
Preliminary experience of hybrid endoscopic submucosal dissection by duodenoscope for recurrent laterally spreading papillary lesions
2020-10-23 07:25:28ZiKaiWangFangLiuYunWangXiangDongWangPingTangWenLi
World Journal of Gastroenterology 2020年37期
Zi-Kai Wang, Fang Liu, Yun Wang, Xiang-Dong Wang, Ping Tang, Wen Li
Abstract
Key Words: Endoscopic submucosal dissection; Ampullary adenoma; Recurrent; Laterally spreading; Papillary lesions
INTRODUCTION
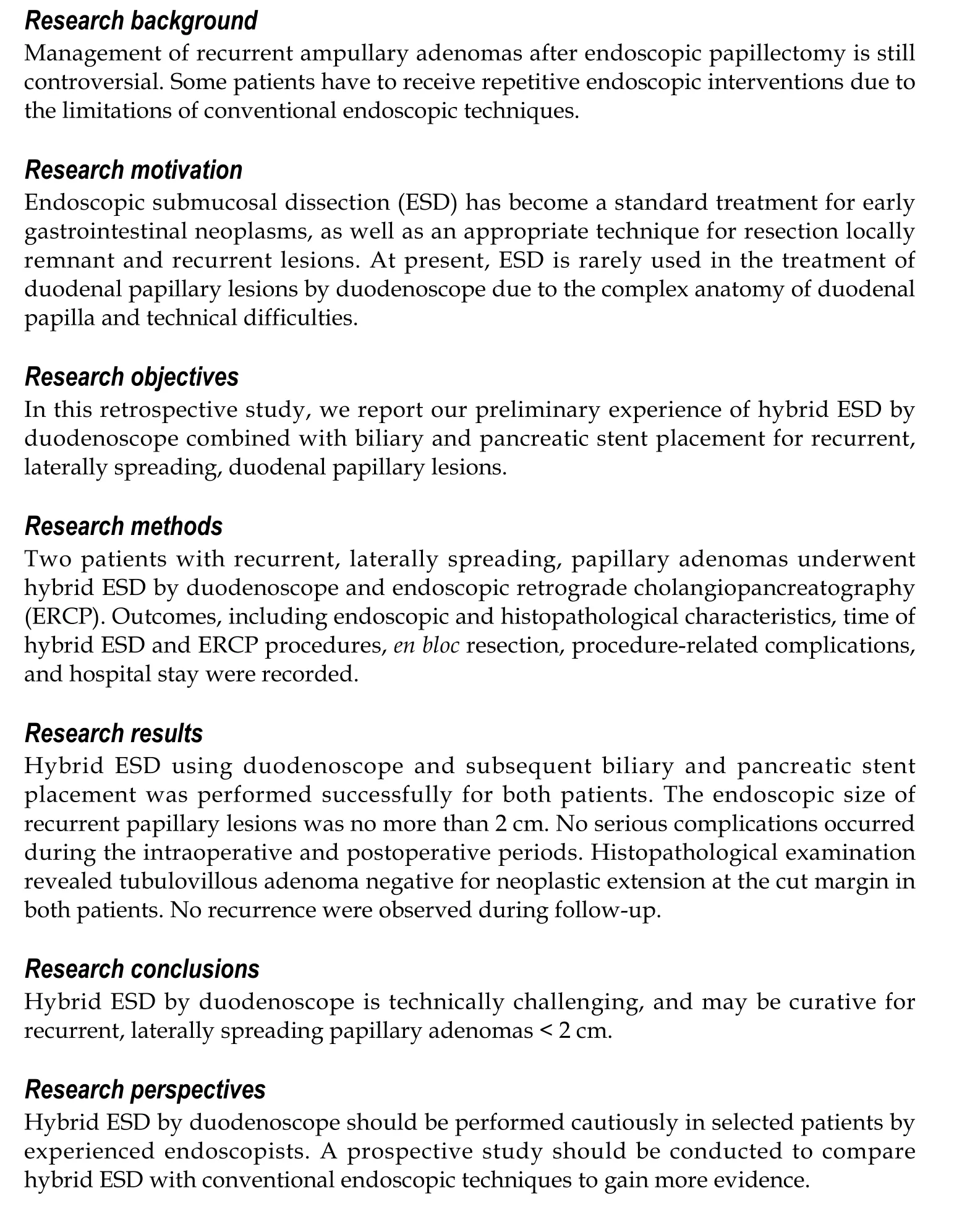
The clinical practice or consensus for endoscopic management of duodenal papillary lesions is not fully established[1]. Several endoscopic resection techniques such as snare polypectomy, endoscopic mucosal resection (EMR) and argon plasma coagulation (APC) ablation are available for papillary lesions[1-3]. Endoscopic resection of the laterally spreading ampullary lesions is difficult technically and usually involves surgery. Moreover, the management strategies for recurrent duodenal papillary adenomas after endoscopic papillectomy are still controversial[2]. Patients with recurrent papillary adenomas need to receive repetitive endoscopic interventions due to the limitations of conventional endoscopic techniques, such as incomplete resection. At present, endoscopic submucosal dissection (ESD) has become common and has gradually replaced most surgical procedures for management of early gastrointestinal neoplasms[4], which could provide a higheren blocresection rate than conventional endoscopic resection techniques. Until now, ESD has rarely been used for the treatment of duodenal papillary lesions by duodenoscope due to the complex anatomy of the duodenal papilla and technical difficulties.
In this paper, we report our preliminary experience of hybrid ESD by duodenoscope combined with biliary and pancreatic stent placement for the treatment of recurrent, laterally spreading, duodenal papillary lesions.
MATERIALS AND METHODS
Patient selection and evaluation
Ten patients with recurrent duodenal papillary adenomatous lesions after endoscopic snare papillectomy were admitted to the Department of Gastroenterology and Hepatology, The First Medical Center of Chinese PLA General Hospital between March 2017 and September 2018. We excluded patients who received endoscopic management using an electric snare or APC ablation for small, locally recurrent adenomas < 1 cm without intraductal growth, and those who underwent pancreatoduodenectomy and/or chemoradiotherapy due to cancerization and ductal infiltration. Finally, we enrolled two patients with recurrent, laterally spreading papillary adenomas confirmed by duodenoscopic and biopsy examination. The patients had undergone hybrid ESD by duodenoscope and subsequent endoscopic retrograde cholangiopancreatography (ERCP). The clinical symptoms and physical and laboratory examination were evaluated. Computed tomography (CT), magnetic resonance imaging, magnetic resonance cholangiopancreatography and abdominal ultrasound were performed preoperatively, and the imaging examinations confirmed no infiltration of tumor into biliary and pancreatic ducts. Moreover, these two patients refused surgical management and gave informed consent.
Materials and equipment
Hybird ESD was performed using a standard duodenoscope (TJF240 or TJF260V; Olympus, Tokyo, Japan). The equipment included a dual knife (KD-650L; Olympus), insulated-tip diathermic (IT) knife II (KD-611L; Olympus), injection needle (NM-200L-0525), hemostatic forceps (FD-410LR; Olympus), electric snare (Cook Medical, Bloomington, IL, United States), endoclips (Olympus), SureClips (Micro-Tech, Nanjing, China), intraductal ultrasound (IDUS) (UM-DG20-31R; Olympus), cannulating sphincterotome (Dreamtome RX, Boston, MA, United States), bile duct stent (10 Fr in diameter, 3-8 cm in length; Cook Medical), pancreatic duct stent (5-7 Fr in diameter, 7-8 cm in length; Cook Medical), and a high-frequency electrosurgical generator (VIO 200D; ERBE, Tubingen, Germany). An endoscopic CO2insufflator (UCR; Olympus) was used during the endoscopic procedures. Saline solution with diluted methylene blue, sodium hyaluronate and adrenaline was used for submucosal injection, and 1:10000 diluted epinephrine submucosal injection was used for hemostasis.
Operative procedures
All endoscopic procedures were performed by an experienced endoscopist who had > 20 years’ experience in advanced endoscopic techniques and had performed > 2000 ESD and ERCP procedures. Patients were placed in the prone position and underwent intravenous anesthesia. Before ESD, the duodenal papillary lesions were evaluated by white light and narrow band imaging. Hybrid ESD with snaring was performed using a standard duodenoscope. After marking the resection borders of the lesion using a dual knife, a submucosal cushion was created by injecting a mixture of saline solution, methylene blue and adrenaline. A total circumferential incision and submucosal excision were performed by Dual knife combined with IT knife, and the lesion was ligated and resected using an electric snare. The electric coagulation, injection of saline solution with epinephrine and endoclips placement were applied for hemostasis during the endoscopic procedures. After hybrid ESD, ERCP, including selective cannulation of biliary and pancreatic ducts, and IDUS were performed to identify whether there was tumor ductal infiltration. Moreover, stent implantation of the biliary and pancreatic ducts was performed to prevent postoperative complications. Endoclip closure for mucosal defect after hybrid ESD was performed. During the postoperative period, intravenous proton pump inhibitors, somatostatin and antibiotics were given to prevent infection and post-ERCP pancreatitis. Meanwhile, diet was gradually restored if no complications occurred after postoperative fasting for 2-3 d.
对前面节所述的3个热传递过程,根据热电比拟理论和历史热点测量数据通过Matlab建模逐过程计算内部导体温升及外壳内外温升。以外壳外表面热点温度为例,其计算流程见图4。
Evaluation data
The primary outcome measures included clinical symptoms; physical and laboratory examination; imaging characteristics, especially endoscopic and histopathological characteristics; detailed procedure-related outcome data, including the time of hybrid ESD and ERCP;en blocresection; procedure-related complications; and hospital stay. Endoscopic and histopathological follow-up was performed to assess the presence of duodenal papillary lesions after hybrid ESD procedures.
RESULTS
This study included two patients with recurrent, laterally spreading, duodenal papillary adenomas. The previous characteristics of recurrent cases are listed in Table 1, and the duodenoscopic follow-up confirmed recurrent adenomas located in the therapeutic scar tissues. The main characteristics of all patients are shown in Table 2. Preoperative imaging confirmed no infiltration of tumor into biliary and pancreatic ducts, and the endoscopic findings showed a clear border with no evidence of malignancy, such as ulceration and spontaneous bleeding.
Hybrid ESD combined with ERCP was performed successfully using duodenoscope. The detailed endoscopic procedures are shown in Figures 1 and 2. The average total procedure time was 95.5 min, and the procedure time of hybrid ESD and ERCP was 38.5 min and 15.5 min, respectively. After submucosal injection, the surrounding mucosa of the lesion was lifted, except the central scar tissues. When the circumferential incision was completed, the IT knife was used to dissect the fibrotic area for prevention of perforation. The lesion was ligated and resecteden blocusing a polypectomy snare. After hybrid ESD, ERCP and IDUS procedures were performed. Selective cannulation, angiography, and IDUS revealed a clear layer of the biliary and pancreatic ducts and no intraductal growth of the lesions in these two patients. Meanwhile, cholangiopancreatography and IDUS revealed common bile duct stones with obvious dilated biliary and pancreatic ducts in case 1, but the stones were not extracted simultaneously, considering the increasing risk of complications. Subsequently, the biliary and pancreatic stents were placed successfully in both cases (Figures 1 and 2, and Table 2). Furthermore, endoscopic clips were deployed for closure of mucosal defects. In both cases, no serious complications occurred during the intraoperative and postoperative periods. Postoperative laboratory tests showed normal routine blood and biochemical examinations, except for transient hyperamylasemia in case 2. Histopathological examination revealed tubulovillous adenoma negative for neoplastic extension at the horizontal and vertical margins in both cases (Figures 1 and 2).
Duodenoscopic and histopathological follow-up was undertaken at 3 mo after hybrid ESD. Endoscopic examination showed no residual or recurrent lesions in ampullary areas in both cases. ERCP showed dilated common bile duct and pancreatic ducts, and the common bile duct stones were extracted successfully in case 1, and the biliary stent was removed in case 2 (Figures 1 and 2). Histopathology of biopsy specimens showed chronic and acute inflammation of small intestinal mucosa with no adenomatous tissues in both cases (Figures 1 and 2). Both cases have been followed up with no recurrence up to June 2020.
DISCUSSION
Duodenal papillary neoplasms are uncommon and occur sporadically with a prevalence of 0.1%-0.2%[5]. The majority of papillary adenomas undergo the adenoma–carcinoma sequence, and complete removal is mandatory for curative therapy due to the malignant potential[6]. Traditionally, recommended surgical management has included pancreaticoduodenectomy and local surgical excision for complete removal of duodenal papillary tumors[7], but surgery often results in extensive resection with significant morbidity and mortality[1]. This is considered overtreatment for some benign duodenal papillary lesions or early noninvasive tumors of the papilla without intraductal growth. Endoscopic papillectomy by snare polypectomy or EMR has the advantages of being less invasiveness, which represents an alternative to surgical resection[1]. At present, it is not definitive which size or endoscopic morphology of ampullary lesions should not be treated by endoscopic resection[2]. Most studies have not recommended endoscopic resection for the duodenal papillary lesions ≥ 3-4 cm or those with extrapapillary extension[8]. Endoscopic snare polypectomy or EMR for ampullary lesions often requires repetitive interventions due to incomplete resection, residual lesion and tumor recurrence. The recurrent rate of ampullary adenomas after endoscopic papillectomy is 7%-33%[9-12]. Our team reported that 13 of 110 patients who underwent endoscopic papillectomy experienced recurrence during a mean follow-up period of 16.3 mo, and the predictive factors related to recurrence were complete resection and final pathological findings[13]. Although 75% of recurrences can be cleared endoscopically[12], surgery is usually the last choice. In our experience, there is still the possibility of multiple recurrence after endoscopic snare polypectomy or APC ablation for recurrent ampullary lesions. This indicates the technical difficulty and limitations of the conventional endoscopic papillectomy for recurrent duodenal papillary lesions.
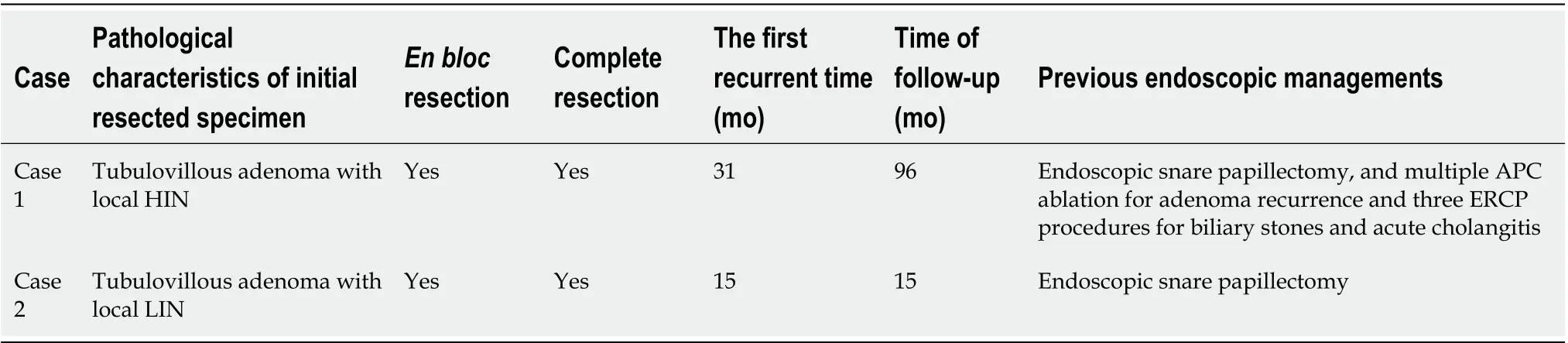
Table 1 Previous characteristics of patients with recurrent laterally spreading duodenal papillary lesions
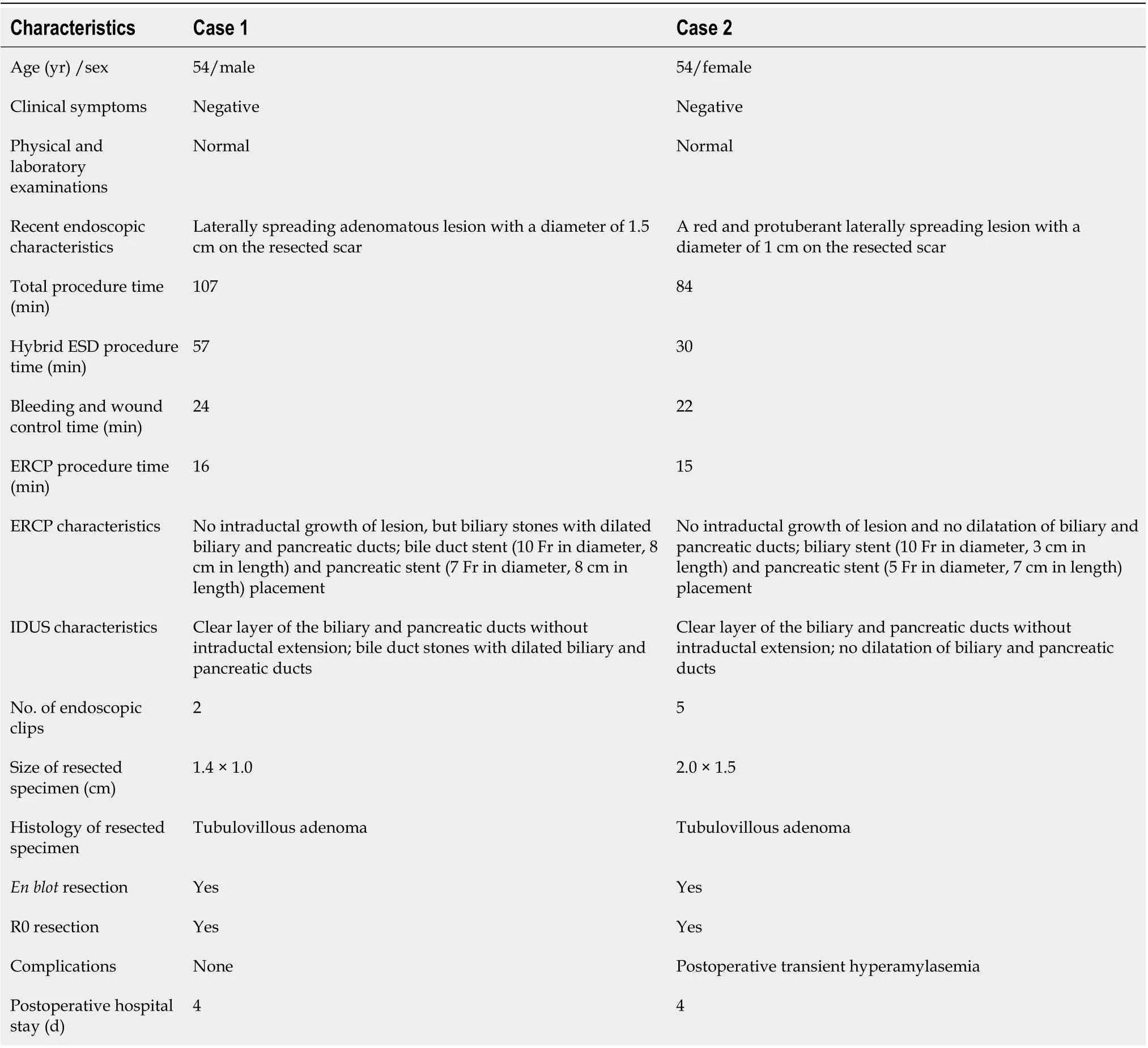
Table 2 Main characteristics of patients in this study
Preoperative evaluation of ampullary lesions is important for the subsequent management strategy. In this study, preoperative endoscopic findings showed a clear border with no evidence of malignancy, such as ulceration or spontaneous bleeding, and the appropriate ampullary lesion size (≤ 2 cm). Meanwhile, preoperative histopathological examination of biopsy sample revealed papillary adenoma for both cases. Furthermore, endoscopic ultrasonography (EUS) and IDUS are useful diagnostic tools for selecting endoscopic or surgical treatment for ampullary adenomas[14,15]. These methods may be more efficient than CT for preoperative evaluation of local T staging, regional lymph node metastasis, ductal infiltration, and major vascular invasion in patients with ampullary lesions. It is reported that the accuracy of EUS in diagnosing extension into the bile duct and pancreatic duct is as high as 86%-90% and 77%-92%, respectively. IDUS can be more accurate in visualizing mucosal layers than conventional EUS, with a high accuracy of 90%-95% and 88%-100% in diagnosing extension into the bile duct and pancreatic duct, respectively[16]. In our study, both patients received careful preoperative evaluation, and several imaging examinations indicated no intraductal involvement of ampullary lesions. EUS for the estimation of tumor staging and ductal infiltration was not performed routinely in this study, but subsequent ERCP and IDUS confirmed no intraductal extension. Whatever, accurate preoperative evaluation could reduce the technical difficulties and the risk of severe complications[17].
At present, ESD has been widely accepted as standard treatment for early gastrointestinal neoplasms and large laterally spreading lesions[4], and as an appropriate resection technique for locally remnant and recurrent lesions in patients receiving endoscopic resection[18,19]. Several studies have reported successful ESD for duodenal lesions[20-22]using therapeutic gastroscopy, but ESD is rarely used for treatment of recurrent, laterally spreading ampullary lesions by duodenoscope. This is mainly due to the special physiology and complex anatomical features of duodenal papillary lesions (e.g., lesion location, lesion size, thin muscle layer, rich blood supply, secretion of biliary and pancreatic juice, and fibrosis of recurrent lesions), and technical difficulties (e.g., limited operating space and operational difficulties to achieve good endoscopic control and optimal visual fields based on forward-viewing endoscopy)[2]. Meanwhile, ESD for recurrent, laterally spreading ampullary adenomas raises concerns about a high risk of procedure-related complications. Therefore, ESD should be performed by experienced endoscopists with both ERCP and ESD techniques to reduce the risk of severe complications. In our study, all endoscopic procedures were performed by an experienced endoscopist who had > 20 years’ experience in advanced endoscopic techniques and had performed > 2000 ESD and ERCP procedures. Carefully attention was focused on endoscopic management for procedure-related complications. Submucosal fibrosis after endoscopic papillectomy for recurrent cases is a significant risk factor for adverse events. Therefore, we used a hybrid ESD technique for complete resection with a polypectomy snare to remove the lesions after dissecting the submucosal layer. Additionally, strict hemostasis including injection, electrocoagulation and endoclip placement during hybrid ESD were compulsory. The resection wound after ampullary hybrid ESD is exposed directly to biliary and pancreatic juices, which is believed to cause postoperative complications, so we suggest that after biliary and pancreatic stent placement, the resection wound should be closed by endoclips as much as possible. In this study, hybrid ESD with snaring using duodenoscope was technically successful, anden blocresection of the therapeutic scar tissue was achieved. The average procedure time of hybrid ESD was 38.5 min, which was acceptable. No severe adverse events such as bleeding and perforation occurred in the recurrent cases.
ERCP as an important procedure and should be performed after ampullary ESD treatment. Generally, it is easy to perform selective cannulation due to the exposure of biliary and pancreatic duct after papillectomy. Limited endoscopic resection of ampullary lesions may have a risk of leaving residual tissues; therefore, ERCP and IDUS are useful for further evaluation of the condition of the biliary and pancreatic ducts. For these cases, selective cannulation for biliary and pancreatic ducts was successfully performed, and ERCP and IDUS demonstrated no biliary or pancreatic extension and no residual lesions after ESD. Prophylactic stent placement in the pancreatic duct after endoscopic removal is necessary to minimize the risk of post-ERCP pancreatitis[23]. In this study, we implanted both biliary and pancreatic stents to avoid early complications and late adverse events. There are four purposes of deploying biliary and pancreatic stenting after ESD: to prevent post-ERCP pancreatitis and cholangitis; to drain bile and pancreatic juice far from the wound surface to reduce the risk of perforation and bleeding; to avoid closure of the pancreaticobiliary opening when the hemostatic clip closes the wound; and to prevent biliary and/or pancreatic stenosis.

Figure 1 Endoscopic and pathological characteristics of case 1. A-D: Hybrid endoscopic submucosal dissection (ESD) for recurrent, laterally spreading, duodenal papillary adenoma, including marks, submucosal injection and submucosal dissection. The lesion was resected completely using a polypectomy snare, and the artificial ulcer was visible; E: Endoscopic retrograde cholangiopancreatography (ERCP) showed the dilated biliary duct, common bile duct stones, and mildly dilated pancreatic duct; F: Biliary and pancreatic duct stents were implanted, and the endoscopic clips were used for closure of mucosal defects and prevention of complications; G: Hematoxylin and eosin stained resected specimen showing tubulovillous adenoma with a clean cutting edge, 4 ×; H: Endoscopic follow-up 3 mo after hybrid ESD, biliary stent and stones were extracted by ERCP; I: Histological follow-up of biopsy specimen revealed chronic and acute inflammation of small intestinal mucosa, 10 ×; J: Endoscopic follow-up 20 mo after hybrid ESD with no recurrence.

Figure 2 Endoscopic and pathological characteristics of case 2. A: Red and protuberant laterally spreading lesion was seen in the mucosa around the opening of the pancreaticobiliary duct; B-D: Hybrid endoscopic submucosal dissection (ESD) such as submucosal injection and submucosal dissection are shown, and the artificial ulcer was created; E and F: Endoscopic retrograde cholangiopancreatography showed the normal bile and pancreatic ducts, biliary and pancreatic stents were implanted, and close incision was performed by endoscopic clips; G: Hematoxylin and eosin-stained resected specimen showing tubulovillous adenoma with clean cutting edge, 4 ×; H: Endoscopic follow-up 3 mo after hybrid ESD showed that the pancreatic stent disappeared, and the biliary stent and clips were removed; I: Histological follow-up of biopsy specimen revealed chronic and acute inflammation of small intestinal mucosa, 20 ×; J: Endoscopic follow-up 38 mo after hybrid ESD with no recurrence.
CONCLUSION
In conclusion, hybrid ESD by duodenoscope is technically challenging, and may be curative for recurrent, laterally spreading ampullary adenomas < 2 cm in diameter. It should be performed with caution by experienced endoscopists in selected patients to avoid severe complications.
ARTICLE HIGHLIGHTS
猜你喜欢
水泵技术(2022年3期)2023-01-15 21:44:59
防爆电机(2022年5期)2022-11-18 07:40:48
防爆电机(2022年4期)2022-08-17 05:59:50
装备制造技术(2019年12期)2019-12-25 03:07:36
模具制造(2019年7期)2019-09-25 07:30:00
电子制作(2018年2期)2018-04-18 07:13:36
电力与能源(2017年6期)2017-05-14 06:19:41
山东工业技术(2016年15期)2016-12-01 05:30:54
化工进展(2015年3期)2015-11-11 09:18:10
河南科技(2015年15期)2015-03-11 16:25:52
 World Journal of Gastroenterology2020年37期
World Journal of Gastroenterology2020年37期
- World Journal of Gastroenterology的其它文章
- Artificial intelligence technologies for the detection of colorectal lesions: The future is now
- Transjugular intrahepatic portosystemic shunt in cirrhosis: An exhaustive critical update
- Abernethy syndrome in Slovenian children: Five case reports and review of literature
- Endoscopic retrograde cholangiopancreatography in the treatment of pancreaticopleural fistula in children
- Risk prediction rule for advanced neoplasia on screening colonoscopy for average-risk individuals
- Endoscopic ultrasound-fine needle biopsies of pancreatic lesions: Prospective study of histology quality using Franseen needle