
Tongue thickness in health vs cirrhosis of the liver: Prospective observational study
2020-12-18 05:31TandonSinghSinglaJainPandeyCK
Tandon M, Singh H, Singla N, Jain P, Pandey CK
Abstract
Key words: Sarcopenia; Malnutrition; Cirrhosis of the liver; Child Turcotte Pugh class;Model for end stage liver disease score; Ultrasonography
INTRODUCTION
Malnutrition has been estimated to affect 50%-90% of patients with cirrhosis of the liver[1].However, malnutrition is frequently overlooked, in part because nutritional assessment can be difficult in patients with cirrhosis due to fluid retention and because patients with cirrhosis may develop simultaneous loss of skeletal muscle and gain of adipose tissue, culminating in the condition of “sarcopenic obesity”[1].Sarcopenia is characterised by the loss of muscle mass and is a surrogate marker of malnutrition[2].Severity of liver disease is assessed using “Model for end stage liver disease” (MELD)score, which is calculated by an online calculator using values for serum creatinine,bilirubin and the international normalised value for prothrombin time.The MELD score is also used to decide upon organ allocation for liver transplant[3], and currently does not include a measure of sarcopenia.Researchers have suggested changes in the MELD score calculation to include a measure of sarcopenia, considering its prognostic implications[4].Similarly, the “Child Turcotte Pugh” (CTP) score, a conventional scoring system for severity of liver disease based on values of serum bilirubin,albumin, international normalised value for prothrombin time, and measures of encephalopathy and ascites, do not include any measure of sarcopenia[5].L3 skeletal muscle index (L3SMI) is presently accepted as the most objective and quantitative measure of sarcopenia[6].However, non-availability of computed tomography (CT)scanning in remote areas, cost, and exposure to radiation are limitations to the use of L3SMI; besides, the use of CT for documenting and quantifying sarcopenia can be justified only in patients who have an indication for CT as part of their standard medical care due to risks of radiation exposure.An optimal index for sarcopenia in terms of availability, reproducibility, practicality, and of prognostic significance is therefore needed and remains a challenging issue.
Malnutrition causes sarcopenia in several muscular structures besides the muchstudied lumbar muscles, such as the diaphragm, psoas muscle and tongue[7-9].In the quest for ultrasonography (USG)-based, bedside targets for documenting sarcopenia,we hypothesised that the tongue being a muscular structure affected by sarcopenia with easy access for inspection and measurement, may also be used to quantify and document sarcopenia.Therefore, a prospective study was conducted with the primary objective to measure and compare tongue thickness in healthy individuals and in patients with cirrhosis of the liver.The secondary objective was to determine the correlation between tongue thickness and conventional prognostic scores for patients with cirrhosis of the liver.
MATERIALS AND METHODS
The study was performed at a tertiary care institution after approval by the institutional ethics committee.Consent for the study protocol was obtained from the study subjects.To study 30% difference with power of 80 and type II error of 5%, we needed to study 30 subjects in each group.A total of 120 subjects, who satisfied the inclusion criteria were enrolled and studied from May 2017 to October 2018.
根据职业教育分专业进行教学的特殊性以及学生层次不一、学习风格各异的特点,职中语文教学要彻底冲破传统观念的束缚,充分尊重学生的需要,遵循市场经济规律,体现语文教学的专业性色彩。
Patients with cirrhosis of the liver due to any aetiology and healthy individuals aged 18-65 years and a body mass index (BMI) > 18 and < 30, visiting the hospital for reasons other than illness, were included in the study.Individuals aged less than 18 years and more than 65 years, patients with acute liver failure and those with glossitis were not included in the study.Tongue thickness was measured using USG with a 3.75 MHz convex probe while the subjects were seated in an upright position.The subjects were instructed to swallow their saliva several times to set the tongue at the resting position, and then the ultrasonic measurements were carried out.The measurement points were determined on the upper and lower surfaces of the lingual muscles in the centre of the plane, perpendicular to the ‘Frankfurt horizontal plane’ in a frontal section (Figure 1).The Frankfurt horizontal plane is formed by drawing a straight horizontal line from the top of the ear canal to the bottom border of the eye along either side of the human skull.This line is called the Frankfurt horizontal line[10].The vertical distance was measured from the surface of the mylohyoid muscle to the tongue dorsum (Figure 2).Measurements were performed thrice in freeze-frame when the tongue was restored to the resting position after swallowing saliva, and the mean values were obtained.Tongue thickness was measured for all the study subjects, but the L3SMI was calculated from CT scans only for patients with CTP class C who were being investigated for liver transplant and for healthy individuals who were evaluated as possible organ donors.MELD scores were calculated using the online calculator at https://www.mdcalc.com/meld-score-model-end-stage-liver-disease-12-older.Tongue thickness was compared between the groups based on CTP scores.Correlations were also determined between measured tongue thickness and MELD score, and between age and measured tongue thickness.
Statistical analysis
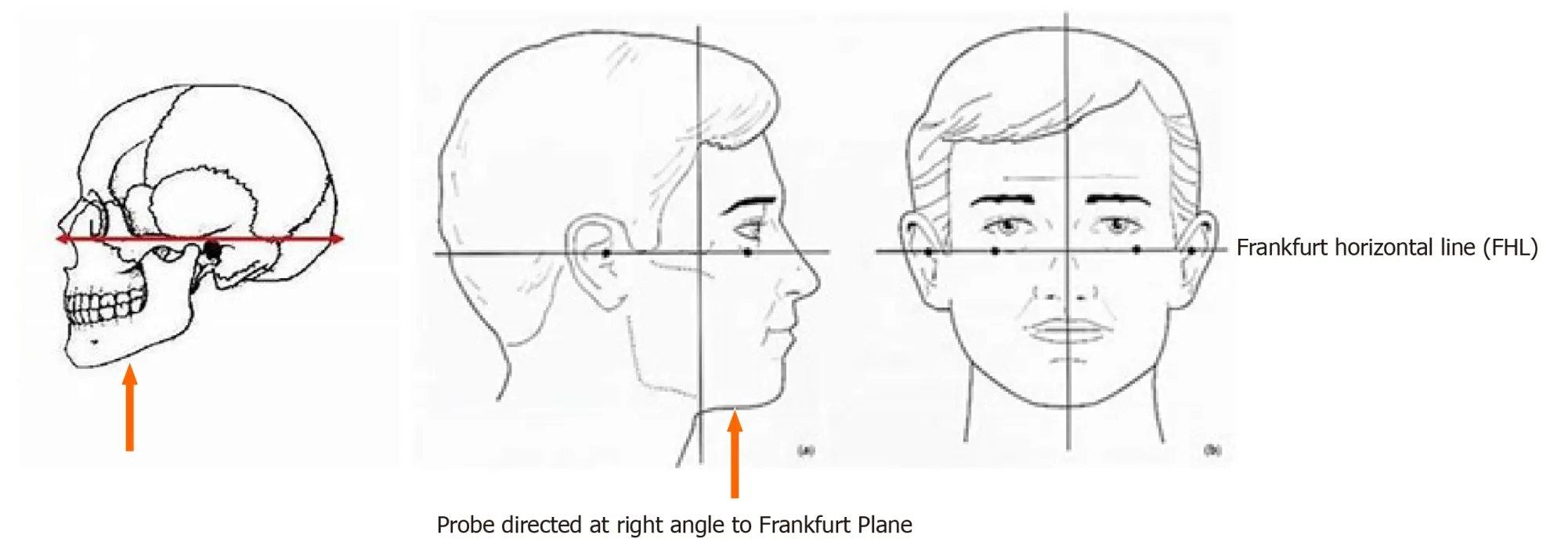
Figure 1 Ultrasonography probe position for measuring tongue thickness.
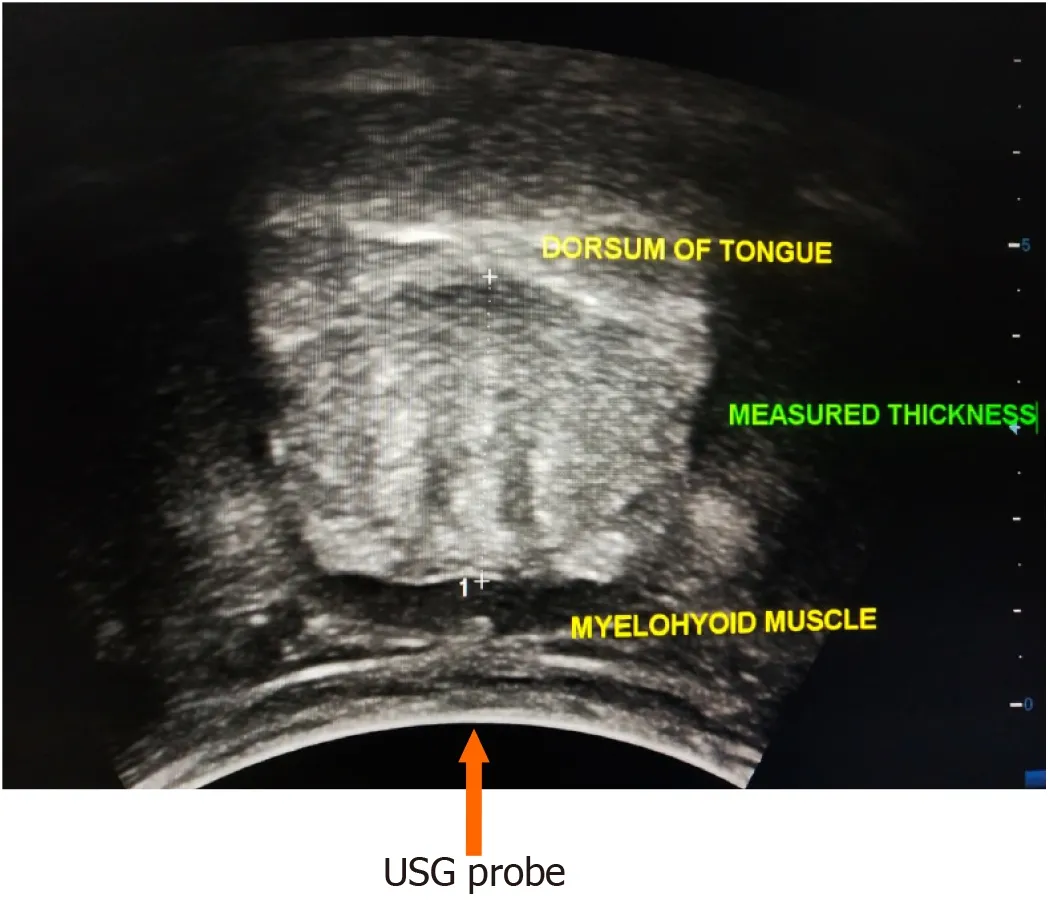
Figure 2 Vertical distance measured from the surface of the mylohyoid muscle to the tongue dorsum.USG: Ultrasonography.
Data are presented as mean ± SD or frequencies (percentage) and were analysed using SPSS 23.0 software.One-way ANOVA was used to test the significance of parametric data and the Kruskal-Wallis test for non-parametric data.Comparison of categorical data was carried out using the chi square test/Fisher’s exact test.Continuous data were compared by the studentt-test/Mann-Whitney test, as applicable.APvalue less than 0.05 was considered significant.Intra-class correlation coefficient (ICC) was used to determine the reliability and agreement of the tongue thickness measurements.
RESULTS
Of 120 patients, 96 were males and 24 were females with a mean age of 47.12 years.The various aetiologies of cirrhosis were ethanol-related, non-alcoholic steatohepatitis, cryptogenic, hepatitis B virus, hepatitis C virus, autoimmune, hepatic vein outflow tract obstruction, non-alcoholic fatty liver disease, and primary sclerosing cholangitis (Figure 3).
Tongue thickness and CTP score
Mean tongue thickness in patients with CTP class A was 4.39 ± 0.39 cm (range 4.25-4.53), in patients with CTP class B was 4.19 ± 0.53 cm (range 3.99-4.39), in patients with CTP class C was 3.87 ± 0.42 cm (range 3.71- 4.02) and in normal healthy individuals was 4.33 ± 0.49 cm (range 4.15-4.51) (Table 1; Figure 4).
A significant difference was seen in tongue thickness between patients with CTP class C and those with CTP class A and B (P< 0.05).Patients with CTP class C also had significantly reduced tongue thickness than normal individuals (P< 0.05).However,no significant difference was observed in tongue thickness between patients with CTP class A and B and normal individuals (Table 2).

Table 1 Tongue thickness in the study groups
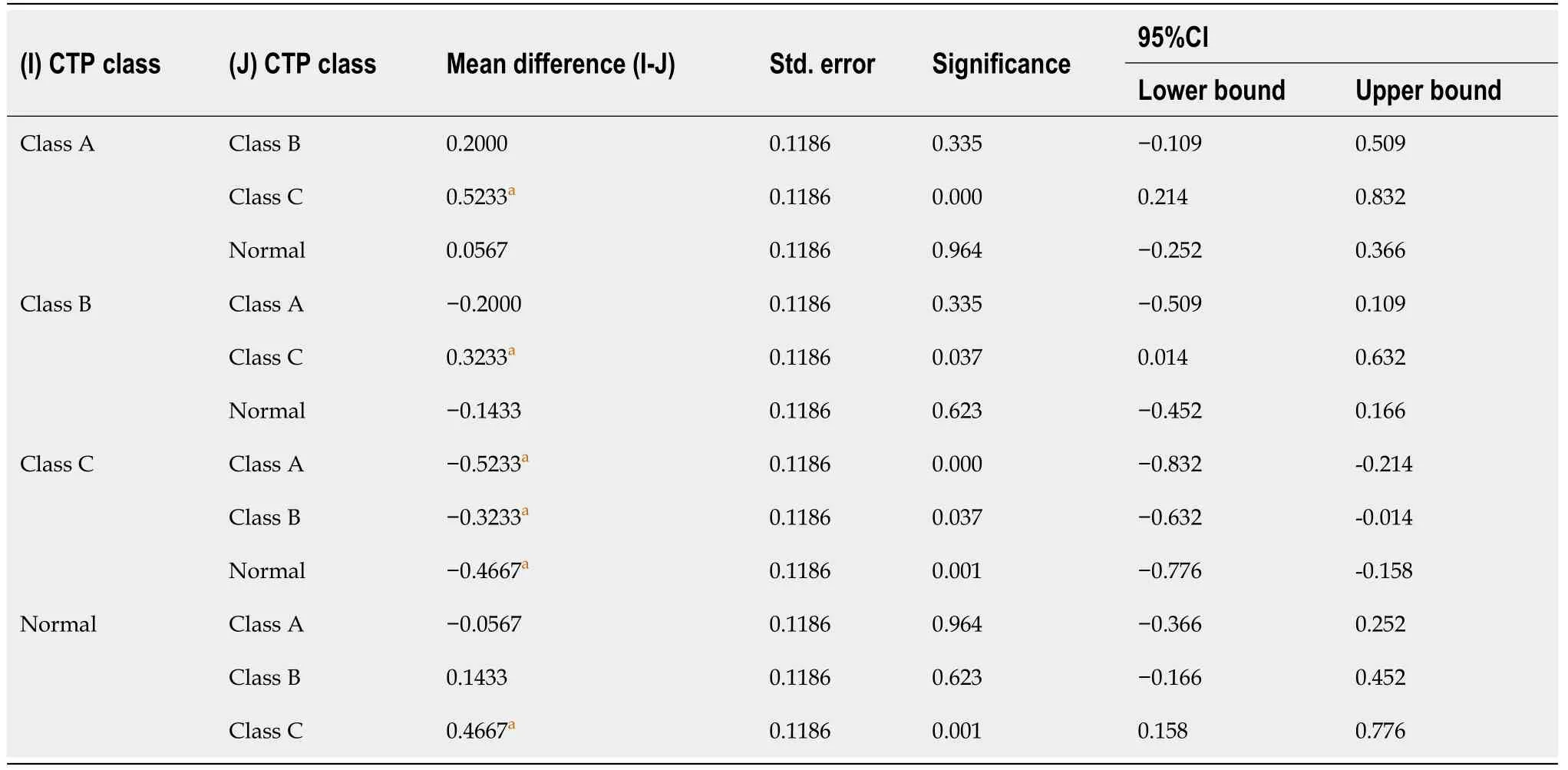
Table 2 Comparison of tongue thickness in the study groups
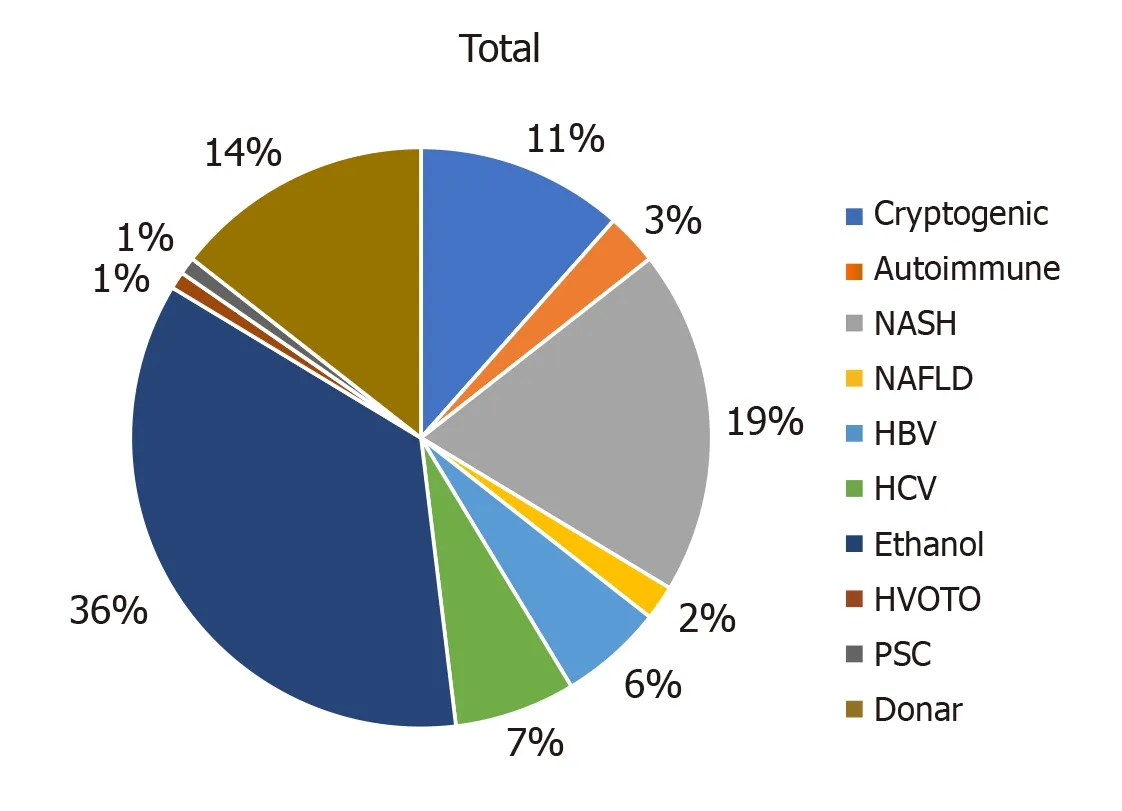
Figure 3 Aetiologies of liver cirrhosis.
MELD score
mean (± SD) MELD score in patients with CTP class A, B and C was 9.63 ± 2.24, 13.90 ±2.96 and 25.37 ± 7.92, respectively.
Tongue thickness and MELD score
A statistically significant, negative correlation was found between MELD score and tongue thickness (r: −0.331) (P< 0.001) (Table 3).

Table 3 Correlation between “Model for end stage liver disease” score and tongue thickness
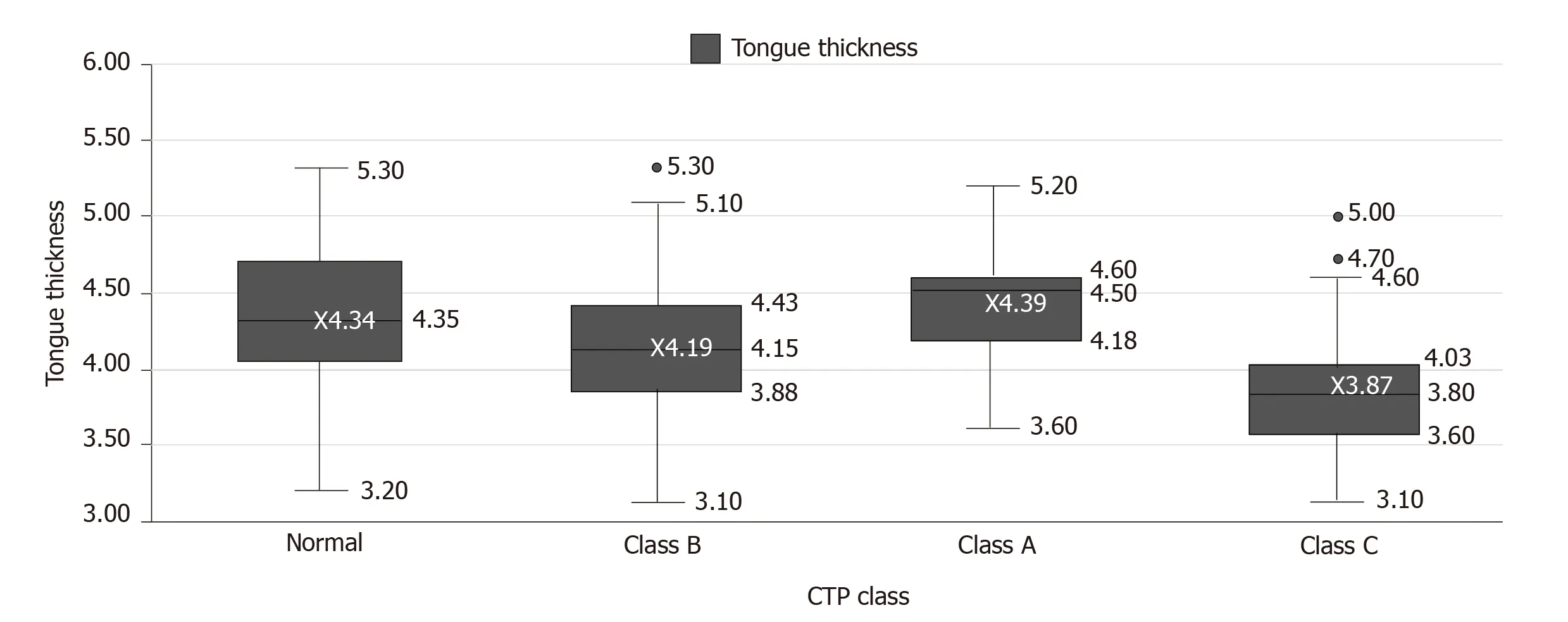
Figure 4 Box plot of the distribution of tongue thickness in different “Child Turcotte Pugh” class patients and normal healthy subjects.CTP class: Child Turcotte Pugh class.
Age and tongue thickness
No significant correlation was found between age of the patients and tongue thickness by USG (Table 4).
Tongue thickness and L3SMI
No significant correlation was found between tongue thickness and L3SMI (P= 0.83)(Table 5).In healthy subjects, the mean (± SD) L3SMI value was 39.66 ± 6.8, and was 38.26 ± 8.88 in patients of CTP class C.The difference was not significant (P= 0.63)(Table 6).Barring the outliers, in 2 healthy subjects and in 2 CTP class C patients, the median L3SMI was 40.19 (33.89-45.4) and 39.39 (32.68-45.35), respectively (Figure 5).ICC was used to determine the reliability of tongue thickness measurements.The ICC value was 0.984 (95%CI: 0.979-0.989) and was indicative of good reliability (Table 7).
在高速公路桥梁施工混凝土浇筑项目开始前,技术部门为了确保拼缝的严密程度以及支撑实用性价值,要整合技术要点和技术要求,合理减少漏浆和跑模问题,确保能对模板刚度以及拼接效果予以严格监督和检查,一定程度上维护了管理工作体系的安全性和完整性。需要注意的是,技术部门要对混凝土的基本成分进行监督,适当掺加高强纤维,以保证整体结构的耐酸碱度腐蚀性能以及抗裂性能的优化,避免低收缩以及早强混凝土。
DISCUSSION
Our study indicates that tongue thickness measurement by USG correlates significantly with the severity of liver disease, as assessed by CTP scores.The study established that patients with a CTP score ≥ 10 have significantly reduced tongue thickness as compared to normal individuals and those with less severe liver disease with CTP scores of 5-9.Studies have shown that sarcopenia also affects other muscles besides the much studied L3SMI[7-9].Tongue thickness has even been examined as a bedside measure of sarcopenia in patients with critical illness and has also been correlated with clinical outcome[9].
Malnutrition in cirrhosis is secondary to a multifactorial process and is seen more often in patients with more severe liver disease.We studied the correlation between tongue thickness and MELD score and found a significant negative correlationbetween the two (r: -0.331,P< 0.01), indicating that as the MELD score increased,tongue thickness decreased and may be interpreted as worsening of sarcopenia with worsening of liver disease.We also found a significant difference in tongue thickness between CTP class C patients and healthy individuals and between CTP class C patients compared to CTP class A and B patients.However, we did not find any significant difference in tongue thickness between healthy individuals and CTP class A and B patients.Apparently, an appreciable degree of sarcopenia manifests only later in the course of liver cirrhosis when a patient qualifies for CTP class C categorisation.Similar to our findings, Montano-Lozaet al[11]studied 248 patients and found that sarcopenia was more prevalent in patients with CTP class C (P< 0.05) and in patients
with higher MELD scores (P< 0.02).In other studies, Thandasseryet al[6]and Tandonet al[12]also found a correlation between the prevalence of sarcopenia and disease severity, as measured by L3SMI and CTP.
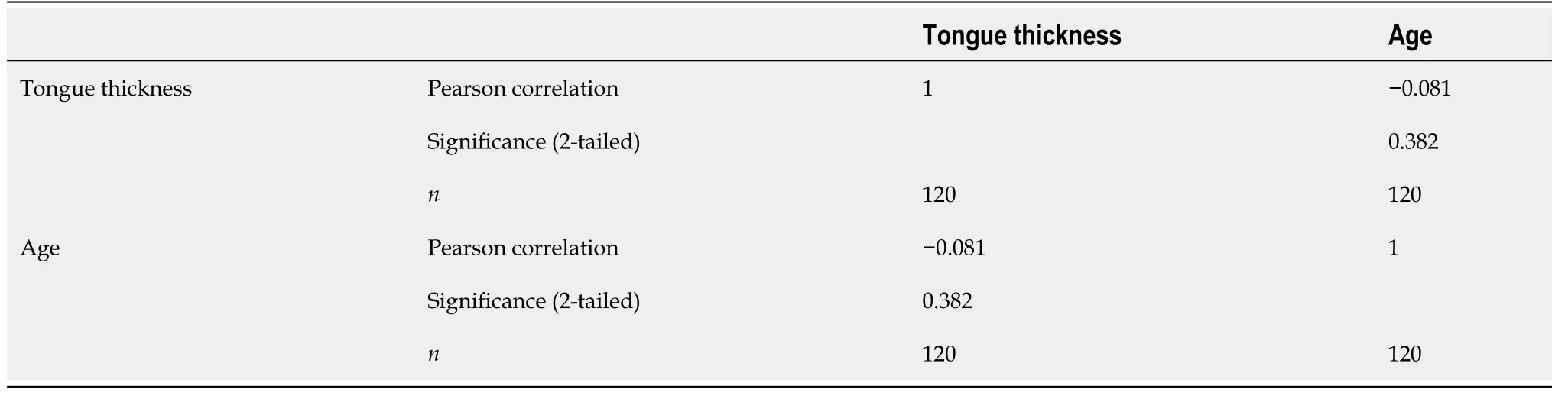
Table 4 Correlation between age and tongue thickness
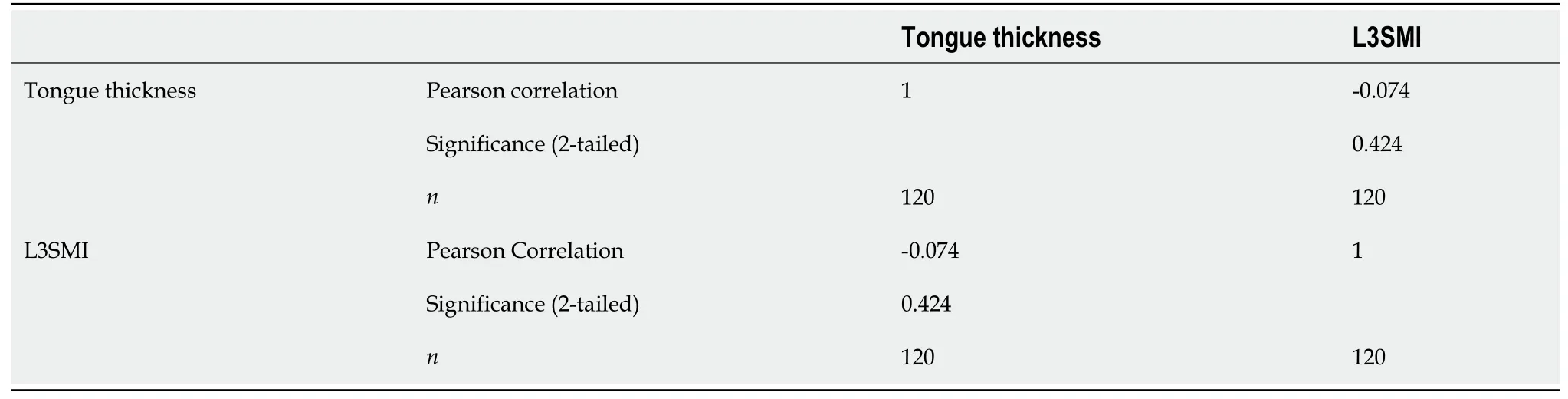
Table 5 Correlation between tongue thickness and L3 skeletal muscle index

Table 6 Comparison of L3 skeletal muscle index in Child Turcotte Pugh class C and normal healthy subjects

Table 7 Intraclass correlation coefficient for ultrasonography measurements of tongue thickness
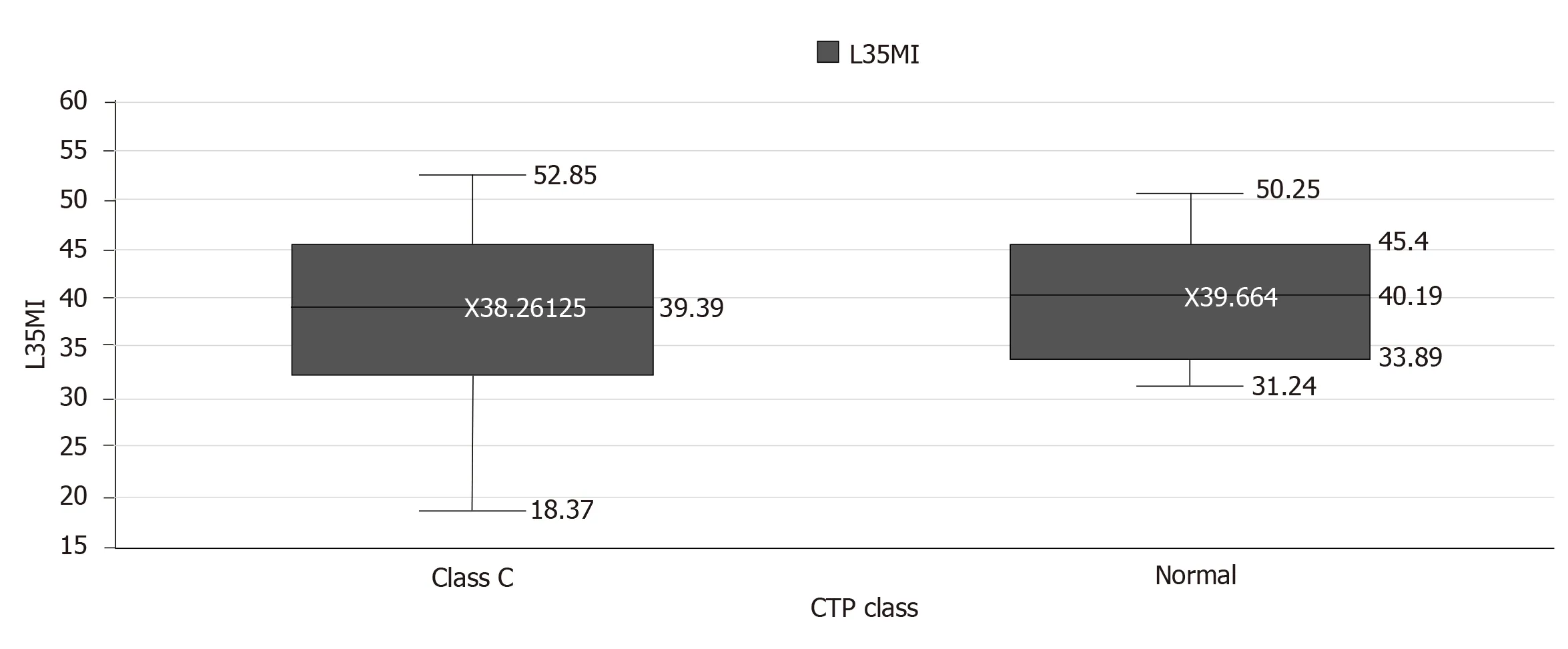
Figure 5 Box plot of the distribution of L3 skeletal muscle index in Child Turcotte Pugh class C patients and healthy individuals.L3SMI:L3 skeletal muscle index; CTP class: Child Turcotte Pugh class.
However, in the present study, we did not find a correlation between tongue thickness and L3SMI.We also did not find any significant difference in L3SMI between healthy subjects and CTP class C patients.Measuring the mass of a muscle or group of muscles that predominantly have dynamic or postural functions, we believe, is flawed and the paravertebral muscles being postural muscles, are apparently only affected to an appreciable degree late in the disease course when patients may be critically ill and become bedridden.None of the patients included in this study were critically ill and/or admitted to the intensive care unit or were bedridden, and this could possibly be the reason why no difference was found between L3SMI in healthy subjects and CTP class C patients.This reasoning may also be inferred from the study of 116 patients with cirrhosis and hepatocellular carcinoma by Meza-Juncoet al[13].In their study, similar to our findings, the degree of sarcopenia measured using L3SMI did not correlate with CTP or MELD scores.However, in our study, tongue thickness was consistently and significantly decreased in CTP class C patients.Tongue thickness is probably a more sensitive marker of sarcopenia compared to L3SMI and requires further investigation.
A significant number of people more than 65 years old have decreased muscle mass[14].In this study, we did not include patients more than 65 years, but we did not find a significant correlation between tongue thickness and age of the subjects included (Table 4).Sarcopenia in cirrhotic patients has been associated with increased mortality, sepsis, hyperammonemia, overt hepatic encephalopathy, and increased length of stay after liver transplantation[6].The literature also suggests that patients with cirrhosis, poor nutritional status and sarcopenia have a higher risk of mortality,independent of the CTP and MELD scores[15].It is therefore important to diagnose,quantify and perhaps classify the degree of sarcopenia for the medical management of patients with cirrhosis of the liver, for outcome prognosis and for planning interventions such as liver transplantation.This could be greatly helped by having a readily available and reproducible method for the diagnosis and quantification of sarcopenia.
The tongue has the advantages of direct inspection and ease of bedside measurement of thickness using USG, which is more readily available than CT scanning and is without the risk of radiation exposure, and unlike CT does not require extensive training.Tongue thickness measurement, as suggested by our findings, in addition to being objective, reproducible and easy, could be a more sensitive index for detecting sarcopenia than L3SMI.Our study was limited due to it being located at a single centre, and directed at patients with only a single disease, namely cirrhosis of the liver.Further studies exploring USG-measured tongue thickness in people of diverse ethnicity and different age groups in health and in disease, should be carried out to validate our findings and to establish this as a convenient bedside tool for diagnosing sarcopenia.In view of our study findings, we propose that tongue thickness measurement using USG should be considered for the diagnosis and quantification of sarcopenia.
ARTICLE HIGHLIGHTS
Research background
Sarcopenia in patients with chronic liver disease has prognostic implications.L3 skeletal muscle index (L3SMI) calculated from computed tomography (CT) images is currently the only objective and reproducible method accepted for the quantification of sarcopenia.This study aims to determine tongue thickness measured using ultrasonography as an alternative method for diagnosing sarcopenia.
Research motivation
Sarcopenia in patients with chronic liver disease has prognostic implications.Wider application of L3SMI calculated from CT images is limited by cost, the need for extensive training, limited availability and due to the risk of radiation exposure.Clinical researchers have suggested the inclusion of a measure of sarcopenia in established prognostic models for patients with liver disease.A dependable and reproducible method with wider availability is therefore needed.
Research objectives
This study aimed to examine tongue thickness measured using ultrasonography as a dependable bedside tool for the diagnosis of sarcopenia.Significant differences were seen in tongue thickness between healthy individuals and individuals with less severe liver disease compared to patients with more severe chronic liver disease.
Research methods
Patients with chronic liver disease and healthy individuals who satisfied the inclusion criteria underwent tongue thickness measurement using ultrasonography.The study was observational in nature and no intervention was planned on the basis of observations made.Tongue thickness measurements were compared between healthy individuals and patients with liver disease of different severity.The imaging technique used was ultrasonography, which has wider availability and does not involve radiation exposure unlike CT scanning used to measure L3SMI.
Research results
Significant differences were seen in tongue thickness between healthy subjects and patients with less severe liver disease compared to patients with more severe liver disease.Tongue thickness measured using ultrasonography is therefore proposed as a bedside measure of sarcopenia.However, its application requires further validation in studies involving subjects of different ethnicity, in health and in disease.
Research conclusions
This study established consistent and significantly reduced tongue thickness in patients with severe liver disease compared to healthy individuals and patients with less severe liver disease.Tongue thickness measured using ultrasonography may therefore be used as a bedside tool for the diagnosis of sarcopenia, an application with wide availability and no risk of radiation exposure compared to CT-based measurement of L3SMI.
Research perspectives
The findings in this study require validation in a similar study of tongue thickness using ultrasonography in people of different ethnicity in health and in disease.
猜你喜欢
建材发展导向(2022年23期)2022-12-22
建材发展导向(2022年20期)2022-11-03
现代装饰(2022年5期)2022-10-13
建材发展导向(2022年18期)2022-09-22
建材发展导向(2022年12期)2022-08-19
建材发展导向(2022年10期)2022-07-28
快乐语文(2021年35期)2022-01-18
建材发展导向(2021年7期)2021-07-16
考试与评价·高二版(2020年2期)2020-09-10
少年文艺·我爱写作文(2009年5期)2009-06-08
 World Journal of Gastrointestinal Pharmacology and Therapeutics2020年3期
World Journal of Gastrointestinal Pharmacology and Therapeutics2020年3期
- World Journal of Gastrointestinal Pharmacology and Therapeutics的其它文章
- Shared changes in angiogenic factors across gastrointestinal vascular conditions: A pilot study
- Hepatobiliary manifestations in children with inflammatory bowel disease: A single-center experience in a low/middle income country