
Clinical efficacy and safety of second line and salvage aflibercept for advanced colorectal cancer in Akita prefecture
2021-04-25 01:43:30TaichiYoshidaKentaroTakahashiKengoShibuyaOsamuMutoYukoYoshidaDaikiTaguchiKazuhiroShimazuKojiFukudaFuminoriOnoKyokoNomuraHiroyukiShibata
Taichi Yoshida,Kentaro Takahashi,Kengo Shibuya,Osamu Muto,Yuko Yoshida,Daiki Taguchi,Kazuhiro Shimazu,Koji Fukuda,Fuminori Ono,Kyoko Nomura,Hiroyuki Shibata
Taichi Yoshida,Daiki Taguchi,Kazuhiro Shimazu,Koji Fukuda,Hiroyuki Shibata,Department ofClinical Oncology,Akita University Graduate School of Medicine,Akita 010-8543,Japan
Kentaro Takahashi,Department ofGastroenterological Surgery,Nakadori General Hospital,Akita 010-8577,Japan
Kengo Shibuya,Department ofGastroenterology,Akita Kousei Medical,Akita 010-0948,Japan
Osamu Muto,Yuko Yoshida,Department ofMedical Oncology,Akita Red Cross Hospital,Akita 010-1495,Japan
Fuminori Ono,Department ofSurgery,Omagari Kousei Medical Center,Akita 014-0027,Japan
Kyoko Nomura,Department ofEnvironmental Health Science and Public Health,Akita University Graduate School of Medicine,Akita 010-8543,Japan
Abstract BACKGROUND Angiogenesis inhibitors(AIs)combination with cytotoxic chemotherapy is a promising treatment for patients with colorectal cancer(CRC).Aflibercept(AFL)is an option for second-line treatment of CRC,according to the ‘VELOUR' trial.Currently,we can choose from three AIs,including bevacizumab,ramucirumab,and AFL.Different AIs can be used in subsequent treatment because of their distinctive mechanisms of action.We addressed the uncertainty regarding AFL efficacy and safety in heavily-treated patients by comparing outcomes of survival treatment with second-line treatment.AIM To determine and compare the efficacy and safety profiles of AFL in the secondline and salvage therapy settings.METHODS Clinical data of 41 patients with advanced CRC who received intravenous AFL combined with the folinic acid-fluorouracil-irinotecan(FOLFIRI)regimen were collected retrospectively from six institutions in Japan,for the period from May 2017 to March 2019.Patient characteristics collected included age,sex,tumor location,RAS and RAF status,metastatic sites,number of previous treatment cycles,therapeutic response,adverse events,duration of previous AI treatment,and survival time.The end points were time to AFL treatment failure(aTTF)and median survival time post-AFL(aMST).Statistical analyses were performed to compare the efficacy and safety in the second-line setting with those of the salvage therapy setting,which was defined as the days since the end of secondline therapy.RESULTS All 41 patients who received AFL + FOLFIRI for advanced CRC had metastatic or unresectable cancer.Twenty-two patients received AFL in the second-line setting and nineteen in the salvage therapy setting.The patient characteristics were similar in the two groups,except for two factors.The median duration of the previous AI administration was shorter in the second-line patients compared with that in the salvage therapy patients(144 d vs 323 d,P = 0.006).In the second-line and salvage therapy groups,the objective response rates were 11% and 0%,respectively(P = 0.50),and the disease control rates were 53% and 50%,respectively(P = 1.00).In the second-line and salvage therapy groups,the aTTF(123 d vs 71 d,respectively),aMST(673 d vs 396 d,respectively),and incidence of adverse events of grade 3[8(36%)vs 9(47%)]were not significantly different between the two groups.CONCLUSION AFL can be used to treat advanced CRC patients,with a similar safety and efficacy in the salvage therapy setting as in the second-line setting.
Key Words:Colorectal cancer;Aflibercept;Second-line chemotherapy;Folinic acidfluorouracil-irinotecan;Palliative chemotherapy;Observational cohort study
INTRODUCTION
Colorectal cancer(CRC)is the second leading cause of cancer-related death globally[1].In Japan in 2017,more than 130000 people were newly diagnosed with CRC and more than 50000 patients died of this disease[2,3].Surgery and endoscopic resection are currently the only curative therapies for CRC.Patients with unresectable metastatic CRC are given chemotherapy;also considered a standard-of-care chemotherapy for unresectable metastatic CRC are the angiogenesis inhibitors(AIs)[4-7].
Three Ais-bevacizumab(Bmab),ramucirumab(Rmab),and aflibercept(AFL)-have been used recently in the second-line setting[8-10].AFL is a recombinant fusion protein containing vascular endothelial growth factor(VEGF)-binding portions from the extracellular domains of human VEGF receptors 1 and 2,which are fused to the Fc portion of human immunoglobulin G1.AFL blocks the activity of VEGF-A,VEGF-B,and placental growth factor by acting as a high-affinity ligand trap to prevent these ligands from binding to their endogenous receptors[11,12].In the ‘VELOUR' trial,a survival benefit was demonstrated when AFL addition to the folinic acid-fluorouracilirinotecan regimen(FOLFIRI)was compared with placebo and FOLFIRI alone[10].However,no means of choosing among the three AIs in the second-line setting has been established because of the absence of direct comparisons.
As the three AIs have their own mechanisms for inhibiting the VEGF pathway,it is quite natural to use all in series for treatment of CRC.It is uncertain,however,whether AFL is effective and safe in heavily-treated patients.Therefore,we compared the efficacy and safety of AFL used in salvage therapy with those during its use in secondline treatment.For this purpose,we organized the All Akita Aflibercept(AAA)group,which included the following six institutions in Japan:Omagari Kousei Medical Center,Akita Kousei Medical Center,Akita City Hospital,Nakadori General Hospital,Japanese Red Cross Akita Hospital,and Akita University Hospital in Akita.
MATERIALS AND METHODS
Study design and patients
Clinical data of patients with advanced CRC treated with AFL as second-line or later treatments were retrospectively collected by the AAA group for the period from May 2017 to March 2019.Patients' information collected included age,sex,primary tumor location,RASandBRAFstatus,metastatic sites,complications,cycles of prior chemotherapies,therapeutic drug types,treatment response,adverse events(AEs),duration of prior treatment with AIs,and survival time after initial AFL administration.We divided the patients into two groups:The first included patients treated with AFL in the second-line setting,and the second included patients treated with AFL as salvage therapy.Salvage therapy was defined as treatment after secondline therapy.
This study was conducted in accordance with the Declaration of Helsinki.The protocol was approved by the Institutional Review Board at Akita University in November 2018(#2070).Informed consent was not acquired from all participants,but information regarding this study and an opt-out option appeared on our institution's website(https://www2.hos.akita-u.ac.jp/chiken/info/pdf/20181122_2070.pdf).
Treatment
Patients received 4 mg/kg of AFL intravenously(IV)over 1 h on day 1 every 2 wk,followed by the FOLFIRI regimen(150 mg/m2of irinotecan IV over 90 min,with 200 mg/m2of levofolinate IV over 2 h,followed by 400 mg/m2of 5-fluorouracil bolus and 2400 mg/m2of 5-fluorouracil continuous infusion over 46 h)[10].Irinotecan was used at a dose of 180 mg/m2in the VELOUR trial but the approved dose in Japan is 150 mg/m2;we chose to use that dose in our study.Supportive care(e.g.,antiemetics,anticholinergics,etc.)as well as dose modification and discontinuation were conducted promptly.
Assessment
The investigators performed radiological assessment according to Response Evaluation Criteria in Solid Tumor(RECIST)version 1.1[13].The AEs were described according to National Cancer Institute Common Terminology Criteria for Adverse Events,version 4.03[14].
Statistical analysis
The cutoff date for the efficacy and safety analysis was June 18,2020.We investigated the differences in the patient characteristics between the two groups as follows:Qualitative variables were compared using Fisher's exact test,and quantitative variables with the Student'st-test.Time to AFL treatment failure(aTTF)was defined as the time from the first AFL administration date to the last.There were no censored data because all patients had discontinued AFL at the time of the analysis.The median survival time post-AFL(aMST)was defined as the time from the date of the first AFL administration to the date of death from any cause.Patients alive at the time of the analysis were censored at the date of the last follow-up.Subgroup comparisons according to the tumor location,RASstatus,duration of the prior AI administration,and liver metastasis,were conducted.We used the Kaplan-Meier method to calculate survival curves for each group and the log-rank test to perform the subgroup comparisons.An objective response rate was defined as the proportion of patients with either a complete response(CR)or a partial response(PR).The disease control rate was defined as the proportion of patients with a CR,PR,or stable disease.We used Spearman's correlation coefficient to analyze the relationships between aTTF and the predefined subgroups,such as age,sex,tumor location,liver metastases,lung metastases,treatment line,RASstatus,duration of the prior AI treatment,objective response,and disease control.All statistical analyses were performed with BellCurve for Excel(version 3.20).Pvalues less than 0.05 were considered to indicate statistical significance.
RESULTS
Patient characteristics
Data were collected from 41 patients,including 22 treated in the second-line setting and 19 treated as salvage therapy.Patient characteristics are summarized in Table 1.Most of the baseline characteristics were similar in the two groups.The median age was 61.5 years in the second-line group and 63 years in the salvage therapy group(P=0.16).The number of male patients was 12(55%)in the second-line group and 14(74%)in the salvage therapy group(P= 0.33).The number of patients with a left-side tumor was 14(64%)in the second-line group and 13(68%)in the salvage therapy group(P=1.00).The number of patients with liver metastasis was 15(68%)in the second-line group and 12(63%)in the salvage therapy group(P= 0.75).The number of patients with lung metastasis was 7(32%)in the second-line group and 8(42%)in the salvage therapy group(P= 0.53).The number of patients with other metastasis(e.g.,lymph node,bone,peritoneal,etc.)was 14(64%)in the second-line group and 11(58%)in the salvage therapy group(P= 0.76).The proportion of patients who had wild-typeRASCRC was lower in the second-line group compared with that in the salvage therapy group[4 of 22(18%)vs10 of 19(53%),respectively,P= 0.026].Further,the median duration of previous AI administration was shorter in the second-line group compared with that in the salvage therapy group(144 dvs323 d,respectively,P= 0.006).Nine patients each in the second-line and salvage therapy groups(41% and 47%,respectively)had complications,the most common of which were hypertension[n= 6(27%)and 1(5%),respectively],hyperlipidemia[n= 4(18%)and 2(11%),respectively],and diabetes mellitus[n= 2(9%)and 1(5%),respectively].
Therapeutic efficacy
Therapeutic responses were evaluated in 19 of 22 patients in the second-line group and 14 of 19 patients in the salvage therapy group(Table 2).No patient achieved CR in either group;two patients in the second-line group but none in the salvage therapy group achieved a PR,resulting in objective response rates of 11% and 0%,respectively(P= 0.50).Disease control was achieved in 10 patients(53%)in the second-line group and 7 patients(50%)in the salvage therapy group(P= 1.00).At the time of data cutoff,all patients had already discontinued AFL treatment and 13 patients had died.In the overall population,the aTTFs and aMSTs were 71 d[95% confidence interval(CI):45-97]and 456 d(95%CI:359-553),respectively.In the second-line and salvage therapy groups,the aTTFs were 123 d(95%CI:68-178)and 71 d(95%CI:64-78),respectively(P= 0.93;Figure 1A).The aMST was 673 d(95%CI:299-1047)in the second-line group and 396 d(95%CI:260-532)in the salvage therapy group(P= 0.22;Figure 1B).Subgroup analyses showed there were no significant differences between the two groups for any of the subgroups.
Safety
AEs of grade 3 occurred in 8 patients(36%)in the second-line group and 9 patients(47%)in the salvage therapy group.In the second-line group,the most common AE was neutropenia,which was observed in 3 patients(14%).In the salvage therapy group,the most common AEs were leukopenia,neutropenia,and peripheral sensory neuropathy,which were observed in 2 patients each(11% each).AI-related hypertension occurred in 2(9%)of the second-line patients and 1(5%)of the salvagetherapy patients.Proteinuria occurred in 1(5%)of the second-line patents and 2(11%)of the salvage therapy patients,and perianal abscess occurred in 1 patient in each group(both 5%)(Table 3).There was no significant difference in the incidence of AEs grade 3 between the two groups(P= 0.54).One patient died of febrile neutropenia in the second-line treatment group.
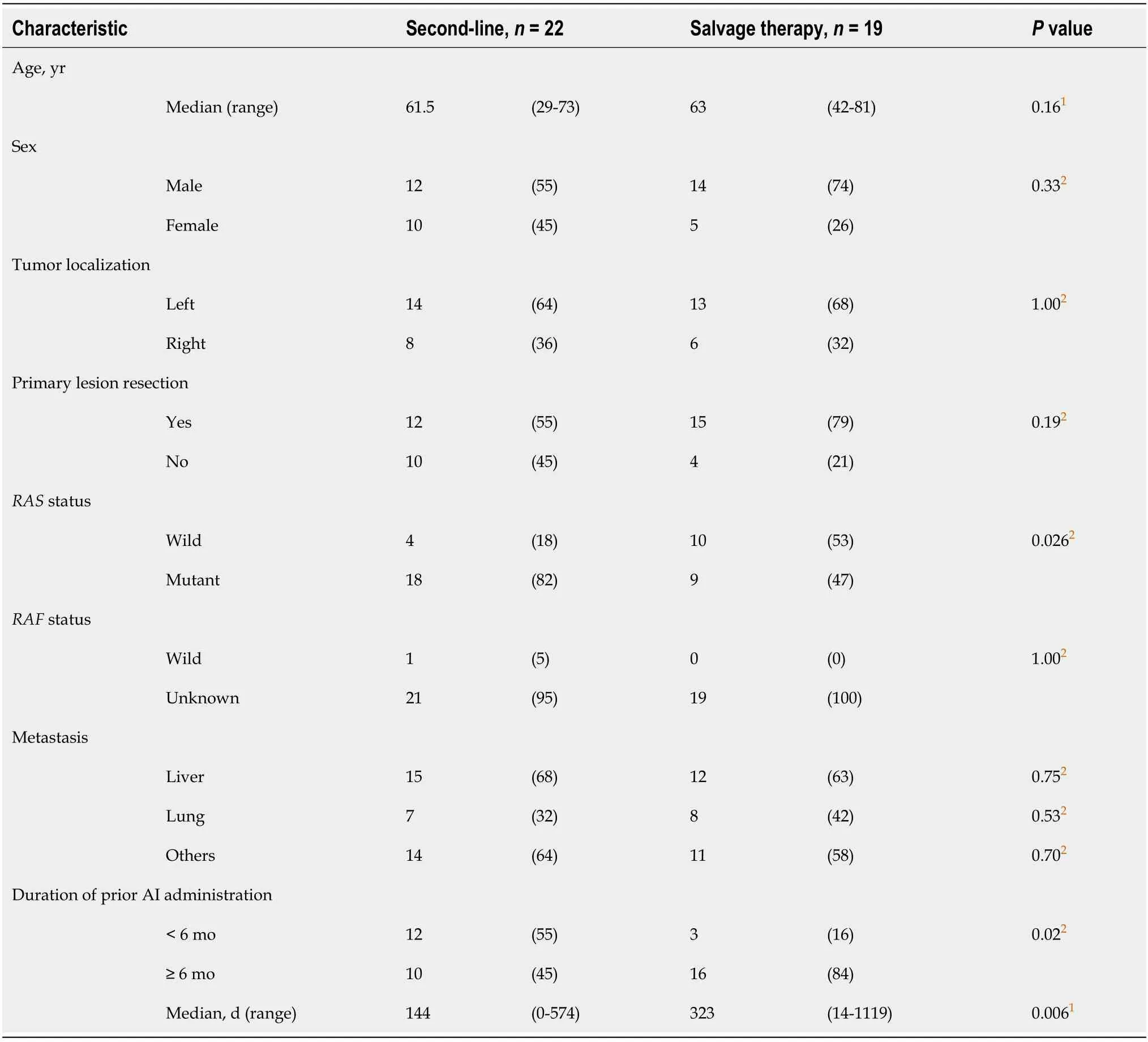
Table 1 Baseline patient characteristics
DISCUSSION
We investigated the efficacy and safety of ALF + FOLFIRI as salvage therapy and second-line chemotherapy.Actually,similar numbers of patients were treated in the salvage therapy and the second-line groups.We compared the therapeutic outcomes of this study with those of historical records.We could not examine the progressionfree survival(PFS),because it is measured from the date of randomization,but the AAA study was an observational study.Instead,we evaluated the aTTF,which was the time from the first date of AFL administration to the end.For this reason,the aTTF seems to be slightly shorter than the usual PFS.Nonetheless,the aTTF(4.1 mo)for thesecond-line therapy group in this study was much shorter than the median PFS(6.9 mo)in the VELOUR study.The participants in clinical trials tend to be more selected from the point of view of performance status and organ functions,as compared with patients treated in routine practice.Then,we evaluated the aMST,where the survival time was measured from the start of AFL treatment to death,instead of the usual MST.The aMST(22.4 mo)in the second-line group of the AAA study was much longer than the MST(13.5 mo)in the VELOUR trial.Although the number of participants in the AAA study was small,it is still evident that the survival benefit of AFL was exerted in routine clinical use.The aTTF(2.4 mo)in the salvage therapy group of the AAA study was much shorter than the median PFS(6.9 mo)in the VELOUR trial.This is quite predictable because it is a salvage setting.However,it was quite unexpected that the aMST(13.2 mo)with salvage therapy in the AAA study was comparable to the MST(13.5 mo)in the VELOUR trial.Of note,there were fewer participants in the AAA study than in the VELOR trial,but it might be possible that AFL has some survival benefits after resistance to other AIs.
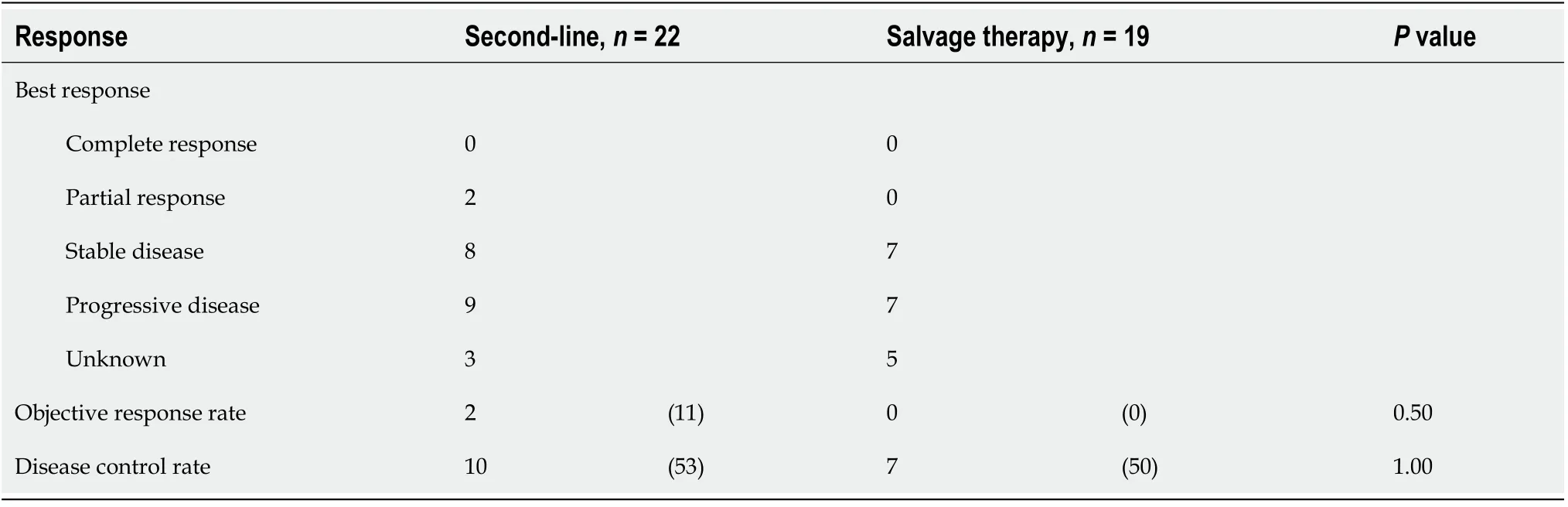
Table 2 Best response to treatment
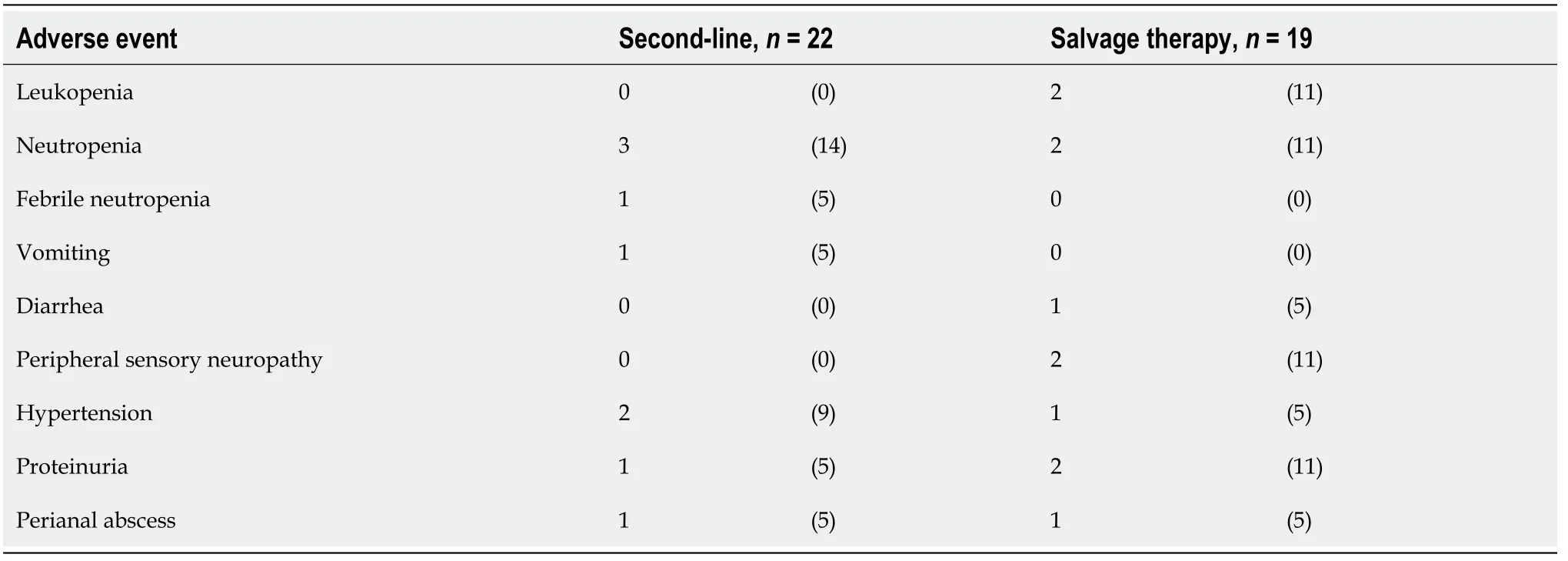
Table 3 Grade 3 or worse adverse events
The AAA study also indicated that AFL could be used for salvage therapy treatment of CRC with safety similar to that in the VELOUR trial.The most common grade ≥ 3 AE was neutropenia.The incidence was lower in our study(14% in the second-line group and 11% in the salvage therapy group)than that in the VELOUR trial(36.7%).Only 1 patient(5%)experienced febrile neutropenia in the second-line group.Hypertension(grade ≥ 3)was observed in 9% of the second-line group and 5% of the salvage therapy group.The incidence of grade ≥ 3 hypertension in previous trials,such as the AL18147,RAISE,VELOUR,E3200,and AXEPT,ranged from 2.0% to 19.3%[8-10,15,16].These incidences are quite comparable to our incidences in both the salvage and the second-line groups.Proteinuria(grade ≥ 3)was observed in 5% of the second-line group and 11% of the salvage therapy group in our study.The incidence in the second-line group in our study was comparable to the incidences of grade ≥ 3 proteinuria reported in previous trials,which ranged from 0.7% to 7.8%[8-10,15,16];however,the incidence in the salvage therapy group(11%)in our study was more frequent than previously reported.Proteinuria induced by AIs are difficult to manage.Proteinuria also is encountered more frequently as the length of exposure to AIs increases.That might be a reason for the higher incidence of proteinuria in the salvage therapy patients in our study.No grade ≥ 3 bleeding or hemorrhage in the gastrointestinal tract or in other lesion was observed.

Figure 1 KapIan-Meier curves of time of afIibercept treatment faiIure and median survivaI time post-afIibercept in the second-Iine and the saIvage therapy settings.A:Time to aflibercept treatment failure;B:Median survival time post-aflibercept.P values were calculated by the log-rank test.aTTF:Time to aflibercept treatment failure;aMST:Median survival time post-aflibercept.
We gathered the data in the literature including rather smaller number of patients as many as 20 patients,where the AIs were applied in the salvage setting(Table 4).There are two Rmab papers,three Bmab papers,and one AFL paper.We compared the efficacies(PFS and overall survival)and safety(the rate of the adverse events)with ours.There were no differences in the efficacy with 3 AIs in the salvage lines,but the Bmab was most safety among them,followed by AFL and Rmab in this order.
CONCLUSION
Currently,we have three AIs for the treatment of metastatic CRC,all of which have individual targets.For example,Bmab targets VEGF-A,and Rmab targets VEGF receptor 2,which receives VEGF-A,VEGF-C and VEGF-D signaling[17].However,it is difficult to determine differences between the treatment from the results of previous clinical trials.When we use the AIs sequentially,a different inhibitory mechanism from that of the previously used AI might exert a suppressive effect on the remaining tumor.Our observation might be a hint towards the sequential use of AIs.Actually,it was reported that the MST was 11.1 mo for patients who were treated with AFL in the third-line and 8.1 mo for those treated in the fourth-line[18].As our conclusion has been drawn from exploratory observation,it should be confirmed by a prospective study composed of a larger number of participants.In summary,AFL might be safe and confer a survival benefit in patients treated in later lines as well as in the second-line.
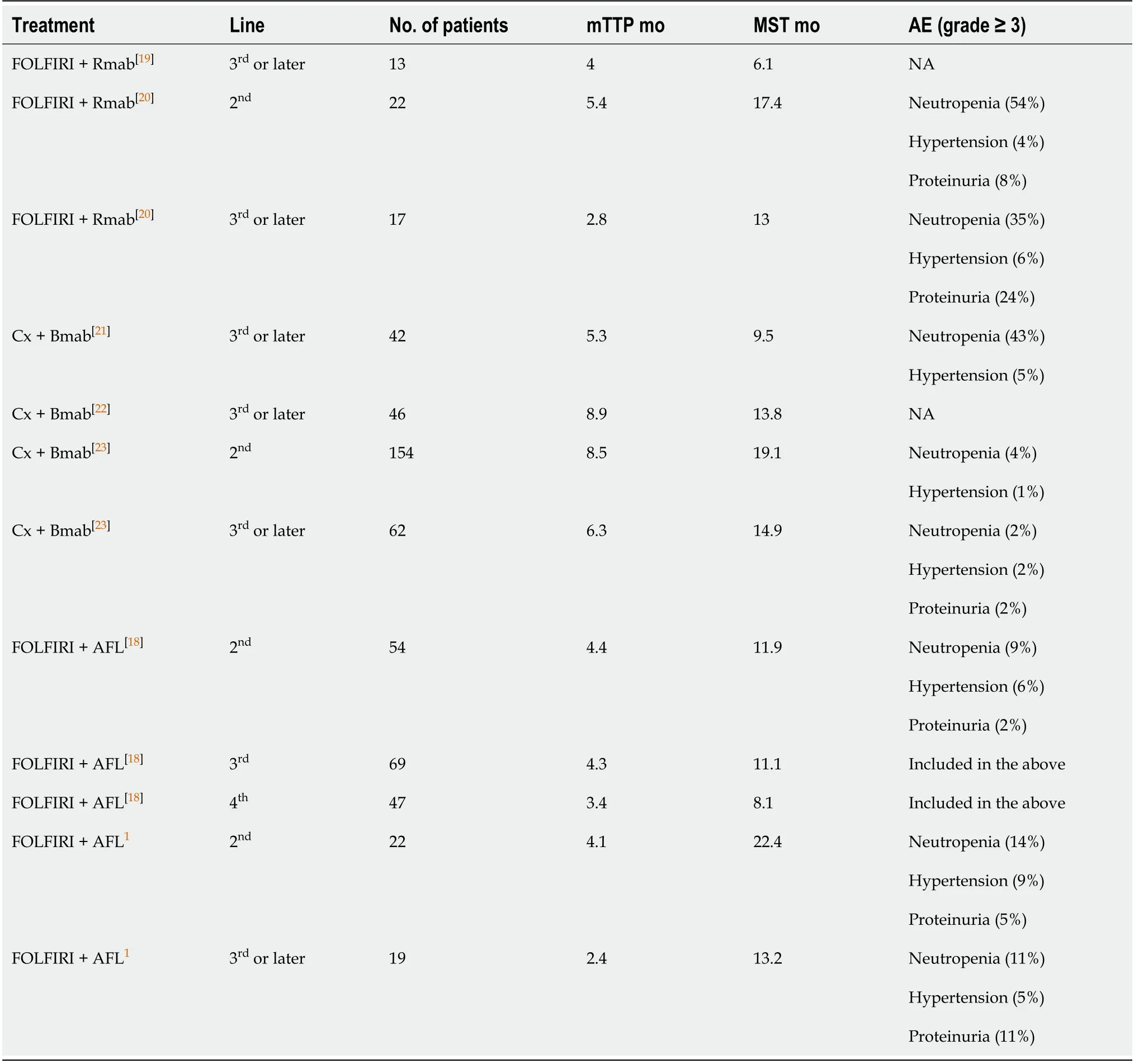
Table 4 summary of data from recent reports including salvage therapy with three angiogenesis inhibitors plus chemotherapy
ARTICLE HIGHLIGHTS
Research background
We usually use angiogenesis inhibitors(AIs)for chemotherapy in metastatic colorectal cancer(CRC).Aflibercept(AFL),one of the AIs,has been shown to be effective in second-line treatment by the ‘VELOUR' study.
Research motivation
We can choose three Ais-bevacizumab,ramucirumab,and AFL-for treating with second-line chemotherapy.No means of choosing among the three AIs has been established because of the absence of direct comparisons.
Research objectives
We researched whether AFL is a treatment option for second-line chemotherapy with CRC in the ordinary clinical setting in Akita,Japan.
Research methods
Medical records including age,sex,primary tumor location,RASandBRAFstatus,metastatic sites,cycles of prior chemotherapies,survival time after initial AFL administration,etc.were collected from each institution.We investigated the efficacy and safety for AFLviaa statistical approach.
Research results
Time to AFL treatment failure was 123 d in the second-line group and 71 d in the salvage therapy group.The median survival time post-AFL was 673 d in the secondline group and 396 d in the salvage therapy group.Adverse events of grade ≥ 3 occurred in 8 patients(36%)in the second-line group and 9 patients(47%)in the salvage therapy group.
Research conclusions
Our study indicated that the efficacy and safety was the same as in the VELOUR study and that AFL contributes survival benefit similarly in both the second-line and salvage therapy settings.Patients with unresectable metastatic CRC should consider receiving AFL,regardless of number of treatment cycles.
Research perspectives
AFL is a promising agent,along with chemotherapy,for CRC.Further study should verify whether AFL will be affected by sequential therapy;for example,investigating the particular regimen used as first-line therapy before AFL administration.
ACKNOWLEDGEMENTS
The authors would like to thank Sato Y and Ota S for their contributions to this study.
 World Journal of Gastrointestinal Oncology2021年4期
World Journal of Gastrointestinal Oncology2021年4期
- World Journal of Gastrointestinal Oncology的其它文章
- Crohn's disease with infIiximab treatment compIicated by rapidIy progressing coIorectaI cancer:A case report
- MuItinationaI survey on the preferred approach to management of Barrett's esophagus in the Asia-Pacific region
- Expression profiles of gastric cancer molecular subtypes in remnant tumors
- Predictive factors for early distant metastasis after neoadjuvant chemoradiotherapy in locally advanced rectal cancer
- Colorectal cancer screening in the COVID-19 era
- Nanotechnology and pancreatic cancer management:State of the art and further perspectives