patterns of mutations according to the specific anatomic subtype have been described, highlighting the high molecular heterogeneity - and possibly diverse etiopathogenesis - of histologically similar cancers [Figure 2]. The predominant molecular changes in BTCs are associated with epigenetic processes, particularly for iCCA, characterised by a higher frequency of mutations inIDH1, relevant for the cell metabolism processes (found in 10%-20% of cases) andFGFR2rearrangements (found in up to 23% of patients). The latter consists in the fusion of the intact kinase domain ofFGFR2with several genes (BICC1,AHCYL1,TACC3,MGEA5andPPHLN1), which constitutively activates theFGFR2fusion protein and the downstream pathways, thus promoting tumour growth[60-66]. In contrast, alterations in other genes such asBAP1,TP53,KRAS,ERBB2,SMAD4,ARID1B,

Figure 2. BTCs subtypes and therapeutic targets. Figure 2 shows the recurrent molecular aberrations in biliary tract cancers (BTCs)with a focus on the prevalence variations according to the anatomic subtypes. Fibroblast growth factor receptor 2 (FGFR2) fusions (f)and isocitrate dehydrogenase 1 (IDH-1) mutations (m) are more common in intrahepatic cholangiocarcinoma (iCCA), while human epidermal growth factor receptor 2 (HER2) mutations and amplifications (a) are more common in extrahepatic cholangiocarcinoma(eCCA) and gallbladder cancer (GCB). Aberrations in other genes and pathways (including immune microenvironment characteristics)are independent of the anatomic location (indicated outside the circle). In red: established targets and approved drugs; in black:targeted therapies under clinical investigation. CCA: Cholangiocarcinoma; DDR: DNA damage repair. HRD: homologous recombination deficiency; MSI-H: microsatellite instability-high; NA: not available.
ELF,PBRM1, andSTK11are more common in perihilar, eCCA, and gallbladder cancer[46,56,67,68].Integrative genomics studies have also unravelled the genomic characterisation of the most prevalent oncogenic signalling pathways, including those involved in cell survival, angiogenesis, signal transduction and transcriptional control[69,70]. Genetic and epigenetic changes in BTCs cooperate in complex oncogenic networks, including NADPH metabolism, SWI-SNF complex, de-ubiquitination, and histone(de-)methylation, kinase signalling, WNT-CTNNB1 network, cell cycle control, WNT/Notch signalling,DNA damage repair, and many others[69,70]. This knowledge underlines the significant complexity of the molecular biology of biliary malignancies and poses major challenges in translating the genomic discoveries into the clinic. In particular, therapeutic inhibition of single gene activations is unlikely to achieve the durable antitumour activity, while combinatorial approaches targeting different pathways may result in more effectiveness. On the other hand, the identification of patient groups with shared molecular aberrations beyond point mutations in coding genes could overcome the above-mentioned challenges, thus facilitating the personalised drug development process.
In this context, distinct recurring molecular subgroups with different prognoses and responses to therapy have been identified. Siaet al.[69]described two subtypes of iCCA with different activated pathways and prognosis: the inflammation class (38% of cases) associated with the activation of inflammatory pathways,overexpression of cytokines, andSTAT3activation; and the proliferation class (62% of cases) associated withKRASandBRAFmutations and oncogenic pathways activation (i.e., RAS,MAPK, andMET).
Through integrated genomic analysis of iCCA (whole-exome sequencing, targeted exome sequencing) and epigenomic data from 496 patients, Nepalet al.[71]described unique mutational signatures, structural variants and epigenomic alterations and proposed four different molecular subgroups with specific drugresponse profiles:IDHmutant (drug: metabolic modulators),KRASmutant (drug: microtubule modulators),TP53mutant (drug: topoisomerase inhibitors), and “undetermined” (drug: mTOR inhibitors).
Another interesting classification that considers the tumour microenvironment (TME) characteristics of iCCA has identified 4 TME-based subtypes related to distinct immune escape mechanisms and patient outcomes[72]. About 45% of iCCA displayed an immune desert phenotype, while the 11% presented a massive T lymphocyte infiltration, activation of inflammatory and immune checkpoint pathways, and was associated with the longest patient survival (inflamed subtype). The other two subtypes differed in nature(lymphoid, myeloid, mesenchymal) and abundance of tumour-infiltrating cells[72]. The inflamed subgroup constitutes the most clinically relevant as it may potentially identify patients who are more likely to benefit from ICIs.
Personalised therapeutic approaches in aBTCs
The above data indicate the potential for oncogenic network characterisation to enable efficient stratification and therapy optimisation for patients with biliary cancers. A deeper understanding of the molecular biology underlying biliary tract malignancies and the high genomic/anatomical heterogeneity identified across histologically similar tumours may also partially explain the limited clinical advances achieved in the past decades. The lack of therapeutic targets, along with the “all-comers” design of clinical trials investigating targeted therapies in unselected patients (widely unsuccessful) may be an additional explanation for disappointing results achieved in past years[15-24].
On the other hand, promising results of personalised medicine for aBTCs have been demonstrated in molecularly driven studies. Among 43 pre-treated patients with aBTCs included in the prospective clinical trial MOSCATO-01, successful biopsy with multiple high-throughput molecular analysis was obtained in 34 patients. Orientation to an appropriate early clinical trial or administration of molecular-targeted agents was possible for 23 of these patients (68%), and 18 (53%) have received matched treatment. Among them, the ORR was 33%, and the DCR was 88%, while a PFS ≥ 6 months was observed in 37%. These patients had a lower risk for death as compared to the 20 patients not orientated to a matched treatment (mOS 17 monthsvs. 5 months; HR = 0.29; 95%CI: 0.11-0.76;P= 0.008)[73].
This analysis highlighted the relevance of histology-agnostic personalised medicine in the identification of patient subgroups to be matched with compounds targeting the specific molecular alteration and paved the way for the next-generation personalised medicine programs in BTCs.
Several compounds targeting single gene alterations have shown clinical activity and efficacy in advanced BTCs [Figure 2], others are currently under clinical investigation [Table 3], and many others are on the horizon [Figure 2].
Currently, the most promising and clinically relevant target therapies are IDH inhibitors for patients carryingIDH-mutations and compounds targetingFGFR2gene fusions[48]. Several IDH inhibitors are being explored for the treatment of advanced iCCA: inhibitors of IDH1 (ivosidenib), IDH2 (AG221), and pan-IDH1/2 (AG881). Ivosidenib showed encouraging results in a phase I dose escalation and expansion basket study. A total of 77IDH1mutant patients with refractory iCCA received the IDH1 inhibitor with stable disease and partial response achieved in 40 and 4 patients, respectively[74]. The positive results were subsequently confirmed in the ClarIDHy phase III trial, where 185 patients withIDH1-mutant CCA were randomised to receive the IDH1 inhibitor ivosidenib or placebo after 1-2 lines of unsuccessful systemic therapy. Ivosidenib significantly improved PFS (the primary endpoint). mPFS was 2.7 months in the experimental group and 1.4 months in the placebo group (HR = 0.37; 95%CI: 0.25-0.54;P< 0.001), with a 12 months PFS rate of 22%vs. 0%[10]. The intention to treat analysis showed a mOS of 10.3 months in patients treated with ivosidenibvs.7.5 months in the placebo group (HR = 0.79; 95%CI: 0.56-1.12;P= 0.093)[75].However, the design of the study allowed crossover to ivosidenib in the placebo arm at progression resulting in 35 patients receiving the experimental drug in the control group. A rank preserving structural failure time-adjusted analysis taking into consideration the effects of the crossover showed a more clinically meaningful result with a 4-months increase in median OS (10.3 monthsvs. 5.1 months;P= 0.0008)[75]. On the basis of this trial, ivosidenib has been recently approved by the Food and Drug Administration (FDA)for adult patients with previously treated, locally advanced or metastaticIDH1-mutated iCCA, which represent around 13% of all CCA[76].
Multiple inhibitors ofFGFRisoforms 1-3 have shown activity in phase I/II clinical trials of advanced, pretreated, CCA withFGFR2translocations, including several ATP-competitive, reversible inhibitors(erdafitinib, infigratinib, pemigatinib, and derazantinib) and non-ATP competitive, covalent inhibitor(futibatinib)[24]. The panFGFRinhibitors BGJ398/infigratinib and ARQ087/Derazantinib showed meaningful clinical benefits in chemorefractory iCCA patients carryingFGFR2fusions in a phase II trial,with tumour stabilisation or regression achieved in the majority of patients. The ORR was 18.8% and 20.7%,respectively, and DCR 83.3% and 82.8%[77,78]. Infigratinib has recently received FDA approval for the treatment of chemoresistantFGFR2rearranged CCA. The FIGHT-202 study investigated theFGFR1-3inhibitor pemigatinib in 107 pre-treated CCA patients withFGFR2fusions, obtaining an impressive 37%ORR, with a median duration of response of 8.1 months, PFS of 7.0 months and mOS of 17.5 months[14,79].No activity was recorded for pemigatinib in tumours harbouring mutations ofFGFR2, making this approach specifically for the 10% of CCA withFGFR2genomic rearrangements. Despite the exciting result of the FIGHT-202 trial, the enthusiasm is slightly hampered by the single-arm design of the trial, which lacks randomisation. Nonetheless, FDA and the European Medicines Evaluation Agency have approvedpemigatinib in the second-line setting of CCA withFGFR2fusions based on the comparison with historical data. Indeed, mOS for aBTC patients treated with ASC or chemotherapy in second-line is 6 months, as highlighted in the ABC-06 and ClarIDHy trial. Even considering the better prognosis of iCCA patients[8],according to the subgroup analysis of the ABC trials, this is expected to be around 16 months from diagnosis, leaving an expected survival of <8 months from the starting of second-line treatment providing a mPFS of 8 months for first-line CisGem [Figure 3].FGFR2fusions are also known to be associated with a better prognosis with a higher number of patients being diagnosed at an early stage which justifies the difference in OS between patients with and withoutFGFR2rearranged CCA in a retrospective multiinstitutional American cohort. In this analysis of 377 patients, mOS from diagnosis was 37 monthsvs.20 months in patients withFGFR2-fused tumours (P< 0.01) compared to those without these genetic abnormalities[80]. Of note, 40% in theFGFR2-fused group underwent surgical resection, likely impacting these figures. Indeed, Javleet al.[81]demonstrated thatFGFR2-fused CCA undergoing second-line chemotherapy are not associated with better response with a PFS of 4.63 months, comparable to the
findings observed in the ABC-06. This is in line with the recent updates from the FIGHT-202 trial, which showed a remarkable impact of pemigatinib onFGFR2fused tumours with mOS of 30 months for those patients who achieved ORRvs. 13.7 months for patients who did not[82].
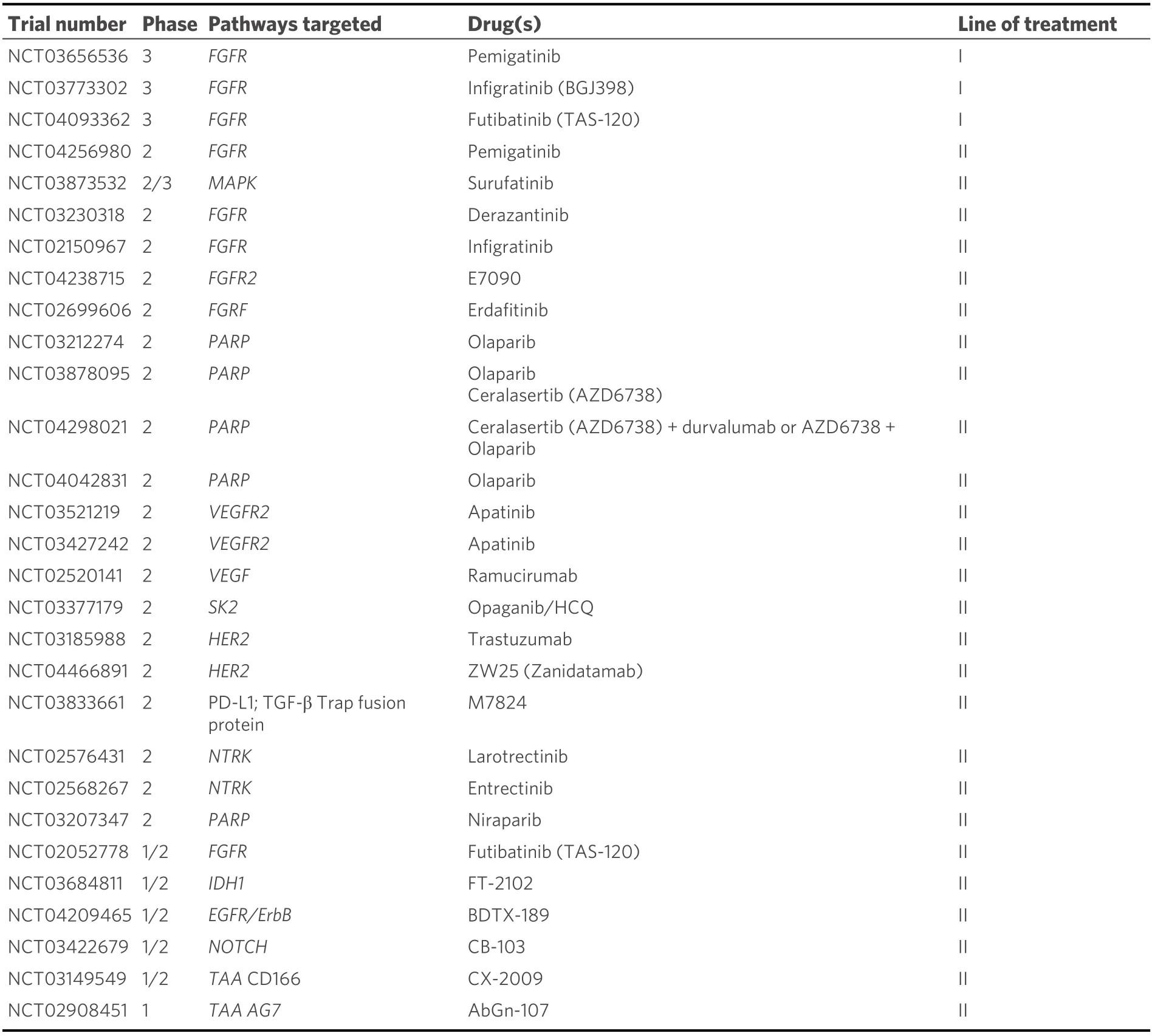
Table 3. Targeted therapies: ongoing clinical trials
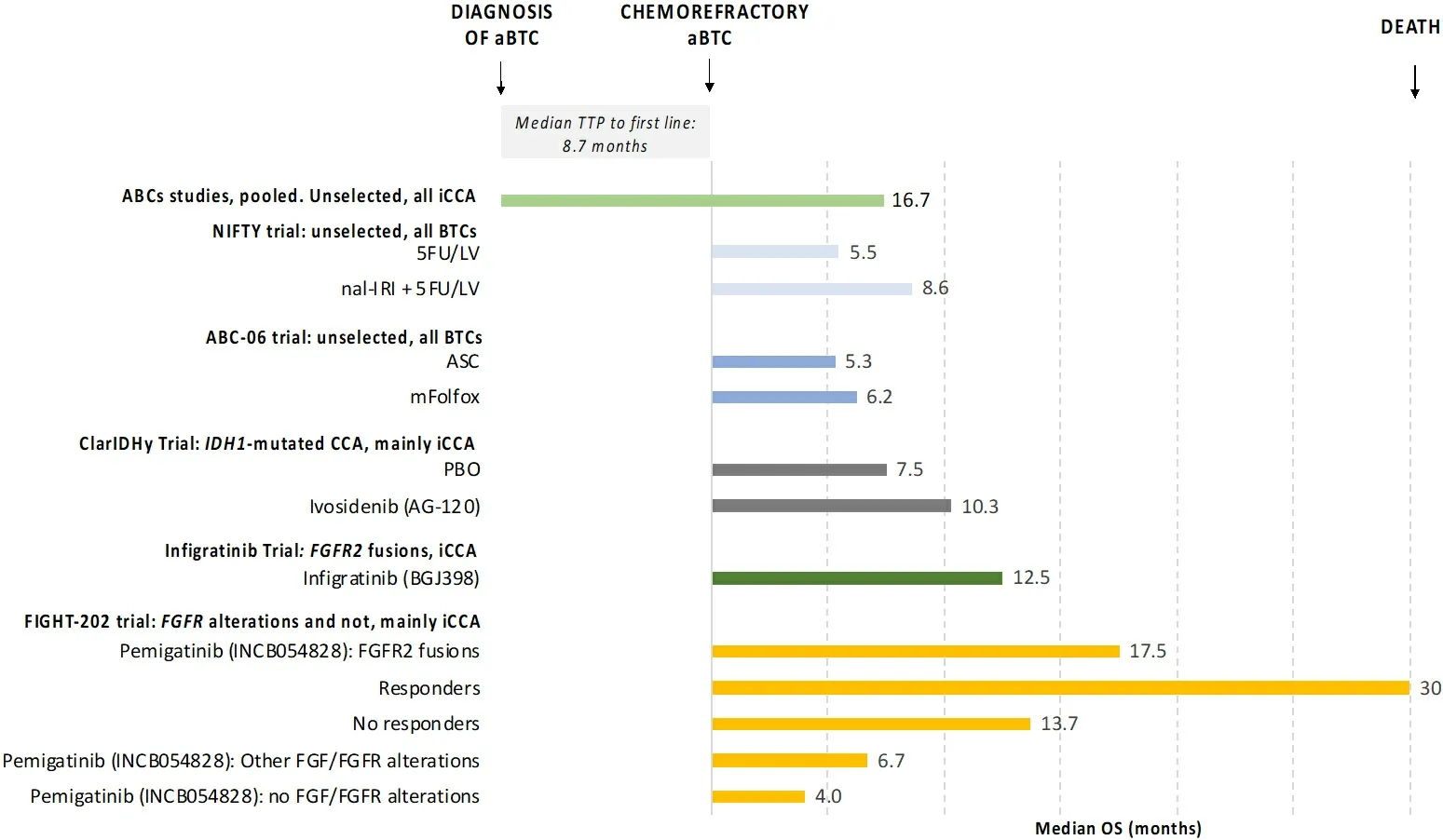
Figure 3. Overall survival of chemorefractory aBTC. Figure 3 shows overall survival (OS) of chemorefractory aBTCs from pooled analysis of ABCs studies and second line clinical trials. ABCs studies include ABC-01, -02 and -03 clinical trials which explored the role of first-line systemic chemotherapy in advanced BTCs [cisplatin and gemcitabine vs. gemcitabine (ABC-01 and ABC-02) and cisplatingemcitabine-cediranib vs. cisplatin-gemcitabine-placebo (ABC-03)]. ASC: Active symptom control; PBO: placebo; FGF: fibroblast growth factor; FGFR: fibroblast growth factor receptor; IDH-1: isocitrate dehydrogenase 1; CCA: cholangiocarcinoma; BTCs: biliary tract cancers; aBTCs: advanced biliary tract cancers; 5FU/LV: 5-fluorouracil plus leucovorin; nal-IRI: fluorouracil and liposomial irinotecan;mFOLFOX: 5-fluorouracil plus oxaliplatin.
On the basis of the data described above, FGFR2 inhibitors have now become the standard of care for chemorefractory CCA withFGFR2genomic rearrangements. As their use increase in clinic, we are called to face other challenges. First, it is a common observation to notice secondary resistance with FGFR2 inhibitors. According to data by Goyalet al.[83], resistance seems to be associated withde-novo FGFR2mutations. The development of the second generation of FGFR2 inhibitors is ongoing to address this issue.Futibatinib, a highly selective irreversible FGFR1-4 inhibitor, seemed to be effective to overcome resistance,likely due to an effective target engagement due to its covalent binding to the FGFR2 kinase[84]. Futibatinib is currently tested in the phase II FOENIX-CCA2 trial in chemoresistantFGFR2fused CCA and showed promising preliminary results (ORR = 34%, DCR = 76%, median duration of response 6.2 months)[84]. The next steps would be to increase the specificity of drugs to theFGFR2isoform to prevent side effects such as hyperphosphatemia and identify biomarkers for patients’ selection. Sub-analysis of the FIGHT-202 showed that co-occurrence of TP53 is associated with lack of response (ORR 0%vs. 45% inTP53-mutatedvs.TP53-wild type tumours), raising the question of whether FISH for identification ofFGFR2fusion is too limited for an optimal selection of patients[85].
Currently, results from randomised controlled phase III trials recruiting patients withFGFR2-fusions/rearrangements that compare the standard of care (CisGem) with different FGFR inhibitors in firstline setting are awaited (pemigatinib, NCT03656536; infigratinib, NCT03773302; futibatinib,NCT04093362)[9].
The whole plethora of FGFR-targeted therapies, characterised by different mechanisms of action, offers a unique opportunity for a paradigm shift in the treatment of a subgroup of patients with advanced BTCs,providing the potential for personalised treatment with active compounds and a sequential approach to be investigated in the next future. The challenge of primary and secondary resistance limits the efficacy of this class of drugs[83-85]. Exploring the potential of combining FGFR inhibitors with other treatments able to target signalling shared by wild-type and resistant tumour cells may help prevent the emergence of resistance mutations. This strategy stands on the biological rationale that blocking a driver kinase is more efficacious when downstream pathway components are targeted as well[86,87].
Expanding precision medicine in aBTCs: challenges and opportunities
Despite the opportunity to improve treatment and outcomes in a personalised manner, a major challenge,consisting in the design (and conduction) of adequately powered clinical trials in small patient subgroups,limits a rapid and effective drug development process based on traditional clinical trials design. However,the advent of precision medicine has been followed by novel clinical trial models to identify biomarkermatched subgroups of patients likely to benefit from specific targeted therapies, independently from histology. The overall objective of this innovation is to answer multiple questions at the same time and more efficiently in order to accelerate clinical drug testing and approval. In this light, novel strategies such as platform studies with adaptive designs which consider innovative endpoints may represent a potential opportunity to advance the precision drug development process in rare tumours such as BTCs. Recently,basket trials have been developed to investigate the efficacy of molecular-targeted therapy for similar oncogene-defined subgroups across different tumour types[88].
The activity of theBRAF V600kinase inhibitor vemurafenib has been explored in a basket trial enrolling 120 patients with refractoryBRAFmutated cancers. In the BTCs patient cohort, vemurafenib monotherapy showed 62% of DCR[89].
Another phase II basket trial of the BRAF inhibitor dabrafenib in combination with the MEK inhibitor trametinib in multiple refractory tumour types withBRAFV600Emutation showed ORR in 51% (22/43) of patients with BTCs[90]. Common treatment-related adverse events included pyrexia, rash, and nausea. The most common grade 3 or worse adverse event was increased γ-glutamyltransferase in five (12%) patients.No treatment-related deaths were reported. Further investigation in larger trials is warranted to confirm these early promising results.
A similar experience included 251 patients with 35 different advanced refractory tumour types with alterations inHER-2,EGFR,BRAF, and Hedgehog pathway, who were treated with pertuzumab plus trastuzumab, erlotinib, vemurafenib, or vismodegib, respectively[91]. In the small BTCs cohort (n= 7),HER-2 targeted therapy (trastuzumab plus pertuzumab) resulted in objective response in two patients while three patients experienced durable response (disease stability > 6 months)[91].
In another basket trial of patients withHER-2orHER-3mutations treated with neratinib, 2/9 patients of the BTCs cohort experienced partial response[90].Basket trials have also demonstrated the clinical activity of tropomyosin receptor kinase (TRK) inhibitors inTRKfusion-positive cancers. Entrectinib and Larotrectinib are potent, highly selective inhibitors of tropomyosinTRK A,B, andC, which has been shown promising results with RR up to 75% inNTRKgene fusion-positive advanced solid tumours, including BTCs, in early-phase trials[90]. The long duration of response (10 months for entrectinib and not reached for larotrectinib), and the good tolerability, led to expedite approval from the FDA in 2018 and 2019 for larotrectinib and entrectinib for patients with histology-agnostic solid tumours harbouringNTRKfusions. Although present in a small percentage of BTCs patients (3%-5%),NTRKfusion constitutes a promising therapeutic target to further investigate in this disease. NTRK inhibitors are currently being explored in clinical studies, which include advanced BTCs(NCT02576431, NCT02568267).
The above-mentioned studies demonstrate that histology-independent, biomarker-driven trials are feasible and represent a potential tool for developing targeted therapies for small - molecularly selected - patient subgroups of refractory cancers, thus constituting a unique opportunity to advance the paradigm shift from unselected to genome-driven oncology. However, major efforts are necessary to expand biomarker-directed clinical trials that are adequately powered for small groups of patients with a wide range of potentially actionable genetic aberrations.
In this context, several studies based on tumour sequencings such as TAPUR (NCT02693535) and MATCH(NCT02465060) trials are investigating the clinical activity of a series of compounds in patients with advanced solid tumours, including BTCs. The rationale is that patients with genetic abnormalities (such as mutations, amplifications, or translocations) may benefit from treatments matching the genetic profile that are either in clinical trials or already approved for the treatment of other cancer types.
Immunotherapy
Immunotherapy based on monoclonal antibodies targeting the immune checkpoint regulators such as cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) or programmed death ligand 1 (PD-L1), has emerged as a promising therapeutic strategy for several tumour types, including melanoma, non-small cell lung cancer, urothelial carcinoma, renal-cell carcinoma, head and neck cancer,and hepatocellular carcinoma[92]. In contrast, this strategy was associated with modest efficacy in unselected patients with aBTCs[93,94]. The only FDA-approved immunotherapy in BTCs is pembrolizumab, an anti-PD-1 antibody, which received tissue-agnostic approval for the treatment of advanced solid tumours with DNA mismatch repair deficiency (dMMR) or microsatellite instability (MSI), including those of the biliary tract (< 3% cases)[95].
The safety and activity of Pembrolizumab in patients with aBTCs have been investigated in the phase 1b multicohort study KEYNOTE-028 (NCT02054806) and the phase 2 multicohort study KEYNOTE-158(NCT02628067), respectively[96]. PD-L1 positive tumours were required for eligibility in KEYNOTE-028 only. These two studies demonstrated that pembrolizumab monotherapy provides durable antitumor activity in 6% to 13% of patients with advanced BTC, regardless of PD-L1 expression, and has a manageable toxicity profile. In KEYNOTE-028, ORR was 13% (3/23), mOS and mPFS were 5.7 and 1.8 months. In KEYNOTE-158, ORR was 5.8% (6/104), mOS and mPFS were 7.4 and 2 months. ORR was 6.6% (4/61) and 2.9% (1/34) among PD-L1-expressers (n= 61) defined by using a threshold of ≥ 1% of tumours cells or infiltrating lymphocytes expressing PD-L1, and PD-L1-nonexpressers (n= 34), respectively[96]. Whether this improved ORR translates into improved longer overall survival in patients with PD-L1-negative tumours remains unclear.The overall disappointing results achieved with ICIs monotherapy in BTCs compared to other tumour types can be explained by their biological features. BTCs are characterised by “cold” TME that lacks dendritic cells and effector T cells, essential for an effective immunomodulatory activity[97,98]. A different TME/immune cell infiltrate may also explain the higher sensitivity to ICIs observed in patients with hepatocellular carcinoma[99].
The only subgroup of patients with higher sensitivity to ICIs is that with dMMR/MSI high, as already mentioned. This genomic alteration represents the only potential biomarker that can predict the activity of this class of drugs identified to date. In the BTC cohort of 22 patients enrolled in the KEYNOTE-158 phase II study evaluating pembrolizumab in previously-treated patients with advanced non-colorectal dMMR/MSI high cancer, the ORR was 40.9% (including complete response in 2 patients), mPFS 4.2 months, and mOS 24.3 months[100]. The biological explanation of these results is that cancers with dMMR/MSI high (either due to inherited germline variants or epigenetic inactivation of MMR genes) are associated with a high degree of somatic mutations and have peculiar biological characteristics such as increased expression of neoantigens, abundant tumour-infiltrating lymphocyte (TIL), and high tumour mutational burden (TMB) that stimulate the immune checkpoint axis. Beyond dMMR/MSI-H, TMB is emerging as an additional predictive biomarker for PD-1/PD-L1 immune checkpoint inhibitors. A wholeexome-sequencing study of paired tumour/normal BTCs showed that 6% (14/239) were defined as high TMB using a threshold of > 11.13 Δ/Mb, which corresponded to a median of 641 non-silent mutations in this subset of hypermutated tumours. Hypermutation was associated with concurrent MMR deficiency and/or MSI in about 36% of cases[57].
Given to poor results achieved with immune checkpoint inhibitors monotherapy, combinatorial strategies to enhance the efficacy of this class of drugs in patients with BTCs are currently under clinical investigation.One promising approach is represented by immunotherapy-chemotherapy combination. The anti-PD-1 nivolumab has been associated with CisGem chemotherapy in phase II clinical trials. The association resulted in 37% ORR and mPFS and mOS of 4.2 and 15.4 months[101]. Phase III studies aimed at assessing the clinical efficacy of this therapeutic opportunity are currently ongoing, including the TOPAZ-1 and KEYNOTE-966, in which patients are randomised towards receiving CisGem alone or in combination with the anti-PD-L1 durvalumab or and PD-1 pembrolizumab, respectively. A phase II trial is investigating the activity of the triplet combination of durvalumab, tremelimumab (anti-CTLA-4), and paclitaxel(NCT03704480).
The inhibition of the transforming growth factor β (TGF-β) pathway has shown promising preliminary results. Bintrafusp alfa (M7824) is a first-in-class bifunctional fusion protein composed of the extracellular domain of the transforming growth factor (TGF)βRII receptor (a TGF-β trap) fused to a human IgG1 monoclonal antibody blocking PD-L1. It has been tested in an expansion cohort from a phase 1 study(NCT02699515), including 30 patients with advanced refractory BTCs. The ORR by central assessment was 20%, mPFS was 2.6 months and mOS 12.7 months[99]. However, despite initial enthusiasm, results from recent phase II clinical trials showed disappointing results in first- and second-line settings. Single-agent bintrafusp alfa demonstrated efficacy, durability, and an acceptable toxicity profile when used in patients with locally advanced or metastatic BTC who failed or were intolerant to frontline chemotherapy platinumbased chemotherapy, according to recent data from the phase 2 INTR@PID BTC 047 trial (NCT03833661).After more than 9 months of follow-up, the independent review committee adjudicated an ORR of 10.1%(95%CI: 5.9%-15.8%). Despite the benefit showcased, the trial did not meet the predefined threshold that would have allowed for regulatory filing for the agent’s use in the second-line treatment of BTC[102].Bintrafusp alfa was also under investigation in combination with CisGem in the frontline treatment of patients with BTC as part of the phase 2/3 INTR@PID BTC 055 trial (NCT04066491). However, due to disappointing preliminary results, the trial has been recently discontinued[103].
Immune checkpoint inhibitors have also been tested in association with anti-angiogenic drugs. However,results in BTCs were not satisfactory, in contrast with high efficacy observed in hepatocellular carcinoma[99].Pembrolizumab plus ramucirumab, anti-vascular-endothelial growth factor, showed limited efficacy in patients with previously treated aBTC, with a mOS of 6.4 months and mPFS of 1.6 months[104]. Data from the ongoing IMbrave-151 phase II trial are awaited to assess the role of the combination of CisGem chemotherapy with Atezolizumab plus/minus Bevacizumab in the first-line setting (NCT04677504).
In conclusion, the efficacy and safety of immunotherapies for BTC are still unclear. ICIs monotherapy has limited efficacy in unselected patients, while the combinations of ICIs and chemotherapies/targeted therapies seem to achieve better results. However, further clinical trials are necessary to find the optimal combination strategy and identify the predictive biomarkers for improved treatment selection. Table 4 shows a selection of ongoing clinical trials exploring ICIs.
Targeting the TME
For many tumour types, targeting the TME is an attractive therapeutic strategy in BTCs. High heterogeneity of TME both at the molecular and the cellular level has been demonstrated through multi-omics studies,and different clinically relevant subtypes of BTCs have been suggested based on TME specific characteristics[72,105,106]. This increasing knowledge has led to the identification of possible therapeutic strategies targeting several cell types and/or signalling pathways of the TME. In addition to treatments targeting the immune cell infiltrate (already discussed above), many others addressed towards different components of the TME have been recently proposed. In particular, their association with cytotoxic chemotherapy and tumour cells targeted therapies represents a promising opportunity[107].
BTCs are characterised by significant desmoplastic reactions orchestrated by stromal cells, and different types of immune cells infiltrate. The complex TME ecosystem is populated with a wide variety of cells,including cancer cells, cancer-associated fibroblasts (CAFs), myeloid-derived suppressor cells, tumourassociated macrophages (TAMs), TILs, tumour-associated neutrophils, natural killer cells, and many others[108,109]. TME has a significant role in shaping a chemoresistant phenotype. On the one hand, it constitutes a barrier that obstacles drug delivery; on the other, TME cells interact in dynamic crosstalk with components of the extracellular matrix (ECM), soluble factors - including cytokines, chemokines, growth factors - and biliary tumour cells to modulate chemo-resistance and drive tumour progression[110-112]. From a therapeutic point, the most interesting cells are CAFs and TAMs.
CAFs are a heterogeneous group of cells characterised by the expression of alpha-smooth muscle actin and platelet-derived growth factor receptor beta. They are the key protagonists in the TME of BTCs and have a pivotal role in ECM composition and crosstalk with cancer cells through the secretion of TGF-β, stromal cell‐derived factor 1, hepatocyte growth factor, connective tissue growth factor, epidermal growth factor and platelet-derived growth factor[108]. CAFs are first recruited by CCA tumour cells which subsequently exert positive feedback and amplify their activity. Once activated, CAFs promote CCA progression.
TAMs and exerts a key role in cancer-related inflammation by promoting tumour-cell proliferation,angiogenesis, matrix turnover and suppression of the adaptive immune response[113]. TAMs create a favourable niche by interacting with biliary cancer cells and other stromal cells via releasing multiple protumour factors (including IL-4, IL-6 and IL-10, CCL17, CCL18, and MMP9) that ultimately sustain
CCA growth. In addition, TAMs exert immunosuppressive and chemoresistant effects.
Several therapeutic strategies targeting TME and associated cell types showed promising preclinical activity.Navitoclax (Bcl-2 inhibitor) was shown to induce apoptosis in CAFs leading to decreased ECM and stroma deposition and tumour sizein vivousing rat xenograft models transplanted with rat CCA cell line BDEneu cells[114]. Similarly, 1D11, a monoclonal antibody targeting TGF-β, demonstrated the ability to inhibit TGF-β,decrease fibrogenesis, ECM deposition, and CCA development in rats[115].
WNT pathway is important for CCA progression and growth, and its activation is maintained by inflammatory macrophages in the tumour stromain vivo. Mouse and rat CCA models demonstrated that depletion of TAMs or inhibition of WNT signalling with one of two small molecules significantly reduces tumour proliferation and increased apoptosis, resulting in tumour regression[115].TWEAK/Fn14 pathway is also increasingly expressed in CCA. It not only supports tumour proliferation but also modulates migration and polarisation of TME cells, including macrophages and CAFs. The pharmacological inhibition of TWEAK/Fn14 and of its downstream signals significantly reduced CCA xenograft growth, inflammation and fibrosis, while TWEAK overexpression drove cancer-associated fibroblast proliferation and collagen deposition in the tumour niche in preclinical models[115].
These preliminary studies indicate that targeting TME is a promising therapeutic strategy to further investigate in clinical trials.
Other potential therapeutic targets on the horizon
In addition to those discussed in the previous sections, many other potential targets include DNA damage response (DDR),METaberrations, PI3K/AKT/mTOR signalling pathway, and chromatin remodelling gene alterations (ARID1,BAP1andPBRM1).
DDR can be found in up to 60% of BTCs and may offer several therapeutic advantages with PARP inhibitors (PARPi)[116,117]. Inactivation ofBRCA1andBRCA2genes is the most frequent event associated with DDR[118]. In a retrospective multicentric study, Golanet al.[119]demonstrated that 4/18 CCA patients withBRCApathogenic variants (somatic or germline) treated with PARPi achieved a favourable response in first or subsequent lines, of whom one experienced sustained disease response with a PFS of 42.6 months.The 44% of patients (8/18) had a previous personal or a family history ofBRCA-associated cancer (breast,ovarian, prostate and pancreatic cancer).
Several PARPi are currently being investigated in BTCs patients, including olaparib, rucaparib, and niraparib, as single agents or associated with other strategies [Table 3]. In particular, the combination of PARPi and IDH1 inhibitors or ICIs is based on the preclinical rationale of potential synergistic activity.Mutations inIDHgene are shown to significantly decrease homologous recombination repair activity by inhibiting the αKG-dependent dioxygenases, therefore enhancing the sensitivity to PARPi[120]. Ongoing clinical trials are exploring the efficacy of PARPi inIDH1/2mutant iCAA in order to assess their synthetic lethality and to targetIDH1/2-related dependencies (NCT03212274, NCT03878095).
Treatment with PARPi has also been associated with increased genomic instability, immune pathway activation, and PD-L1 expression on cancer cells, which might promote responsiveness to ICIs[121].
Highc-Metexpression andMETamplifications are described in up to 16% and 7% of BTCs, respectively[122].Cabozantinib is a multi-kinase inhibitor ofMET, already approved for the treatment of advanced renal cell and thyroid carcinoma[123]. It showed limited activity and significant toxicity in a study of 19 unselected,previously treated, BTCs patients with a mPFS and mOS of 1.8 (95%CI: 1.6-5.4) and 5.2 (95%CI: 2.7-10.5)months, respectively[124]. However, the administration of this agent-based on molecular selection may be more effective.
Mutations in the PI3K/AKT/mTOR signalling pathway have been described in 40% of eCCA and 25% of iCCA (25%)[125,126]. Preclinical studies have shown activity of PI3K/AKT/mTOR inhibition in BTCs,suggesting that this therapeutic strategy may have clinical utility for a subset of BTCs harbouring aberrations in this pathway[125]. However, despite initial enthusiasm from clinical studies with rapamycin analogues, showing interesting activity with an acceptable toxicity profile, novel strategies exploring AKT and PI3K inhibitors have raised serious safety concerns, highlighting the need for improved patient selection and increased target specificity for the clinical development of these agents[126]. Several ongoing trials are currently investigating the combination (or sequential approach) of AKT-mTOR inhibitors or PI3K-mTOR inhibitors plus chemotherapy (NCT02465060, NCT02836847, NCT02631590).
Lastly, numerous chromatin-modifying enzymes are frequently mutated or altered by copy number aberrations in BTCs. Blocking these targets when found dysregulated represent a compelling strategy to explore in BTCs[54,127,128]
CONCLUSION
Overall, BTCs constitute a neglected disease for which novel therapeutic strategies are urgently needed.After years of “one-size fits all” approach, characterised by a series of failures in improving patient outcomes with only marginal progress made thanks to the allocation of first-line chemotherapy, we are now witnessing the dawn of a new era based on molecularly driven decision making. The current standard therapeutic portfolio includes chemotherapy in first-line (CisGem) and second-line for unselected patients(FOLFOX); patients with molecular aberrations (IDHmutations,FGFRfusions, MSI high) can be treated with targeted therapies or pembrolizumab following progression to frontline chemotherapy [Figure 1].
Despite currently being limited to small patient subgroups, “precision medicine” for BTCs is possible - and desirable - given the numerosity of ongoing biomarker-based/enriched clinical trials and potential therapeutic vulnerabilities recently identified, both in the tumour and in the immune-microenvironment.To reach this ambitious goal, a revolution in patient management is much needed. Large-scale efforts to implement tumour’s molecular characterisation at diagnoses with a rapid translation of information to clinical research, in addition to expanding clinical trials (and trial enrolment), should be a health priority.Implementing liquid biopsy studies will be a crucial step to facilitate sample collection for biomarker discovery, treatment monitoring, and disease surveillance in BTCs. In parallel, enhanced preclinical research will be essential to the identification of predictive biomarkers and to the elucidation of mechanisms of primary and acquired resistance. Multi-omics studies and international collaborations are also fundamental to accelerate the precision therapeutic development in this aggressive disease.
DECLARATIONS
Authors’ contributions
Conception and design of the study: Braconi C, Casolino R
Drafting the manuscript: Casolino R
Review of the manuscript: Braconi C
Approval of the final version of the manuscript: Casolino R, Braconi C
Availability of data and materials
Not applicable.
Financial support and sponsorship
Braconi C is a recipient of the Lord Kelvin Adam Smith Readership from the University of Glasgow.
Conflicts of interest
Braconi C (or spouse) received honoraria from Incyte, Bayer, Eli-Lilly, Pfizer, Merck-Serono.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2021.