
A systematic review and meta-analysis to compare the effects of Chinese herbal pieces and granule in different diseaseherbal pieces
2020-09-29 08:09YangYuLuWangJingBoZhaiChangGangSun
TMR Integrative Medicine 2020年18期
Yang Yu,Lu Wang,Jing-Bo Zhai,Chang-Gang Sun
1School of Traditional Chinese Medicine, Shandong University of Traditional Chinese Medicine, Jinan 250355, China. 2Scientific Research Office, Shandong University of Traditional Chinese Medicine, Jinan 250355, China. 3Tianjin University of Traditional Chinese Medicine, Tianjin 301608, China. 4Institute of Traditional Chinese Medicine Innovation, Shandong University of Traditional Chinese Medicine,Jinan 250355,China.
Abstract
Keywords: TCM granules, TCM herbal pieces, Cold, Hypertension, Osteoporosis, Digestive system diseases,Migraines,Meta-analysis
Background
Traditional Chinese medicine(TCM)has been used for thousands of years. Up to 2,598 varieties of species,12,807 varieties of herbs, and more than 100,000 traditional prescriptions are included in theChinese Pharmacopoeia(2015 Edition) [1]. For thousands of years, the use of TCM has changed from simple to complex. A combination of multiple drugs is used as the main weapon to prevent and cure diseases.Chinese herbal pieces decoctionis the most common and primitive application method. However, as there is a variety of complex ingredients [2], the correct utensils,water quality, heat, stewing time, and the decoction methods maybe influence the ingredients activity.Decoctions are also inconvenient to transport and store.With the development of modern technology, TCM formulations have also been improved, including the use of TCM formula granules. These were first developed by Tianjiang Pharmaceutical Co., Ltd., in the early 1990s, and officially named “TCM formula granules” [3] in June 2001 after the State Food and Drug Administration organized discussions among experts(nomenclature committee).They are defined as the granules made from single TCM herbs through extraction and concentration and used for TCM clinical prescriptions. The granule is a good solution to the problems of decoction, such as quality control,preparation, and dose. Therefore, the use of granules has increased sharply in China and other Asian countries and regions[4–6].
With the wide application, effectiveness and safety of TCM formula granules are worthy of further discussion. When decocting herbs, high temperature can promote the dissolution of active ingredients, but whether the granules directly dissolved in boiling water can achieve this process is still worth exploring.Some clinical studies have shown that, compared with TCM herbal piecespieces, TCM granules have better or equivalent efficacy [7], while other studies have shown the opposite [8–10]. Because of limitations in methodological quality [11], there is no high-quality systematic evaluation of this evidence. The purpose of this study was to summarize all available data on the validity of traditional Chinese medicine granules and Chinese medicine tablets through retrieval and inclusion of 98 articles, including 8 diseases, to provide quantitative evaluation and evidence for clinical use of TCM granules.
Methods
Inclusion criteria
(1) Type of study:randomized controlled trials(RCTs)and controlled clinical trials (CCT); (2) intervention measures: TCM granules for the experimental group and TCM herbal piecespieces for the control group;(3)oral administration; (4) the efficacy, safety, and other efficacy indicators are reported in the results, and the efficacy was evaluated according to the Criteria of Diagnosis and Therapeutic effect of Diseases and Syndromes in Traditional Chinese Medicine[12].
Exclusion criteria
(1) Animal studies, case reports, literature reviews,summaries of experience, abstracts, and so forth; (2)articles that have been published repeatedly; (3)inconsistent interventions for the experimental group and control group; (4) external interventions. Articles meeting any of the above criteria were excluded.
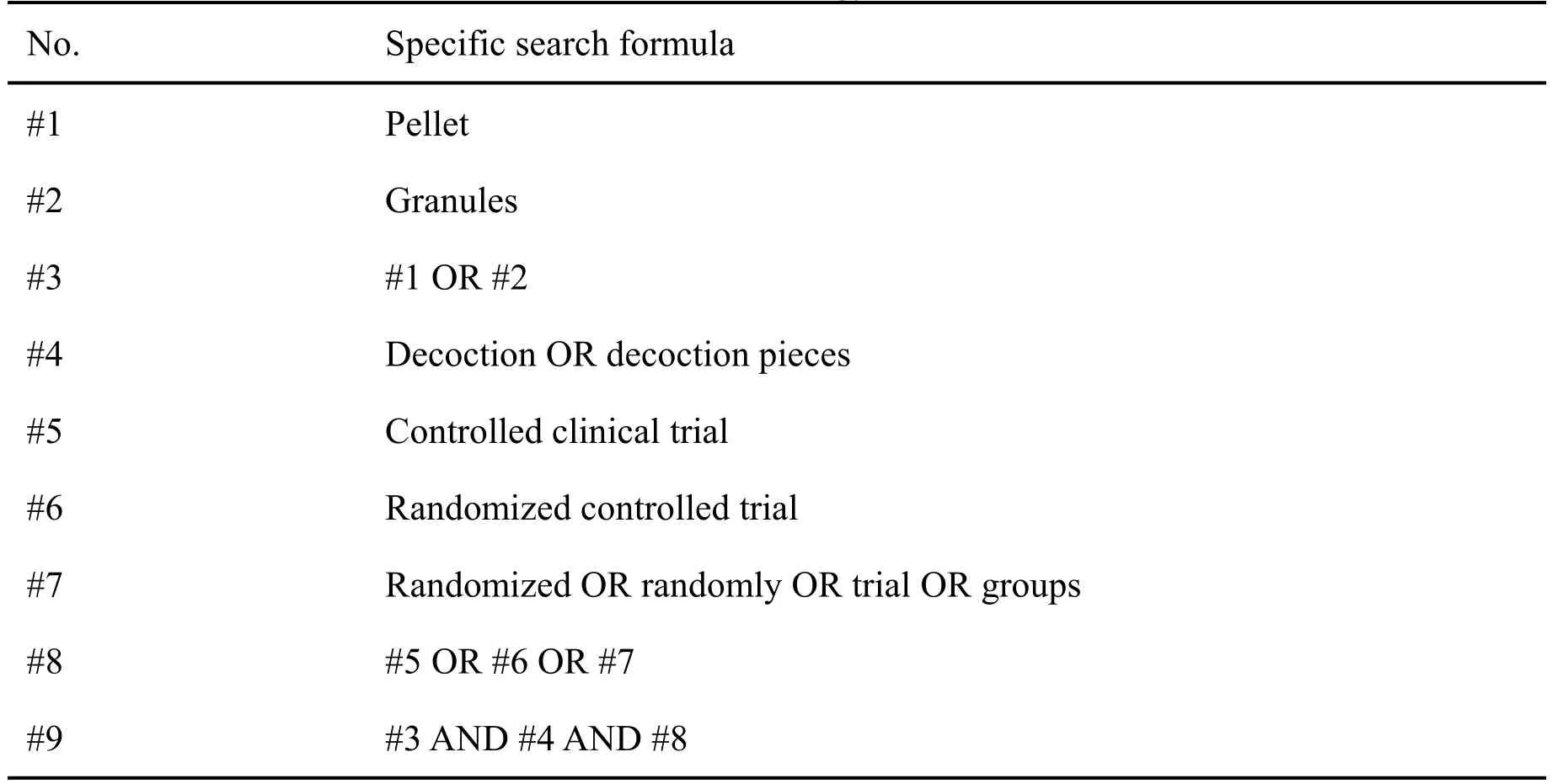
Table 1 Search strategy in PubMed
Search strategy
A search for eligible articles on online databases was performed, including China National Knowledge Internet, WanFang, Chongqing VIP Information,PubMed, Embase, Cochrane Library, and Web of Science.A search for other potentially eligible articles was also performed on Google, Baidu, China Clinical Trial Registry,World Health Organization International Clinical Trials Registry Platform, ClinicalTrials.gov,and so forth. The search terms included “granule”,“granules”, “decocting-free granule”, “formula granule”, “traditional decoction”, “decoction”, “herbal pieces”, “TCM herbal pieces”, “trial”, “randomized”,“controlled”, and so forth. Taking PubMed as an example, the specific search strategy is shown in Table 1.
Article screening and data extraction
Article screening and data extraction were completed independently by 2 investigators. First, the articles found in databases were entered into Endnote reference management software.Repeated articles were removed after the author, title, publication year, and abstract were checked. Next, ineligible articles were removed after title and abstract were consulted. Finally, eligible articles were obtained by reading the full text.The data extracted mainly included the publication year, first author, intervention measures, sample size, and outcome indicators.
Methodological quality assessment
The risk of bias of eligible articles was assessed with the bias assessment tool in the Cochrane Handbook 5.1.0. The tool was used to assess the content of the articles, including random sequence generation,allocation concealment, masking of subjects and investigators, masking of outcome assessors,incomplete outcome data, selective reporting, and other bias.The assessment result of each item was low risk,high risk,or unclear risk.
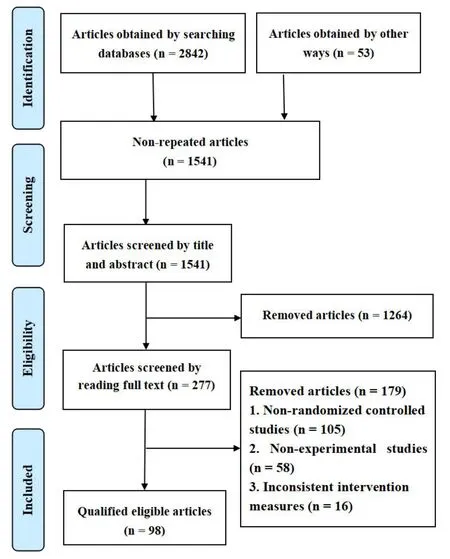
Figure 1 Flow chart of article screening
Statistical analysis
The meta-analysis was performed with RevMan 5.3 software. When there was no clinical heterogeneity in the studies, a meta-analysis was performed to merge data of 2 or more articles to evaluate the combined efficacy. The mean difference was used as the effect size for quantitative data. The relative risk (RR) was used as the effect size for qualitative data.Heterogeneity was assessed with chi-squared test andI2. IfI2was less than or equal to 50% and thePvalue obtained from the chi-squared test was greater than 0.05, data were merged using the fixed effects model.Otherwise, data were merged using the random effects model.
Results
Search results of articles
As shown in Figure 1, a total of 2,895 potentially eligible articles were searched in this study. After removal of 1,354 repeated articles and 1,264 articles that were found to be ineligible after checking the title and abstract according to the inclusion and exclusion criteria, 98 eligible articles were finally included after checking the full text of the remaining 277 articles.
Features of the included articles
As shown in Figure 2, the number of related articles has increased significantly in the past 5 years. As shown in Figure 3, in 66 randomized controlled trials ,8 different diseases were investigated, such as common cold, migraine, hypertension, gastrointestinal diseases, etc. Most of the intervention measures were based on syndrome differentiation and fixed prescription, and clinical efficacy was the evaluation index.The specific publication year and first author of the included articles are shown in Table 2.
Methodological quality assessment
Table 3 shows a random grouping of the case allocation in all articles. The allocation concealment,blind method, reporting bias, and so forth, are unknown in almost all of the included articles. The quality of the articles is relatively low.
Meta-analysis results of anemopyretic cold
As shown in Figure 4, the RR of using TCM granules or herbal pieces for the cold virus was reported in a total of 31 studies [13–43]. The test for effect size showedZ= 3.62, RR = 0.97, and 95% confidence interval (CI) = 0.94 to 1.01. The difference was not statistically significant(P=0.10).
This study showed that adverse events were reported in a total of 7 cold-related articles [37–43], of which 5 articles showed no adverse events in the experimental group or control group, and 1 article [43] showed that there was no statistical significance between the experimental group and control group in the incidence of adverse events.
Meta-analysis results of migraine
As shown in Figure 5,the RR of using TCM granules or herbal pieces for migraine was reported in a total of 12 studies[44,46–55].The meta-analysis showed that the RR was slightly higher in the experimental group than that in the control group, and the difference was statistically significant (RR =1.04, 95% CI =1.01 to 1.08,P= 0.02).As shown in Figure 6, the migraine duration was reported in a total of 11 studies[45–55].The meta-analysis showed that the experimental group had better reduction of migraine duration than that in the control group (mean difference(MD)=-0.30,95%CI = -0.52 to -0.08). The difference was statistically significant(P=0.008).
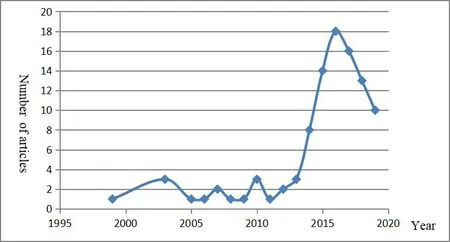
Figure 2 Distribution of articles by year
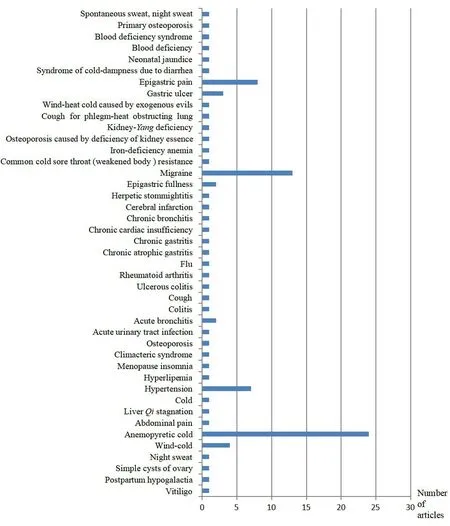
Figure 3 Distribution of the illnesses studied in the literature
Migraine frequency was reported in 11 [45–55] of the included studies, and the meta-analysis was performed with the random effects model due to the large amount of heterogeneity between these studies. As shown in Figure 7, the migraine frequency was slightly lower in the experimental group than in the control group (MD= -0.55, 95% CI = -1.39 to 0.29), and the difference was not statistically significant(P=0.20).
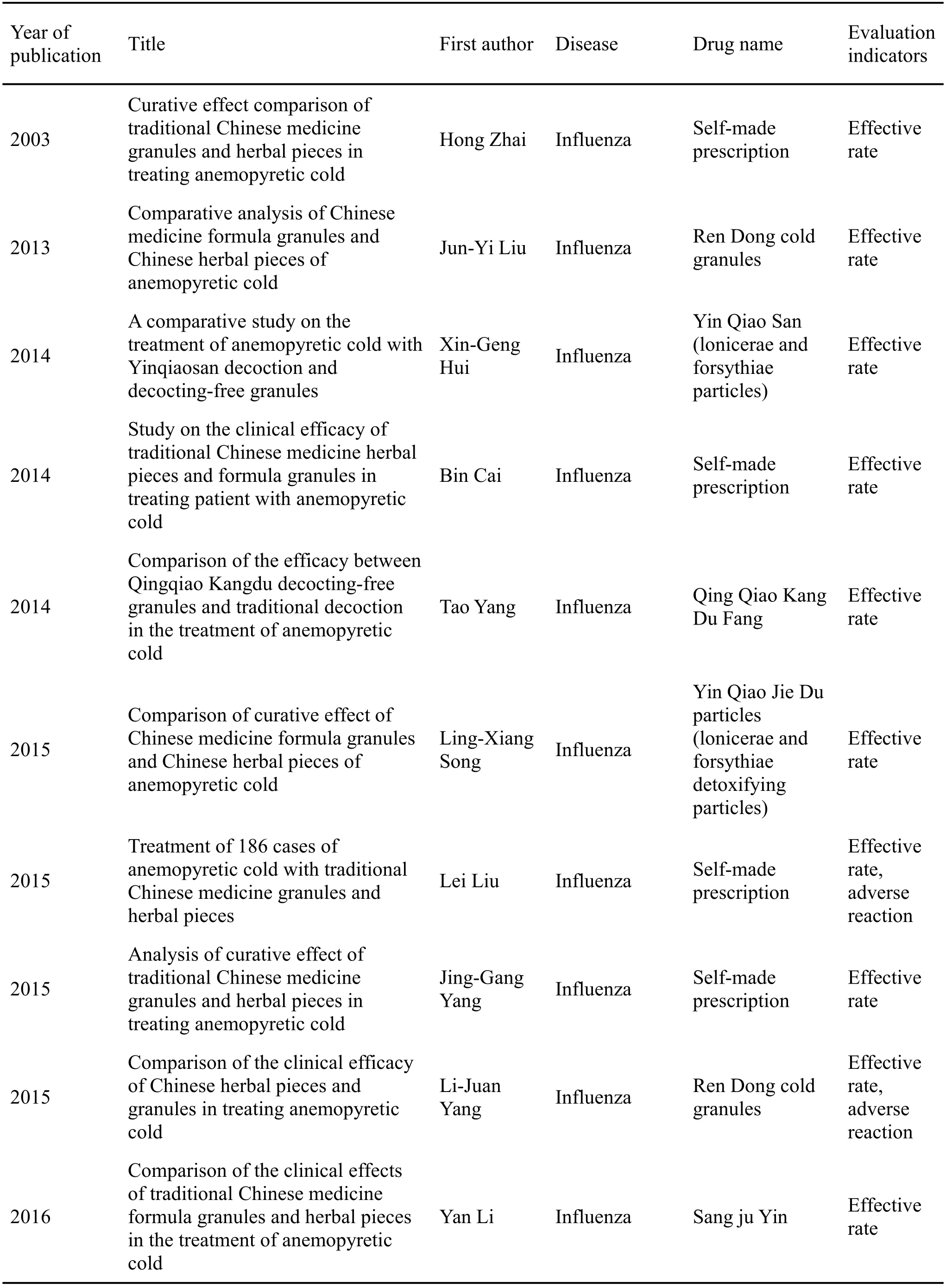
Table 2 Features of literature included in this study
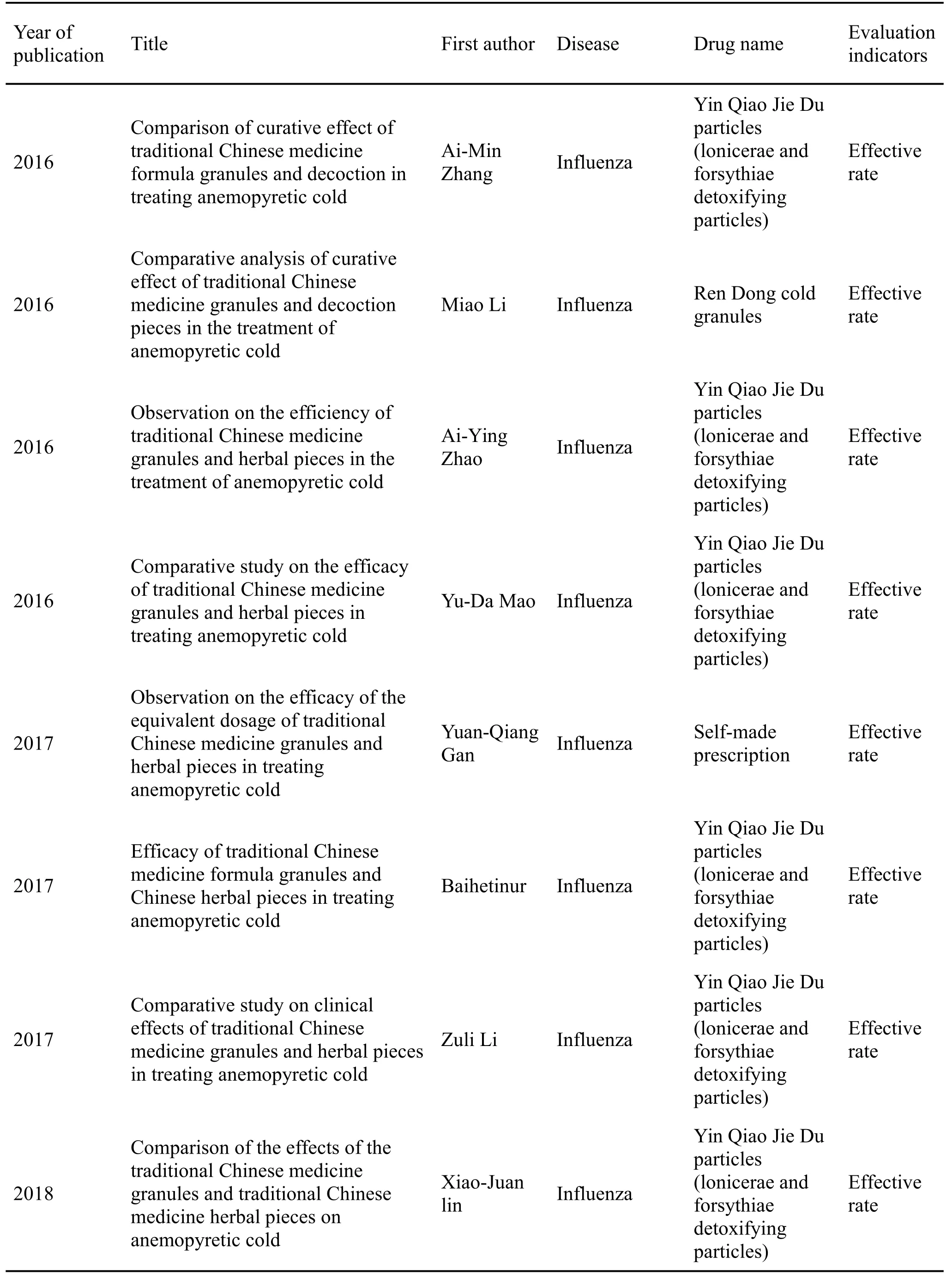
Table 2 Features of literature included in this study(continued)
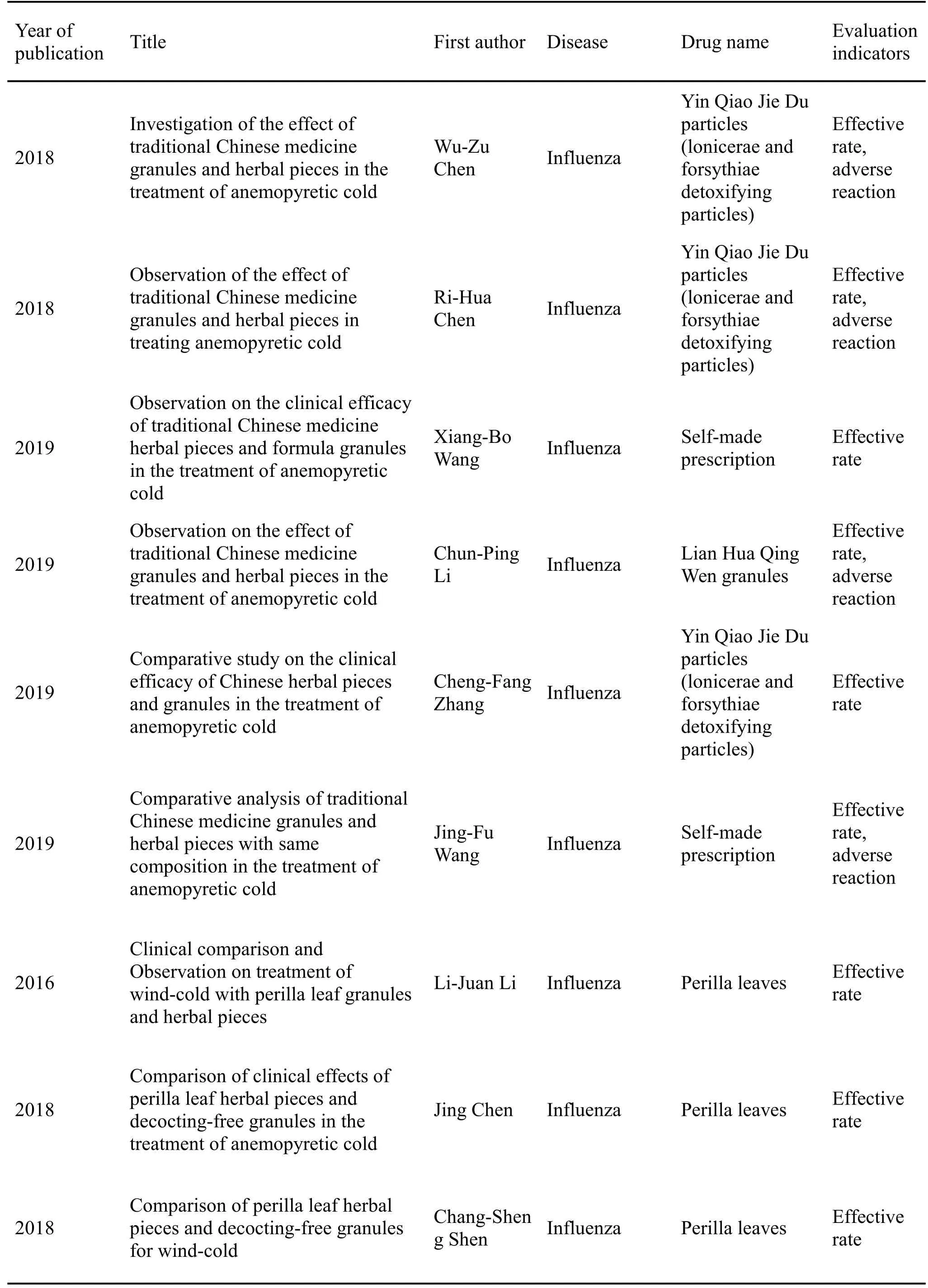
Table 2 Features of literature included in this study(continued)

Table 2 Features of literature included in this study(continued)
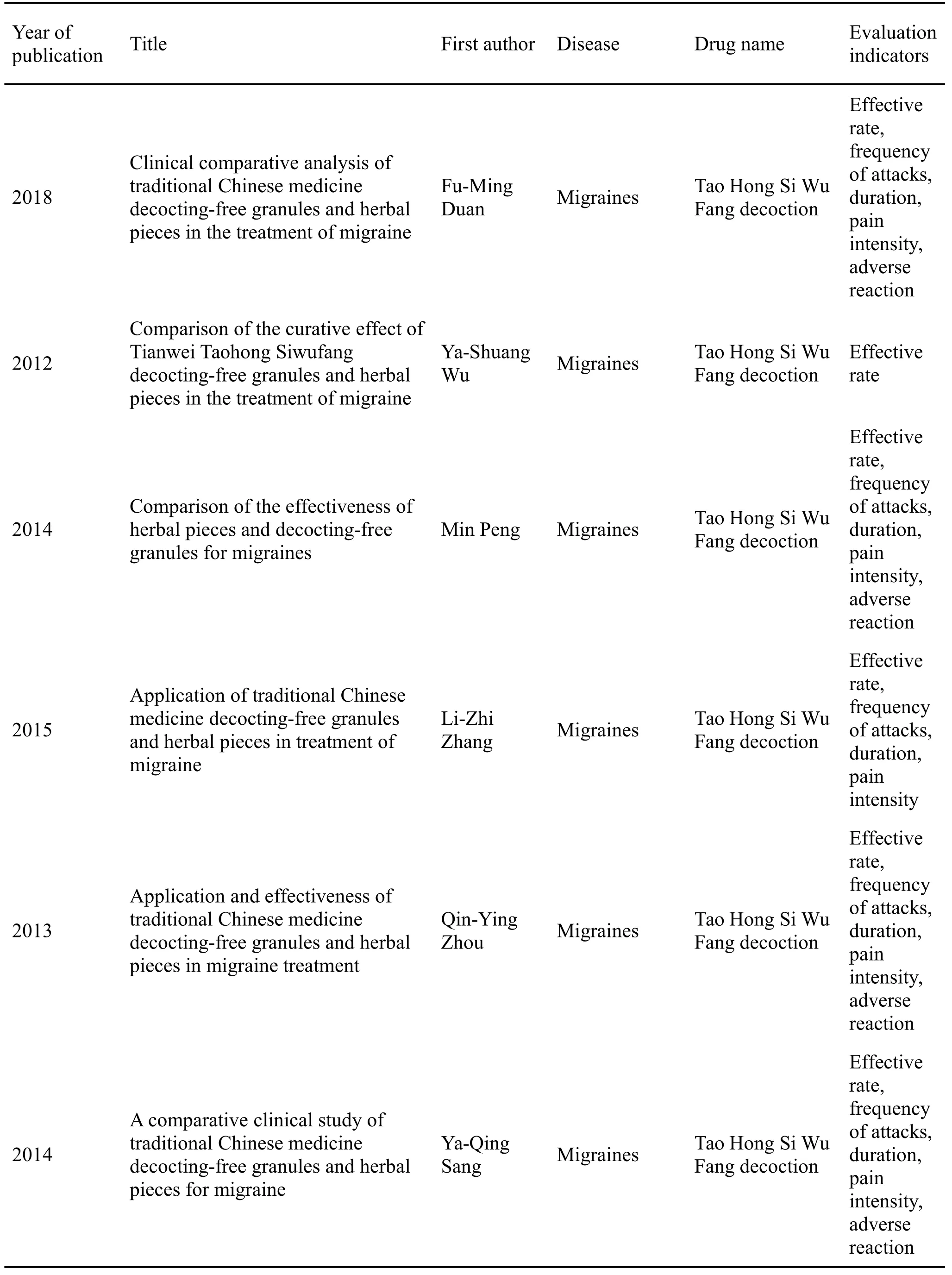
Table 2 Features of literature included in this study(continued)
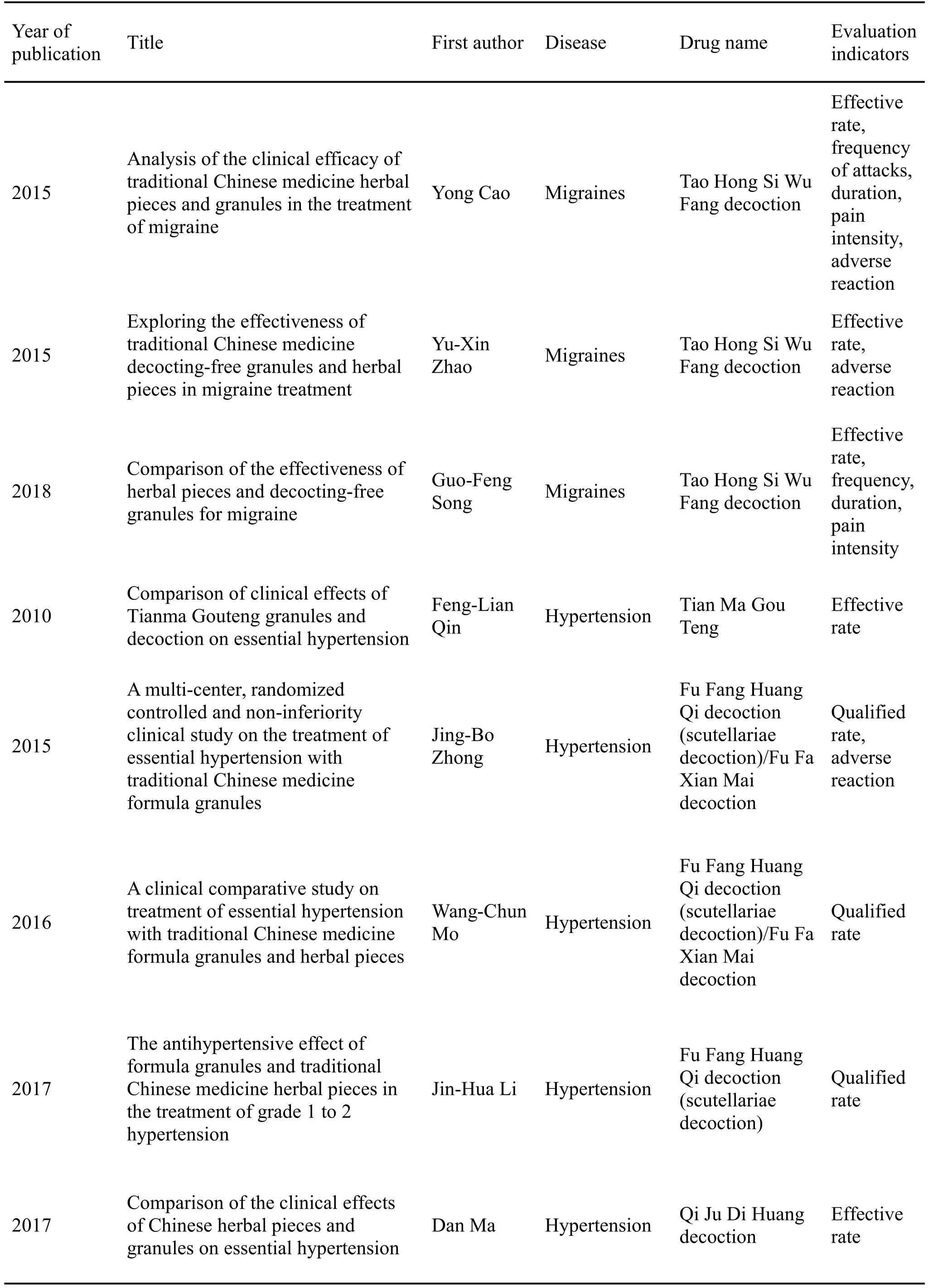
Table 2 Features of literature included in this study(continued)
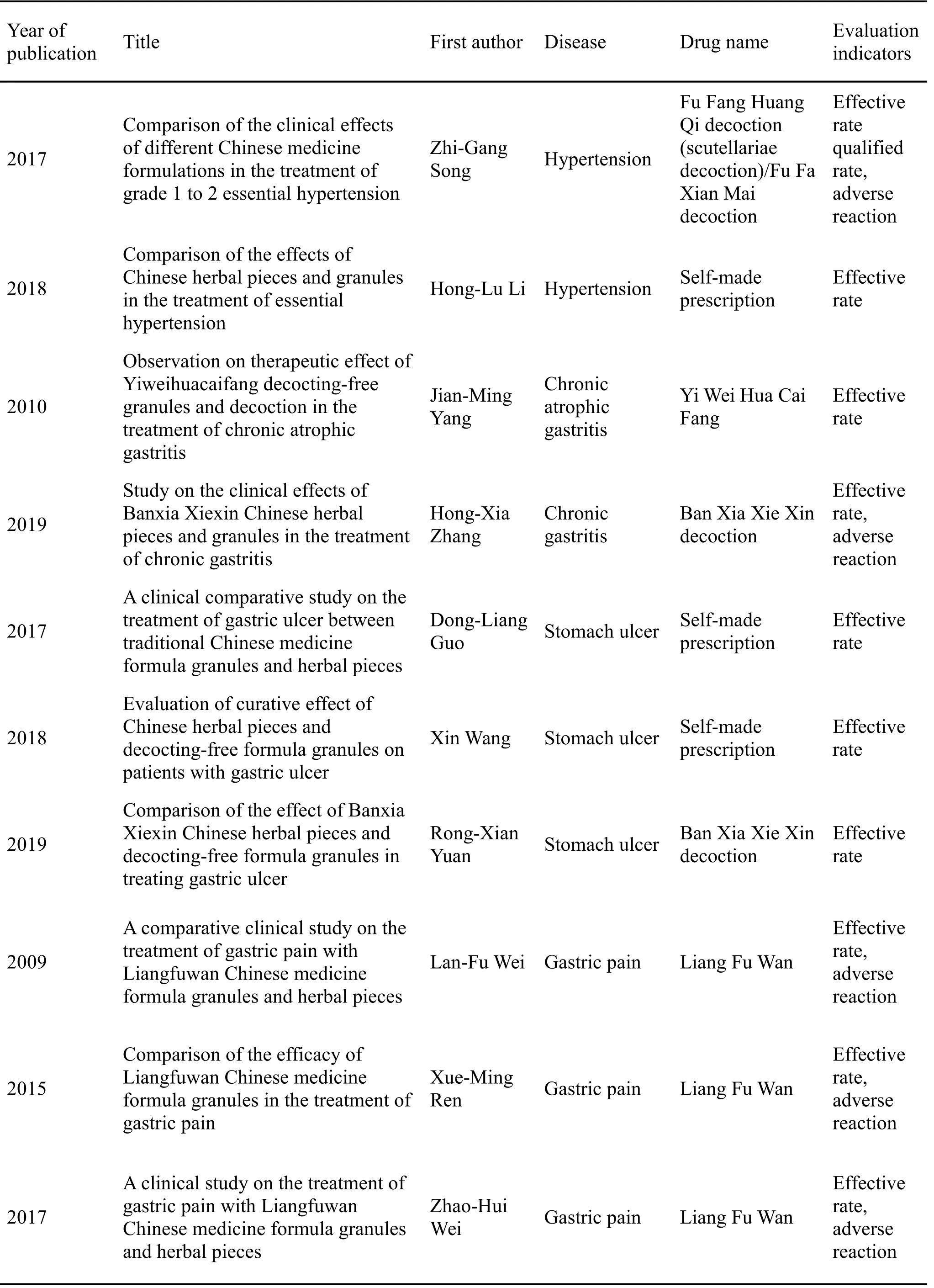
Table 2 Features of literature included in this study(continued)

Table 2 Features of literature included in this study(continued)
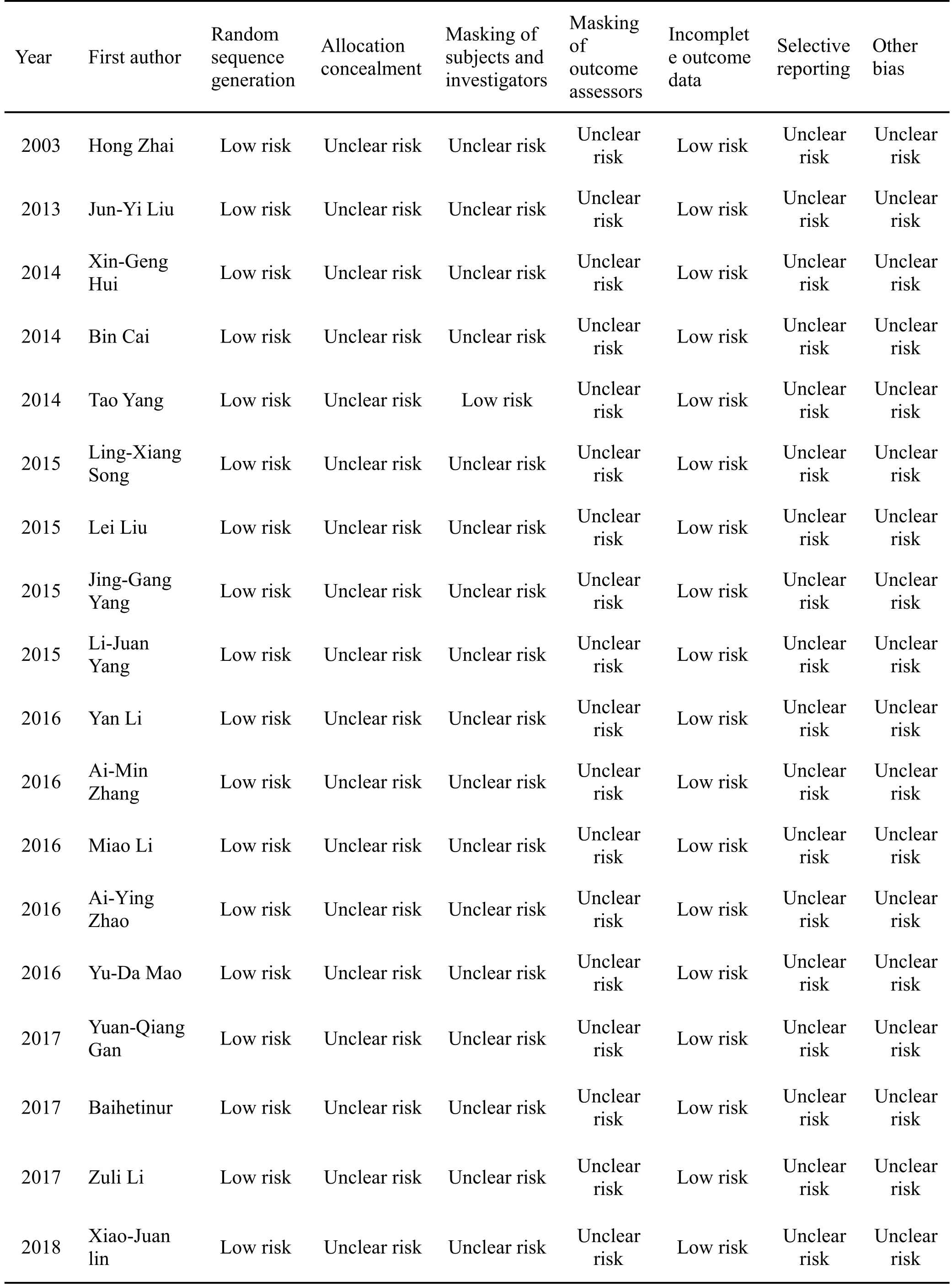
Figure 3 Features of the included articles
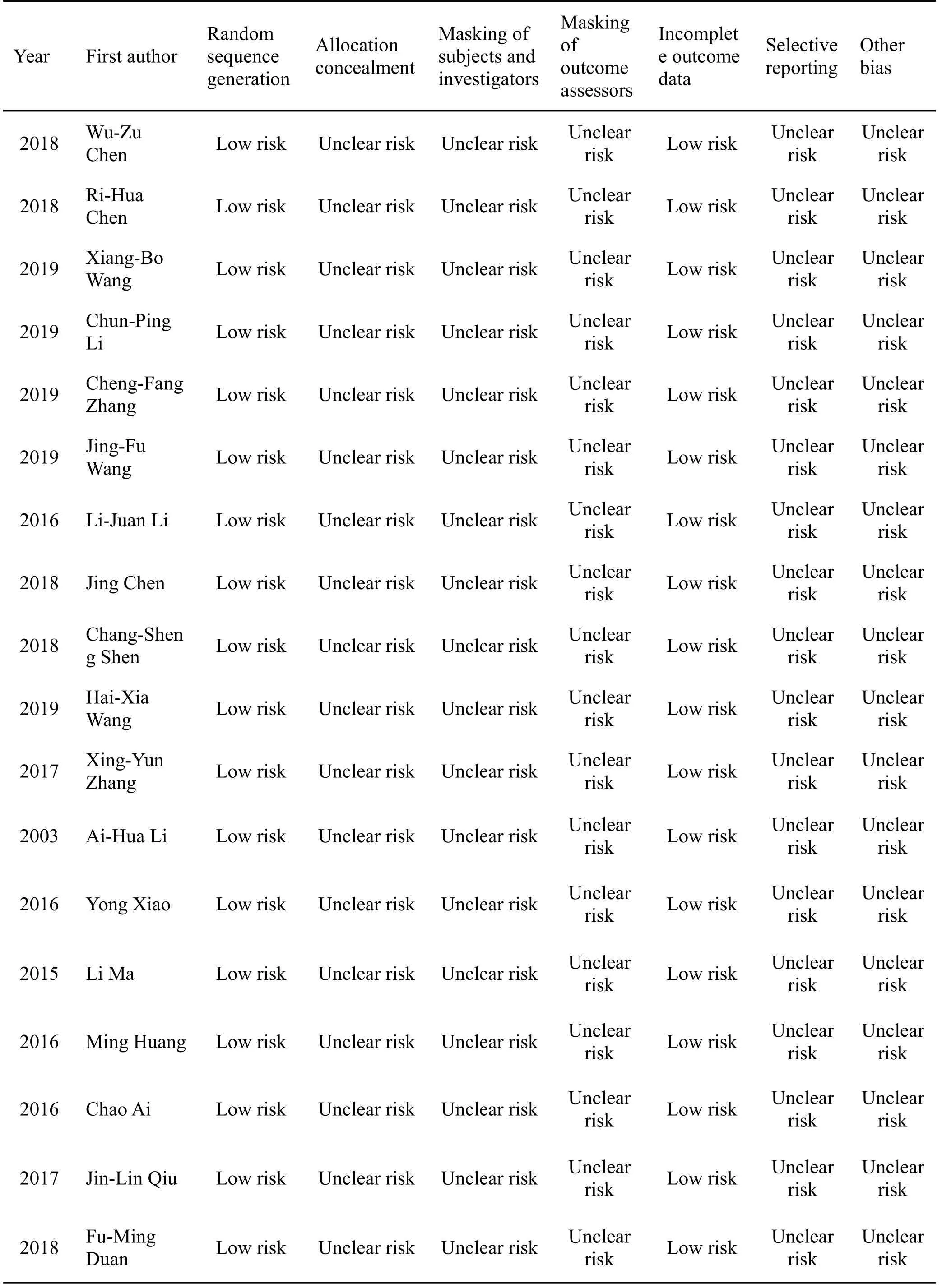
Figure 3 Features of the included articles(continued)
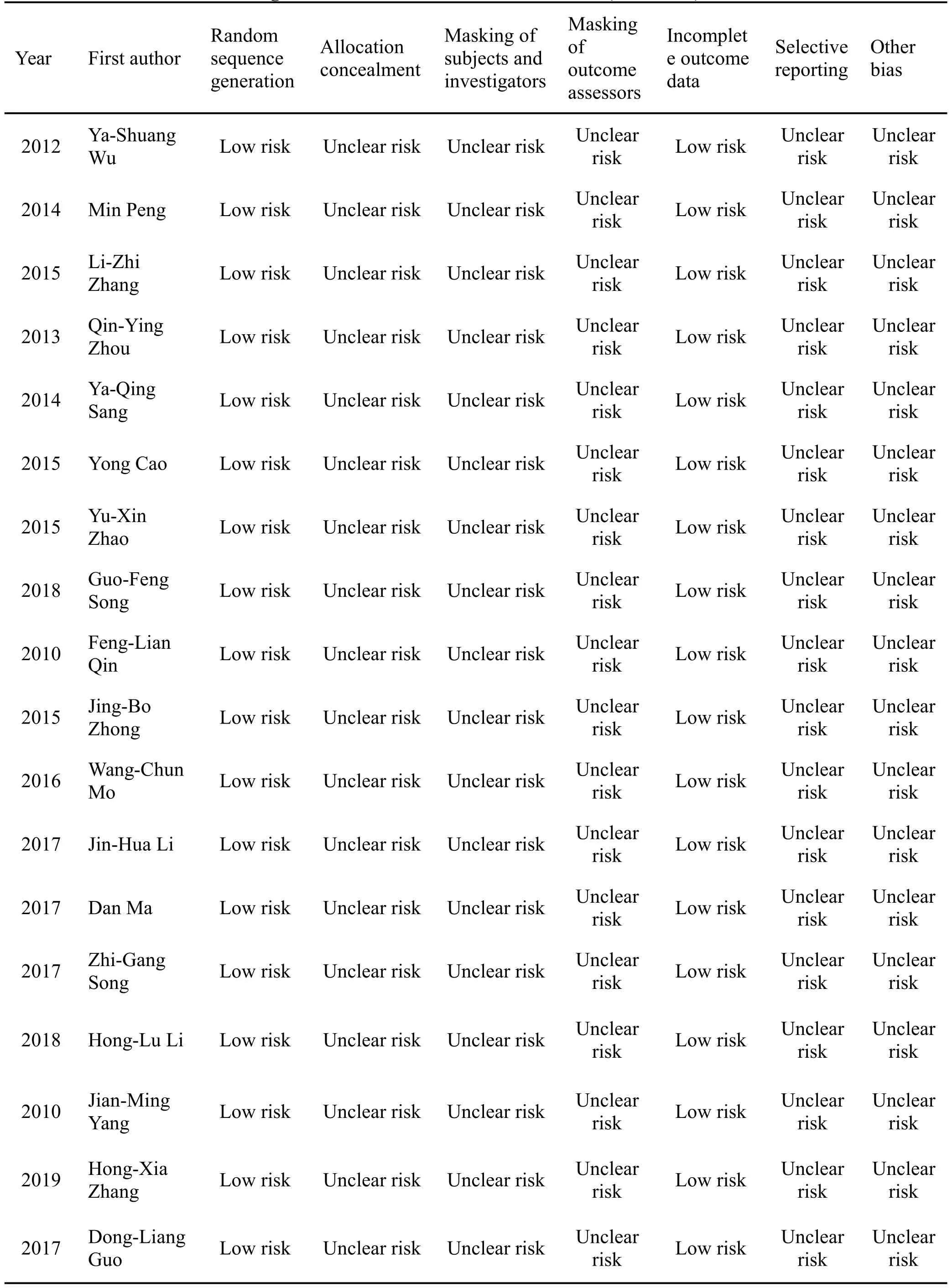
Figure 3 Features of the included articles(continued)
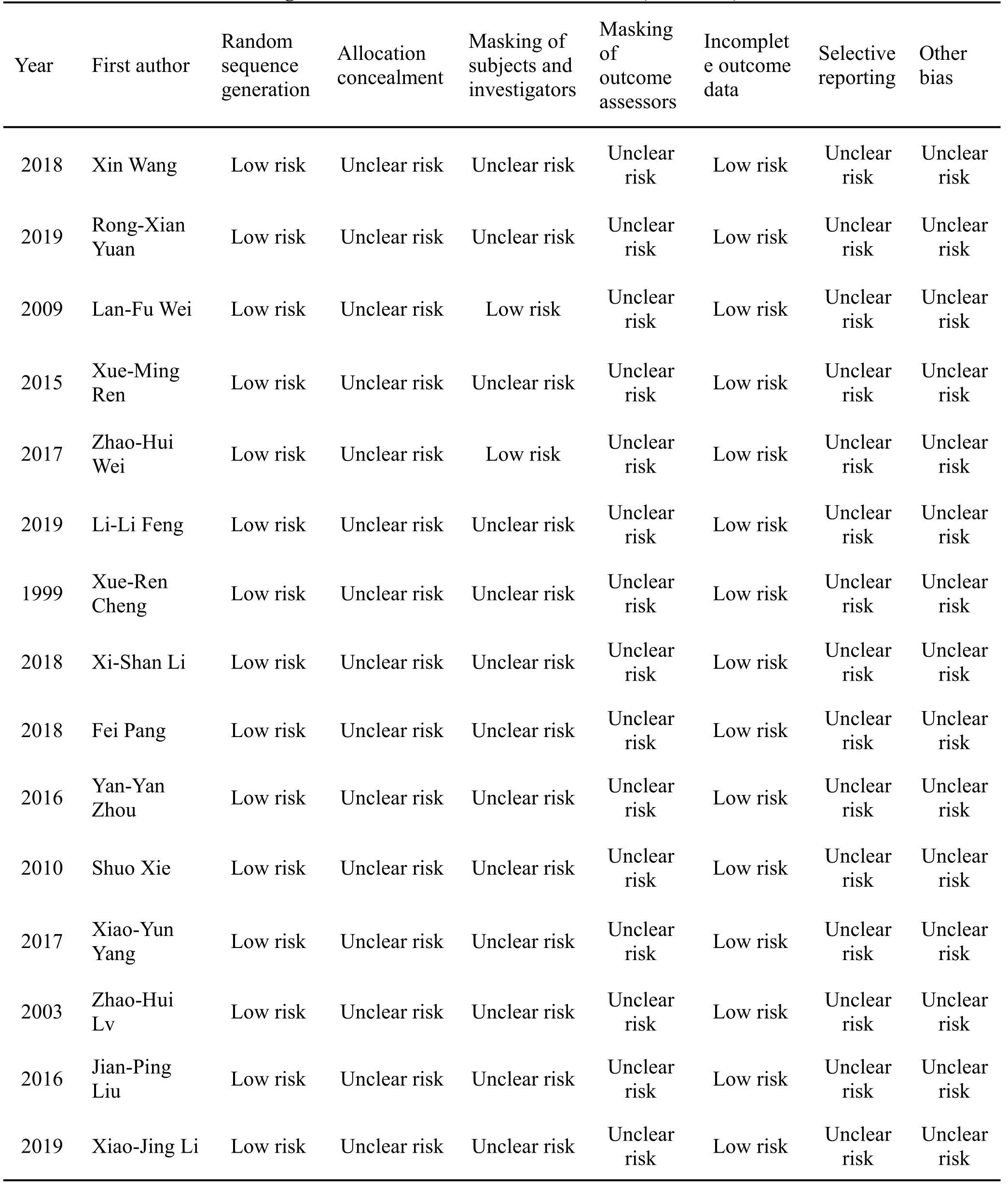
Figure 3 Features of the included articles(continued)
The migraine pain level was reported in a total of 11 studies [45–55]. As shown in Figure 8, there was no statistically significant difference between the experimental group and control group in improving the pain level of patients with migraines (MD = -0.12,95%CI=-0.48 to 0.23,P=0.49).
This study showed that adverse events were reported in a total of 7 [50–56] migraine-related articles, no adverse event was found in the experimental group or control group in 2 articles [50, 51], and the difference in adverse events between the two groups was not statistically significant in 5 articles[52–56].
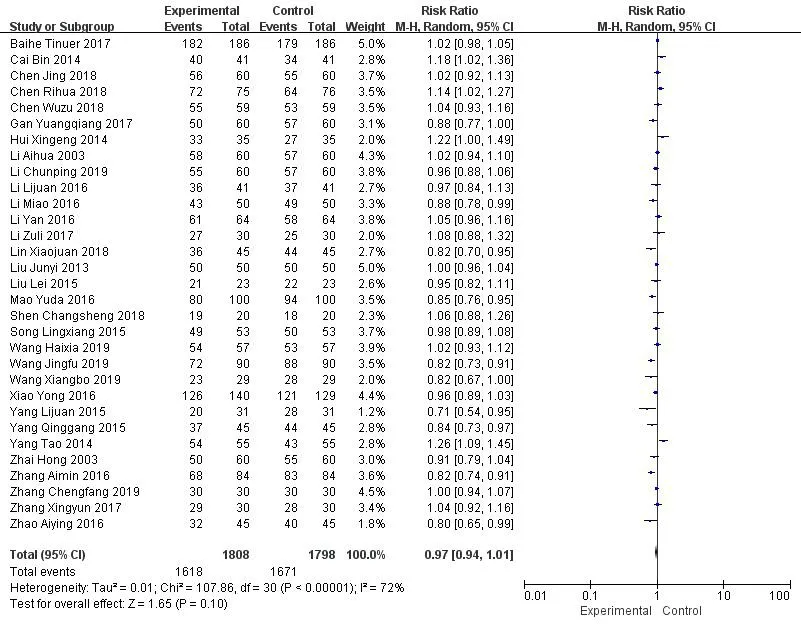
Figure 4 Meta-analysis of literatures that investigated the relative risk (RR) of using TCM granules or herbal products for the cold virus
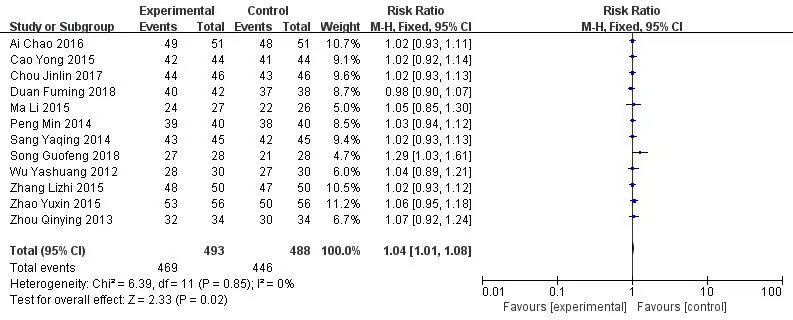
Figure 5 Meta-analysis of the relative risk(RR)of using TCM granules or herbal products for migraine
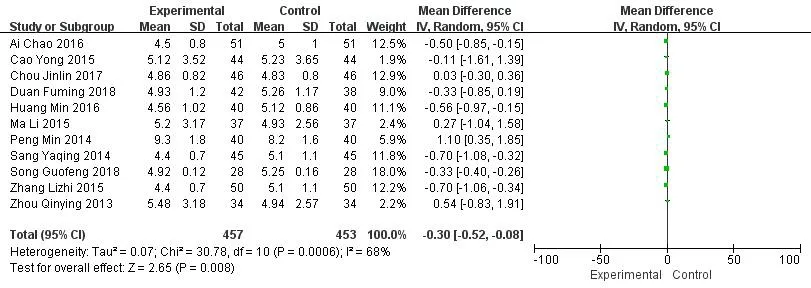
Figure 6 Meta-analysis of migraine duration
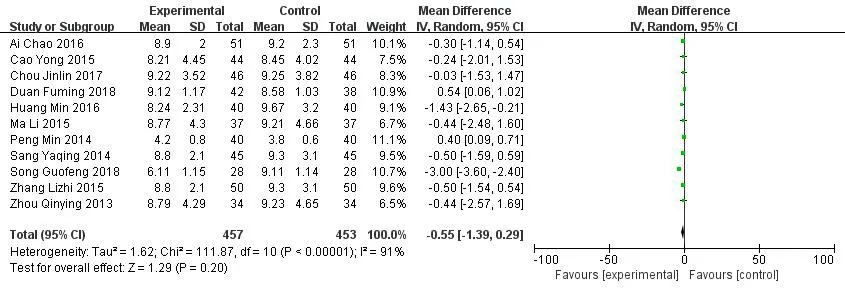
Figure 7 Meta-analysis of migraine frequency
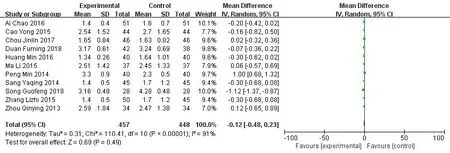
Figure 8 Meta-analysis of migraine pain level
Meta-analysis results of hypertension
As shown in Figure 9, the RR of TCM granules or herbal pieces for hypertension was reported in a total of 4 studies [57–60]. The test for effect size showedZ= 0.97 (P= 0.33), RR = 1.03, and 95% CI = 0.97 to 1.10,and the difference was not statistically significant(P= 0.33). The control rate of hypertension was reported in a total of 4 articles [60–63]. As shown in Figure 10,the control rate of hypertension was slightly higher in the experimental group than that in the control group, and the difference was not statistically significant (RR = 1.04, 95% CI = 0.95 to 1.12,P=0.41).
This study showed that adverse events were reported in a total of 2[60,61]hypertension-related articles,and the results showed the differences between adverse events in the experimental group and control group were not statistically significant.
Meta-analysis results of diseases of the digestive system
As shown in Figure 11,the RR of using TCM granules or herbal pieces for diseases of the digestive system was reported in a total of 15 studies [64–78]. The meta-analysis showed that TCM granules had a higher RR when used with gastric ulcer than TCM herbal pieces, and the difference was statistically significant(RR=1.12,95%CI=1.06 to 1.19,P<0.000,1).
According to the subgroup analysis, the RR for epigastric pain was reported in a total of 8 [64–71]studies. The results showed that the control group had a lower RR with epigastric pain than the experimental group, and the difference was statistically significant(RR = 1.15, 95% CI = 1.07 to 1.25,P= 0.000,3). Six articles [65–70] showed that no adverse event was observed in either group. One article [71] showed that the incidence of adverse events was lower in the experimental group than that in the control group, and the difference was statistically significant. The RR for gastritis was reported in 2 studies [72, 73], and the meta-analysis showed that RR in the experimental group was similar to that in the control group, and the difference was not statistically significant (RR = 1.05,95% CI = 0.91 to 1.21,P= 0.52). In 1 article, there was no adverse event [72]. The RR for colitis was reported in 2 studies [74, 75]. The test for effect size showedZ=0.59(P=0.55),RR=0.98,and 95%CI=0.90 to 1.06, and the difference was not statistically significant(P=0.55),indicating that the RR for colitis in the experimental group was similar to that in the control group. Adverse events were reported in 1 article, slight tenesmus occurred in 3 patients, 2 had taken ultrafine granule decoction, and 1 had taken traditional decoction.The adverse event occurred at 30 min after enema, lasted for around 1 h, and was relieved after defecation.No other adverse events were found after drug withdrawal.
Meta-analysis results of osteoporosis
As shown in Figure 12, the RR for osteoporosis was reported in a total of 3 studies [79–81]. The meta-analysis showed that the RR for osteoporosis in the experimental group was similar to that in the control group, and the difference was not statistically significant (RR = 1.00, 95% CI = 0.93 to 1.07,P=0.96).In 1 article there was no adverse event[80].One article [81] reported that the incidence of adverse events was lower in the experimental group than that in the control group, and the difference was statistically significant.
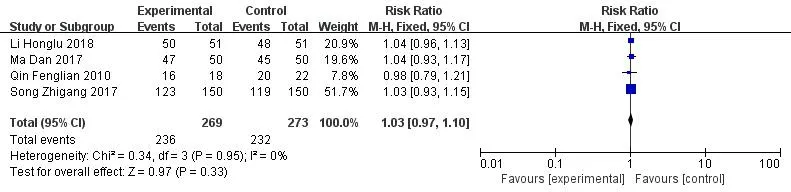
Figure 9 Meta-analysis of the relative risk of using TCM granules or herbal products for hypertension
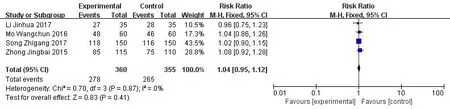
Figure 10 Meta-analysis of control rate of hypertension
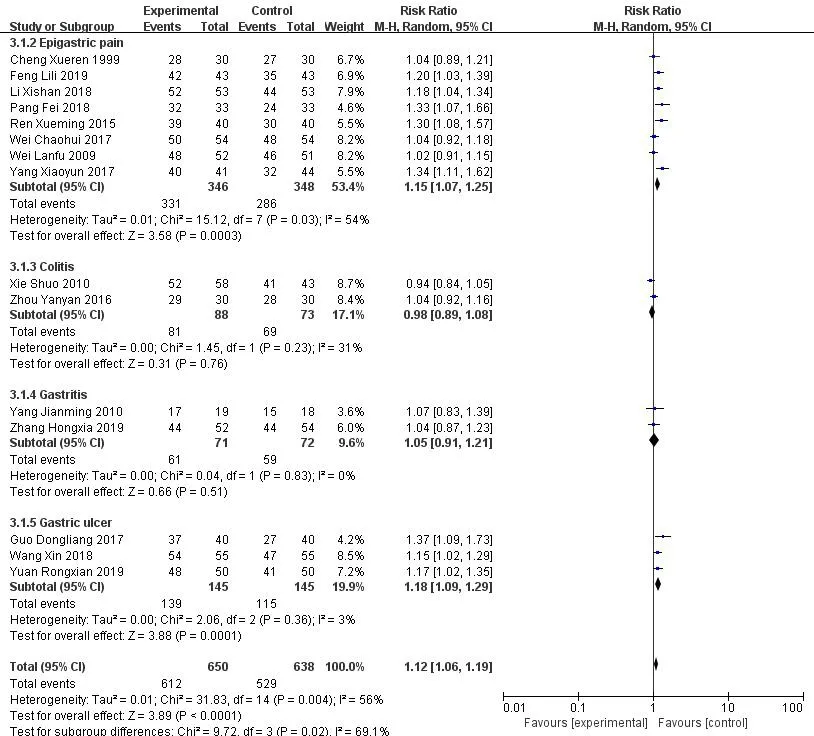
Figure 11 Meta-analysis results of diseases of the digestive system
Discussion
Guided by theories of traditional Chinese medicine,formula granules are a new formulation of TCM,which are made through extraction, separation,concentration, drying, granulation, and sealing. They are instant and portable. Formula granules retain the properties and efficacy of TCM herbal pieces and are easy to store and carry. However, whether they can replace TCM herbal pieces in traditional Chinese medicine clinical practice has become a question among doctors and patients in recent years[82,83].
Firstly, in terms of active ingredients, TCM herbal pieces are made under the guidance of TCM theory,which can increase the efficacy, decrease the toxicity,and change the properties by producing a series of physical and chemical changes in the mixed decoction,where precipitates or new ingredients may form[84–86]. Studies have shown that when rhubarb and aconite are decocted together, tannic aconitine salt is produced, which cannot be absorbed by the intestine and reduces the toxicity of aconite [87]. Using the KPLC method, Pei-Xue Caoet al.[88] determined that the content of glycyrrhizic acid produced in a mixed decoction of Ma-Huang-Tang was higher than that in a separate decoction, which enhanced immune functions of cells, but the specific mechanism was unknown.Other studies have shown that a new substance,5-hydroxymethylfurfural, is produced in the mixed decoction of sheng-mai san, which improves the overall effect of the compound[89].
Secondly, in terms of clinical efficacy, TCM granules are a mixture of single medicines extracted separately. They lack the interactions of mixed decoctions, and therefore their clinical efficacy has been long questioned by patients and medical professionals. Several systematic reviews on the comparison of clinical efficacy between TCM granules and herbal pieces have been published [90–92].However, in our study there were problems reviewing this literature, such as a small number of included articles, single type of disease, and incomplete searches. In this study, the type of disease involved was used as the stratifying factor, and the results of similar studies were analyzed using meta-analysis.
66 RCTs were included to compare the TCM granules and decoctions. Eight types of disease were investigated. Most trials had a low methodological quality. Meta-analysis showed that compared with TCM herbal pieces, TCM granules had similar effectiveness and safety in treating colds,hypertension,and osteoporosis, but higher RR for migraine, a better effect for reducing migraine duration, and higher RR for diseases of the digestive system, with an especially better effect in treating epigastric pain and gastric ulcer.Meta-analysis is a clinical evidence-based secondary analysis method and the preferred way to gather evidence in evidence-based medicine; however,it does not help us understand the mechanisms involved.Although we consulted a lot of relevant articles, we still failed to find the reason why granules are effective for migraine and diseases of the digestive system.This may be partly attributable to the relatively large sample size of the TCM granules and herbal pieces, which provided us with reliable conclusions. The value of granules in other diseases may be gradually revealed as research increases.
The traditional decoction method of Chinese medicine has a low yield of fat-soluble ingredients,and volatile oil is easily lost due to the decoction. Modern pharmacological studies have confirmed that a large amount of fat-soluble ingredients and volatile oil can penetrate the blood-brain barrier and ease pain[93–95].During the extraction of granules, volatile oil can be efficiently extracted by means such as distillation, and fat-soluble ingredients can also be efficiently extracted by using solvents such as alcohol. Traditional decoction leaves many impurities, causing irritation to the stomach. When the impurities are eliminated, the granules don’t irritate the stomach, which may be one of the reasons why granules are better than herbal pieces in treating gastric ulcers.
There is a publication bias because the articles included in this study have limited clinical samples,low methodological quality, and insufficient evidence.It is difficult for investigators to merge data, because different diseases are studied with different prescriptions. Some of the diseases in the included articles are self-limited diseases,and so it is difficult to determine whether the granules or herbal pieces work.Results of most articles are symptom-related or patient-reported, which may also cause a certain bias.Based on the above factors, no definite conclusion can be drawn that TCM granules can replace TCM herbal pieces. However, it is suggested that TCM granules may be similar to herbal pieces as far as effectiveness and safety. In order to increase the clinical application value of TCM granules, more well-designed,large-scale, multi-center RCTs are needed [96, 97].Compared with TCM herbal pieces,TCM granules are easy to take, easy to store, are stable and controllable,and can improve the patient’s compliance.
Conclusion
In summary, traditional Chinese medicine granules are just as effective and safe as traditional decoctions, and they are better than traditional decoctions in treating migraine and digestive system diseases. However, due to the low quality of randomized control in the investigated studies, more evidence is still needed to prove their effectiveness and safety in order to promote the development of Chinese medicine.