
Large lingual heterotopic gastrointestinal cyst in a newborn:A case report
2020-09-18 08:03AtsushiDoksaLeeKazumaHaradaSusumuTanakaYusukeYokotaTakashiMimaAkifumiEnomotoMikihikoKogo
World Journal of Clinical Cases 2020年17期
Atsushi-Doksa Lee,Kazuma Harada,Susumu Tanaka,Yusuke Yokota,Takashi Mima,Akifumi Enomoto,Mikihiko Kogo
Atsushi-Doksa Lee,Kazuma Harada,Susumu Tanaka,Yusuke Yokota,Mikihiko Kogo,First Department of Oral and Maxillofacial Surgery,Graduate School of Dentistry,Osaka University,Suita 565-0871,Osaka,Japan
Atsushi-Doksa Lee,Akifumi Enomoto,Department of Oral and Maxillofacial Surgery,Faculty of Medicine,Kindai University,Osaka-Sayama 589-8511,Osaka,Japan
Takashi Mima,Department of Oral and Maxillofacial Surgery,Daini Osaka Police Hospital,Osaka 543-8922,Osaka,Japan
Abstract
Key words:Tongue cyst;Congenital cyst;Prenatal diagnosis;Airway management;Gastrointestinal epithelium;Case report
INTRODUCTION
Heterotopic gastrointestinal cysts have gastrointestinal epithelium in the cyst wall and rarely occur in the oral cavity[1].When heterotopic gastrointestinal cysts do occur in the oral cavity,they frequently occur in the anterior part of the tongue and are mainly found in the neonatal period;however,some cases become asymptomatic in adulthood[2,3].The diagnosis of a heterotopic gastrointestinal cyst as a congenital tongue cyst by routine ultrasonography is extremely rare[4-10].Congenital tongue cysts can cause respiratory distress and require multidisciplinary treatment for airway management.Intratracheal intubation and reduction procedures may be required immediately after delivery[5-7,9].The treatment is complete surgical resection,and there are very few cases of recurrence[2].However,there is no consensus on the optimal timing of surgery and the effectiveness of preoperative cyst reduction procedures.Herein,we report a rare case of a congenital heterotopic gastrointestinal cyst of the tongue.Cyst aspiration successfully avoided airway distress and feeding difficulty.
CASE PRESENTATION
Chief complaints
A 12-day-old female was referred to our hospital for tongue swelling.
History of present illness
The obstetrician had detected significant swelling of the tongue on fetal ultrasonography performed in the 35thgestational week.Because of the anticipated high risk of breathing difficulty,the female was born by cesarean delivery at gestational week 39 in the presence of a pediatric surgeon.
History of past illness
The medical and obstetric history of the mother was unremarkable,with no family history of any congenital anomalies.The patient had no other congenital anomalies.
Physical examination
The cystic legion was located hypoglossally and measured 15 mm × 25 mm.The cyst elevated the tongue and occupied the oral cavity,preventing the mouth from closing(Figure 1A).She became dyspneic soon after delivery,and so the pediatric surgeon aspirated the cyst (Figure 1B).

Figure 1 Neonatal appearance at birth.A:The tongue cyst occupies the oral cavity before needle aspiration;B:Tongue cyst aspiration with an 18-gauge indwelling needle.
Laboratory examinations
Histopathologic examination showed that the specimen was a true cyst,and that its wall consisted of a lining of columnar gastrointestinal-type epithelium and pseudostratified ciliated epithelium (Figure 2).
Imaging examinations
Magnetic resonance imaging (MRI) performed on the 24thday showed that the 25 mm circular-shaped cyst was located hypoglossally without expansion in the oral floor(Figure 3).
FINAL DIAGNOSIS
The final diagnosis was a heterotopic gastrointestinal cyst of the tongue.
TREATMENT
To avoid the repetition of aspiration,immediate surgical resection was recommended.However,the mother of the patient did not want her to undergo surgery in the neonatal period.Thus,a second aspiration was performed on the 7thday.However,the cyst was found to be gradually increasing in size,the excision procedure was performed with the patient under general anesthesia on the 67thday.The tongue was pulled forward and an incision was made on the anterior midline under the tongue.The submucosal tissue was bluntly dissected until the cyst wall was observed(Figure 4A).The cyst was excised by dissecting the connective tissue (Figure 4B).The cyst contained viscous dark brown fluid.The wound was sutured with absorbable thread.
OUTCOME AND FOLLOW-UP
The patient was able to breastfeed 3 h after surgery.The postoperative course was uneventful,and there has been no recurrence during 5 years of follow-up.
DISCUSSION
The reported congenital cystic lesions of the tongue include a ranula[11],teratoma[12],thyroglossal duct cyst[13],lymphangioma[14],and heterotopic gastrointestinal cyst.However,heterotopic gastrointestinal cyst of the tongue is rare[1].Although this type of cyst is most commonly referred to as a heterotopic gastrointestinal cyst,it is also known by various terms such as a foregut duplication cyst,choristomatic cyst,ciliated epithelial cyst,lingual duplication cyst,cystic tumor of the tongue,unusual thyroglossal duct cyst,heterotopic large bowel cyst,enterocystoma,and alimentarytract cyst[1,3].It is rare to see heterotopic gastrointestinal epithelium in the oral region,while it is more commonly reported in the duodenum,gallbladder,common bile duct,jejunum,Merkel diverticulum,ileum,appendix,colon,and rectum[15].The wall of a heterotopic gastrointestinal cyst may consist of a lining of ciliated epithelium and squamous epithelium in addition to gastrointestinal epithelium[3].The pathogenesis of a heterotopic gastrointestinal cyst is still unknown,but the cyst may arise from undifferentiated ectoderm lining of the primitive stomodeum that becomes entrapped within the oral cavity during the 4th week of fetal development[16].Most heterotopic gastrointestinal cysts are discovered by 2 years of age[3].The treatment is surgical resection.Possible surgical complications are Wharton's duct injury and lingual muscle injury.Preoperative MRI is helpful to show the expansion to adjacent structures and the localization of the cyst.Recurrence is rare with complete resection[1].
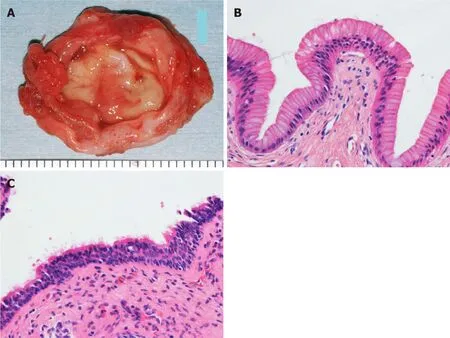
Figure 2 Pathological findings of the cyst.A:Gross anatomy of the excised cyst.The cyst wall is elastic and soft,and the lumen is smooth;B:Hematoxylineosin stained specimen showing columnar gastrointestinal epithelium lining the cyst wall (× 400 original magnification);C:Ciliated pseudostratified epithelium is also seen in another part (× 400 original magnification).

Figure 3 T2-weighted magnetic resonance imaging shows that the cyst is located at the ventral part of the anterior tongue.A:Horizontal view;B:Sagittal view.
Cases in which a heterotopic gastrointestinal cyst is detected in the prenatal period are extremely rare.To the best of our knowledge,there are only nine cases in which a lingual heterotopic gastrointestinal cyst has been diagnosed prenatally (Table 1)[4-10].Inall of these cases,a lingual cyst was detected with ultrasonography.Large cysts on the tongue may cause airway obstruction.Therefore,prenatal ultrasonographic diagnosis is essential to predict the risk of upper airway obstruction at delivery.Multidisciplinary collaboration is also essential to formulate a careful delivery plan that ensures airway protection in the neonate[7].Prenatal MRI is a useful way to evaluate the risk of airway obstruction[7-10].If an airway problem is detected with echo,an ex-utero intrapartum treatment procedure may provide time to open the infant’s airway while maintaining the placental blood supply[8].
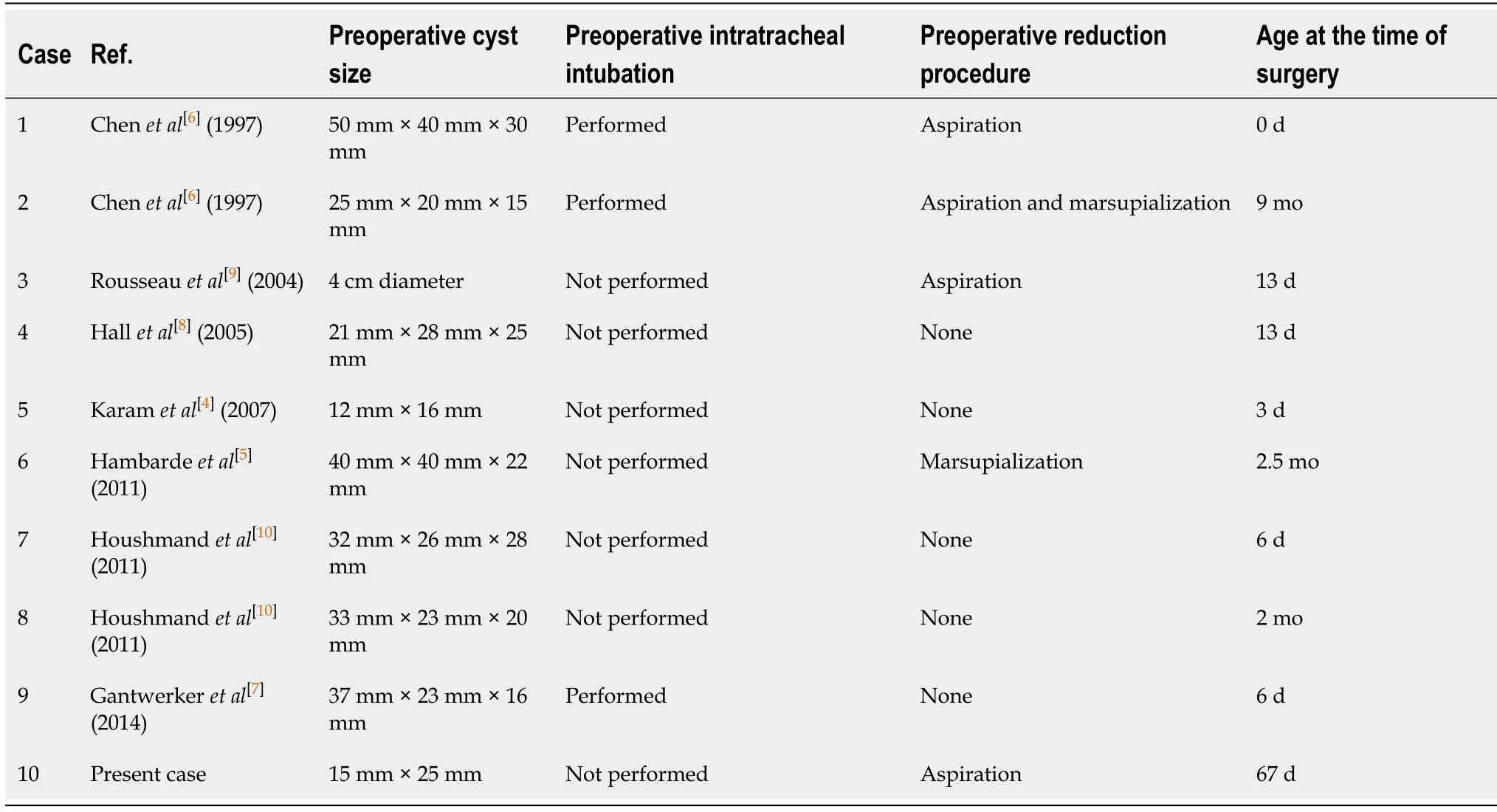
Table 1 Cases of heterotopic gastrointestinal cyst detected in the prenatal period

Figure 4 Intraoperative findings.A:A smooth cyst wall is observed after dissecting the tongue mucosa;B:Loose connective tissue is attached to the cyst.
In previous reports of lingual heterotopic gastrointestinal cysts,intubation was required for airway management in three of nine cases[6,7].The remaining seven patients were not intubated,as ultrasonographic imaging showed that there were no airway problems[4,5,8-10].Preoperative aspiration or marsupialization was performed in four cases,while aspiration alone was performed in two cases[5,6,9].All aspiration procedures were performed at birth.Our case was the only case in which aspiration was performed twice.The timing of cystectomy was within 2 wk in six cases[4,6-10].Around two months in three cases (including the present case)[5,10],and at nine months in one case[6].In all cases,there were no problems with the postoperative respiratory and nutritional statuses.Although previous reports did not describe the preoperative feeding status and intubation at the time of general anesthesia induction,the infant in our case was able to breastfeed just before the surgery,and oral intubation was easy despite the remaining swelling of the tongue.
In our case,immediate cyst aspiration was performed at birth,and the respiratorycondition and feeding function were stable;therefore,surgery was postponed.There is no consensus on the optimal timing of surgical removal of congenital tongue cysts,including heterotopic gastrointestinal cysts.Kanekoet al[11]suggested that surgical resection of a congenital mucous cyst of the tongue is safely performed at 1 year of age,although the timing of surgery depends on the degree of breathing and feeding impairments,and the child’s development.However,all reported cases of prenatally diagnosed heterotopic gastrointestinal cysts,including our case,involved cyst excision within 1 year and had a good outcome[4-10].Thus,aspiration is effective for initial airway and feeding management,but frequent aspiration should be avoided because of the risk of infection and adjacent tissue damage.If the cyst grows and repeated aspiration is difficult,it may be better to perform excision at that time.
CONCLUSION
We described the surgical treatment of a lingual heterotopic gastrointestinal cyst in a newborn.Airway distress and feeding difficulty were successfully avoided by cyst aspiration,and surgical resection was performed on the 67thday with no perioperative complications.
 World Journal of Clinical Cases2020年17期
World Journal of Clinical Cases2020年17期
- World Journal of Clinical Cases的其它文章
- Autoimmunity as the comet tail of COVID-19 pandemic
- Gender medicine:Lessons from COVID-19 and other medical conditions for designing health policy
- Complexities of diagnosis and management of COVID-19 in autoimmune diseases:Potential benefits and detriments of immunosuppression
- Incidental anal 18fluorodeoxyglucose uptake:Should we further examine the patient?
- Emergency surgery in COVID-19 outbreak:Has anything changed?Single center experience
- Somatostatin receptor scintigraphy in the follow up of neuroendocrine neoplasms of appendix